Abstract
Background: This study aimed to examine whether individuals with chronic tinnitus report more positive experiences following internet-based cognitive behavioral therapy (CBT). Methods: A mixed-methods design was used, nested in clinical trials evaluating internet interventions for tinnitus. Participants (n = 164) completed online questionnaires (both structured and open-ended) providing demographic information as well as health variables (e.g., tinnitus distress, anxiety, depression, insomnia). An open-ended question listing positive effects or outcomes related to having tinnitus was also included. Responses to the open-ended questions were analyzed using qualitative content analysis. Results: Of the 164 eligible participants, 32.3% (n = 53) provided at least 1 positive experience both at pre- and post-intervention, with 9.1% (n = 19) providing positive experiences only at pre-intervention, 49 (29.9%) providing positive experiences only at post-intervention, and 28.7% (n = 47) of the participants did not provide any positive experiences on either measurement occasion. Significantly more positive experiences were reported following the intervention in the overall sample (p < 0.0001, paired sample t-test). In addition, participants who reported positive experiences in both pre- and post-intervention also reported more positive experiences following intervention (p = 0.008, paired sample t-test). Conclusions: Internet-based CBT can help individuals with tinnitus to think more positively by changing unhelpful thought patterns. Open-ended questions can supplement structured questionnaires to measure treatment outcomes.
1. Introduction
Individuals with tinnitus experience perception of sound(s) in the absence of any external sound stimulus. Tinnitus is a common chronic condition in adults, affecting nearly 15% of the population around the world [1]. While a majority of individuals with tinnitus adapt well and learn different ways to cope with the condition, some of the individuals with severe tinnitus may develop maladaptive strategies and experience many negative consequences such as difficulty focusing on a task, difficulty sleeping, anxiety, depression, and reduced health-related quality of life [2,3]. For this reason, many individuals with tinnitus may need an intervention to manage their condition and to live well with their tinnitus.
Tinnitus can be of various types [4]. For instance, if no clear cause can be found, it is referred to as primary tinnitus. On the other hand, if there is an identifiable cause (e.g., ear infection, ear drum perforation, vascular disease), it is referred to as secondary tinnitus. Also, chronic tinnitus is referred to as experiencing these sounds for three months or longer.
Currently, there is no known cure for tinnitus, with a few exceptions when an otological condition is causing tinnitus (e.g., ear infection). There are, however, several management strategies that can help those individuals who experience negative consequences. These can be broadly grouped into four groups. First, psychological interventions such as cognitive behavioral therapy (CBT). Second, sound therapy-based interventions such as hearing aids, masking devices, or neuromodulation (i.e., training the brain to ignore tinnitus sound through delivery of sound, electricity, or other stimuli). It is noteworthy that hearing aid intervention is suggested for individuals with tinnitus who have an accompanying hearing loss. Third, a combination of psychological and sound-therapy-based interventions such as progressive tinnitus management (PTM) or Tinnitus Retraining Therapy (TRT). Fourth, alternative/complementary medicine treatments such as herbal therapies, etc. Out of these management strategies, CBT intervention has the best research support for reducing tinnitus distress [5]. CBT is a form of psychotherapy and aims to improve the quality of life in individuals with tinnitus through principles of habituation, cognitive restructuring, and the development of coping skills [6]. Relaxation strategies as well as thought modification involve skills to handle dysfunctional cognitions in relation to tinnitus (such as catastrophizing) [7]. While clinical trials on CBT have reported a range of positive outcomes in terms of reduced tinnitus distress, insomnia, anxiety, and depression, the extent to which CBT strategies increase positive thoughts and experiences in individuals with tinnitus has not been reported.
A sub-field of psychology studying positive experiences related to chronic health conditions and disabilities is referred to as positive psychology. Positive psychology focuses on wellbeing with the idea that individuals with chronic conditions may benefit from creating a context for wellbeing in addition to symptom reduction [8]. Several studies have examined the effect of using a positive psychology approach to building psychological interventions for various conditions and have reported positive outcomes [9,10]. In addition, during the last decade, numerous studies have examined positive experiences related to hearing and balance conditions such as hearing loss, tinnitus, and Ménière’s disease (for review see [11]. Three separate cross-sectional studies conducted in Finland [12], the United Kingdom [13], and the United States [14] have examined and reported positive experiences related to tinnitus elicited from an open-ended question. The common themes tend to be about outlook on life (e.g., I am grateful for my life), personal development (e.g., I am more aware of what I can handle), treatment-related benefits (e.g., I am protecting my ears by wearing ear plugs), coping strategies (e.g., learned how to manage stress through relaxation exercises), support received (e.g., compassion from others with tinnitus), and disease-specific aspects (e.g., I think it may actually help lull me to sleep).
Despite the progress in adopting positive psychology approaches to hearing health, much of the published literature focuses solely on the natural course of disease and open-ended questions on how individuals with hearing and balance problems identify and report positive experiences. The studies do provide some understanding of acceptance and coping. We are, however, not aware of any studies examining the effects of psychological interventions in promoting positive psychology within the field of hearing and also more specifically to tinnitus populations. The current study therefore examined if individuals with tinnitus report more positive experiences to an open-ended question following an internet-based CBT (ICBT).
2. Methods
2.1. Study Design
This study used a pretest–posttest design and was nested in clinical trials (Clinical Trials.gov registration numbers NCT04004260, NCT04335812) that were aimed at evaluating the efficacy of ICBT for tinnitus [15,16,17]. Ethics approval was granted by the Institutional Review Board at Lamar University (IRB-FY17-209 and IRB-FY20-200). All participants completed informed consent prior to participating in the study.
2.2. Data Collection
All participants (n = 164) who were enrolled in the ICBT clinical trials were asked to complete a series of questionnaires before and after the intervention through the online platform (i.e., iTerapi) that was used to administer ICBT. The inclusion (i.e., adults > 18 years, ability to read and type in English or Spanish, access to computer, having tinnitus for longer than 3 months, at least a mild severity of tinnitus) and exclusion criteria (i.e., having significant depression, psychiatric condition, pulsatile or objective tinnitus, currently undergoing other tinnitus therapies) are detailed in the clinical trial publications [15,16,17]. Chronic tinnitus was defined as experiencing tinnitus for at least 3 months or longer. These included (a) a demographic questionnaire, (b) several standardized structured questionnaires focusing on tinnitus distress (i.e., Tinnitus Functional Index; TFI), anxiety (i.e., Generalized Anxiety Disorder 7; GAD7), depression (i.e., Patient Health Questionnaire 9; PHQ9), insomnia (i.e., Insomnia Severity Index; ISI), and health-related quality of life (i.e., Euroqol EQ-5D-5L), and (b) open-ended questions. The current study was focused on analyzing the responses to an open-ended question focusing on positive experiences, which was worded as “Make a list of any positive effects or outcomes related to having tinnitus, list as many as you can think of”. Further details about the data collection have been provided in our clinical trial reporting [15,16,17]. The study sample was categorized into four groups based on their response patterns to the open-ended question: Group 1 (n = 53): both pre- and post-intervention; Group 2 (n = 15): only during pre-intervention; Group 3 (n = 49): only during post-intervention; and Group 4 (n = 47): no response in both pre- and post-intervention.
2.3. Data Analysis
The data analysis included a mixed methods approach. The demographic items and responses to structured questionnaires across groups were analyzed using descriptive and analytical statistics using the IBM SPSS software version 29. Responses to open-ended questions were coded using qualitative content analysis [18]. Only the responses of Group 1 were included in the qualitative analysis. Differences in the mean number of responses to open-ended questions in the overall sample as well as in groups that provided at least one response in both pre- and post-intervention were examined using the paired sample t-test as the data met the assumption of normality using the Shapiro–Wilk test (p > 0.05).
3. Results
3.1. Participant Characteristics
One hundred and sixty-four individuals participating in ICBT clinical trials were included in the present study. Participants had a mean age of 58.44 years (SD: 11.54 years, mean duration of tinnitus in 13.91 years; 97 females and 67 males). Table 1 provides the participant characteristics, including responses to structured questionnaires across the four groups.

Table 1.
Demographic details of study participants (n = 163).
3.2. Number of Positive Experiences
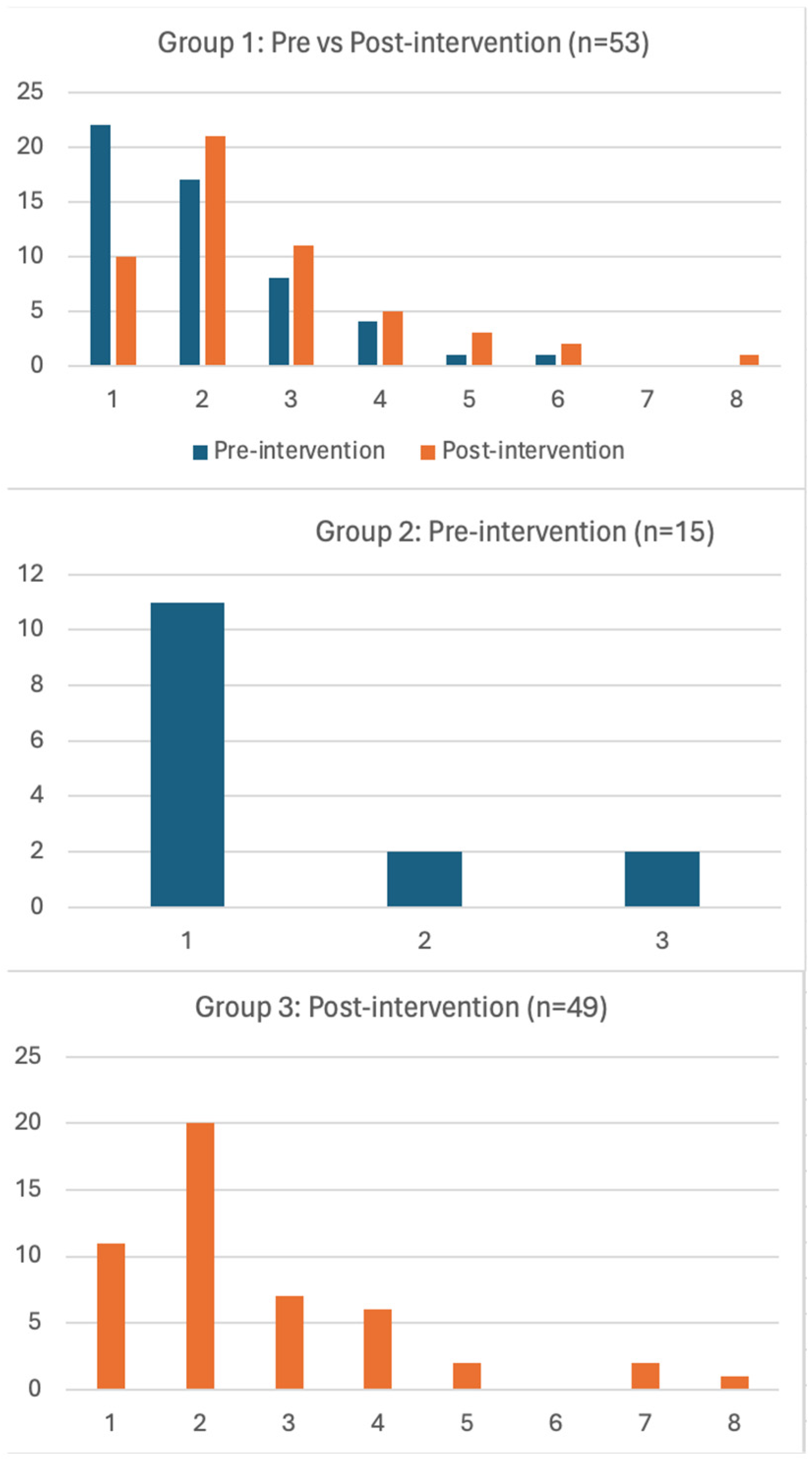
Figure 1 presents the number of positive experiences per participant across groups. Of the 163 participants, 54 (32.3%) provided at least one positive experience in both pre- and post-intervention (group 1), 15 (9.1%) provided positive experiences only during pre-intervention, 49 (29.9%) provided positive experiences only during post-intervention, and 47 (28.7%) participants did not provide any positive experience in both pre- and post-intervention. Table 2 presents the number of participants reporting positive experiences pre- and post-intervention in the overall sample as well as across the sub-groups. A total of 128 and 268 responses were reported in pre- and post-intervention, respectively, in the overall sample. More participants reported positive experiences following the intervention in the overall sample (pre-intervention mean = 0.78, post-intervention mean = 1.63, p < 0.0001). In addition, a total of 107 and 140 responses were reported in pre- and post-intervention, respectively, in Group 1 showing that participants who reported positive experiences in both pre- and post-intervention also reported more positive experiences following intervention (pre-intervention mean = 2.02; post-intervention mean = 2.6; p = 0.008).
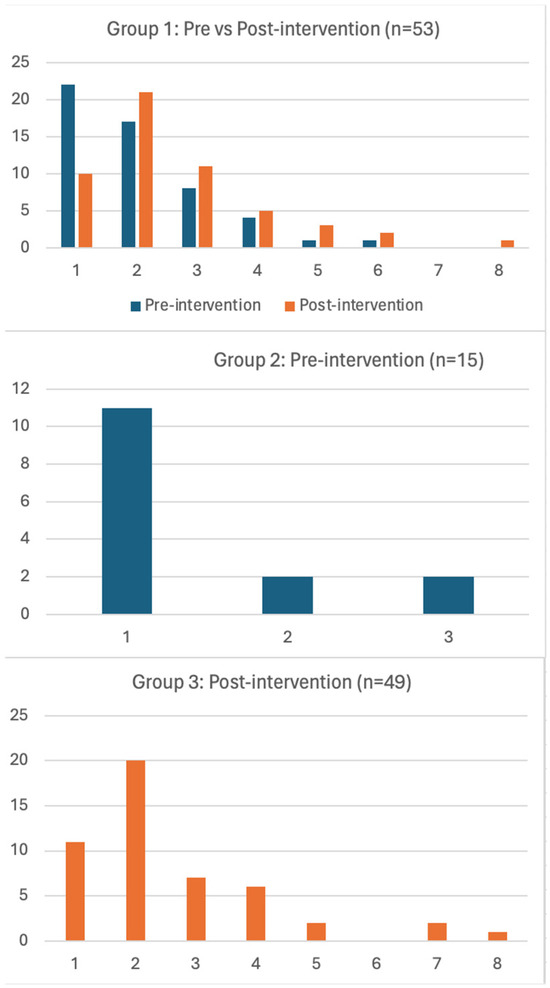
Figure 1.
Number of positive experiences (x-axis) reported by individual study participants (y-axis) in different groups during pre- and post-intervention.
Table 2.
Total number of positive experiences reported by overall sample and different groups during pre- and post-intervention (statistical significance tested at p < 0.05).
3.3. Positive Experiences Related to Tinnitus
Table 3 presents the categories, sub-categories, frequencies, and an example of a meaning unit based on the qualitative content analysis of responses to open-ended questions on positive experiences. The analyses identified 6 categories and 23 sub-categories. The categories remained the same, for both pre- and post-intervention, although some variation in sub-categories was found. For instance, the sub-category learned new techniques and skills only emerged in post-intervention. The sub-categories empathy, resilience, self-care, self-improvement, spirituality, helping others, and new relationships were only found in pre-intervention responses.
Table 3.
Positive experiences reported for an open-ended question pre- and post-intervention.
3.4. Outlook
This theme focused on change in outlook in terms of point of view or general attitude. Many participants reported that they realized they are not alone, developed appreciation for what they have and empathy towards others, and also developed self-awareness and resilience. This was the dominant theme in pre-intervention with 50 (46.7%) and 34 (24.3%) meaning units identified in pre- and post-intervention responses, respectively.
3.5. Personal Development
Many individuals with tinnitus reported that experiencing chronic conditions such as tinnitus helped them reflect on their condition, which resulted in the realization of self-awareness of their capabilities as well as care for themselves, resulting in personal development. This theme was reported in 10 (9.3%) and 7 (5%) meaning units, respectively, in pre- and post-intervention.
3.6. Coping
This theme included items on how individuals were coping with their condition. This included adaptation, making behavior changes, as well as finding spiritual reasons. The coping theme had 16 (15%) and 26 (18.6%) meaning units in pre- and post-interventions, respectively.
3.7. Support
Support from other is an important component in managing chronic conditions such as tinnitus. Many individuals with tinnitus reported that their condition helped them better understand their relationships as well as think about helping others. Many also sought help from local and national support groups, which helped them make new friends. This theme had 7 (6.5%) and 1 (0.7%) in pre- and post-interventions, respectively.
3.8. Treatment-Related
Managing tinnitus and in particular finding an evidence-based management for tinnitus is challenging. Hence, many individuals with tinnitus were appreciative of helpful treatments that resulted in positive experiences in terms of learning new techniques as well as making behavior changes. As expected, this was the dominant theme post-intervention. A total of 17 (16%) and 61 (43.5%) meaning units were identified in pre- and post-intervention responses, respectively.
3.9. Disease-Specific Experiences
Some individuals with tinnitus think they have positive experiences directly or indirectly as a result of living with this condition. This is a way for some individuals to accept the condition and learn to cope. This theme had 7 (6.5%) and 11 (7.9%) meaning units, respectively, in pre- and post-intervention responses.
4. Discussion
Our findings suggest that more participants reported positive experiences following the intervention, which align with previous research demonstrating the efficacy of CBT in reducing tinnitus distress [5,6]. However, our study uniquely contributes to the literature by showing an increase in positive experiences, a novel outcome in the context of tinnitus management. The increase in positive experiences post-intervention could be attributed to the principles of cognitive restructuring and the development of coping skills inherent in CBT [9,10]. These elements help individuals reframe their perceptions of tinnitus, thereby fostering a more positive outlook.
In both research and healthcare service delivery, it is common to ask individuals with chronic conditions about the adverse effects of their illness, disease, or condition. This of course is key to understanding the extent to which the individual is impacted and to aid in the understanding of both severity and intervention strategies. However, this approach assumes that chronic conditions such as tinnitus could only have negative consequences. Recent disability models such as the World Health Organization’s International Classification of Functioning, Disability, and Health [19] recognize that the outcome of the disease and/or health conditions can be modified by contextual factors (i.e., environmental and personal factors). In this context, personal factors such as personality and temperament could make some individuals think alternatively and consider both positive and negative consequences. This small difference could indeed determine who may cope and manage well with their chronic condition versus those who do not. Nevertheless, an even more important question is if the interventions we provide could change the thought patterns of individuals with chronic conditions such as tinnitus and make them think more positively. The current study provides some preliminary data to support this idea.
During the pre-intervention, outlook was the dominant theme (39% meaning units), suggesting that individuals who report positive experiences are mainly related to their point of view or attitude. On the other hand, treatment-related benefits were the dominant theme of positive experiences post-intervention, suggesting individuals can indeed derive positive benefits. Nevertheless, it is important to recognize that many individuals with chronic conditions such as tinnitus continue to look for a cure or silencing their tinnitus [20]. However, in conditions where we do not have a known cure, considering evidence-based treatments such as CBT and making them accessible and affordable through the use of digital technologies should be a priority. The study results also support the idea of including positive questioning during case history and during treatment sessions, especially using open-ended questions.
Although many of this study’s participants reported finding positive experiences, many individuals noted a small number of positive experiences. Additionally, some participants were unable to identify positive experiences. These results are similar to those previously reported (e.g., [13], suggesting potential improvement with modification of the intervention. For instance, adding information in the interventions highlighting the main themes surrounding the key positive experience themes, such as outlook, support, and personal development, would be beneficial. It may also be that tailoring the intervention for certain populations is required. Loughlin et al. (2024), for instance, identified that younger participants and those with lower hearing disability were more likely to report positive experiences, which also appears to be the case in the present research. Older adults may need more guidance and examples.
4.1. Clinical Implications
Clinicians should consider incorporating open-ended questions into their assessment protocols to capture a broader range of patient experiences. This approach can complement standardized measures and provide a more comprehensive understanding of treatment outcomes. Moreover, integrating modules that focus on fostering positive experiences and resilience into CBT programs for tinnitus could enhance overall treatment efficacy. Clinicians might also benefit from training in positive psychology techniques to support this integration.
4.2. Study Limitations
This study has some limitations that need consideration. First, this study was nested in a clinical trial that had many outcome measures. This may have resulted in an additional burden for individuals and, as a result, participants may have provided limited data for an open-ended question that is optional, resulting in a potential response bias. Second, our literature review on positive experiences related to hearing and balance conditions found that only about 40–45% of individuals provide answers to open questions, and this can increase to a 90% response rate when using structured questionnaires [11]. For this reason, developing a structured positive experience questionnaire based on qualitative data for future studies could be helpful. The core outcome set (COS) based on the Core Outcome Measures in Tinnitus (COMiT) initiative suggests including an outcome measure on negative thoughts and beliefs in psychology-based tinnitus intervention [21]. We would argue that it may be helpful to also include a positive approach focusing on negative thoughts to help understand symptom resolution, whereas examining positive aspects helps understand well-being.
5. Conclusions
Overall, this study highlights the potential of internet-based CBT to not only reduce tinnitus distress but also enhance positive experiences among individuals with tinnitus. Incorporating positive psychology into tinnitus management could provide a more holistic approach to improving patient outcomes.
Author Contributions
Conceptualization, V.M., E.W.B. and G.A.; formal analysis, V.M., E.B. and V.; methodology, V.M., E.W.B., G.A., D.W.S., K.U. and V.; writing—original draft, V.M.; Writing—review and editing, E.W.B., G.A., E.B., D.W.S., K.U. and V. All authors have read and agreed to the published version of the manuscript.
Funding
This work was partially funded by the National Institute on Deafness and Communication Disorders (NIDCD) of the National Institute of Health (NIH) under the award number R21DC017214. The funding agency did not have any role in the design or execution of the study.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and ethics approval was granted by the Institutional Review Board at Lamar University (IRB-FY17-209 and IRB-FY20-200).
Informed Consent Statement
All participants completed informed consent prior to participating in the study.
Data Availability Statement
The data that support the findings of this study are openly available in Figshare at http://doi.org/10.6084/m9.figshare.13681924 (accessed on 18 August 2024).
Conflicts of Interest
The authors declare no conflict of interest.
References
- Jarach, C.M.; Lugo, A.; Scala, M.; van den Brandt, P.A.; Cederroth, C.R.; Odone, A.; Garavello, W.; Schlee, W.; Langguth, B.; Gallus, S. Global Prevalence and Incidence of Tinnitus: A Systematic Review and Meta-analysis. JAMA Neurol. 2022, 79, 888–900. [Google Scholar] [CrossRef] [PubMed]
- Manchaiah, V.; Nisha, K.V.; Prabhu, P.; Granberg, S.; Karlsson, E.; Andersson, G.; Beukes, E.W. Examining the consequences of tinnitus using the multidimensional perspective. Acta Oto Laryngol. 2022, 142, 67–72. [Google Scholar] [CrossRef]
- Molnár, A.; Mavrogeni, P.; Tamás, L.; Maihoub, S. Correlation Between Tinnitus Handicap and Depression and Anxiety Scores. Ear Nose Throat J. 2022, 01455613221139211. [Google Scholar] [CrossRef]
- Mavrogeni, P.; Maihoub, S.; Tamás, L.; Molnár, A. Tinnitus characteristics and associated variables on Tinnitus Handicap Inventory among a Hungarian population. J. Otol. 2022, 17, 136–139. [Google Scholar] [CrossRef] [PubMed]
- Fuller, T.; Cima, R.; Langguth, B.; Mazurek, B.; Vlaeyen, J.W.S.; Hoare, D.J. Cognitive behavioural therapy for tinnitus. Cochrane Database Syst. Rev. 2020, 1, CD012614. [Google Scholar] [CrossRef] [PubMed]
- Jun, H.J.; Park, M.K. Cognitive behavioral therapy for tinnitus: Evidence and efficacy. Korean J. Audiol. 2013, 17, 101–104. [Google Scholar] [CrossRef] [PubMed]
- Andersson, G. Psychological aspects of tinnitus and the application of cognitive-behavioral therapy. Clin. Psychol. Rev. 2002, 22, 977–990. [Google Scholar] [CrossRef] [PubMed]
- Tulip, C.; Fisher, Z.; Bankhead, H.; Wilkie, L.; Pridmore, J.; Gracey, F.; Tree, J.; Kemp, A.H. Building Wellbeing in People with Chronic Conditions: A Qualitative Evaluation of an 8-Week Positive Psychotherapy Intervention for People Living with an Acquired Brain Injury. Front. Psychol. 2020, 11, 66. [Google Scholar] [CrossRef]
- Bolier, L.; Haverman, M.; Westerhof, G.J.; Riper, H.; Smit, F.; Bohlmeijer, E. Positive psychology interventions: A meta-analysis of randomized controlled studies. BMC Public Health 2013, 13, 119. [Google Scholar] [CrossRef]
- Chakhssi, F.; Kraiss, J.T.; Sommers-Spijkerman, M.; Bohlmeijer, E.T. The effect of positive psychology interventions on well-being and distress in clinical samples with psychiatric or somatic disorders: A systematic review and meta-analysis. BMC Psychiatry 2018, 18, 211. [Google Scholar] [CrossRef]
- Manchaiah, V.; Baguley, D.M.; Pyykkö, I.; Kentala, E.; Levo, H. Positive experiences associated with acquired hearing loss, Ménière’s disease, and tinnitus: A review. Int. J. Audiol. 2015, 54, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Kentala, E.; Wilson, C.; Pyykkö, I.; Varpa, K.; Stephens, D. Positive experiences associated with tinnitus and balance problems. Audiol. Med. 2008, 6, 55–61. [Google Scholar]
- Beukes, E.W.; Manchaiah, V.; Valien, T.E.; Baguley, D.M.; Allen, P.M.; Andersson, G. Positive experiences related to living with tinnitus: A cross-sectional survey. Clin. Otolaryngol. 2018, 43, 489–495. [Google Scholar] [CrossRef] [PubMed]
- Loughlin, J.; Das, V.; Manchaiah, V.; Beukes, E.; Andersson, G.; Shekhawat, G.S. The positive side of living with tinnitus: A cross-sectional study. Int. J. Audiol. 2024, 63, 358–365. [Google Scholar] [CrossRef] [PubMed]
- Beukes, E.W.; Andersson, G.; Fagelson, M.; Manchaiah, V. Audiologist-Supported Internet-Based Cognitive Behavioral Therapy for Tinnitus in the United States: A Pilot Trial. Am. J. Audiol. 2021, 30, 717–729. [Google Scholar] [CrossRef] [PubMed]
- Beukes, E.W.; Andersson, G.; Fagelson, M.A.; Manchaiah, V. Dismantling internet-based cognitive behavioral therapy for tinnitus. The contribution of applied relaxation: A randomized controlled trial. Internet Interv. 2021, 25, 100402. [Google Scholar] [CrossRef] [PubMed]
- Beukes, E.W.; Andersson, G.; Fagelson, M.; Manchaiah, V. Internet-Based Audiologist-Guided Cognitive Behavioral Therapy for Tinnitus: Randomized Controlled Trial. J. Med. Internet Res. 2022, 24, e27584. [Google Scholar] [CrossRef]
- Graneheim, U.H.; Lundman, B. Qualitative content analysis in nursing research: Concepts, procedures and measures to achieve trustworthiness. Nurse Educ. Today 2004, 24, 105–112. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. International Classification of Functioning, Disability and Health: ICF; WHO: Geneva, Switzerland, 2001; Available online: https://iris.who.int/handle/10665/42407 (accessed on 7 July 2024).
- Manchaiah, V.; Londero, A.; Deshpande, A.K.; Revel, M.; Palacios, G.; Boyd, R.L.; Ratinaud, P. Online Discussions About Tinnitus: What Can We Learn From Natural Language Processing of Reddit Posts? Am. J. Audiol. 2022, 31, 993–1002. [Google Scholar] [CrossRef]
- Hall, D.A.; Smith, H.; Hibbert, A.; Colley, V.; Haider, H.F.; Horobin, A.; Londero, A.; Mazurek, B.; Thacker, B.; Fackrell, K.; et al. The COMiT’ID Study: Developing Core Outcome Domains Sets for Clinical Trials of Sound-, Psychology-, and Pharmacology-Based Interventions for Chronic Subjective Tinnitus in Adults. Trends Hear. 2018, 22, 2331216518814384. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).