
Association of Postoperative Serum Lactate Levels with Acute Kidney Injury in Mexican Patients Undergoing Cardiac Surgery
 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Clinical Characteristics
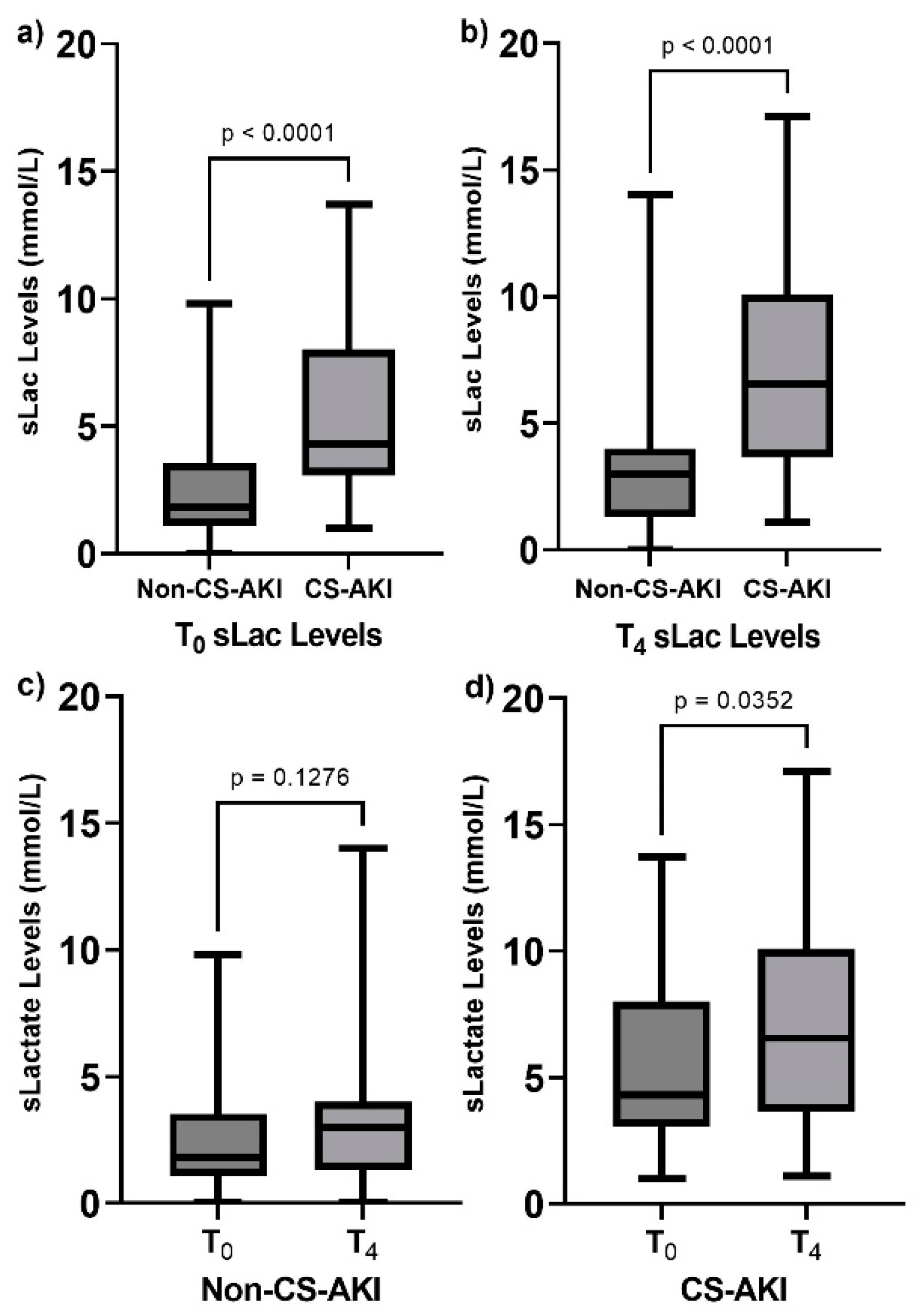
3.2. Serum Lactate Levels
3.3. Multivariate Analysis
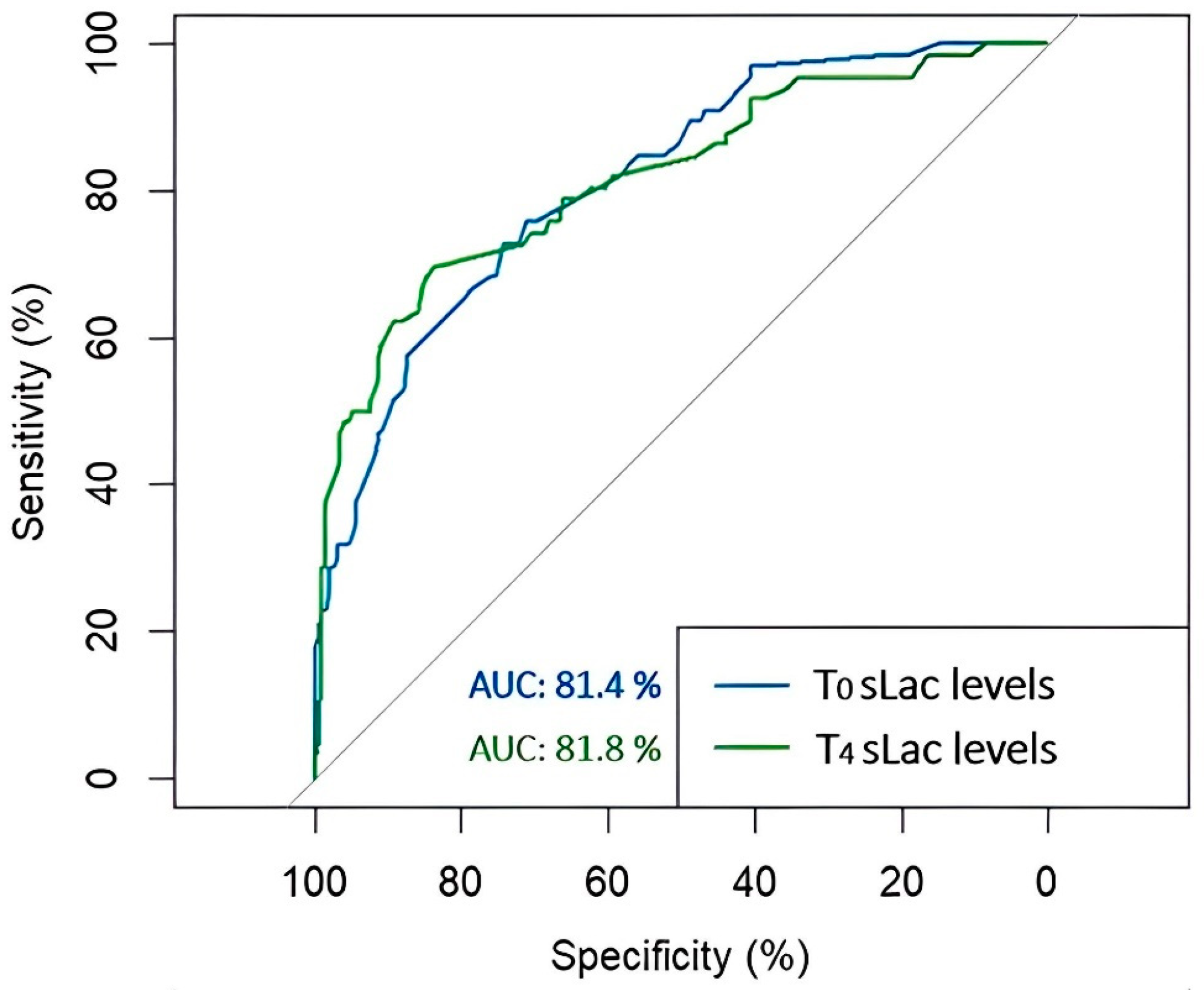
3.4. Receiver Operating Characteristic Curve of Serum Lactate Levels
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kellum, J.A.; Lameire, N. Diagnosis, evaluation, and management of acute kidney injury: A KDIGO summary (Part 1). Crit. Care 2013, 4, 204. [Google Scholar] [CrossRef]
- Harky, A.; Joshi, M.; Gupta, S.; Teoh, W.Y.; Gatta, F.; Snosi, M. Acute Kidney Injury Associated with Cardiac Surgery: A Comprehensive Literature Review. Braz. J. Cardiovasc. Surg. 2020, 35, 211–224. [Google Scholar] [CrossRef]
- Pickkers, P.; Darmon, M.; Hoste, E.; Joannidis, M.; Legrand, M.; Ostermann, M.; Prowle, J.R.; Schneider, A.; Schetz, M. Acute kidney injury in the critically ill: An updated review on pathophysiology and management. Intensive Care Med. 2021, 47, 835–850. [Google Scholar] [CrossRef]
- Su, L.J.; Li, Y.M.; Kellum, J.A.; Peng, Z.Y. Predictive value of cell cycle arrest biomarkers for cardiac surgery-associated acute kidney injury: A meta-analysis. Br. J. Anaesth. 2018, 121, 350–357. [Google Scholar] [CrossRef]
- Thiele, R.H.; Isbell, J.M.; Rosner, M.H. AKI associated with cardiac surgery. Clin. J. Am. Soc. Nephrol. 2015, 10, 500–514. [Google Scholar] [CrossRef]
- Wang, Y.; Bellomo, R. Cardiac surgery-associated acute kidney injury: Risk factors, pathophysiology and treatment. Nat. Rev. Nephrol. 2017, 13, 697–711. [Google Scholar] [CrossRef]
- Boyer, N.; Eldridge, J.; Prowle, J.R.; Forni, L.G. Postoperative Acute Kidney Injury. Clin. J. Am. Soc. Nephrol. 2022, 17, 1535–1545. [Google Scholar] [CrossRef]
- Hobson, C.; Ruchi, R.; Bihorac, A. Perioperative Acute Kidney Injury: Risk Factors and Predictive Strategies. Crit. Care Clin. 2017, 33, 379–396. [Google Scholar] [CrossRef]
- Gonçalves, M.; Gameiro, J.; Pereira, M.; Rodrigues, N.; Godinho, I.; Neves, M.; Gouveia, J.; Jorge, S.; Lopes, J.A. Serum lactates and acute kidney injury in patients with sepsis: A cohort analysis. Cogent Med. 2017, 4, 1388209. [Google Scholar] [CrossRef]
- Yan, G.; Wang, D.; Tang, C.; Ma, G. The Association of Serum Lactate Level with the Occurrence of Contrast-Induced Acute Kidney Injury and Long-Term Prognosis in Patients Undergoing Emergency Percutaneous Coronary Intervention. Int. J. Gen. Med. 2021, 14, 3087–3097. [Google Scholar] [CrossRef]
- Gomez-Martinez, R.; Tlacuilo-Parra, A.; Garibaldi-Covarrubias, R. Use of complementary and alternative medicine in children with cancer in Occidental, Mexico. Pediatr. Blood Cancer 2007, 49, 820–823. [Google Scholar] [CrossRef] [PubMed]
- Andersen, L.W.; Holmberg, M.J.; Doherty, M.; Khabbaz, K.; Lerner, A.; Berg, K.M.; Donnino, M.W. Postoperative Lactate Levels and Hospital Length of Stay After Cardiac Surgery. J. Cardiothorac. Vasc. Anesth. 2015, 29, 1454–1460. [Google Scholar] [CrossRef]
- El-Khoury, J.M.; Hoenig, M.P.; Jones, G.R.D.; Lamb, E.J.; Parikh, C.R.; Tolan, N.V.; Wilson, F.P. AACC Guidance Document on Laboratory Investigation of Acute Kidney Injury. J. Appl. Lab. Med. 2021, 6, 1316–1337. [Google Scholar] [CrossRef]
- Chavez-Iniguez, J.S.; Madero, M. Global Perspectives in Acute Kidney Injury: Mexico. Kidney360 2022, 3, 737–739. [Google Scholar] [CrossRef]
- Kellum, J.A.; Romagnani, P.; Ashuntantang, G.; Ronco, C.; Zarbock, A.; Hans-Joachim, A. Acute kidney injury. Nat. Rev. Dis. Primers 2021, 7, 52. [Google Scholar] [CrossRef]
- Negi, S.; Koreeda, D.; Kobayashi, S.; Iwashita, Y.; Shigematu, T. Renal replacement therapy for acute kidney injury. Ren. Replace. Ther. 2016, 27, 31. [Google Scholar] [CrossRef]
- Bairey-Merz, C.N.; Dember, L.M.; Ingelfinger, J.R.; Vinson, A.; Neugarten, J.; Sandberg, K.L.; Sullivan, J.C.; Maric-Bilkan, C.; Rankin, T.L.; Kimmel, P.L.; et al. Sex and the kidneys: Current understanding and research opportunities. Nat. Rev. Nephrol. 2019, 15, 776–783. [Google Scholar] [CrossRef]
- Darvishzadeh-Mahani, F.; Khaksari, M.; Raji-Amirhasani, A. Renoprotective effects of estrogen on acute kidney injury: The role of SIRT1. Int. Urol. Nephrol. 2021, 53, 2299–2310. [Google Scholar] [CrossRef]
- Wang, G.; Yang, L.; Ye, N.; Bian, W.; Ma, C.; Zhao, D.; Liu, J.; Hao, Y.; Yang, N.; Cheng, H. In-hospital acute kidney injury and atrial fibrillation: Incidence, risk factors, and outcome. Ren. Fail. 2021, 43, 949–957. [Google Scholar] [CrossRef]
- Karim, H.M.; Yunus, M.; Saikia, M.K.; Kalita, J.P.; Mandal, M. Incidence and progression of cardiac surgery-associated acute kidney injury and its relationship with bypass and cross clamp time. Ann. Card. Anaesth. 2017, 20, 22–27. [Google Scholar] [CrossRef]
- López-Delgado, J.C.; Esteve, F.; Torrado, H.; Rodríguez-Castro, D.; Carrio, M.L.; Farrero, E.; Javierre, C.; Ventura, J.L.; Manez, R. Influence of acute kidney injury on short- and long-term outcomes in patients undergoing cardiac surgery: Risk factors and prognostic value of a modified RIFLE classification. Crit. Care 2013, 17, R293. [Google Scholar] [CrossRef]
- Lombardi, R.; Ferreiro, A.; Servetto, C. Renal function after cardiac surgery: Adverse effect of furosemide. Ren. Fail. 2003, 25, 775–786. [Google Scholar] [CrossRef]
- Lassnigg, A.; Donner, E.; Grubhofer, G.; Presterl, E.; Druml, W.; Hiesmayr, M. Lack of renoprotective effects of dopamine and furosemide during cardiac surgery. J. Am. Soc. Nephrol. 2000, 11, 97–104. [Google Scholar] [CrossRef]
- Matsuura, R.; Komaru, Y.; Miyamoto, Y.; Yoshida, T.; Yoshimoto, K.; Isshiki, R.; Mayumi, K.; Yamashita, T.; Hamasaki, Y.; Nangaku, M.; et al. Response to different furosemide doses predicts AKI progression in ICU patients with elevated plasma NGAL levels. Ann. Intensive Care 2018, 17, 8. [Google Scholar] [CrossRef]
- Okorie, O.N.; Dellinger, P. Lactate: Biomarker and potential therapeutic target. Crit. Care Clin. 2011, 27, 299–326. [Google Scholar] [CrossRef]
- Vincent, J.L.; Quintairos, E.S.A.; Couto, L., Jr.; Taccone, F.S. The value of blood lactate kinetics in critically ill patients: A systematic review. Crit. Care 2016, 20, 257. [Google Scholar] [CrossRef]
- Zhang, Z.; Ni, H. Normalized lactate load is associated with development of acute kidney injury in patients who underwent cardiopulmonary bypass surgery. PLoS ONE 2015, 10, e0120466. [Google Scholar] [CrossRef]
- Radovic, M.; Bojic, S.; Kotur-Stevuljevic, J.; Lezaic, V.; Milicic, B.; Velinovic, M.; Karan, R.; Simic-Ogrizovic, S. Serum Lactate as Reliable Biomarker of Acute Kidney Injury in Low-risk Cardiac Surgery Patients. J. Med. Biochem. 2019, 38, 118–125. [Google Scholar] [CrossRef]
- Surgenor, S.D.; DeFoe, G.R.; Fillinger, M.P.; Likosky, D.S.; Groom, R.C.; Clark, C.; Helm, R.E.; Kramer, R.S.; Leavitt, B.J.; Klemperer, J.D.; et al. Intraoperative red blood cell transfusion during coronary artery bypass graft surgery increases the risk of postoperative low-output heart failure. Circ. J. 2006, 114, I43–I48. [Google Scholar] [CrossRef]
- Czempik, P.F.; Gierczak, D.; Wilczek, D.; Krzych, Ł.J. The Impact of Red Blood Cell Transfusion on Blood Lactate in Non-Bleeding Critically Ill Patients-A Retrospective Cohort Study. J. Clin. Med. 2022, 17, 1037. [Google Scholar] [CrossRef]
- Fakhari, S.; Bavil, F.M.; Bilehjani, E.; Abolhasani, S.; Mirinazhad, M.; Naghipour, B. Prophylactic furosemide infusion decreasing early major postoperative renal dysfunction in on-pump adult cardiac surgery: A randomized clinical trial. Res. Rep. Urol. 2017, 9, 5–13. [Google Scholar] [CrossRef]
- Wang, N.; Jiang, L.; Zhu, B.; Wen, Y.; Xi, X.M. Fluid balance and mortality in critically ill patients with acute kidney injury: A multicenter prospective epidemiological study. Crit. Care 2015, 19, 371. [Google Scholar] [CrossRef]
- Hobson, C.; Ozrazgat-Baslanti, T.; Kuxhausen, A.; Thottakkara, P.; Efron, P.A.; Moore, F.A.; Moldawer, L.L.; Segal, M.S.; Bihorac, A. Cost and Mortality Associated with Postoperative Acute Kidney Injury. Ann. Surg. 2015, 261, 1207–1214. [Google Scholar] [CrossRef]
- Mandelbaum, T.; Scott, D.J.; Lee, J.; Mark, R.G.; Malhotra, A.; Waikar, S.S.; Howell, M.D.; Talmor, D. Outcome of critically ill patients with acute kidney injury using the Acute Kidney Injury Network criteria. Crit. Care Med. 2011, 39, 2659–2664. [Google Scholar] [CrossRef]
- Mak, N.T.; Iqbal, S.; de Varennes, B.; Khwaja, K. Outcomes of post-cardiac surgery patients with persistent hyperlactatemia in the intensive care unit: A matched cohort study. J. Cardiothorac. Surg. 2016, 11, 33. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Variable | CS-AKI n = 66 (%) | Non-CS-AKI n = 198 (%) | p-Value |
|---|---|---|---|
| Preoperative risk factors | |||
| Age | 60 | 59 | 0.4407 |
| Gender | |||
| Female | 12 (18.2) | 64 (32.3) | 0.04 |
| Male | 54 (81.8) | 134 (67.7) | |
| T2DM | 26 (39.4) | 53 (26.8) | 0.07 |
| Smoking | 26 (39.4) | 71 (35.8) | 0.71 |
| Systemic Arterial Hypertension | 42 (63.6) | 103 (52) | 0.13 |
| Obesity | 34 (51.5) | 68 (34.3) | 0.019 |
| Dyslipidemia | 16 (24.2) | 52 (26.3) | 0.870 |
| Diastolic dysfunction | 54 (81.8) | 136 (68.6) | 0.057 |
| Atrial fibrillation | 24 (36.3) | 34 (17.2) | 0.002 |
| ACEI consumption | 17 (25.7) | 38 (19.2) | 0.33 |
| ARA consumption | 26 (39.4) | 56 (28.3) | 0.12 |
| Intraoperative risk factors | |||
| Transfusion | 66 (100) | 185 (93.4) | NA |
| <3 PRBCs | 28 (43) | 145 (73) | NA |
| ≥4 PRBCs | 37 (56) | 53 (27) | NA |
| CPB time | 156.0 [124.2–191.5] | 121.5 [87.25–159.75] | <0.0001 |
| AxC time | 109 [88–150] | 90 [67.5–116.8] | 0.0009 |
| Use of inotropes | 54 (81.8) | 142 (71.7) | 0.14 |
| Postoperative risk factors | |||
| Use of Furosemide | 15 (22.7) | 178 (89.8) | <0.0001 |
| Antiarrhythmics | 23 (34.8) | 34 (17.2) | 0.004 |
| Use of Vasopressors | 56 (84.8) | 123 (62.1) | 0.001 |
| Hospital length of stay (days) | 5 [3–8] | 3 [2–5] | <0.0001 |
| Variable | T0 Serum Lactate Level | T4 Serum Lactate Level | ||||
|---|---|---|---|---|---|---|
| β | OR [95%CI] | p-Value | β | OR [95%CI] | p-Value | |
| Hospital length of stay | 0.11 | 1.11 [1.05, 1.17] | 0.0002 | 0.08 | 1.10 [1.03–1.18] | 0.009 |
| Transfusion | ||||||
| ≤3 PRBCs | −1.16 | 0.31 [0.18, 0.53] | <0.0001 | −1.64 | 0.17 [0.08, 0.34] | <0.0001 |
| Furosemide use | ||||||
| ≤40 mg | −0.95 | 0.38 [0.16, 0.89] | 0.027 | −2.20 | 0.12 [0.04, 0.36] | <0.0001 |
| Variable | β Coefficient | OR [95% CI] | p-Value |
|---|---|---|---|
| Female gender | −1.46 | 0.23 [0.06, 0.71] | 0.015 |
| Hospital length of stay | 0.13 | 1.15 [1.04, 1.29] | 0.013 |
| CPB time | 0.02 | 1.03 [1.01–1.05] | 0.008 |
| Atrial fibrillation | 1.13 | 3.11 [1.08–9.40] | 0.037 |
| T0 serum lactate | 0.36 | 1.44 [1.12, 1.91] | 0.007 |
| T4 serum lactate | 0.31 | 1.38 [1.13, 1.69] | 0.001 |
| Use of furosemide ≤ 40 mg | −2.52 | 0.08 [0.02, 0.31] | 0.0005 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Flores-Salinas, H.-E.; Zambada-Gamboa, A.d.J.; Garcia-Garduño, T.-C.; Rodríguez-Zavala, G.; Valle, Y.; Chávez-Herrera, J.-C.; Martinez-Gutierrez, P.-E.; Godinez-Flores, A.; Jiménez-Limón, S.; Padilla-Gutiérrez, J.-R. Association of Postoperative Serum Lactate Levels with Acute Kidney Injury in Mexican Patients Undergoing Cardiac Surgery. Clin. Pract. 2024, 14, 1100-1109. https://doi.org/10.3390/clinpract14030087
Flores-Salinas H-E, Zambada-Gamboa AdJ, Garcia-Garduño T-C, Rodríguez-Zavala G, Valle Y, Chávez-Herrera J-C, Martinez-Gutierrez P-E, Godinez-Flores A, Jiménez-Limón S, Padilla-Gutiérrez J-R. Association of Postoperative Serum Lactate Levels with Acute Kidney Injury in Mexican Patients Undergoing Cardiac Surgery. Clinics and Practice. 2024; 14(3):1100-1109. https://doi.org/10.3390/clinpract14030087
Chicago/Turabian StyleFlores-Salinas, Héctor-Enrique, Anahí de Jesús Zambada-Gamboa, Texali-Candelaria Garcia-Garduño, Guillermo Rodríguez-Zavala, Yeminia Valle, Juan-Carlos Chávez-Herrera, Porfirio-Eduardo Martinez-Gutierrez, Arturo Godinez-Flores, Salvador Jiménez-Limón, and Jorge-Ramón Padilla-Gutiérrez. 2024. "Association of Postoperative Serum Lactate Levels with Acute Kidney Injury in Mexican Patients Undergoing Cardiac Surgery" Clinics and Practice 14, no. 3: 1100-1109. https://doi.org/10.3390/clinpract14030087
APA StyleFlores-Salinas, H.-E., Zambada-Gamboa, A. d. J., Garcia-Garduño, T.-C., Rodríguez-Zavala, G., Valle, Y., Chávez-Herrera, J.-C., Martinez-Gutierrez, P.-E., Godinez-Flores, A., Jiménez-Limón, S., & Padilla-Gutiérrez, J.-R. (2024). Association of Postoperative Serum Lactate Levels with Acute Kidney Injury in Mexican Patients Undergoing Cardiac Surgery. Clinics and Practice, 14(3), 1100-1109. https://doi.org/10.3390/clinpract14030087