

Magnesium Is a Vital Ion in the Body—It Is Time to Consider Its Supplementation on a Routine Basis



Abstract
1. Introduction
2. Search Methods
3. Results
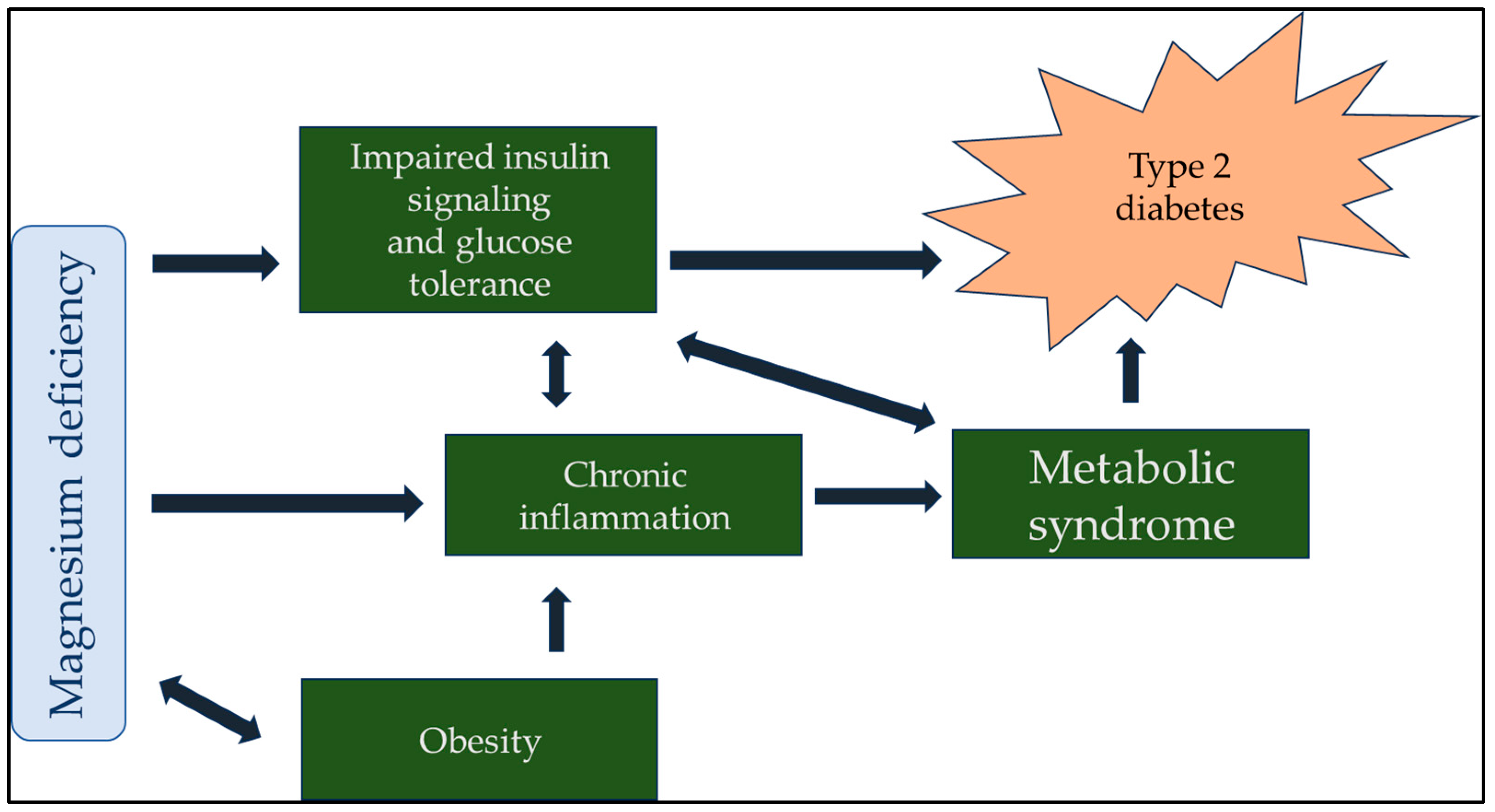
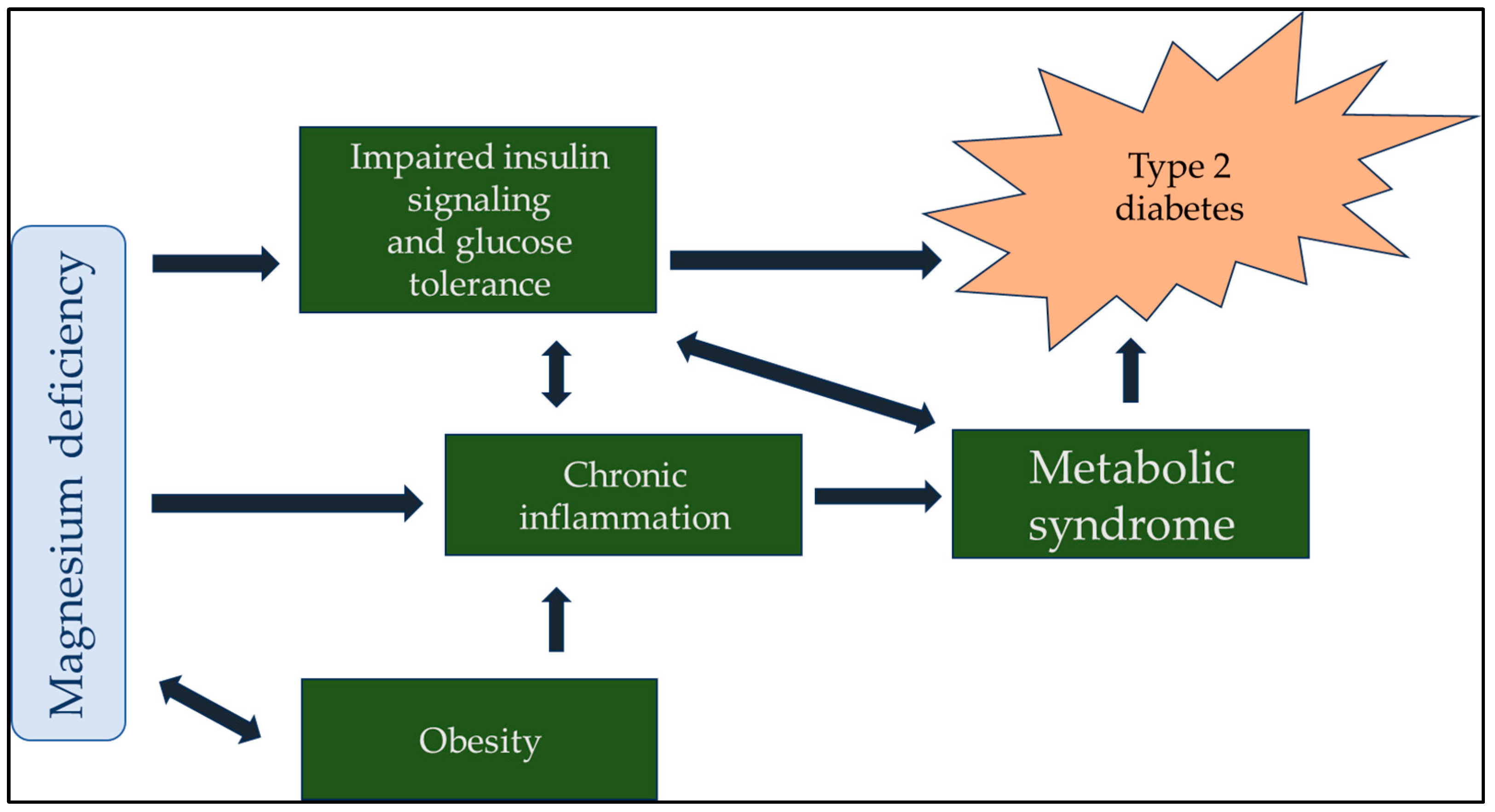
4. Hypomagnesemia and Diabetes
5. Hypomagnesemia and Cardiovascular Mortality
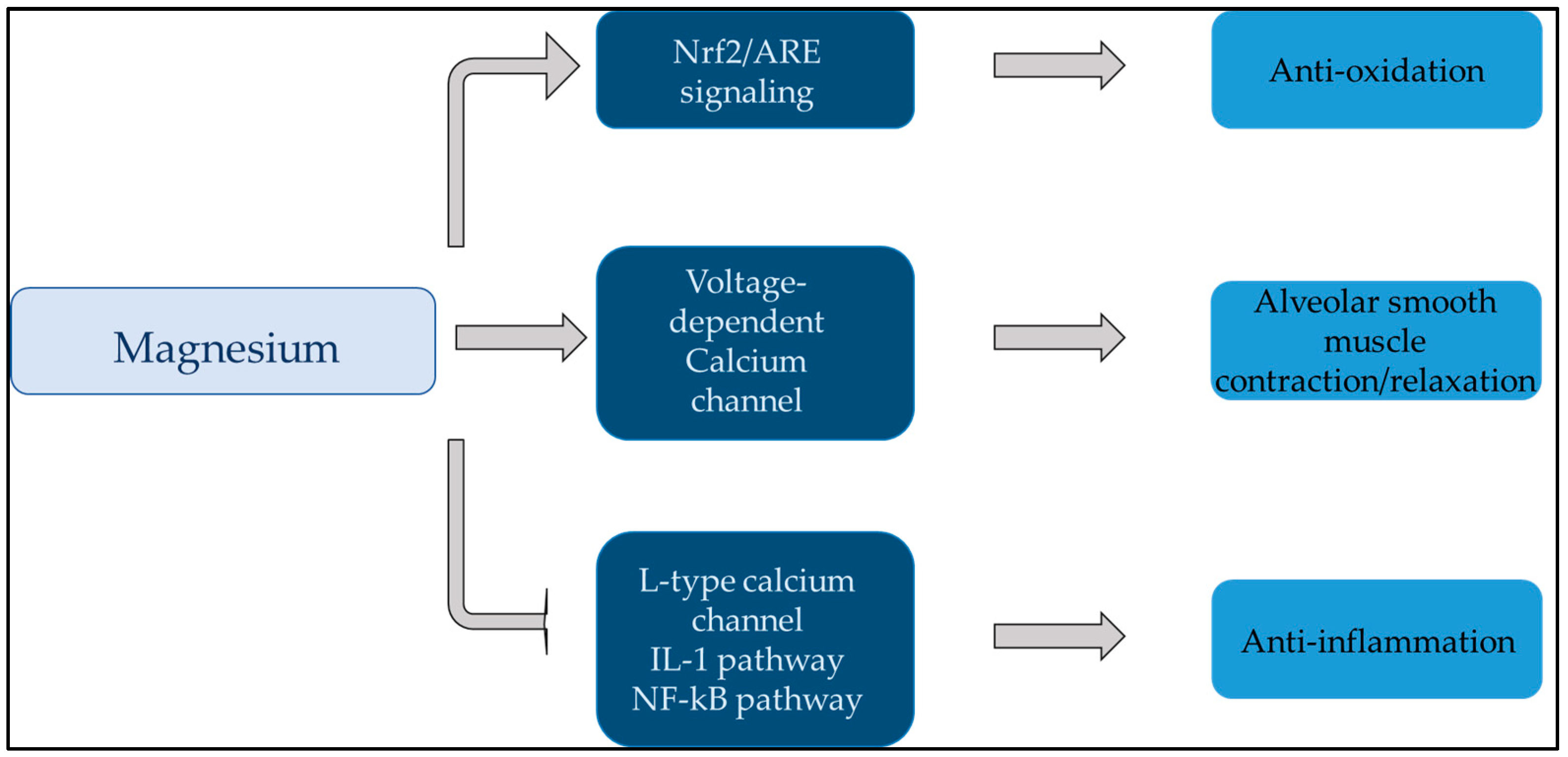
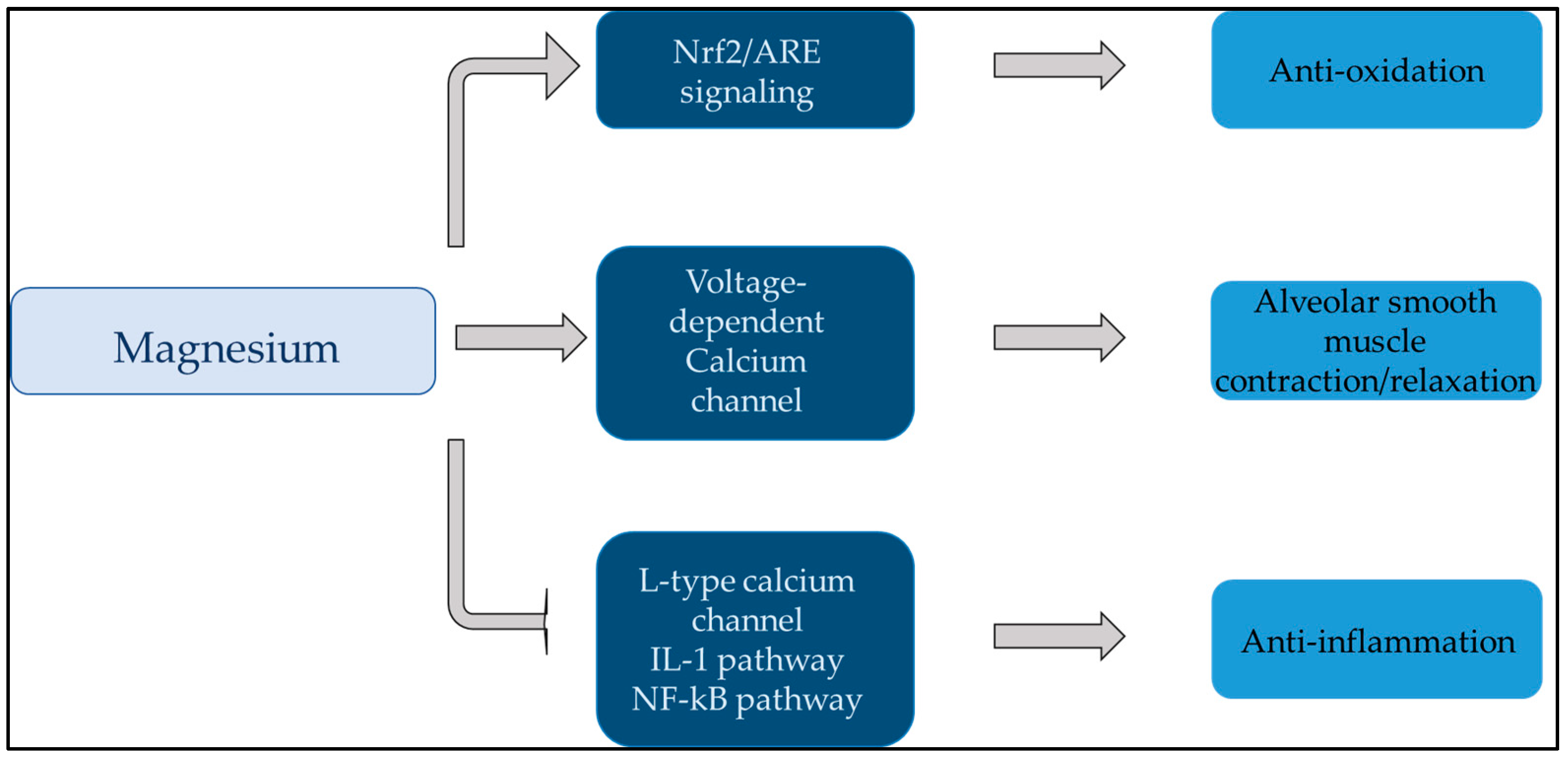
6. Hypomagnesemia and Respiratory Diseases
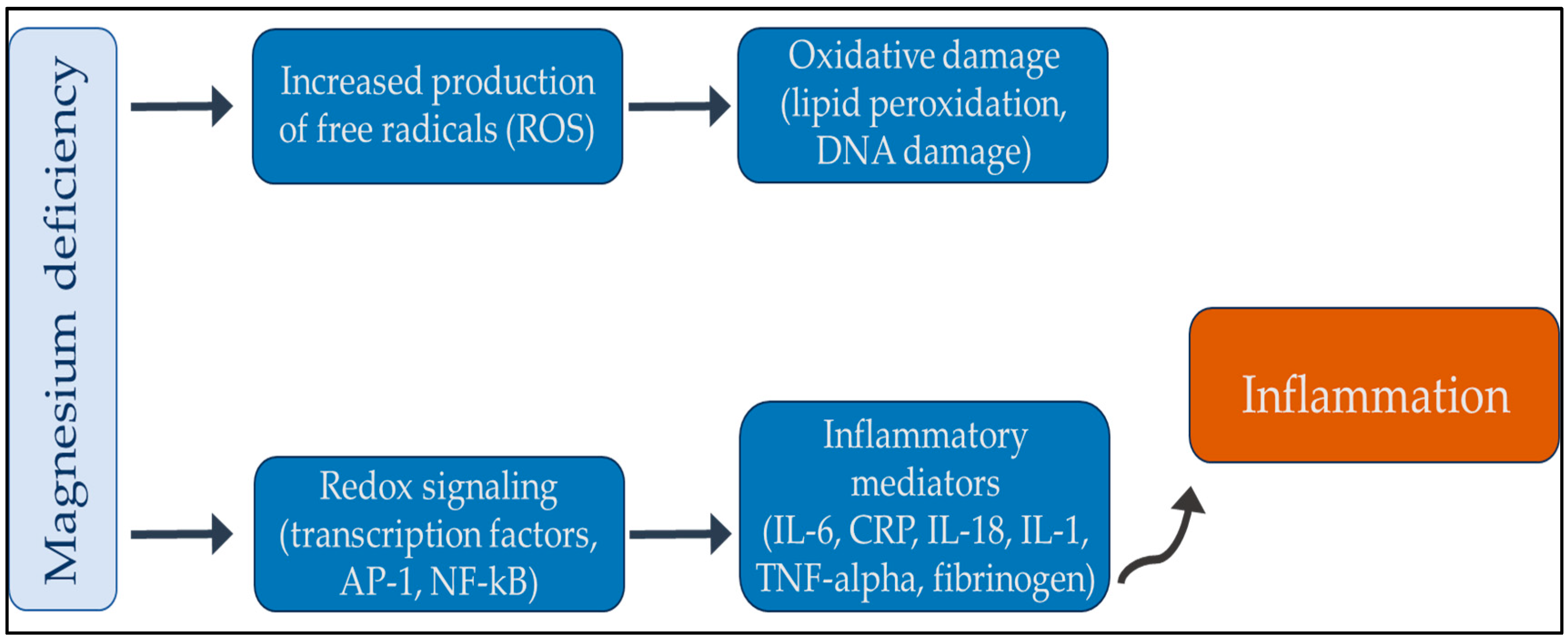
7. Hypomagnesemia and the Immune System
8. Hypomagnesemia and Cancer
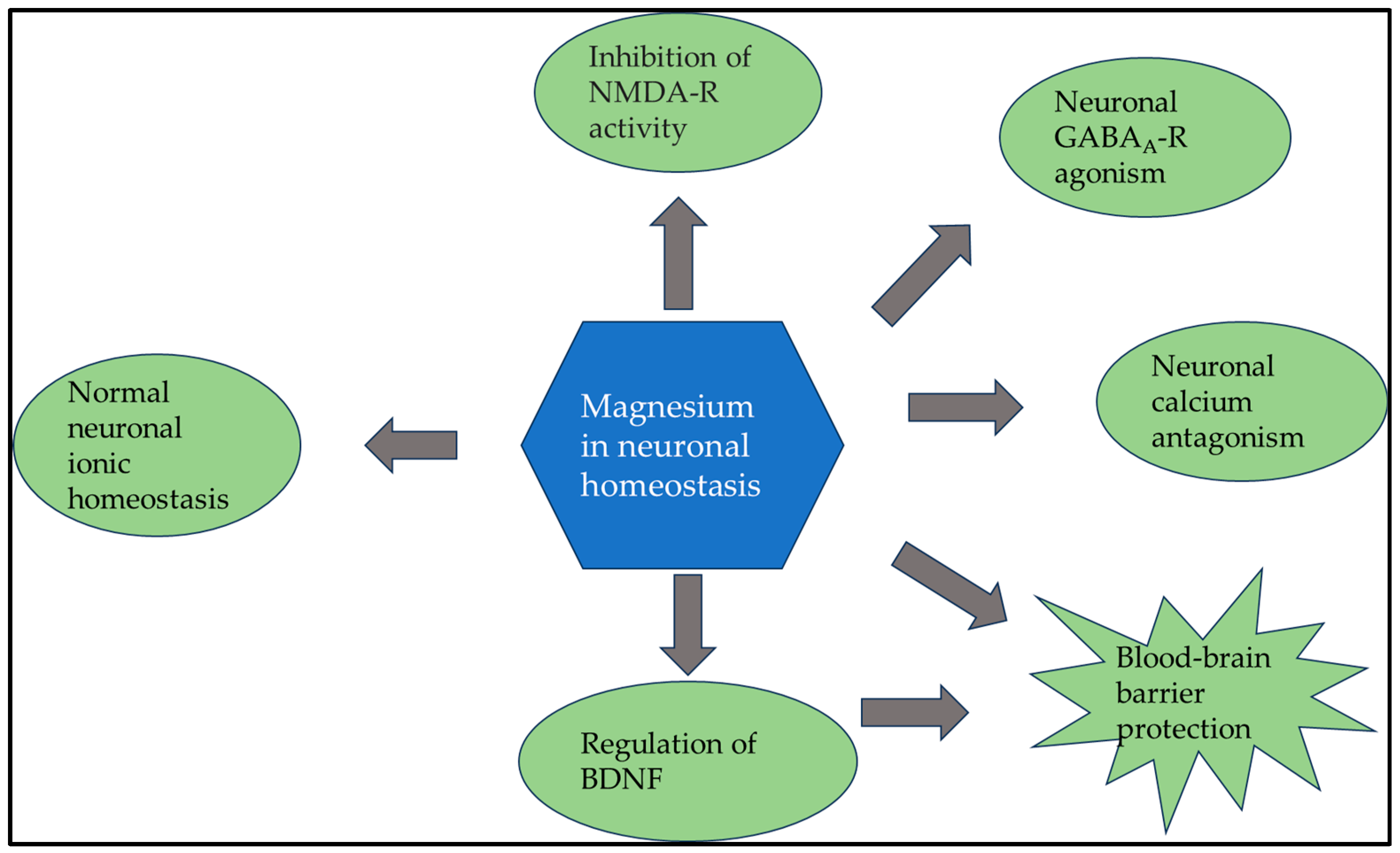
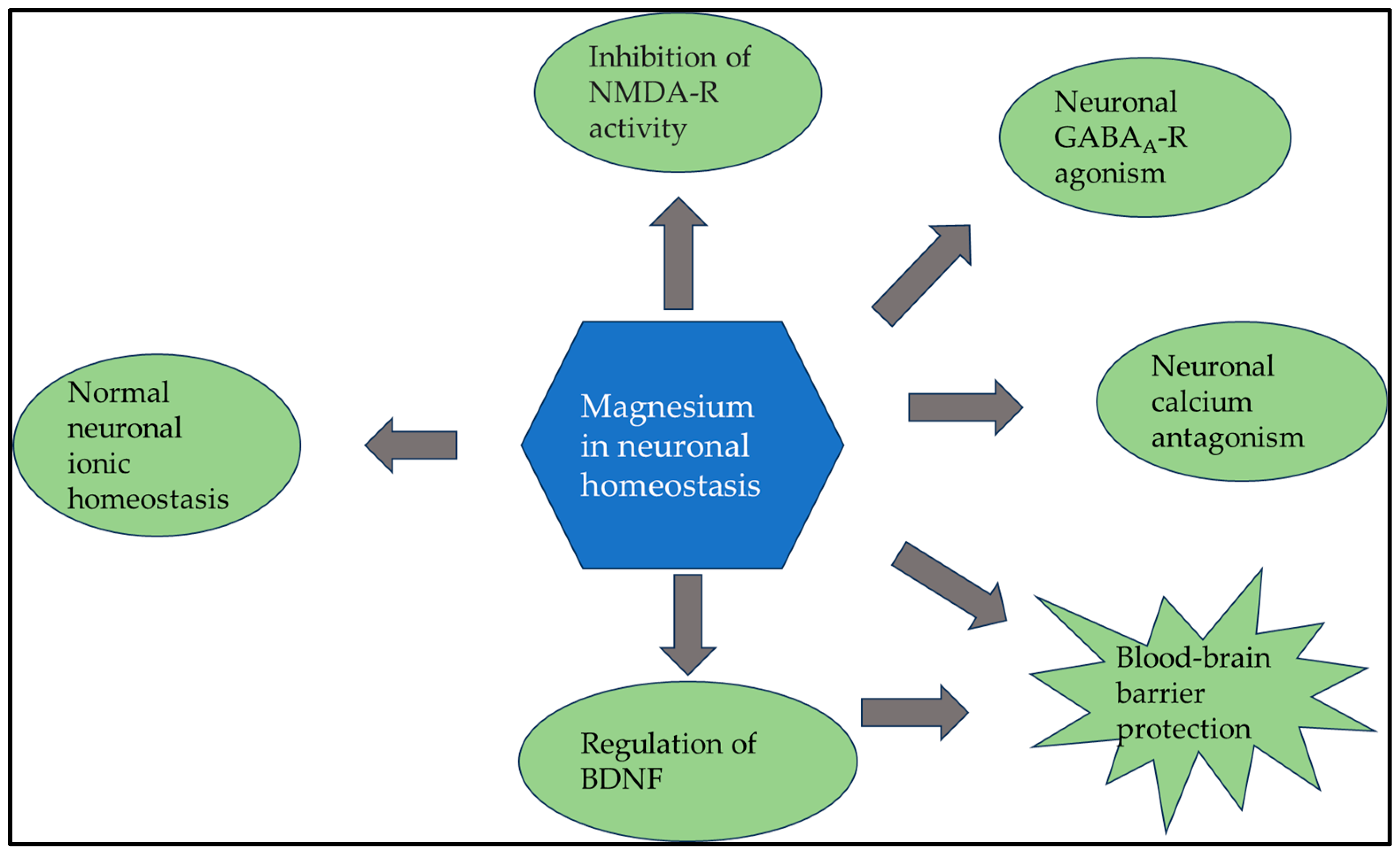
9. Hypomagnesemia and Neuropsychiatric Diseases
10. Summary
11. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- De Baaij, J.H.; Hoenderop, J.G.; Bindels, R.J. Magnesium in man: Implications for health and disease. Physiol. Rev. 2015, 95, 1–46. [Google Scholar] [CrossRef] [PubMed]
- De Baaij, J.H.; Hoenderop, J.G.; Bindels, R.J. Regulation of magnesium balance: Lessons learned from human genetic disease. Clin. Kidney J. 2012, 5 (Suppl. S1), i15–i24. [Google Scholar] [CrossRef] [PubMed]
- Romani, A.M. Cellular magnesium homeostasis. Arch. Biochem. Biophys. 2011, 512, 1–23. [Google Scholar] [CrossRef]
- Grober, U.; Schmidt, J.; Kisters, K. Magnesium in Prevention and Therapy. Nutrients 2015, 7, 8199–8226. [Google Scholar] [CrossRef] [PubMed]
- Jahnen-Dechent, W.; Ketteler, M. Magnesium basics. Clin. Kidney J. 2012, 5 (Suppl. S1), i3–i14. [Google Scholar] [CrossRef]
- Fülöp, T. Hypomagnesemia. 2022. Available online: https://emedicine.medscape.com/article/2038394-overview?form=fpf#a5 (accessed on 2 November 2023).
- Whang, R.; Hampton, E.M.; Whang, D.D. Magnesium homeostasis and clinical disorders of magnesium deficiency. Ann. Pharmacother. 1994, 28, 220–226. [Google Scholar] [CrossRef]
- Pitzer Mutchler, A.; Huynh, L.; Patel, R.; Lam, T.; Bain, D.; Jamison, S.; Kirabo, A.; Ray, E.C. The role of dietary magnesium deficiency in inflammatory hypertension. Front. Physiol. 2023, 14, 1167904. [Google Scholar] [CrossRef] [PubMed]
- Fang, X.; Wang, K.; Han, D.; He, X.; Wei, J.; Zhao, L.; Imam, M.U.; Ping, Z.; Li, Y.; Xu, Y.; et al. Dietary magnesium intake and the risk of cardiovascular disease, type 2 diabetes, and all-cause mortality: A dose-response meta-analysis of prospective cohort studies. BMC Med. 2016, 14, 210. [Google Scholar] [CrossRef]
- Lo Piano, F.; Corsonello, A.; Corica, F. Magnesium and elderly patient: The explored paths and the ones to be explored: A review. Magnes. Res. 2019, 32, 1–15. [Google Scholar]
- Felsenfeld, A.J.; Levine, B.S.; Rodriguez, M. Pathophysiology of Calcium, Phosphorus, and Magnesium Dysregulation in Chronic Kidney Disease. Semin. Dial. 2015, 28, 564–577. [Google Scholar] [CrossRef]
- Yamaguchi, H.; Shimada, H.; Yoshita, K.; Tsubata, Y.; Ikarashi, K.; Morioka, T.; Saito, N.; Sakai, S.; Narita, I. Severe hypermagnesemia induced by magnesium oxide ingestion: A case series. CEN Case Rep. 2019, 8, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Aal-Hamad, A.H.; Al-Alawi, A.M.; Kashoub, M.S.; Falhammar, H. Hypermagnesemia in Clinical Practice. Medicina 2023, 59, 1190. [Google Scholar] [CrossRef]
- Templier, M.; Paré, G. Transparency in literature reviews: An assessment of reporting practices across review types and genres in top IS journals. Eur. J. Inf. Syst. 2017, 27, 503–550. [Google Scholar] [CrossRef]
- Guy Paré, S.K. Methods for Literature Reviews. In Handbook of eHealth Evaluation: An Evidence-Based Approach; Lau, F.K.C., Ed.; University of Victoria: Victoria, BC, Canada, 2017; pp. 157–179. [Google Scholar]
- Kao, W.H.; Folsom, A.R.; Nieto, F.J.; Mo, J.P.; Watson, R.L.; Brancati, F.L. Serum and dietary magnesium and the risk for type 2 diabetes mellitus: The Atherosclerosis Risk in Communities Study. Arch. Intern. Med. 1999, 159, 2151–2159. [Google Scholar] [CrossRef] [PubMed]
- Kuppusamy, S.; Dhanasinghu, R.; Sakthivadivel, V.; Kaliappan, A.; Gaur, A.; Balan, Y.; Tadi, L.J.; Sundaramurthy, R. Association of Serum Magnesium with Insulin Indices in Patients with Type 2 Diabetes Mellitus. Maedica 2022, 17, 596–601. [Google Scholar]
- Simental-Mendia, L.E.; Sahebkar, A.; Rodriguez-Moran, M.; Guerrero-Romero, F. A systematic review and meta-analysis of randomized controlled trials on the effects of magnesium supplementation on insulin sensitivity and glucose control. Pharmacol. Res. 2016, 111, 272–282. [Google Scholar] [CrossRef]
- Orchard, T.J. Magnesium and type 2 diabetes mellitus. Arch. Intern. Med. 1999, 159, 2119–2120. [Google Scholar] [CrossRef]
- McNair, P.; Christensen, M.S.; Christiansen, C.; Madsbad, S.; Transbol, I. Renal hypomagnesaemia in human diabetes mellitus: Its relation to glucose homeostasis. Eur. J. Clin. Investig. 1982, 12, 81–85. [Google Scholar] [CrossRef]
- Saris, N.E.L.; Mervaala, E.; Karppanen, H.; Khawaja, J.A.; Lewenstam, A. Magnesium: An update on physiological, clinical and analytical aspects. Clin. Chim. Acta 2000, 294, 1–26. [Google Scholar] [CrossRef]
- Barbagallo, M. Role of magnesium in insulin action, diabetes and cardio-metabolic syndrome X. Mol. Asp. Med. 2003, 24, 39–52. [Google Scholar] [CrossRef]
- Hosseini Dastgerdi, A.; Rad, M.G.; Soltani, N. The Therapeutic Effects of Magnesium in Insulin Secretion and Insulin Resistance. Adv. Biomed. Res. 2022, 11, 54. [Google Scholar]
- Li, H.J.; Groden, C.; Hoenig, M.P.; Ray, E.C.; Ferreira, C.R.; Gahl, W.; Novacic, D. Case report: Extreme coronary calcifications and hypomagnesemia in a patient with a 17q12 deletion involving HNF1B. BMC Nephrol. 2019, 20, 353. [Google Scholar] [CrossRef]
- Petho, A.G.; Tapolyai, M.; Browne, M.; Fulop, T. Hypomagnesemia as a Risk Factor and Accelerator for Vascular Aging in Diabetes Mellitus and Chronic Kidney Disease. Metabolites 2023, 13, 306. [Google Scholar] [CrossRef]
- Severino, P.; Netti, L.; Mariani, M.V.; Maraone, A.; D’Amato, A.; Scarpati, R.; Infusino, F.; Pucci, M.; Lavalle, C.; Maestrini, V. Prevention of Cardiovascular Disease: Screening for Magnesium Deficiency. Cardiol. Res. Pract. 2019, 2019, 4874921. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Dudley, S.C., Jr. Beyond Ion Homeostasis: Hypomagnesemia, Transient Receptor Potential Melastatin Channel 7, Mitochondrial Function, and Inflammation. Nutrients 2023, 15, 3920. [Google Scholar] [CrossRef]
- Voultsos, P.; Bazmpani, M.A.; Papanastasiou, C.A.; Papadopoulos, C.E.; Efthimiadis, G.; Karvounis, H.; Kalogeropoulos, A.P.; Karamitsos, T.D. Magnesium Disorders and Prognosis in Heart Failure: A Systematic Review. Cardiol. Rev. 2022, 30, 281–285. [Google Scholar] [CrossRef] [PubMed]
- Zaslow, S.J.; Oliveira-Paula, G.H.; Chen, W. Magnesium and Vascular Calcification in Chronic Kidney Disease: Current Insights. Int. J. Mol. Sci. 2024, 25, 1155. [Google Scholar] [CrossRef]
- Sakaguchi, Y.; Hamano, T.; Obi, Y.; Monden, C.; Oka, T.; Yamaguchi, S.; Matsui, I.; Hashimoto, N.; Matsumoto, A.; Shimada, K.; et al. A Randomized Trial of Magnesium Oxide and Oral Carbon Adsorbent for Coronary Artery Calcification in Predialysis CKD. J. Am. Soc. Nephrol. 2019, 30, 1073–1085. [Google Scholar] [CrossRef]
- Sakaguchi, Y. The emerging role of magnesium in CKD. Clin. Exp. Nephrol. 2022, 26, 379–384. [Google Scholar] [CrossRef]
- Haury, V.G. Blood serum magnesium in bronchial asthma and its treatment by the administration of magnesium sulfate. J. Lab. Clin.Med. 1940, 26, 340–344. [Google Scholar]
- Brunner, E.H.; Delabroise, A.M.; Haddad, Z.H. Effect of parenteral magnesium on pulmonary function, plasma cAMP, and histamine in bronchial asthma. J. Asthma 1985, 22, 3–11. [Google Scholar] [CrossRef]
- Rolla, G.; Bucca, C.; Arossa, W.; Bugiani, M. Magnesium attenuates methacholine-induced bronchoconstriction in asthmatics. Magnesium 1987, 6, 201–204. [Google Scholar]
- Chande, V.T.; Skoner, D.P. A trial of nebulized magnesium sulfate to reverse bronchospasm in asthmatic patients. Ann. Emerg. Med. 1992, 21, 1111–1115. [Google Scholar] [CrossRef]
- Bernstein, W.K.; Khastgir, T.; Khastgir, A.; Hernandez, E.; Miller, J.; Schonfeld, S.A.; Nissim, J.E.; Chernow, B. Lack of effectiveness of magnesium in chronic stable asthma. A prospective, randomized, double-blind, placebo-controlled, crossover trial in normal subjects and in patients with chronic stable asthma. Arch. Intern. Med. 1995, 155, 271–276. [Google Scholar] [CrossRef]
- Goodacre, S.; Cohen, J.; Bradburn, M.; Gray, A.; Benger, J.; Coats, T.; 3Mg Research Team. Intravenous or nebulised magnesium sulphate versus standard therapy for severe acute asthma (3Mg trial): A double-blind, randomised controlled trial. Lancet Respir. Med. 2013, 1, 293–300. [Google Scholar] [CrossRef]
- Zaidan, M.F.; Ameredes, B.T.; Calhoun, W.J. Management of Acute Asthma in Adults in 2020. JAMA 2020, 323, 563–564. [Google Scholar] [CrossRef]
- Graff, D.M.; Stevenson, M.D.; Berkenbosch, J.W. Safety of prolonged magnesium sulfate infusions during treatment for severe pediatric status asthmaticus. Pediatr. Pulmonol. 2019, 54, 1941–1947. [Google Scholar] [CrossRef] [PubMed]
- Ozdemir, A.; Dogruel, D. Efficacy of Magnesium Sulfate Treatment in Children with Acute Asthma. Med. Princ. Pract. 2020, 29, 292–298. [Google Scholar] [CrossRef] [PubMed]
- Kapuscinski, C.A.; Stauber, S.D.; Hutchinson, D.J. Escalation in Therapy Based on Intravenous Magnesium Sulfate Dosing in Pediatric Patients With Asthma Exacerbations. J. Pediatr. Pharmacol. Ther. 2020, 25, 314–319. [Google Scholar] [CrossRef] [PubMed]
- Cheng, W.T.; Hon, K.L.; Chan, R.W.Y.; Chan, L.C.N.; Wong, W.; Cheung, H.M.; Qian, S.Y. Outcome of status asthmaticus at a pediatric intensive care unit in Hong Kong. Clin. Respir. J. 2020, 14, 462–470. [Google Scholar] [CrossRef] [PubMed]
- Van Weelden, M.; van Ewijk, B.E.; Plotz, F.B. Intravenous magnesium sulphate in children with acute wheeze: A nationwide survey. J. Asthma 2021, 58, 1444–1450. [Google Scholar] [CrossRef] [PubMed]
- Schuh, S.; Sweeney, J.; Rumantir, M.; Coates, A.L.; Willan, A.R.; Stephens, D.; Atenafu, E.G.; Finkelstein, Y.; Thompson, G.; Zemek, R.; et al. Effect of Nebulized Magnesium vs Placebo Added to Albuterol on Hospitalization Among Children With Refractory Acute Asthma Treated in the Emergency Department: A Randomized Clinical Trial. JAMA 2020, 324, 2038–2047. [Google Scholar] [CrossRef]
- Pourdowlat, G.; Mousavinasab, S.R.; Farzanegan, B.; Kashefizadeh, A.; Meybodi, Z.A.; Jafarzadeh, M.; Baniasadi, S. Evaluation of the efficacy and safety of inhaled magnesium sulphate in combination with standard treatment in patients with moderate or severe COVID-19: A structured summary of a study protocol for a randomised controlled trial. Trials 2021, 22, 60. [Google Scholar] [CrossRef]
- Jia, L.; Wei, Z.; Zhang, H.; Wang, J.; Jia, R.; Zhou, M.; Li, X.; Zhang, H.; Chen, X.; Yu, Z.; et al. An interpretable machine learning model based on a quick pre-screening system enables accurate deterioration risk prediction for COVID-19. Sci. Rep. 2021, 11, 23127. [Google Scholar] [CrossRef] [PubMed]
- Beigmohammadi, M.T.; Bitarafan, S.; Abdollahi, A.; Amoozadeh, L.; Salahshour, F.; Mahmoodi Ali Abadi, M.; Soltani, D.; Motallebnejad, Z.A. The association between serum levels of micronutrients and the severity of disease in patients with COVID-19. Nutrition 2021, 91–92, 111400. [Google Scholar] [CrossRef]
- Iotti, S.; Wolf, F.; Mazur, A.; Maier, J.A. The COVID-19 pandemic: Is there a role for magnesium? Hypotheses and perspectives. Magnes. Res. 2020, 33, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Mathew, R.; Altura, B.M. The role of magnesium in lung diseases: Asthma, allergy and pulmonary hypertension. Magnes. Trace Elem. 1991, 10, 220–228. [Google Scholar] [PubMed]
- McLean, R.M. Magnesium and its therapeutic uses: A review. Am. J. Med. 1994, 96, 63–76. [Google Scholar] [CrossRef]
- Berthon, B.S.; Wood, L.G. Nutrition and respiratory health—feature review. Nutrients 2015, 7, 1618–1643. [Google Scholar] [CrossRef]
- Dedhia, H.V.; Banks, D.E. Pulmonary response to hyperoxia: Effects of magnesium. Environ. Health Perspect. 1994, 102 (Suppl. S10), 101–105. [Google Scholar]
- Jiang, P.; Lv, Q.; Lai, T.; Xu, F. Does Hypomagnesemia Impact on the Outcome of Patients Admitted to the Intensive Care Unit? A Systematic Review and Meta-Analysis. Shock 2017, 47, 288–295. [Google Scholar] [CrossRef]
- Mazur, A.; Maier, J.A.; Rock, E.; Gueux, E.; Nowacki, W.; Rayssiguier, Y. Magnesium and the inflammatory response: Potential physiopathological implications. Arch. Biochem. Biophys. 2007, 458, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Bussiere, F.I.; Gueux, E.; Rock, E.; Girardeau, J.P.; Tridon, A.; Mazur, A.; Rayssiguier, Y. Increased phagocytosis and production of reactive oxygen species by neutrophils during magnesium deficiency in rats and inhibition by high magnesium concentration. Br. J. Nutr. 2002, 87, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Dominguez, L.J.; Veronese, N.; Guerrero-Romero, F.; Barbagallo, M. Magnesium in Infectious Diseases in Older People. Nutrients 2021, 13, 180. [Google Scholar] [CrossRef]
- Feske, S.; Skolnik, E.Y.; Prakriya, M. Ion channels and transporters in lymphocyte function and immunity. Nat. Rev. Immunol. 2012, 12, 532–547. [Google Scholar] [CrossRef] [PubMed]
- Schmitz, C.; Perraud, A.L.; Johnson, C.O.; Inabe, K.; Smith, M.K.; Penner, R.; Kurosaki, T.; Fleig, A.; Scharenberg, A.M. Regulation of vertebrate cellular Mg2+ homeostasis by TRPM7. Cell 2003, 114, 191–200. [Google Scholar] [CrossRef]
- Jin, J.; Desai, B.N.; Navarro, B.; Donovan, A.; Andrews, N.C.; Clapham, D.E. Deletion of Trpm7 disrupts embryonic development and thymopoiesis without altering Mg2+ homeostasis. Science 2008, 322, 756–760. [Google Scholar] [CrossRef]
- Bantug, G.R.; Galluzzi, L.; Kroemer, G.; Hess, C. The spectrum of T cell metabolism in health and disease. Nat. Rev. Immunol. 2018, 18, 19–34. [Google Scholar] [CrossRef]
- Hogg, N.; Patzak, I.; Willenbrock, F. The insider’s guide to leukocyte integrin signalling and function. Nat. Rev. Immunol. 2011, 11, 416–426. [Google Scholar] [CrossRef]
- Trapani, V.; Rosanoff, A.; Baniasadi, S.; Barbagallo, M.; Castiglioni, S.; Guerrero-Romero, F.; Iotti, S.; Mazur, A.; Micke, O.; Pourdowlat, G.; et al. The relevance of magnesium homeostasis in COVID-19. Eur. J. Nutr. 2022, 61, 625–636. [Google Scholar] [CrossRef]
- Al-Fartusie, F.S.; Kader, S.I.; Mohammed, S.J.; Farhan, M.N.; Mahmood, F.M.; Algaber, A.A. A comparative study of serum Zn, Cu, Mg, Mn, Cr, and Fe levels and their association with the vulnerability of Iraqi COVID-19 patients. J. Trace Elem. Med. Biol. 2023, 79, 127242. [Google Scholar] [CrossRef]
- Kanellopoulou, C.; George, A.B.; Masutani, E.; Cannons, J.L.; Ravell, J.C.; Yamamoto, T.N.; Smelkinson, M.G.; Jiang, P.D.; Matsuda-Lennikov, M.; Reilley, J.; et al. Mg2+ regulation of kinase signaling and immune function. J. Exp. Med. 2019, 216, 1828–1842. [Google Scholar] [CrossRef] [PubMed]
- Arablou, T.; Aryaeian, N.; Djalali, M.; Shahram, F.; Rasouli, L. Association between dietary intake of some antioxidant micronutrients with some inflammatory and antioxidant markers in active Rheumatoid Arthritis patients. Int. J. Vitam. Nutr. Res. 2019, 89, 238–245. [Google Scholar] [CrossRef]
- Lee, B.; Song, Y.S.; Rhodes, C.; Goh, T.S.; Roh, J.S.; Jeong, H.; Park, J.; Lee, H.N.; Lee, S.G.; Kim, S.; et al. Protein phosphatase magnesium-dependent 1A induces inflammation in rheumatoid arthritis. Biochem. Biophys. Res. Commun. 2020, 522, 731–735. [Google Scholar] [CrossRef] [PubMed]
- Luo, Z.; Chen, S.; Chen, X. CircMAPK9 promotes the progression of fibroblast-like synoviocytes in rheumatoid arthritis via the miR-140-3p/PPM1A axis. J. Orthop. Surg. Res. 2021, 16, 395. [Google Scholar] [CrossRef]
- Hu, C.; Zhu, F.; Liu, L.; Zhang, M.; Chen, G. Relationship between dietary magnesium intake and rheumatoid arthritis in US women: A cross-sectional study. BMJ Open 2020, 10, e039640. [Google Scholar] [CrossRef]
- Yang, W.; Lian, X.; Chen, H. The association of serum magnesium with infection in new-onset systemic lupus erythematosus patients. Lupus 2023, 32, 380–387. [Google Scholar] [CrossRef]
- Luo, Y.; Zeng, H.; Ye, Y.; Yu, G.; Song, C.; Liu, S.; Chen, X.; Jiang, Y.; Duan, H.; Li, Y.; et al. Associations of metal profiles in blood with thyroiditis: A cross-sectional study. Environ. Sci. Pollut. Res. Int. 2023, 30, 21072–21080. [Google Scholar] [CrossRef]
- Zhou, Q.; Xue, S.; Zhang, L.; Chen, G. Trace elements and the thyroid. Front. Endocrinol. 2022, 13, 904889. [Google Scholar] [CrossRef]
- Khan, S.Z.A.; Lungba, R.M.; Ajibawo-Aganbi, U.; Veliginti, S.; Perez Bastidas, M.V.; Saleem, S.; Cancarevic, I. Minerals: An Untapped Remedy for Autoimmune Hypothyroidism? Cureus 2020, 12, e11008. [Google Scholar] [CrossRef]
- Nasulewicz, A.; Wietrzyk, J.; Wolf, F.I.; Dzimira, S.; Madej, J.; Maier, J.A.; Rayssiguier, Y.; Mazur, A.; Opolski, A. Magnesium deficiency inhibits primary tumor growth but favors metastasis in mice. Biochim. Biophys. Acta 2004, 1739, 26–32. [Google Scholar] [CrossRef]
- Kasprzak, K.S.; Diwan, B.A.; Rice, J.M. Iron accelerates while magnesium inhibits nickel-induced carcinogenesis in the rat kidney. Toxicology 1994, 90, 129–140. [Google Scholar] [CrossRef]
- Patiroglu, T.; Sahin, G.; Kontas, O.; Uzum, K.; Saraymen, R. Protective effect of magnesium supplementation on experimental 3-methyl cholanthrene-induced fibrosarcoma and changes in tissue magnesium distribution during carcinogenesis in rats. Biol. Trace Elem. Res. 1997, 56, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Colotta, F.; Allavena, P.; Sica, A.; Garlanda, C.; Mantovani, A. Cancer-related inflammation, the seventh hallmark of cancer: Links to genetic instability. Carcinogenesis 2009, 30, 1073–1081. [Google Scholar] [CrossRef] [PubMed]
- Royuela, M.; Rodriguez-Berriguete, G.; Fraile, B.; Paniagua, R. TNF-alpha/IL-1/NF-kappaB transduction pathway in human cancer prostate. Histol. Histopathol. 2008, 23, 1279–1290. [Google Scholar] [PubMed]
- Bagheri, A.; Naghshi, S.; Sadeghi, O.; Larijani, B.; Esmaillzadeh, A. Total, Dietary, and Supplemental Magnesium Intakes and Risk of All-Cause, Cardiovascular, and Cancer Mortality: A Systematic Review and Dose-Response Meta-Analysis of Prospective Cohort Studies. Adv. Nutr. 2021, 12, 1196–1210. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Chinnathambi, S.; Kumar, M.; Pandian, G.N. Food Intake and Colorectal Cancer. Nutr. Cancer 2023, 75, 1710–1742. [Google Scholar] [CrossRef] [PubMed]
- Wark, P.A.; Lau, R.; Norat, T.; Kampman, E. Magnesium intake and colorectal tumor risk: A case-control study and meta-analysis. Am. J. Clin. Nutr. 2012, 96, 622–631. [Google Scholar] [CrossRef]
- Zhong, G.C.; Peng, Y.; Wang, K.; Wan, L.; Wu, Y.Q.; Hao, F.B.; Hu, J.J.; Gu, H.T. Magnesium intake and primary liver cancer incidence and mortality in the Prostate, Lung, Colorectal and Ovarian Cancer Screening Trial. Int. J. Cancer 2020, 147, 1577–1586. [Google Scholar] [CrossRef]
- Li, H.; Feng, X.; Li, H.; Ma, S.; Song, W.; Yang, B.; Jiang, T.; Yang, C. The Supplement of Magnesium Element to Inhibit Colorectal Tumor Cells. Biol. Trace Elem. Res. 2023, 201, 2895–2903. [Google Scholar] [CrossRef]
- Yu, Y.C.; Paragomi, P.; Wang, R.; Liang, F.; Luu, H.N.; Behari, J.; Yuan, J.M. High serum magnesium is associated with lower risk of hepatocellular carcinoma among patients with nonalcoholic fatty liver disease. Cancer 2023, 129, 2341–2347. [Google Scholar] [CrossRef]
- Shah, S.C.; Zhu, X.; Dai, Q.; Peek, R.M.; Shrubsole, M.J. Magnesium intake is associated with a reduced risk of incident liver cancer, based on an analysis of the NIH-American Association of Retired Persons (NIH-AARP) Diet and Health Study prospective cohort. Am. J. Clin. Nutr. 2021, 113, 630–638. [Google Scholar] [CrossRef]
- Mahabir, S.; Wei, Q.; Barrera, S.L.; Dong, Y.Q.; Etzel, C.J.; Spitz, M.R.; Forman, M.R. Dietary magnesium and DNA repair capacity as risk factors for lung cancer. Carcinogenesis 2008, 29, 949–956. [Google Scholar] [CrossRef]
- Cho, S.; Chae, J.S.; Shin, H.; Shin, Y.; Kim, Y.; Kil, E.J.; Byun, H.S.; Cho, S.H.; Park, S.; Lee, S.; et al. Enhanced Anticancer Effect of Adding Magnesium to Vitamin C Therapy: Inhibition of Hormetic Response by SVCT-2 Activation. Transl. Oncol. 2020, 13, 401–409. [Google Scholar] [CrossRef]
- Santos, J.M.; Hussain, F. Magnesium Chloride increases apoptosis and decreases prostate cancer cells migration. Funct. Foods Health Dis. 2018, 8, 62–78. [Google Scholar] [CrossRef]
- Weisleder, P.; Tobin, J.A.; Kerrigan, J.F., 3rd; Bodensteiner, J.B. Hypomagnesemic seizures: Case report and presumed pathophysiology. J. Child Neurol. 2002, 17, 59–61. [Google Scholar] [CrossRef] [PubMed]
- Espay, A.J. Neurologic complications of electrolyte disturbances and acid-base balance. Handb. Clin. Neurol. 2014, 119, 365–382. [Google Scholar] [PubMed]
- Pickering, G.; Mazur, A.; Trousselard, M.; Bienkowski, P.; Yaltsewa, N.; Amessou, M.; Noah, L.; Pouteau, E. Magnesium Status and Stress: The Vicious Circle Concept Revisited. Nutrients 2020, 12, 3672. [Google Scholar] [CrossRef] [PubMed]
- Yamanaka, R.; Shindo, Y.; Oka, K. Magnesium Is a Key Player in Neuronal Maturation and Neuropathology. Int. J. Mol. Sci. 2019, 20, 3439. [Google Scholar] [CrossRef] [PubMed]
- Yamanaka, R.; Shindo, Y.; Hotta, K.; Suzuki, K.; Oka, K. GABA-Induced Intracellular Mg2+ Mobilization Integrates and Coordinates Cellular Information Processing for the Maturation of Neural Networks. Curr. Biol. 2018, 28, 3984–3991.e5. [Google Scholar] [CrossRef] [PubMed]
- Romeo, V.; Cazzaniga, A.; Maier, J.A.M. Magnesium and the blood-brain barrier in vitro: Effects on permeability and magnesium transport. Magnes. Res. 2019, 32, 16–24. [Google Scholar]
- Durlach, J.; Bac, P.; Bara, M.; Guiet-Bara, A. Physiopathology of symptomatic and latent forms of central nervous hyperexcitability due to magnesium deficiency: A current general scheme. Magnes. Res. 2000, 13, 293–302. [Google Scholar]
- Baj, J.; Forma, A.; Sitarz, E.; Karakula, K.; Flieger, W.; Sitarz, M.; Grochowski, C.; Maciejewski, R.; Karakula-Juchnowicz, H. Beyond the Mind-Serum Trace Element Levels in Schizophrenic Patients: A Systematic Review. Int. J. Mol. Sci. 2020, 21, 9566. [Google Scholar] [CrossRef]
- Goto, Y.; Nakamura, M.; Abe, S.; Kato, M.; Fukui, M. Physiological correlates of abnormal behaviors in magnesium-deficient rats. Epilepsy Res. 1993, 15, 81–89. [Google Scholar] [CrossRef] [PubMed]
- Achalia, R.; Korhale, D.; Lakkas, Y.; Mehta, U.M. Protracted delirium tremens and the forgotten cation: A case report. Asian J. Psychiatr. 2018, 38, 29–30. [Google Scholar] [CrossRef]
- Galland, L. Magnesium, stress and neuropsychiatric disorders. Magnes Trace Elem. 1991, 10, 287–301. [Google Scholar] [PubMed]
- Derom, M.L.; Sayon-Orea, C.; Martinez-Ortega, J.M.; Martinez-Gonzalez, M.A. Magnesium and depression: A systematic review. Nutr. Neurosci. 2013, 16, 191–206. [Google Scholar] [CrossRef]
- Abbasi, B.; Kimiagar, M.; Sadeghniiat, K.; Shirazi, M.M.; Hedayati, M.; Rashidkhani, B. The effect of magnesium supplementation on primary insomnia in elderly: A double-blind placebo-controlled clinical trial. J. Res. Med. Sci. 2012, 17, 1161–1169. [Google Scholar]
- Imada, Y.; Yoshioka, S.; Ueda, T.; Katayama, S.; Kuno, Y.; Kawahara, R. Relationships between serum magnesium levels and clinical background factors in patients with mood disorders. Psychiatry Clin. Neurosci. 2002, 56, 509–514. [Google Scholar] [CrossRef]
- Glick, J.L. Dementias: The role of magnesium deficiency and an hypothesis concerning the pathogenesis of Alzheimer’s disease. Med. Hypotheses 1990, 31, 211–225. [Google Scholar] [CrossRef]
- Lu, Z.; He, R.; Zhang, Y.; Li, B.; Li, F.; Fu, Y.; Rong, S. Relationship between Whole-Blood Magnesium and Cognitive Performance among Chinese Adults. Nutrients 2023, 15, 2706. [Google Scholar] [CrossRef] [PubMed]
- Maier, J.A.M.; Locatelli, L.; Fedele, G.; Cazzaniga, A.; Mazur, A. Magnesium and the Brain: A Focus on Neuroinflammation and Neurodegeneration. Int. J. Mol. Sci. 2022, 24, 223. [Google Scholar] [CrossRef]
- Barbagallo, M.; Belvedere, M.; Di Bella, G.; Dominguez, L.J. Altered ionized magnesium levels in mild-to-moderate Alzheimer’s disease. Magnes. Res. 2011, 24, S115–S121. [Google Scholar] [CrossRef]
- Vural, H.; Demirin, H.; Kara, Y.; Eren, I.; Delibas, N. Alterations of plasma magnesium, copper, zinc, iron and selenium concentrations and some related erythrocyte antioxidant enzyme activities in patients with Alzheimer’s disease. J. Trace Elem. Med. Biol. 2010, 24, 169–173. [Google Scholar] [CrossRef] [PubMed]
- Xiong, Y.; Ruan, Y.T.; Zhao, J.; Yang, Y.W.; Chen, L.P.; Mai, Y.R.; Yu, Q.; Cao, Z.Y.; Liu, F.F.; Liao, W.; et al. Magnesium-L-threonate exhibited a neuroprotective effect against oxidative stress damage in HT22 cells and Alzheimer’s disease mouse model. World J. Psychiatry 2022, 12, 410–424. [Google Scholar] [CrossRef]
- Wang, P.; Yu, X.; Guan, P.P.; Guo, J.W.; Wang, Y.; Zhang, Y.; Zhao, H.; Wang, Z.Y. Magnesium ion influx reduces neuroinflammation in Abeta precursor protein/Presenilin 1 transgenic mice by suppressing the expression of interleukin-1beta. Cell Mol. Immunol. 2017, 14, 451–464. [Google Scholar] [CrossRef] [PubMed]
- Slutsky, I.; Abumaria, N.; Wu, L.J.; Huang, C.; Zhang, L.; Li, B.; Zhao, X.; Govindarajan, A.; Zhao, M.G.; Zhuo, M.; et al. Enhancement of learning and memory by elevating brain magnesium. Neuron 2010, 65, 165–177. [Google Scholar] [CrossRef]
- Zhou, X.; Huang, Z.; Zhang, J.; Chen, J.L.; Yao, P.W.; Mai, C.L.; Mai, J.Z.; Zhang, H.; Liu, X.G. Chronic Oral Administration of Magnesium-L-Threonate Prevents Oxaliplatin-Induced Memory and Emotional Deficits by Normalization of TNF-alpha/NF-kappaB Signaling in Rats. Neurosci. Bull. 2021, 37, 55–69. [Google Scholar] [CrossRef]
- Yang, Y.; Long, Y.; Yuan, J.; Zha, Y. U-shaped association of serum magnesium with mild cognitive impairment among hemodialysis patients: A multicenter study. Ren. Fail. 2023, 45, 2231084. [Google Scholar] [CrossRef]
- Tao, M.H.; Liu, J.; Cervantes, D. Association between magnesium intake and cognition in US older adults: National Health and Nutrition Examination Survey (NHANES) 2011 to 2014. Alzheimers Dement. 2022, 8, e12250. [Google Scholar] [CrossRef]
- Gao, X.; Sun, Y.; Huang, X.; Zhou, Y.; Zhu, H.; Li, Q.; Ma, Y. Adequate dietary magnesium intake may protect females but not males older than 55 years from cognitive impairment. Nutr. Neurosci. 2023, 27, 184–195. [Google Scholar] [CrossRef] [PubMed]
- Cenacchi, V.; Maier, J.A.; Perini, M.P. A potential protective role of magnesium in neuroCOVID. Magnes. Res. 2022, 35, 18–26. [Google Scholar] [PubMed]
- Martin de Argila de Prados, C.; Cardona, J.L.; Arguelles-Arias, F. Safe use of proton-pump inhibitors. Rev. Esp. Enferm. Dig. 2023, 115, 475–479. [Google Scholar] [CrossRef] [PubMed]
- Cheungpasitporn, W.; Thongprayoon, C.; Kittanamongkolchai, W.; Srivali, N.; Edmonds, P.J.; Ungprasert, P.; O’Corragain, O.A.; Korpaisarn, S.; Erickson, S.B. Proton pump inhibitors linked to hypomagnesemia: A systematic review and meta-analysis of observational studies. Ren. Fail. 2015, 37, 1237–1241. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
|
| Searched Keywords | Number of Publications until 1 August 2023 | First Publication in This Field |
|---|---|---|
| Magnesium and diabetes | 2880 | 1947 |
| Magnesium and cardiovascular disease | 8400 | 1946 |
| Magnesium and respiratory disease | 2052 | 1948 |
| Magnesium and the immune system | 2974 | 1951 |
| Magnesium and inflammation | 1655 | 1920 |
| Magnesium and autoimmune disease | 597 | 1956 |
| Magnesium and neurology | 1054 | 1955 |
| Magnesium and psychiatry | 492 | 1950 |
| Magnesium and cognitive function | 270 | 1967 |
| Magnesium and cancer | 5080 | 1934 |
| Magnesium and vascular calcification | 206 | 1956 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pethő, Á.G.; Fülöp, T.; Orosz, P.; Tapolyai, M. Magnesium Is a Vital Ion in the Body—It Is Time to Consider Its Supplementation on a Routine Basis. Clin. Pract. 2024, 14, 521-535. https://doi.org/10.3390/clinpract14020040
Pethő ÁG, Fülöp T, Orosz P, Tapolyai M. Magnesium Is a Vital Ion in the Body—It Is Time to Consider Its Supplementation on a Routine Basis. Clinics and Practice. 2024; 14(2):521-535. https://doi.org/10.3390/clinpract14020040
Chicago/Turabian StylePethő, Ákos Géza, Tibor Fülöp, Petronella Orosz, and Mihály Tapolyai. 2024. "Magnesium Is a Vital Ion in the Body—It Is Time to Consider Its Supplementation on a Routine Basis" Clinics and Practice 14, no. 2: 521-535. https://doi.org/10.3390/clinpract14020040
APA StylePethő, Á. G., Fülöp, T., Orosz, P., & Tapolyai, M. (2024). Magnesium Is a Vital Ion in the Body—It Is Time to Consider Its Supplementation on a Routine Basis. Clinics and Practice, 14(2), 521-535. https://doi.org/10.3390/clinpract14020040