
The Importance of Psychometric and Physical Scales for the Evaluation of the Consequences of Scars—A Literature Review

 ,
, 
Abstract
1. Introduction
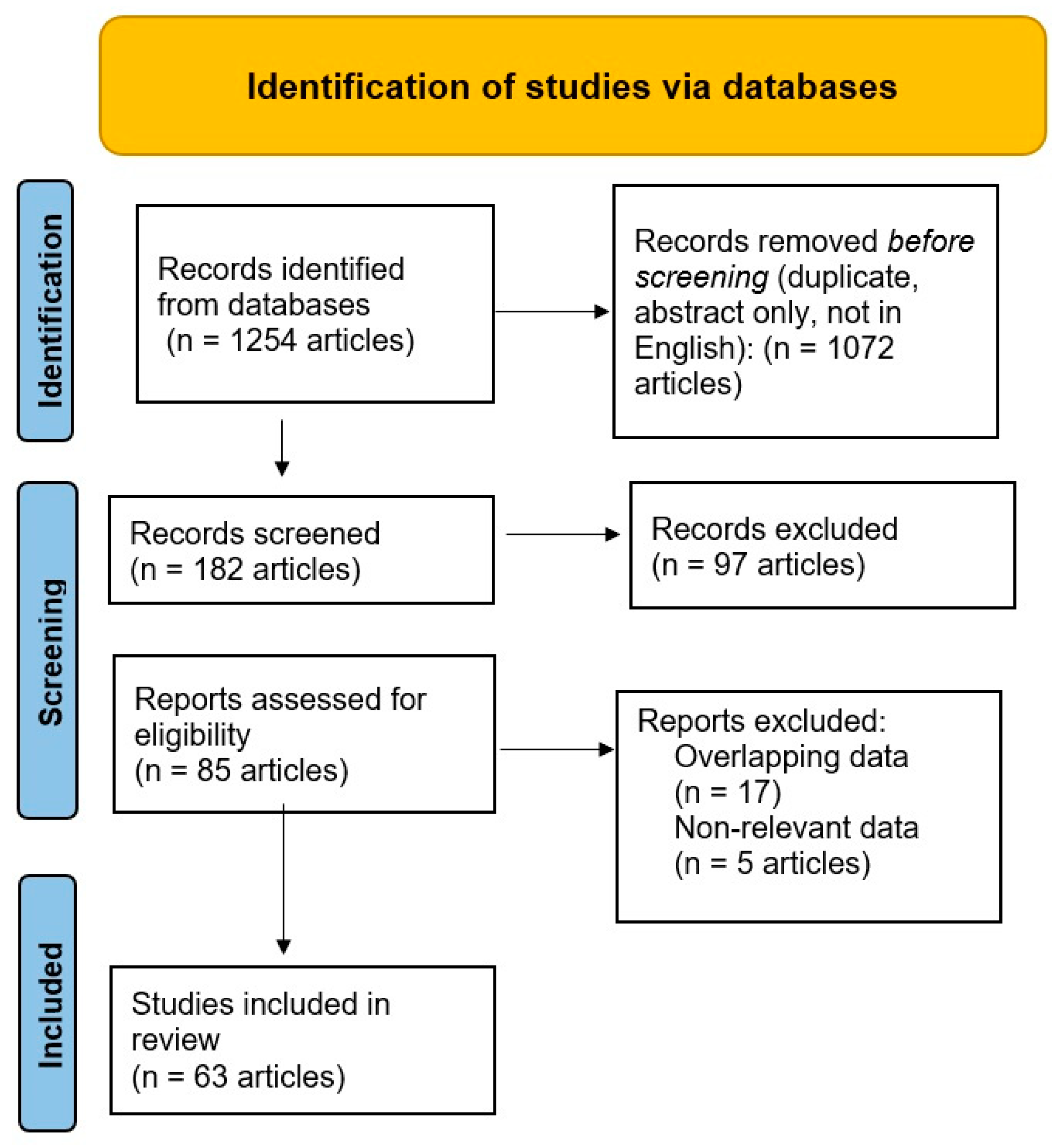
2. Methods
3. Results
3.1. Scales for Physical Assessment of Scars
3.2. Psychometric Scales for the Assessment of Scars
3.3. Scales for Physical and Psychosocial Assessment of Scars
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Coentro, J.Q.; Pugliese, E.; Hanley, G.; Raghunath, M.; Zeugolis, D.I. Current and upcoming therapies to modulate skin scarring and fibrosis. Adv. Drug Deliv. Rev. 2019, 146, 37–59. [Google Scholar] [CrossRef]
- Paşcalău, A.V.; Cheregi, C.D.; Mureşan, M.Ş.; Şandor, M.I.; Huniadi, C.A.; Nikin, Z.; Pusta, C.T.; Bodog, F.D.; Ionescu, C.; Pop, O.L. CD4+ CD25+ regulatory T-cells role in tumor microenvironment of the squamous cell carcinoma. Rom. J. Morphol. Embryol. 2021, 62, 249. [Google Scholar] [CrossRef] [PubMed]
- Burd, A.; Huang, L. Hypertrophic response and keloid diathesis: Two very different forms of scar. Plast. Reconstr. Surg. 2005, 116, 150e–157e. [Google Scholar] [CrossRef] [PubMed]
- Boer, M.; Duchnik, E.; Maleszka, R.; Marchlewicz, M. Structural and biophysical characteristics of human skin in maintaining proper epidermal barrier function. Adv. Dermatol. Allergol. Postȩpy Dermatol. I Alergol. 2016, 33, 1–5. [Google Scholar] [CrossRef]
- Sidgwick, G.P.; McGeorge, D.; Bayat, A. A comprehensive evidence-based review on the role of topicals and dressings in the management of skin scarring. Arch. Dermatol. Res. 2015, 307, 461–477. [Google Scholar] [CrossRef] [PubMed]
- Ardeshirpour, Y.; Gandjbakhche, A.H.; Najafizadeh, L. Biophotonics techniques for structural and functional imaging, in vivo. Stud. Health Technol. Inf. 2013, 11, 265–297. [Google Scholar]
- Mobley, S.R.; Sjogren, P.P. Soft tissue trauma and scar revision. Facial Plast. Surg. Clin. 2014, 22, 639–651. [Google Scholar] [CrossRef]
- Chae, J.K.; Kim, J.H.; Kim, E.J.; Park, K. Values of a patient and observer scar assessment scale to evaluate the facial skin graft scar. Ann. Dermatol. 2016, 28, 615–623. [Google Scholar] [CrossRef]
- El Kinani, M.; Duteille, F. Scar Epidemiology and Consequences. 2020 December 8. In Textbook on Scar Management: State of the Art Management and Emerging Technologies; Téot, L., Mustoe, T.A., Middelkoop, E., Gauglitz, G.G., Eds.; Springer: Cham, Switzerland, 2020; Chapter 6. [Google Scholar]
- Brown, B.C.; McKenna, S.P.; Siddhi, K.; McGrouther, D.A.; Bayat, A. The hidden cost of skin scars: Quality of life after skin scarring. J. Plast. Reconstr. Aesthetic Surg. 2008, 61, 1049–1058. [Google Scholar] [CrossRef]
- Mekereș, F.; Voiță, G.F.; Mekereș, G.M.; Bodog, F.D. Psychosocial impact of scars in evaluation of aesthetic prejudice. Rom. J. Leg. Med. 2017, 25, 435–438. [Google Scholar]
- Chen, C.C.; Chen, S.P.; Lyu, S.Y.; Hsu, C.H. Application of Auriculotherapy for Post-Burn Scar Syndrome in Young Adults with Major Burns. J. Acupunct. Meridian Stud. 2021, 31, 127–136. [Google Scholar] [CrossRef]
- Russo, M.; Bolcato, M.; Sabadin, V.; Aprile, A. The medico-legal assessment of aesthetic damage. A correlation analysis between experts and an operative proposal. Leg. Med. 2019, 40, 47–53. [Google Scholar] [CrossRef]
- Mekereş, F.; Nicoară, N.; Roşu, B.; Mekereş, G.M.; Buhaş, C.L. The psychological impact of scars in forensic practice. Rom. J. Forensic. Sci. 2017, 18, 2552–2554. [Google Scholar]
- Franchitto, N.; Telmon, N.; Grolleau, J.L.; Gavarri, L.; Laguerre, J.; Rougé, D. Medicolegal evaluation of aesthetic impairment: Particularities of post-burn scars. Burns 2009, 35, 642–649. [Google Scholar] [CrossRef] [PubMed]
- Voiță-Mekeres, F.; Buhaș, C.L.; Mekeres, G.M.; Tudoran, C.; Racovita, M.; Faur, C.I.; Tudoran, M.; Abu-Awwad, A.; Voiță, N.C.; Maghiar, T.A. Mekeres’ Psychosocial Internalization Scale: A Scale for the Evaluation of Aesthetic Prejudice in Victims of Accidents and Violence. Healthcare 2021, 9, 1440. [Google Scholar] [CrossRef] [PubMed]
- Maskell, J.; Newcombe, P.; Martin, G.; Kimble, R. Psychological and psychosocial functioning of children with burn scarring using cosmetic camouflage: A multi-centre prospective randomised controlled trial. Burns 2014, 40, 135–149. [Google Scholar] [CrossRef]
- Wilcox, S. Multidimensional scale of perceived social support. Psychol. Trauma Theory Res. Pract. Policy 2010, 2, 175–182. [Google Scholar] [CrossRef]
- Van Loey, N.E.; Van Son, M.J. Psychopathology and psychological problems in patients with burn scars. Am. J. Clin. Dermatol. 2003, 4, 245–272. [Google Scholar] [CrossRef] [PubMed]
- Johnson, M.D.; Galambos, N.L.; Krahn, H.J. Vulnerability, scar, or reciprocal risk? Temporal ordering of self-esteem and depressive symptoms over 25 years. Longitud. Life Course Stud. 2016, 26, 304–319. [Google Scholar] [CrossRef]
- Lari, A.; Alherz, M.; Hussain, S.; Burhamah, W.; Alabbad, F.; Jarragh, A.; Lari, A. The Importance of Scar Cosmesis across the Surgical Specialties: Factors, Perceptions, and Predispositions. Plast. Reconstr. Surg. Glob. Open 2022, 10, e4219. [Google Scholar] [CrossRef]
- Mekeres, G.M.; Voiţă-Mekereş, F.; Tudoran, C.; Buhaş, C.L.; Tudoran, M.; Racoviţă, M.; Voiţă, N.C.; Pop, N.O.; Marian, M. Predictors for Estimating Scars’ Internalization in Victims with Post-Traumatic Scars versus Patients with Postsurgical Scars. InHealthcare 2022, 16, 550. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 29, n71. [Google Scholar] [CrossRef] [PubMed]
- Fearmonti, R.; Bond, J.; Erdmann, D.; Levinson, H. A review of scar scales and scar measuring devices. Eplasty 2010, 10, e43. [Google Scholar] [PubMed]
- Singer, A.J.; Arora, B.; Dagum, A.; Valentine, S.; Hollander, J.E. Development and validation of a novel scar evaluation scale. Plast. Reconstr. Surg. 2007, 120, 1892–1897. [Google Scholar] [CrossRef] [PubMed]
- Vercelli, S.; Ferriero, G.; Sartorio, F.; Cisari, C.; Bravini, E. Clinimetric properties and clinical utility in rehabilitation of postsurgical scar rating scales: A systematic review. Int. J. Rehabil. Res. 2015, 38, 279–286. [Google Scholar] [CrossRef]
- Moran, B.; Humphrey, S.; Seal, A.; Berkowitz, J.; Zloty, D. Photographic assessment of postsurgical facial scars epidermally sutured with rapidly absorbable polyglactin 910 or nylon: A randomized clinical trial. J. Am. Acad. Dermatol. 2020, 83, 1395–1399. [Google Scholar] [CrossRef]
- Draaijers, L.J.; Tempelman, F.R.; Botman, Y.A.; Tuinebreijer, W.E.; Middelkoop, E.; Kreis, R.W.; Van Zuijlen, P.P. The patient and observer scar assessment scale: A reliable and feasible tool for scar evaluation. Plast. Reconstr. Surg. 2004, 113, 1960–1965. [Google Scholar] [CrossRef]
- Roques, C.; Teot, L. A critical analysis of measurements used to assess and manage scars. Int. J. Low. Extrem. Wounds 2007, 6, 249–253. [Google Scholar] [CrossRef]
- Park, J.W.; Koh, Y.G.; Shin, S.H.; Choi, Y.J.; Kim, W.S.; Yoo, H.H.; Lee, J.O.; Jang, Y.N.; Kim, J.; Li, K.; et al. Review of Scar Assessment Scales. Med. Lasers Eng. Basic Res. Clin. Appl. 2022, 30, 7. [Google Scholar] [CrossRef]
- Hjellestad, M.; Strand, L.I.; Eide, G.E.; Brekke, R.; Nesheim, A.; Gjelsvik, B.E. Clinimetric properties of a translated and culturally adapted Norwegian version of the Patient and Observer Scar Assessment Scale for use in clinical practice and research. Burns 2021, 47, 953–960. [Google Scholar] [CrossRef]
- Luze, H.; Nischwitz, S.P.; Smolle, C.; Zrim, R.; Kamolz, L.P. The Use of Acellular Fish Skin Grafts in Burn Wound Management—A Systematic Review. Medicina 2022, 58, 912. [Google Scholar] [CrossRef]
- Peinemann, F.; Behrouz-Pirnia, A. Quality issues identified in systematic reviews on early laser intervention to reduce scar formation in wound healing. J. Plast. Reconstr. Aesthetic Surg. 2020, 73, 1357–1404. [Google Scholar] [CrossRef]
- Beausang, E.; Floyd, H.; Dunn, K.W.; Orton, C.I.; Ferguson, M.W. A new quantitative scale for clinical scar assessment. Plast. Reconstr. Surg. 1998, 102, 1954–1961. [Google Scholar] [CrossRef]
- Brown, B.C.; Moss, T.P.; McGrouther, D.A.; Bayat, A. Skin scar preconceptions must be challenged: Importance of self-perception in skin scarring. J. Plast. Reconstr. Aesthetic Surg. 2010, 63, 1022–1029. [Google Scholar] [CrossRef] [PubMed]
- Bae, S.H.; Bae, Y.C. Analysis of frequency of use of different scar assessment scales based on the scar condition and treatment method. Arch. Plast. Surg. 2014, 41, 111–115. [Google Scholar] [CrossRef] [PubMed]
- van der Wal, M.B.; Verhaegen, P.D.; Middelkoop, E.; van Zuijlen, P.P. A clinimetric overview of scar assessment scales. J. Burn. Care Res. 2012, 33, e79–e87. [Google Scholar] [CrossRef]
- Crowe, J.M.; Simpson, K.; Johnson, W.; Allen, J. Reliability of photographic analysis in determining change in scar appearance. J. Burn. Care Rehabil. 1998, 19, 183–186. [Google Scholar] [CrossRef] [PubMed]
- Brusselaers, N.; Pirayesh, A.; Hoeksema, H.; Verbelen, J.; Blot, S.; Monstrey, S. Burn scar assessment: A systematic review of different scar scales. J. Surg. Res. 2010, 164, e115–e123. [Google Scholar] [CrossRef]
- Yeoung, E.K.; Mann, R.; Engrav, L.H.; Goldberg, M.; Cain, V.; Costa, B.; Moore, M.; Nakamura, D.; Lee, J. Improved burn scar assessment with use of a new scar-rating scale. J. Burn. Care Rehabil. 1997, 18, 353–355. [Google Scholar] [CrossRef]
- Furtado, F.; Hochman, B.; Ferreira, L.M. Evaluating keloid recurrence after surgical excision with prospective longitudinal scar assessment scales. J. Plast. Reconstr. Aesthetic Surg. 2012, 65, e175–e181. [Google Scholar] [CrossRef]
- Sundfeld Spiga Real, D.; Salvador Bagnato, V. Surgical Treatment of Keloids in the Ear: Prospective and Randomized Study Comparing Direct Surgical Excision vs. Keloid Fillet Flap. Asian J. Res. Surg. 2022, 7, 22–23. [Google Scholar]
- Sullivan, T.A.; Smith, J.; Kermode, J.; Mclver, E.; Courtemanche, D.J. Rating the burn scar. J. Burn. Care Rehabil. 1990, 11, 256–260. [Google Scholar] [CrossRef] [PubMed]
- Baryza, M.J.; Baryza, G.A. The Vancouver Scar Scale: An administration tool and its interrater reliability. J. Burn. Care Rehabil. 1995, 16, 535–538. [Google Scholar] [CrossRef]
- Thompson, C.M.; Sood, R.F.; Honari, S.; Carrougher, G.J.; Gibran, N.S. What score on the Vancouver Scar Scale constitutes a hypertrophic scar? Results from a survey of North American burn-care providers. Burns 2015, 41, 1442–1448. [Google Scholar] [CrossRef] [PubMed]
- Mahar, P.D.; Spinks, A.B.; Cleland, H.; Bekhor, P.; Waibel, J.S.; Lo, C.; Goodman, G. Improvement of burn scars treated with fractional ablative CO2 lasers—A systematic review and meta-analysis using the Vancouver Scar Scale. J. Burn. Care Res. 2021, 42, 200–206. [Google Scholar] [CrossRef]
- Pertea, M.; Poroch, V.; Ciobanu, P.; Filip, A.; Velenciuc, N.; Lunca, S.; Panuta, A.; Buna-Arvinte, M.; Luca, S.; Veliceasa, B. Efficiency of Bromelain-Enriched Enzyme Mixture (NexoBrid™) in the Treatment of Burn Wounds. Appl. Sci. 2021, 11, 8134. [Google Scholar] [CrossRef]
- Shin, T.M.; Bordeaux, J.S. The role of massage in scar management: A literature review. Dermatol. Surg. 2012, 38, 414–423. [Google Scholar] [CrossRef]
- Deng, H.; Li-Tsang, C.W. Measurement of vascularity in the scar: A systematic review. Burns 2019, 45, 1253–1265. [Google Scholar] [CrossRef]
- Hodin, D. Esthétimètre: Barème esthétimétrique facial [Esthetimeter: Facial esthetimetric scale]. Med. Leg. Dommage Corpor. 1973, 6, 111–116. [Google Scholar]
- Stanculescu, S.; Hostiuc, S.; Dermengiu, D. The usefulness of evaluating aesthetic prejudice with aesthetimetric scales. Rom. J. Leg. Med. 2008, 16, 117–122. [Google Scholar] [CrossRef]
- Lipman, K.; Wang, M.; Berthiaume, E.; Holloway, J.; Da Lio, A.; Ting, K.; Soo, C.; Zheng, Z. Evaluating current scar assessment methods. Ann. Plast. Surg. 2020, 84, 222–231. [Google Scholar] [CrossRef] [PubMed]
- Argyrides, M.; Kkeli, N. Multidimensional body-self relations questionnaire-appearance scales: Psychometric properties of the Greek version. Psychol. Rep. 2013, 113, 885–897. [Google Scholar] [CrossRef]
- Cash, T.E. Body-image attitudes: Evaluation, investment, and affect. Percept. Mot. Skills 1994, 78, 1168–1170. [Google Scholar] [CrossRef]
- Untas, A.; Koleck, M.; Rascle, N.; Borteyrou, X. Psychometric properties of the french adaptation of the multidimensional body self relations questionnaire–appearance scales. Psychol. Rep. 2009, 105, 461–471. [Google Scholar] [CrossRef] [PubMed]
- Dyer, A.; Hennrich, L.; Borgmann, E.; White, A.J.; Alpers, G.W. Body image and noticeable self-inflicted scars. J. Nerv. Ment. Dis. 2013, 201, 1080–1084. [Google Scholar] [CrossRef]
- Juo, Y.Y.; Park, C.; Yoo, J.; Guerron, D.; Sudan, R.; Friedman, K.; Portenier, D.; Seymour, K.A. Technical Feasibility, Outcomes, and Patient Satisfaction After Needlescopic and Laparoscopic Bariatric Surgery: A Randomized Study. Obes. Surg. 2021, 31, 5085–5091. [Google Scholar] [CrossRef] [PubMed]
- Zimet, G.D.; Dahlem, N.W.; Zimet, S.G.; Farley, G.K. The multidimensional scale of perceived social support. J. Personal. Assess. 1988, 52, 30–41. [Google Scholar] [CrossRef]
- Dambi, J.M.; Corten, L.; Chiwaridzo, M.; Jack, H.; Mlambo, T.; Jelsma, J. A systematic review of the psychometric properties of the cross-cultural translations and adaptations of the Multidimensional Perceived Social Support Scale (MSPSS). Health Qual. Life Outcomes 2018, 16, 9. [Google Scholar] [CrossRef]
- Waqas, A.; Turk, M.; Naveed, S.; Amin, A.; Kiwanuka, H.; Shafique, N.; Chaudhry, M.A. Perceived social support among patients with burn injuries: A perspective from the developing world. Burns 2018, 44, 168–174. [Google Scholar] [CrossRef]
- Abramson, L.Y.; Metalsky, G.I.; Alloy, L.B. Hopelessness depression: A theory-based subtype of depression. Psychol. Rev. 1989, 96, 358. [Google Scholar] [CrossRef]
- Metalsky, G.I.; Joiner, T.E. The hopelessness depression symptom questionnaire. Cogn. Ther. Res. 1997, 21, 359–384. [Google Scholar] [CrossRef]
- Marian, M. Trial of hopelessness theory by the use of modeling. New psychometric data on the Hopelessness Depression Symptom Questionnaire. J. Psychol. Educ. Res. 2012, 20, 45–58. [Google Scholar]
- Chen, J.; Zhou, L. Savoring as a moderator between positive life events and hopelessness depression. Soc. Behav. Personal. Int. J. 2017, 45, 1337–1344. [Google Scholar] [CrossRef]
- Manna, G.; Falgares, G.; Ingoglia, S.; Como, M.R.; De Santis, S. The relationship between self-esteem, depression and anxiety: Comparing vulnerability and scar model in the Italian context. Mediterr. J. Clin. Psychol. 2016, 30, 4. [Google Scholar]
- Klassen, A.F.; Ziolkowski, N.; Mundy, L.R.; Miller, H.C.; McIlvride, A.; DiLaura, A.; Fish, J.; Pusic, A.L. Development of a new patient-reported outcome instrument to evaluate treatments for scars: The SCAR-Q. Plast. Reconstr. Surg. Glob. Open 2018, 6, e1672. [Google Scholar] [CrossRef]
- Ziolkowski, N.I.; Pusic, A.L.; Fish, J.S.; Mundy, L.R.; Wong She, R.; Forrest, C.R.; Hollenbeck, S.; Arriagada, C.; Calcagno, M.; Greenhalgh, D.; et al. Psychometric findings for the SCAR-Q patient-reported outcome measure based on 731 children and adults with surgical, traumatic, and burn scars from four countries. Plast. Reconstr. Surg. 2020, 146, 331e–338e. [Google Scholar] [CrossRef]
- Ziolkowski, N.I.; Behman, R.; Klassen, A.F.; Fish, J.S.; Mundy, L.R.; She, R.W.; Forrest, C.R.; Hollenbeck, S.; Arriagada, C.; Greenhalgh, D.; et al. Determining the independent risk factors for worse SCAR-Q scores and future scar revision surgery. Plast. Reconstr. Surg. 2021, 148, 203–212. [Google Scholar] [CrossRef]
- Pusic, A.L.; Klassen, A.F.; Scott, A.M.; Cano, S.J. Development and psychometric evaluation of the FACE-Q satisfaction with appearance scale: A new patient-reported outcome instrument for facial aesthetics patients. Clin. Plast. Surg. 2013, 40, 249–260. [Google Scholar] [CrossRef]
- Durani, P.; McGrouther, D.A.; Ferguson, M.W. The Patient Scar Assessment Questionnaire: A reliable and valid patient-reported outcomes measure for linear scars. Plast. Reconstr. Surg. 2009, 123, 1481–1489. [Google Scholar] [CrossRef]
- Kim, M.; Mirsky, N.; Spielman, A.; Mathew, P.; Yechieli, R.; Tang, J.C.; Thaller, S.R. Evaluating Symptomatic and Psychosocial Well-being After Keloid Treatment With SCAR-Q. Aesthet Surg. J. 2022, 42, NP416–NP422. [Google Scholar] [CrossRef]
- Ostlie, D.J.; Sharp, N.E.; Thomas, P.; Sharp, S.W.; Holcomb, G.W., III; St Peter, S.D. Patient scar assessment after single-incision versus four-port laparoscopic cholecystectomy: Long-term follow-up from a prospective randomized trial. J. Laparoendosc. Adv. Surg. Tech. A 2013, 23, 553–555. [Google Scholar] [CrossRef] [PubMed]
- Voci, A.; Lee, D.; Ho, E.; Crane-Okada, R.; DiNome, M. Impact of port site scar on perception of patients with breast cancer: Patient-reported outcomes. Breast Cancer Res. Treat. 2018, 170, 569–572. [Google Scholar] [CrossRef]
- Mundy, L.R.; Miller, H.C.; Klassen, A.F.; Cano, S.J.; Pusic, A.L. Patient-Reported Outcome Instruments for Surgical and Traumatic Scars: A Systematic Review of their Development, Content, and Psychometric Validation. Aesthetic Plast Surg. 2016, 40, 792–800. [Google Scholar] [CrossRef]
- Economopoulos, K.P.; Petralias, A.; Linos, E.; Linos, D. Psychometric evaluation of Patient Scar Assessment Questionnaire following thyroid and parathyroid surgery. Thyroid 2012, 22, 145–150. [Google Scholar] [CrossRef] [PubMed]
- Guest, E.; Griffiths, C.; Harcourt, D. A qualitative exploration of psychosocial specialists’ experiences of providing support in UK burn care services. Scars Burn. Health 2018, 4, 2059513118764881. [Google Scholar] [CrossRef] [PubMed]
- Hoogewerf, C.J.; van Baar, M.E.; Middelkoop, E.; van Loey, N.E. Impact of facial burns: Relationship between depressive symptoms, self-esteem and scar severity. Gen. Hosp. Psychiatry 2014, 36, 271–276. [Google Scholar] [CrossRef] [PubMed]
- Macleod, R.; Shepherd, L.; Thompson, A.R. Posttraumatic stress symptomatology and appearance distress following burn injury: An interpretative phenomenological analysis. Health Psychol. 2016, 35, 1197–1204. [Google Scholar] [CrossRef]
- Betarbet, U.; Blalock, T.W. Keloids: A review of etiology, prevention, and treatment. J. Clin. Aesthetic Dermatol. 2020, 13, 33. [Google Scholar]
- Attoe, C.; Pounds-Cornish, E. Psychosocial adjustment following burns: An integrative literature review. Burns 2015, 41, 1375–1384. [Google Scholar] [CrossRef]
- Ngaage, M.; Agius, M. The psychology of scars: A mini-review. Psychiatr. Danub. 2018, 30 (Suppl. S7), 633–638. [Google Scholar]


{kind=link}
| No. | Scale | Year | Scar Consequence | Advantage | Disadvantages | References |
|---|---|---|---|---|---|---|
| 1. | Stony Brook Scar Evaluation Scale (SBSES) | 2007 | -aesthetic; (6 items score: 0—worst to 5—best). | -research measuring short-term (5–10 days) wound outcomes; -cosmetic outcome of wounds (5–10) days after injury until suture removal; -easy to use. | -limited applicability; -psychosocial and juridical consequences are missing. | [24,25,26,27] |
| 2. | Patient and Observer Scar Assessment Scale (POSAS) | 2004 | -physical; -aesthetic (2 subscale score between 1–10). | -assess vascularity, thickness, pigmentation, foldability, relief and pain, itching; -first scale that takes into account observer and patient ratings; -measures scar quality; -evaluates all types of scars. | -lack of psychological and juridical determined by the scar. | [28,29,30,31,32] |
| 3. | Manchester Scar Scale (MSS) | 1998 | -physical (4 parameters, score 4 best outcome-14 severe scar); -aesthetic. | -assess color, shine, contour, distortion); -wider scar applicability; -suitable for surgical scars. | -not used in research; -psychosocial and juridical effect are missing. | [33,34,35,36] |
| 4. | Hamilton Scale | 1998 | -physical; -aesthetic (photographs). | -using only photographs; -thickness, surface irregularity, vascularity, and scar size; -increased ability even in inexperienced persons. | -not based on actual scars; -psychological and juridical damage missing. | [37,38] |
| 5. | Seattle Scar Scale (SSS) | 1997 | -physical; -aesthetic (24 standard color photographs). | -color photographs; -assess: surface, height, thickness, and color differences between the scar and adjacent normal skin, using a numerical scale; -distinguish different types of scars; -scar severity. | -did not include psychological and juridical damage. | [39,40,41] |
| 6. | Vancouver Scar Scale (VSS) | 1990 | -physical (the first scar evaluation scale applied: score 0–13); -aesthetic (score: 0 and 13 points). | -thickness, height, vascularization, pliability, pigmentation; -the most frequently used scar scale; -evaluates post-burn scars; -widely used in clinical practice and research; -document change in scar appearance. | -lacks patient perception; -semi-quantitative approach to subjective characteristics; -inaccurate reproducibility evidence in the case of large or irregular scars; -does not take into account the physical and psychosocial sequelae of scars. | [42,43,44,45,46,47,48,49] |
| 7. | The aesthetic method derived from Greff’s and Hodin’s methods | 1973 | -aesthetic; -physical (divides the face into 122 sectors plus correction coefficients: coefficient C, coefficient F for correcting a fracture, coefficient R for relieves, coefficient P—the plastic coefficient, coefficient c—the coefficient of color, T—texture coefficient). | -assess the face: anterior, lateral view, and correction coefficients. | -the division of the face, the front plane and its side planes into too many sectors plus associated parameters; -does not quantify all body areas; -multiple calculations; -final formula has no interpretability for aesthetic damage; -psychosocial sequelae are missing. | [11,50,51] |
| Nr. | Scale | Year | Scar Consequence | Advantages | Disadvantages | References |
|---|---|---|---|---|---|---|
| 1 | Mekeres’ Psychosocial Internalization Scale (MPIS) | 2017 | -psychosocial; -juridical; (15 items, score between 15 and 75 points). | -assesses internalization, aesthetic prejudice, and disfigurement; -presence or absence of aesthetic prejudice; -easy to use. | -used in post-traumatic injuries; -lack of physical assessment. | [11,16,22] |
| 2 | Multidimensional Body-Self Relations Questionnaire (MBSRQ) | 1990 | -psychosocial; (69 items, subscales: appearance evaluation, appearance orientation, overweight preoccupation, body areas satisfaction scale. | -self-report inventory; -body image construction; -widely, successfully used in body image research. | -no physical or juridical assessment; -long examination time. | [53,54,55,56,57] |
| 3 | Multidimensional Scale of Perceived Social Support (MSPSS) | 1988 | -psychosocial; (12 items, 3 subscales: family, friends, and significant others). | -a self-report scale; -determine social support, appreciation, acceptance, and self-awareness, emotional support in times of crisis; -follows the social perception of friends, family, and significant others. | -missing physical and juridical elements in the examination of the scar. | [18,22,58,59,60,61] |
| 4 | Hopelessness Depression Symptom Questionnaire (HDSQ) | 1987 | -psychosocial; (32 item, 8 subscales). | -supports the existence of hopeless depression, a subtype of depression; -assessment of hopeless depression and hopelessness theory of depression; -clinical tool that takes into account the fact that each minor subscale measures a specific symptom; -allows clinicians and patients to test depression symptoms separately and not just a global score (to reflect the severity of the disorder). | -missing physical and juridical elements in the examination of the scar; -long examination time. | [20,22,62,63,64,65] |
| No. | Scale | Year | Scar Consequence | Advantage | Disadvantages | References |
|---|---|---|---|---|---|---|
| 1. | SCAR-Q Aesthetics | 2018 | -aesthetic; -physical; -psychosocial (48 item, 3 subscale). | -evaluate all types of scars; -3 domains: appearance, health-related quality of life, and adverse effects. | -the juridical aspects missing. | [66,67,68,69,70,71] |
| 2. | The Patient Scar Assessment Questionnaire (PSAQ) | 2009 | -aesthetic; -physical; -psychosocial. | -evaluate surgical scars; -5 subscales: appearance, symptoms, satisfaction with appearance, and with symptoms, consciousness. | -do not evaluate traumatic scars; -reliable for linear scars; -the juridical aspects missing. | [72,73,74,75,76] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mekeres, G.M.; Buhaș, C.L.; Csep, A.N.; Beiușanu, C.; Andreescu, G.; Marian, P.; Cheregi, C.D.; Fodor, R.; Manole, F. The Importance of Psychometric and Physical Scales for the Evaluation of the Consequences of Scars—A Literature Review. Clin. Pract. 2023, 13, 372-383. https://doi.org/10.3390/clinpract13020034
Mekeres GM, Buhaș CL, Csep AN, Beiușanu C, Andreescu G, Marian P, Cheregi CD, Fodor R, Manole F. The Importance of Psychometric and Physical Scales for the Evaluation of the Consequences of Scars—A Literature Review. Clinics and Practice. 2023; 13(2):372-383. https://doi.org/10.3390/clinpract13020034
Chicago/Turabian StyleMekeres, Gabriel Mihai, Camelia Liana Buhaș, Andrei Nicolae Csep, Corina Beiușanu, Gineta Andreescu, Paula Marian, Cornel Dragoș Cheregi, Radu Fodor, and Felicia Manole. 2023. "The Importance of Psychometric and Physical Scales for the Evaluation of the Consequences of Scars—A Literature Review" Clinics and Practice 13, no. 2: 372-383. https://doi.org/10.3390/clinpract13020034
APA StyleMekeres, G. M., Buhaș, C. L., Csep, A. N., Beiușanu, C., Andreescu, G., Marian, P., Cheregi, C. D., Fodor, R., & Manole, F. (2023). The Importance of Psychometric and Physical Scales for the Evaluation of the Consequences of Scars—A Literature Review. Clinics and Practice, 13(2), 372-383. https://doi.org/10.3390/clinpract13020034