
Real-Time Muscle Activity and Joint Range of Motion Monitor to Improve Shoulder Pain Rehabilitation in Wheelchair Basketball Players: A Non-Randomized Clinical Study

 ,
,  ,
,  , , ,
, , ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
- -
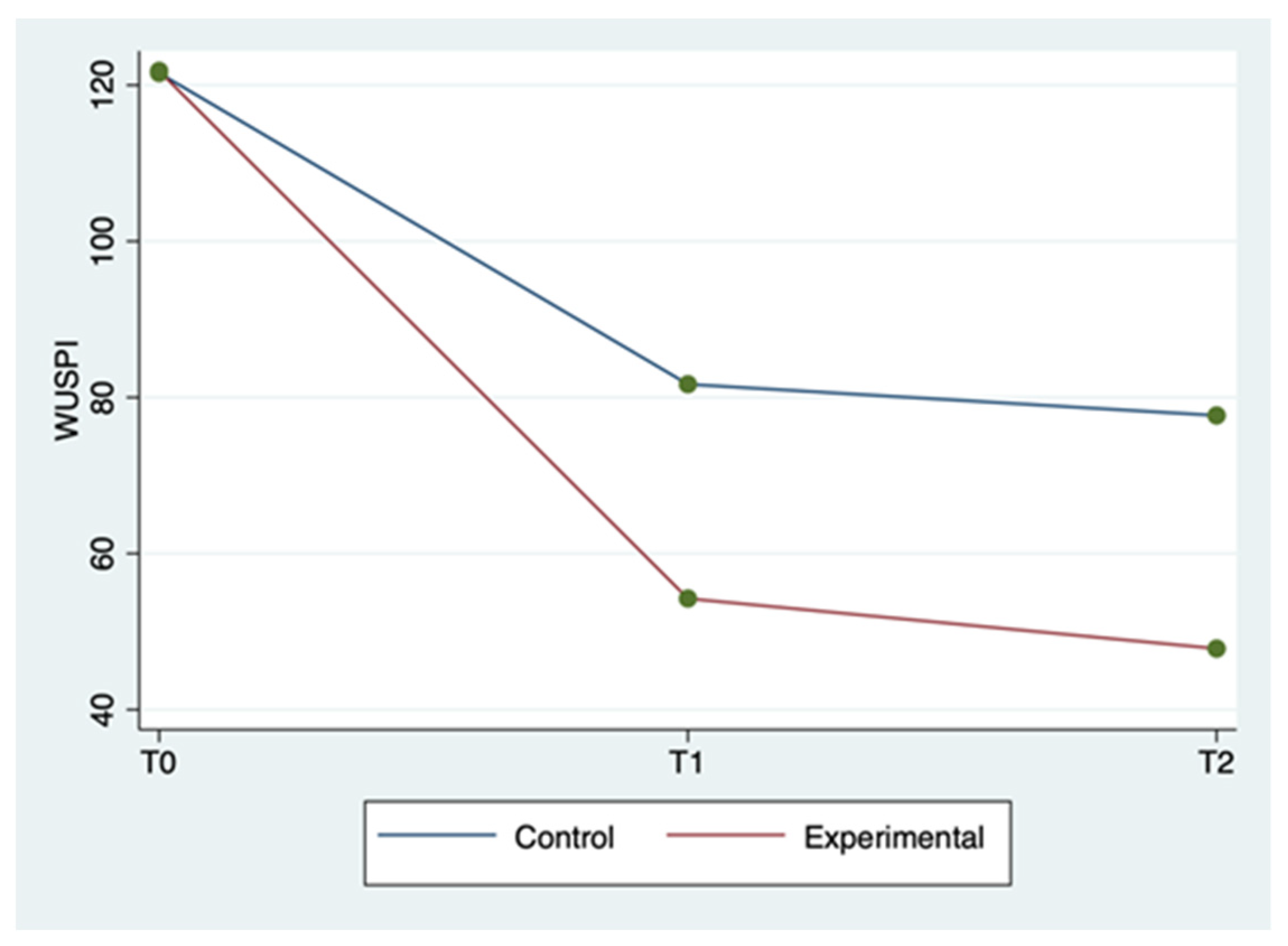
- WUSPI (Wheelchair User’s Shoulder Pain Index): this is a scale that measures shoulder pain associated with the functional activities of wheelchair users. This 15-item functional investigates shoulder pain during transfers, self-care, wheelchair mobility and general activities. The score can range from 0 to 150 [19].
- -
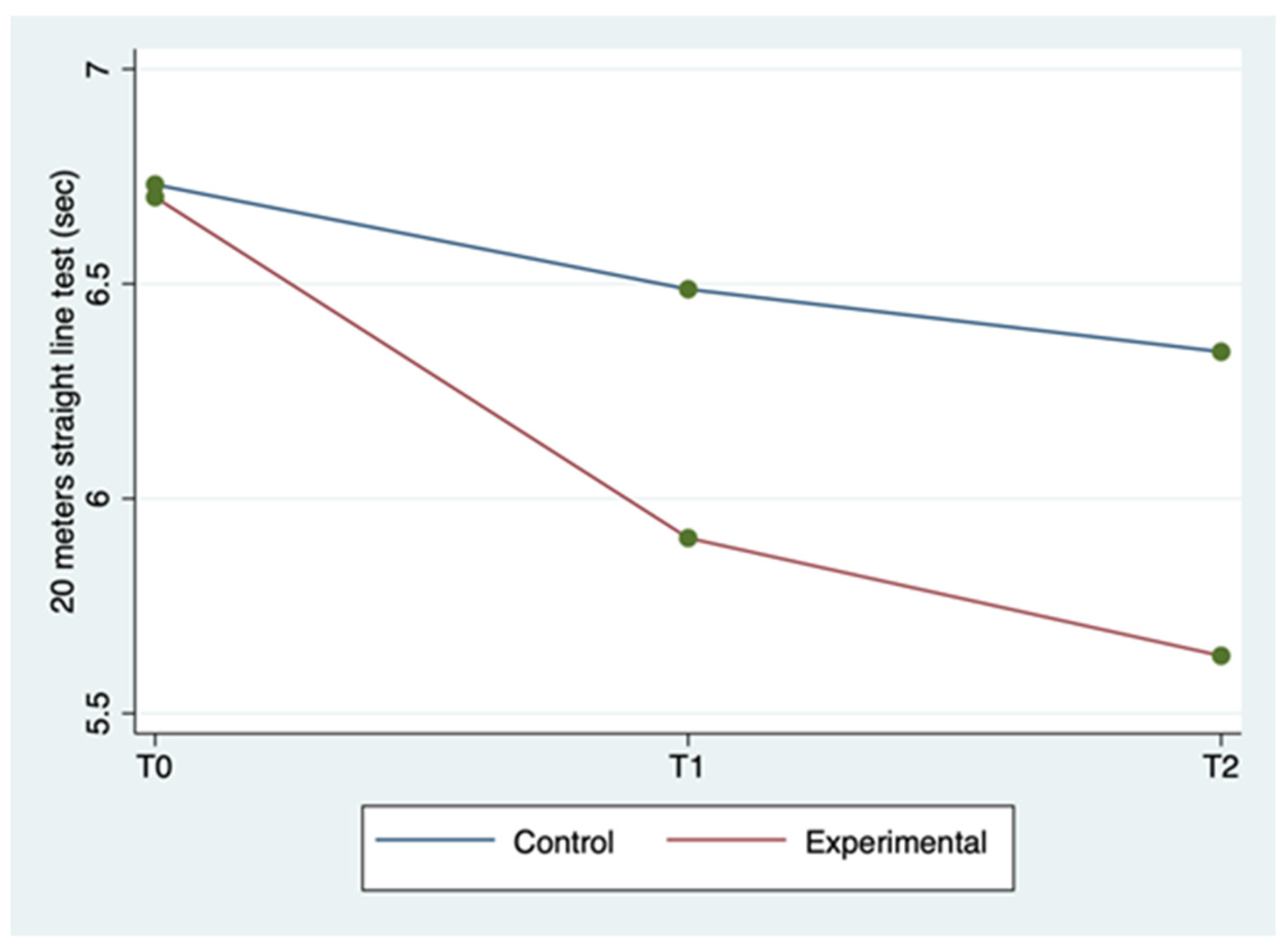
- Twenty meter straight line test: this is an instrument for wheelchair speed evaluation [20]. At the starting signal the athlete sprints, covering a 20 m distance on a straight line in the shortest time possible. Two attempts are given, and just the best one is recorded.
- -
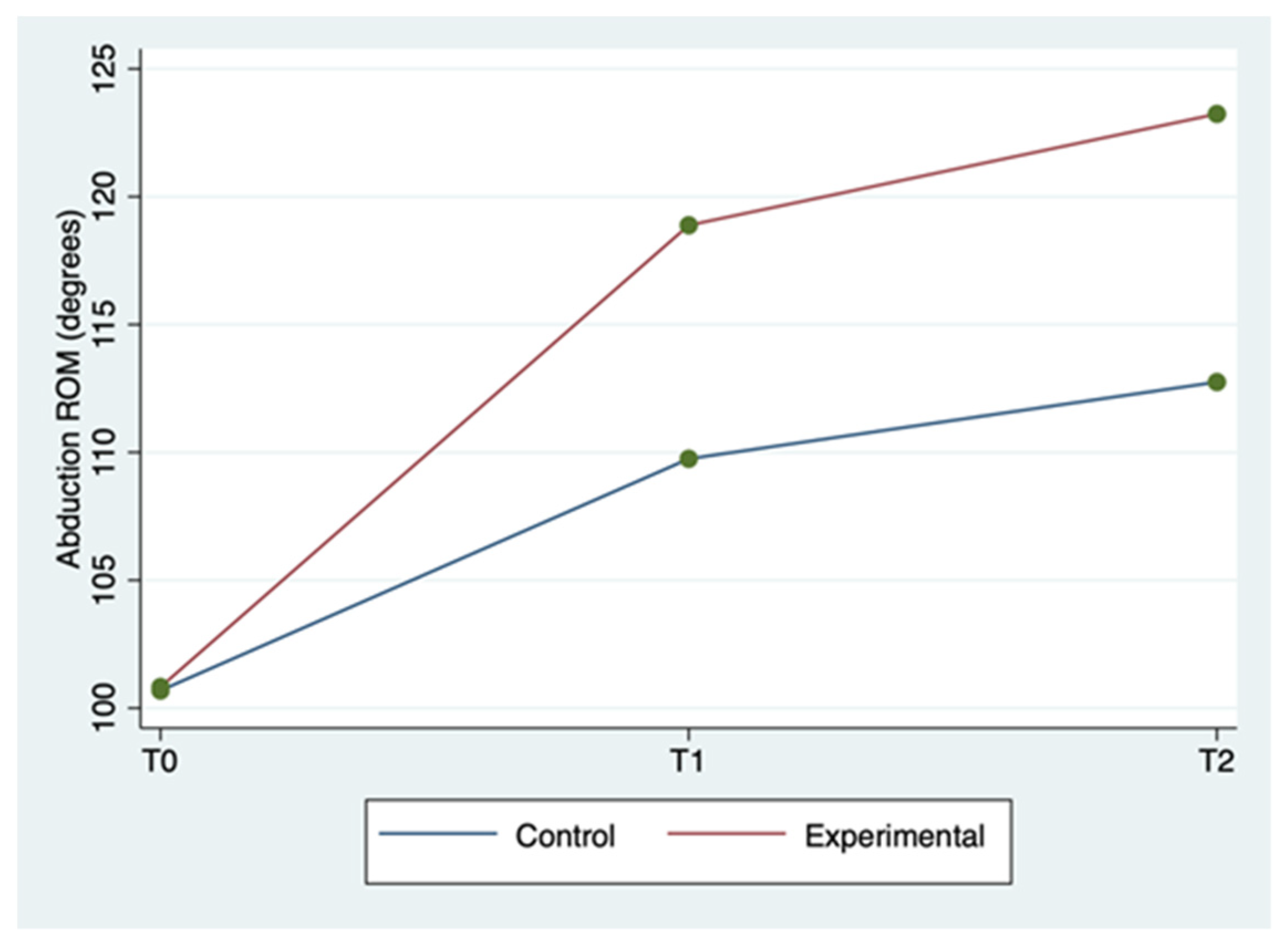
- Range of motion (ROM) in abduction: this is the evaluation measured in degrees° of the shoulder range of movement in the direction most influenced by the activity of the deltoid muscle. This evaluation was performed using the inertial sensors included in the mDurance device.
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- IWBF. International Wheelchair Basketball Federation. Available online: https://iwbf.org/the-game/history-wheelchair-basketball/ (accessed on 21 July 2022).
- Fiorilli, G.; Iuliano, E.; Aquino, G.; Battaglia, C.; Giombini, A.; Calcagno, G.; di Cagno, A. Mental health and social participation skills of wheelchair basketball players: A controlled study. Res. Dev. Disabil. 2013, 34, 3679–3685. [Google Scholar] [CrossRef] [PubMed]
- Bates, L.; Kearns, R.; Witten, K.; Carroll, P. ‘A level playing field’: Young people’s experiences of wheelchair basketball as an enabling place. Health Place 2019, 60, 102192. [Google Scholar] [CrossRef]
- Sá, K.; e Silva, A.C.; Gorla, J.; Silva, A.; e Silva, M.M. Injuries in Wheelchair Basketball Players: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 5869. [Google Scholar] [CrossRef] [PubMed]
- Tsunoda, K.; Mutsuzaki, H.; Hotta, K.; Tachibana, K.; Shimizu, Y.; Fukaya, T.; Ikeda, E.; Wadano, Y. Correlates of shoulder pain in wheelchair basketball players from the Japanese national team: A cross-sectional study. J. Back Musculoskelet. Rehabilitation 2016, 29, 795–800. [Google Scholar] [CrossRef] [PubMed]
- Vanlandewijck, Y.C.; Evaggelinou, C.; Daly, D.J.; Verellen, J.; Van Houtte, S.; Aspeslagh, V.; Hendrickx, R.; Piessens, T.; Zwakhoven, B. The relationship between functional potential and field performance in elite female wheelchair basketball players. J. Sports Sci. 2004, 22, 668–675. [Google Scholar] [CrossRef]
- Karasuyama, M.; Oike, T.; Okamatsu, S.; Kawakami, J. Shoulder pain in wheelchair basketball athletes: A scoping review. J. Spinal Cord Med. 2022, 1–7. [Google Scholar] [CrossRef]
- sunoda, K.; Mutsuzaki, H.; Kanae, K.; Tachibana, K.; Shimizu, Y.; Wadano, Y. Associations between wheelchair user’s shoulder pain index and tendinitis in the long head of the biceps tendon among female wheelchair basketball players from the Japanese national team. Asia-Pacific J. Sports Med. Arthrosc. Rehabilitation Technol. 2021, 24, 29–34. [Google Scholar] [CrossRef]
- de Sire, A.; Ammendolia, A.; Lippi, L.; Farì, G.; Cisari, C.; Invernizzi, M. Percutaneous Electrical Nerve Stimulation (PENS) as a Rehabilitation Approach for Reducing Mixed Chronic Pain in Patients with Musculoskeletal Disorders. Appl. Sci. 2021, 11, 4257. [Google Scholar] [CrossRef]
- García-Gómez, S.; Pérez-Tejero, J.; Hoozemans, M.; Barakat, R. Effect of a Home-based Exercise Program on Shoulder Pain and Range of Motion in Elite Wheelchair Basketball Players: A Non-Randomized Controlled Trial. Sports 2019, 7, 180. [Google Scholar] [CrossRef]
- Merletti, R.; Aventaggiato, M.; Botter, A.; Holobar, A.; Marateb, H.R.; Vieira, T. Advances in Surface EMG: Recent Progress in Detection and Processing Techniques. Crit. Rev. Biomed. Eng. 2010, 38, 305–345. [Google Scholar] [CrossRef]
- Zasadzka, E.; Tobis, S.; Trzmiel, T.; Marchewka, R.; Kozak, D.; Roksela, A.; Pieczyńska, A.; Hojan, K. Application of an EMG-Rehabilitation Robot in Patients with Post-Coronavirus Fatigue Syndrome (COVID-19)—A Feasibility Study. Int. J. Environ. Res. Public Health 2022, 19, 10398. [Google Scholar] [CrossRef] [PubMed]
- Molina-Molina, A.; Ruiz-Malagón, E.J.; Carrillo-Pérez, F.; Roche-Seruendo, L.E.; Damas, M.; Banos, O.; García-Pinillos, F. Validation of mDurance, A Wearable Surface Electromyography System for Muscle Activity Assessment. Front. Physiol. 2020, 11, 606287. [Google Scholar] [CrossRef] [PubMed]
- Juul-Kristensen, B.; Larsen, C.M.; Eshoj, H.; Clemmensen, T.; Hansen, A.; Bo Jensen, P.; Boyle, E.; Søgaard, K. Positive effects of neuromuscular shoulder exercises with or without EMG-biofeedback, on pain and function in participants with subacromial pain syndrome—A randomised controlled trial. J. Electromyogr. Kinesiol. 2019, 48, 161–168. [Google Scholar] [CrossRef] [PubMed]
- Calabrò, R.S.; Filoni, S.; Billeri, L.; Balletta, T.; Cannavò, A.; Militi, A.; Milardi, D.; Pignolo, L.; Naro, A. Robotic Rehabili-tation in Spinal Cord Injury: A Pilot Study on End-Effectors and Neurophysiological Outcomes. Ann. Biomed. Eng. 2021, 49, 732–745. [Google Scholar] [CrossRef]
- Van Straaten, M.G.; Cloud-Biebl, B.; Morrow, M.M.; Ludewig, P.; Zhao, K.D. Effectiveness of Home Exercise on Pain, Function, and Strength of Manual Wheelchair Users with Spinal Cord Injury: A High-Dose Shoulder Program with Telerehabilitation. Arch. Phys. Med. Rehabil. 2014, 95, 1810–1817.e2. [Google Scholar] [CrossRef]
- Tamburella, F.; Moreno, J.C.; Herrera Valenzuela, D.S.; Pisotta, I.; Iosa, M.; Cincotti, F.; Molinari, M. Influences of the biofeedback content on robotic post-stroke gait rehabilitation: Electromyographic vs joint torque bio-feedback. J. Neuroeng. Rehabil. 2019, 16, 95. [Google Scholar] [CrossRef]
- Riley, A.H.; Callahan, C. Shoulder Rehabilitation Protocol and Equipment Fit Recommendations for the Wheelchair Sport Athlete with Shoulder Pain. Sports Med. Arthrosc. Rev. 2019, 27, 67–72. [Google Scholar] [CrossRef]
- A Curtis, K.; E Roach, K.; Applegate, E.B.; Amar, T.; Benbow, C.S.; Genecco, T.D.; Gualano, J. Development of the Wheelchair User’s Shoulder Pain Index (WUSPI). Spinal Cord 1995, 33, 290–293. [Google Scholar] [CrossRef]
- Vanlandewijck, Y.C.; Daly, D.J.; Theisen, D.M. Field Test Evaluation of Aerobic, Anaerobic, and Wheelchair Basketball Skill Performances. Int. J. Sports Med. 1999, 20, 548–554. [Google Scholar] [CrossRef]
- Farì, G.; Notarnicola, A.; DI Paolo, S.; Covelli, I.; Moretti, B. Epidemiology of injuries in water board sports: Trauma versus overuse injury. J. Sports Med. Phys. Fit. 2021, 61, 707–711. [Google Scholar] [CrossRef]
- Farì, G.; Fischetti, F.; Zonno, A.; Marra, F.; Maglie, A.; Bianchi, F.; Messina, G.; Ranieri, M.; Megna, M. Musculoskeletal Pain in Gymnasts: A Retrospective Analysis on a Cohort of Professional Athletes. Int. J. Environ. Res. Public Health 2021, 18, 5460. [Google Scholar] [CrossRef] [PubMed]
- Fagher, K.; Lexell, J. Sports-related injuries in athletes with disabilities. Scand. J. Med. Sci. Sports 2014, 24, e320–e331. [Google Scholar] [CrossRef] [PubMed]
- Van Der Slikke, R.M.A.; Berger, M.A.M.; Bregman, D.J.J.; Veeger, D.H.E.J. Wearable Wheelchair Mobility Performance Measurement in Basketball, Rugby, and Tennis: Lessons for Classification and Training. Sensors 2020, 20, 3518. [Google Scholar] [CrossRef] [PubMed]
- Hoo, J.S. Shoulder Pain and the Weight-bearing Shoulder in the Wheelchair Athlete. Sports Med. Arthrosc. Rev. 2019, 27, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Farì, G.; Santagati, D.; Macchiarola, D.; Ricci, V.; Di Paolo, S.; Caforio, L.; Invernizzi, M.; Notarnicola, A.; Megna, M.; Ranieri, M. Musculoskeletal pain related to surfing practice: Which role for sports rehabilitation strategies? A cross-sectional study. J. Back Musculoskelet. Rehabil. 2022, 35, 911–917. [Google Scholar] [CrossRef]
- Cratsenberg, K.A.; Deitrick, C.E.; Harrington, T.K.; Kopecky, N.R.; Matthews, B.D.; Ott, L.M.; Coeytaux, R.R. Effectiveness of Exercise Programs for Management of Shoulder Pain in Manual Wheelchair Users with Spinal Cord Injury. J. Neurol. Phys. Ther. 2015, 39, 197–203. [Google Scholar] [CrossRef]
- Mason, B.; Warner, M.; Briley, S.; Goosey-Tolfrey, V.; Vegter, R. Managing shoulder pain in manual wheelchair users: A scoping review of conservative treatment interventions. Clin. Rehabil. 2020, 34, 741–753. [Google Scholar] [CrossRef]
- Marisa, M.; Riccardo, M.; Giacomo, F.; Giulia, G.; Franca, D.; Pietro, F.; Giancarlo, I. Pain and Muscles Properties Modifications After Botulinum Toxin Type A (BTX-A) and Radial Extracorporeal Shock Wave (rESWT) Combined Treatment. Endocrine, Metab. Immune Disord. -Drug Targets 2019, 19, 1127–1133. [Google Scholar] [CrossRef]
- Farì, G.; Santagati, D.; Pignatelli, G.; Scacco, V.; Renna, D.; Cascarano, G.; Vendola, F.; Bianchi, F.P.; Fiore, P.; Ranieri, M.; et al. Collagen Peptides, in Association with Vitamin C, Sodium Hyaluronate, Manganese and Copper, as Part of the Rehabilitation Project in the Treatment of Chronic Low Back Pain. Endocrine, Metab. Immune Disord. -Drug Targets 2022, 22, 108–115. [Google Scholar] [CrossRef]
- Farì, G.; Lunetti, P.; Pignatelli, G.; Raele, M.V.; Cera, A.; Mintrone, G.; Ranieri, M.; Megna, M.; Capobianco, L. The Effect of Physical Exercise on Cognitive Impairment in Neurodegenerative Disease: From Pathophysiology to Clinical and Rehabilitative Aspects. Int. J. Mol. Sci. 2021, 22, 11632. [Google Scholar] [CrossRef]
- Nawoczenski, D.A.; Ritter-Soronen, J.M.; Wilson, C.M.; A Howe, B.; Ludewig, P.M. Clinical Trial of Exercise for Shoulder Pain in Chronic Spinal Injury. Phys. Ther. 2006, 86, 1604–1618. [Google Scholar] [CrossRef] [PubMed]
- Middaugh, S.; Thomas, K.J.; Smith, A.R.; McFall, T.L.; Klingmueller, J. EMG Biofeedback and Exercise for Treatment of Cervical and Shoulder Pain in Individuals with a Spinal Cord Injury: A Pilot Study. Top. Spinal Cord Inj. Rehabil. 2013, 19, 311–323. [Google Scholar] [CrossRef] [PubMed]
- Mulroy, S.J.; Thompson, L.; Kemp, B.; Hatchett, P.P.; Newsam, C.J.; Lupold, D.G.; Gordon, J. Strengthening and optimal movements for painful shoulders (STOMPS) in chronic spinal cord injury: A randomized controlled trial. Phys. Ther. 2011, 91, 305–324. [Google Scholar] [CrossRef] [PubMed]
- Pellegrino, R.; Di Iorio, A.; Brindisino, F.; Paolucci, T.; Moretti, A.; Iolascon, G. Effectiveness of combined extracorporeal shock-wave therapy and hyaluronic acid injections for patients with shoulder pain due to rotator cuff tendinopathy: A person-centered approach with a focus on gender differences to treatment response. BMC Musculoskelet. Disord. 2022, 23, 863. [Google Scholar] [CrossRef]
- de Sire, A.; Demeco, A.; Marotta, N.; Spanò, R.; Curci, C.; Farì, G.; Ammendolia, A. Neuromuscular impairment of knee stabilizer muscles in a COVID-19 cluster of female volleyball players: Which role for rehabilitation in the post-COVID-19 return-to-play? Appl. Sci. 2022, 12, 557. [Google Scholar] [CrossRef]
- Pellegrino, R.; Brindisino, F.; Barassi, G.; Sparvieri, E.; DIIorio, A.; de Sire, A.; Ruosi, C. Combined ultrasound guided peritendinous hyaluronic acid (500–730 Kda) injection with extracorporeal shock waves therapy vs. extracorporeal shock waves therapy-only in the treatment of shoulder pain due to rotator cuff tendinopathy. A randomized clinical trial. J. Sports Med. Phys. Fitness 2022, 62, 1211–1218. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | Control (n = 16) | Experimental (n = 17) | Total (n = 33) | p-Value |
|---|---|---|---|---|
| Age; mean ± SD (range) | 38.7 ± 8.7 (23–55) | 37.2 ± 10.0 (24–57) | 37.9 ± 9.3 (23–57) | 0.648 |
| BMI; mean ± SD (range) | 23.7 ± 3.2 (18.8–31.1) | 24.4 ± 4.9 (17.0–35.9) | 24.0 ± 4.1 (17.0–35.9) | 0.623 |
| Right dominant limb; n (%) | 13 (81.3) | 12 (70.6) | 25 (75.8) | 0.475 |
| Shoulder pain on the right side; n (%) | 14 (87.5) | 13 (76.5) | 27 (81.8) | 0.412 |
| Outcome | Group | T0 | T1 | T2 | Comparison between Groups | Comparison between Times | Interaction between Time and Group |
|---|---|---|---|---|---|---|---|
| WUSPI | Control | 121.6 ± 9.6 (107–137) | 81.7 ± 6.3 (71–92) | 77.7 ± 6.6 (66–89) | <0.001 | <0.001 | <0.001 |
| Experimental | 121.8 ± 8.9 (106–135) | 54.2 ± 8.5 (41–70) | 47.8 ± 8.7 (36–67) | ||||
| Total | 121.7 ± 9.1 (106–137) | 67.5 ± 15.8 (41–92) | 62.3 ± 17.0 (36–89) | ||||
| 20 m straight line test (seconds) | Control | 6.7 ± 0.6 (5.7–7.7) | 6.5 ± 0.6 (5.6–7.5) | 6.5 ± 0.6 (5.6–7.5) | 0.014 | <0.001 | <0.001 |
| Experimental | 6.7 ± 0.5(5.7–7.7) | 5.9 ± 0.4 (5.1–6.5) | 5.6 ± 0.5 (4.8–6.4) | ||||
| Total | 6.7 ± 0.6 (5.7–7.7) | 6.2 ± 0.6 (5.1–7.5) | 6.0 ± 0.6 (4.8–7.3) | ||||
| Abduction ROM (degrees) | Control | 100.7 ± 3.4 (97–107) | 109.8 ± 2.6 (105–115) | 112.8 ± 2.6 (108–118) | <0.001 | <0.001 | <0.001 |
| Experimental | 100.8 ± 4.2 (94–110) | 118.9 ± 4.2 (111–126) | 123.2 ± 3.7 (116–128) | ||||
| Total | 100.8 ± 3.8 (94–110) | 114.5 ± 5.8 (105–126) | 118.2 ± 6.2 (108–128) |
| Experimental Group | Control Group | ||||
|---|---|---|---|---|---|
| Outcome | Time | Contrast (95%CI) | p-Value | Contrast (95%CI) | p-Value |
| WUSPI | T1 vs. T0 | −67.6 (−71.2–−63.9) | <0.001 | −39.9 (−43.6–−36.1) | <0.001 |
| T2 vs. T0 | −74.0 (−77.6–−70.4) | <0.001 | −43.9 (−47.6–−40.1) | <0.001 | |
| T2 vs. T1 | −6.4 (−10.0–−2.8) | 0.001 | −4.0 (−7.7–−0.3) | 0.037 | |
| 20 m straight line test | T1 vs. T0 | −0.8 (−1.0–−0.6) | <0.001 | −0.2 (−0.4–0.1) | 0.006 |
| T2 vs. T0 | −1.1 (−1.2–−0.9) | <0.001 | −0.4 (−0.6–−0.2) | <0.001 | |
| T2 vs. T1 | −0.3 (−0.4–−0.1) | 0.002 | −0.1 (−0.3–−0.1) | 0.095 | |
| Abduction ROM | T1 vs. T0 | 18.1 (16.3–19.8) | <0.001 | 9.1 (7.3–10.9) | <0.001 |
| T2 vs. T0 | 22.4 (20.7–24.2) | <0.001 | 12.1 (10.3–13.9) | <0.001 | |
| T2 vs. T1 | 4.4 (2.6–6.1) | <0.001 | 3.0 (1.2–4.8) | 0.001 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Farì, G.; Megna, M.; Fiore, P.; Ranieri, M.; Marvulli, R.; Bonavolontà, V.; Bianchi, F.P.; Puntillo, F.; Varrassi, G.; Reis, V.M. Real-Time Muscle Activity and Joint Range of Motion Monitor to Improve Shoulder Pain Rehabilitation in Wheelchair Basketball Players: A Non-Randomized Clinical Study. Clin. Pract. 2022, 12, 1092-1101. https://doi.org/10.3390/clinpract12060111
Farì G, Megna M, Fiore P, Ranieri M, Marvulli R, Bonavolontà V, Bianchi FP, Puntillo F, Varrassi G, Reis VM. Real-Time Muscle Activity and Joint Range of Motion Monitor to Improve Shoulder Pain Rehabilitation in Wheelchair Basketball Players: A Non-Randomized Clinical Study. Clinics and Practice. 2022; 12(6):1092-1101. https://doi.org/10.3390/clinpract12060111
Chicago/Turabian StyleFarì, Giacomo, Marisa Megna, Pietro Fiore, Maurizio Ranieri, Riccardo Marvulli, Valerio Bonavolontà, Francesco Paolo Bianchi, Filomena Puntillo, Giustino Varrassi, and Victor Machado Reis. 2022. "Real-Time Muscle Activity and Joint Range of Motion Monitor to Improve Shoulder Pain Rehabilitation in Wheelchair Basketball Players: A Non-Randomized Clinical Study" Clinics and Practice 12, no. 6: 1092-1101. https://doi.org/10.3390/clinpract12060111
APA StyleFarì, G., Megna, M., Fiore, P., Ranieri, M., Marvulli, R., Bonavolontà, V., Bianchi, F. P., Puntillo, F., Varrassi, G., & Reis, V. M. (2022). Real-Time Muscle Activity and Joint Range of Motion Monitor to Improve Shoulder Pain Rehabilitation in Wheelchair Basketball Players: A Non-Randomized Clinical Study. Clinics and Practice, 12(6), 1092-1101. https://doi.org/10.3390/clinpract12060111