
Strengthening Saudi Arabia’s Primary Health Care through an e-Referral System: A Case Study

Abstract
:1. Introduction
2. Methods
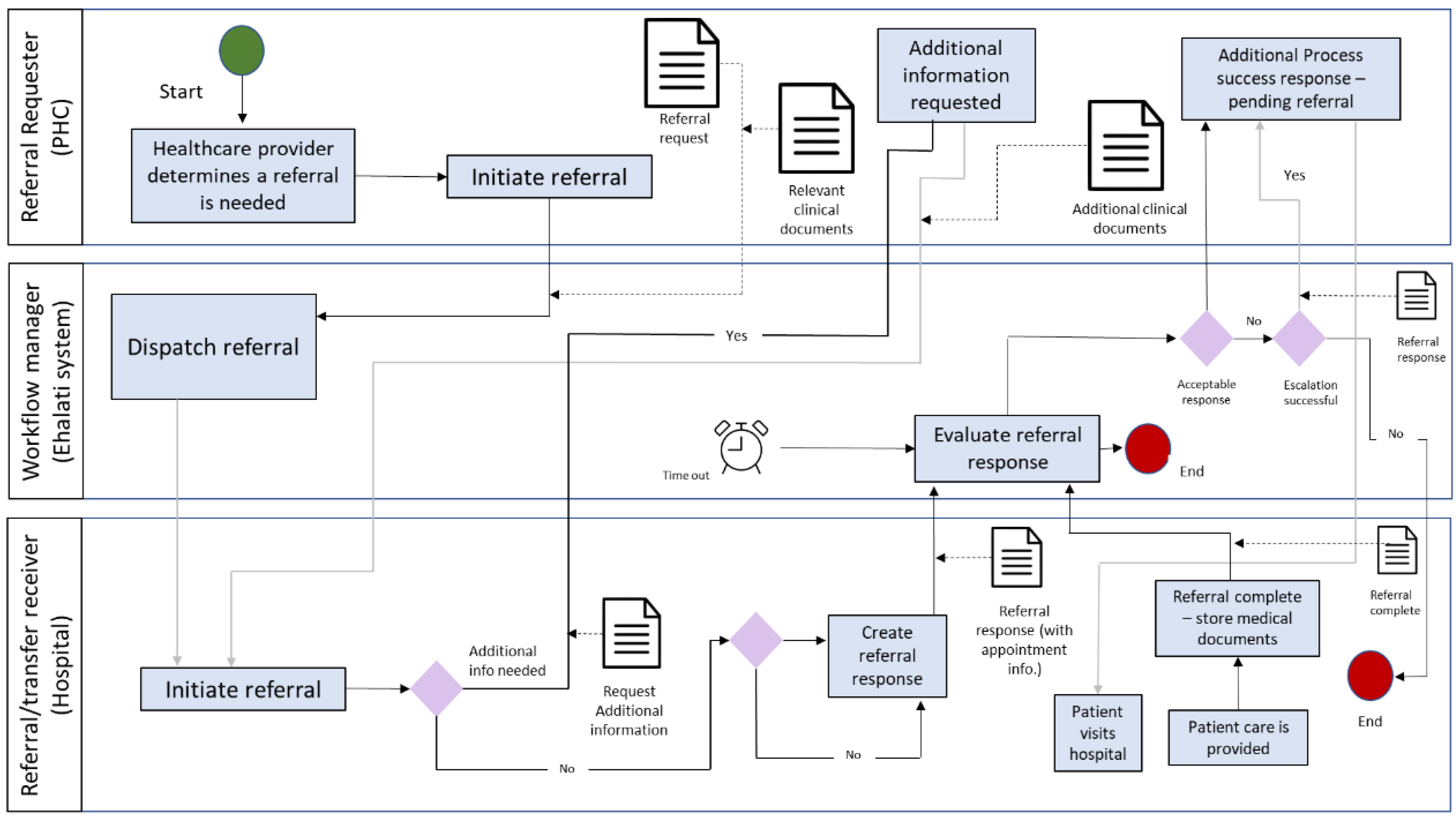
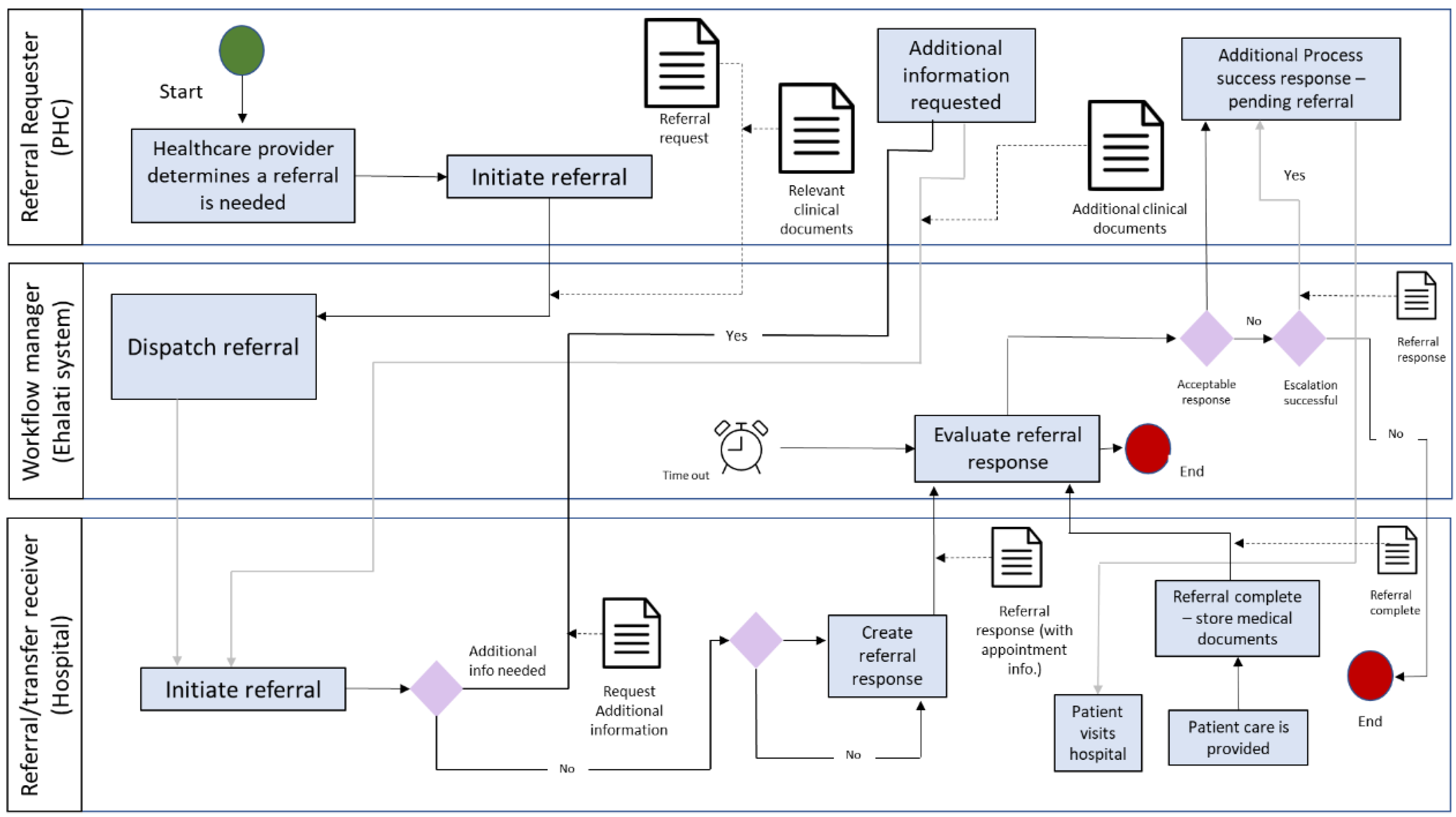
2.1. E-Referral System
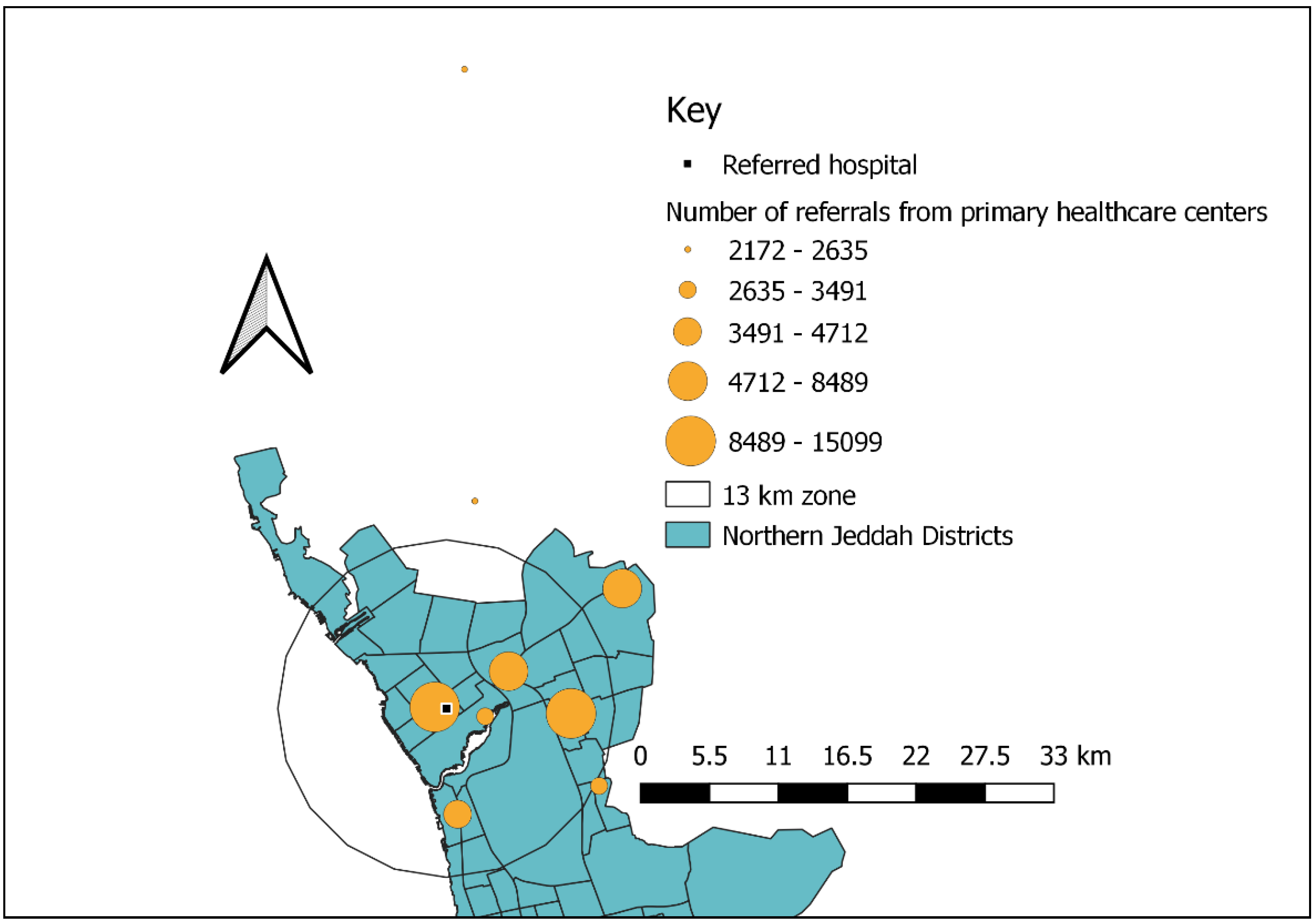
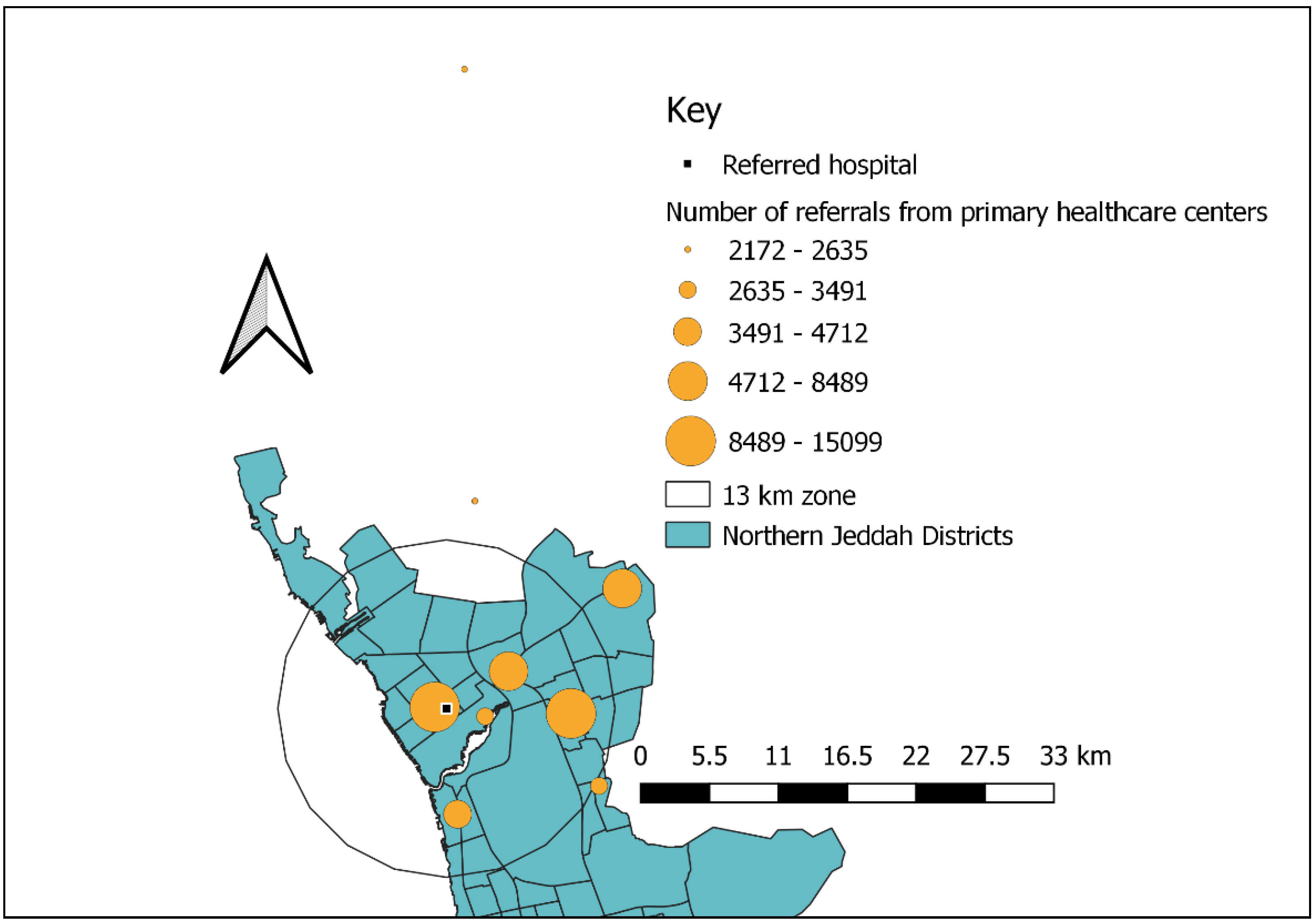
2.2. Study Area
2.3. Study Design, Setting, and Sample Selection
2.4. Measures
2.5. Ethics Approval
2.6. Statistical Analysis
3. Results
3.1. Practice Characteristics
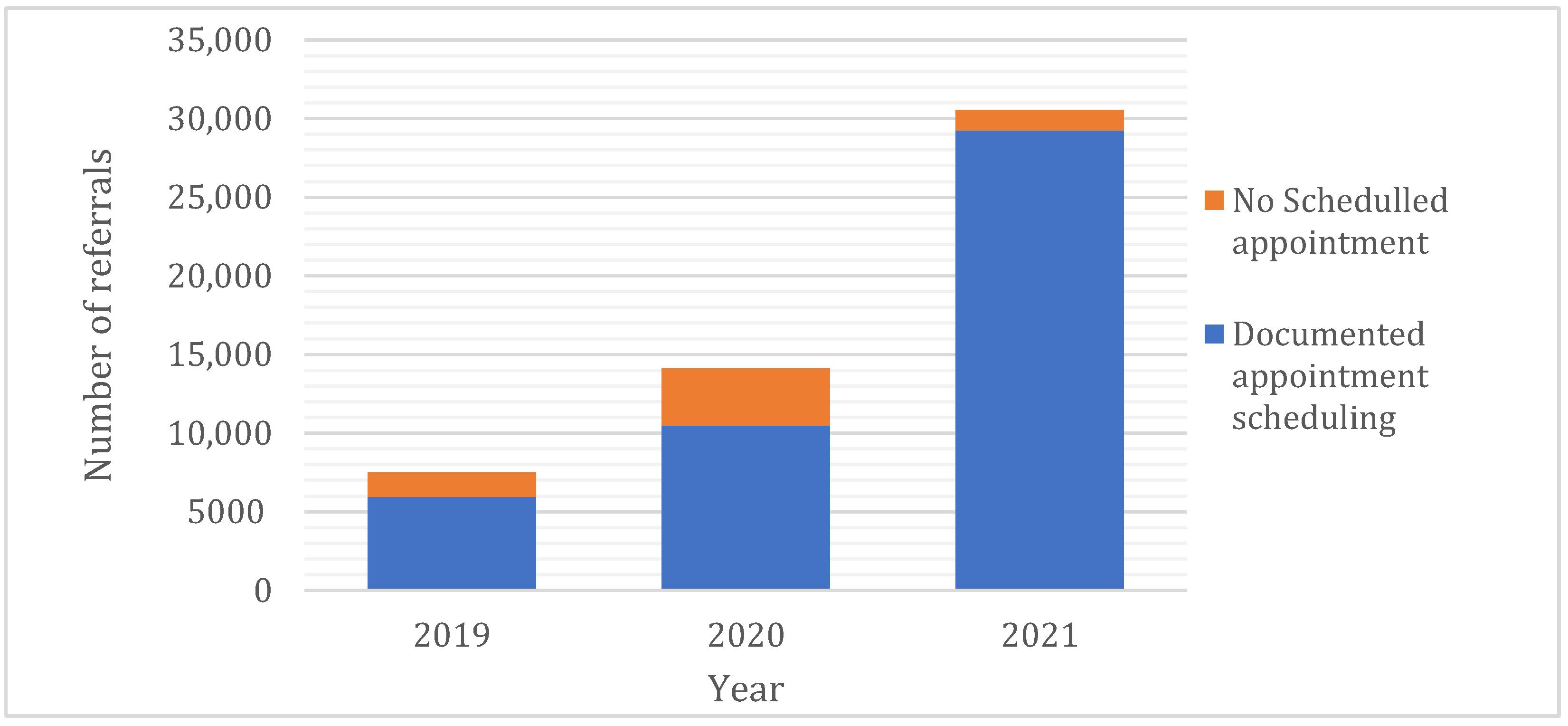
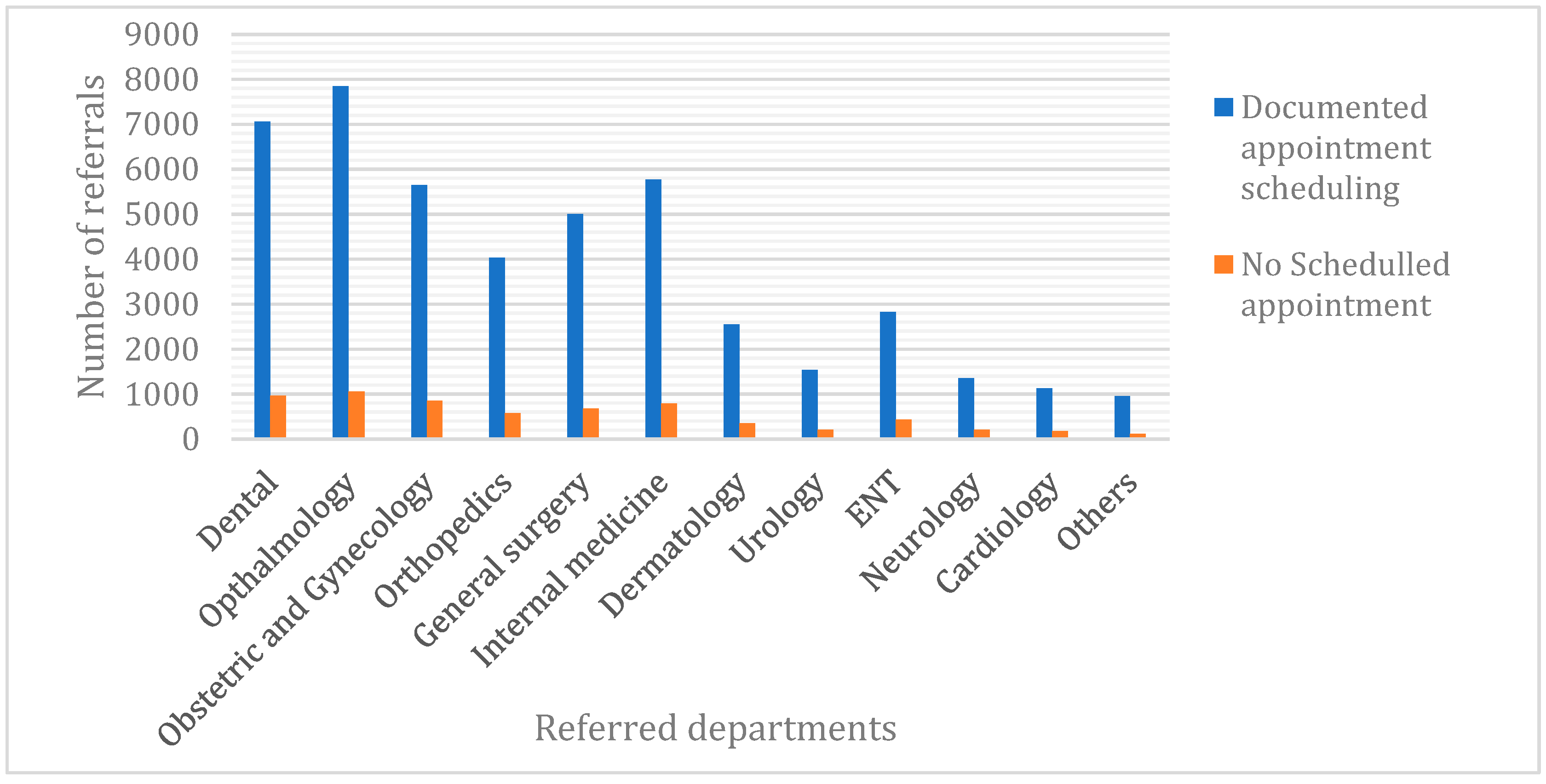
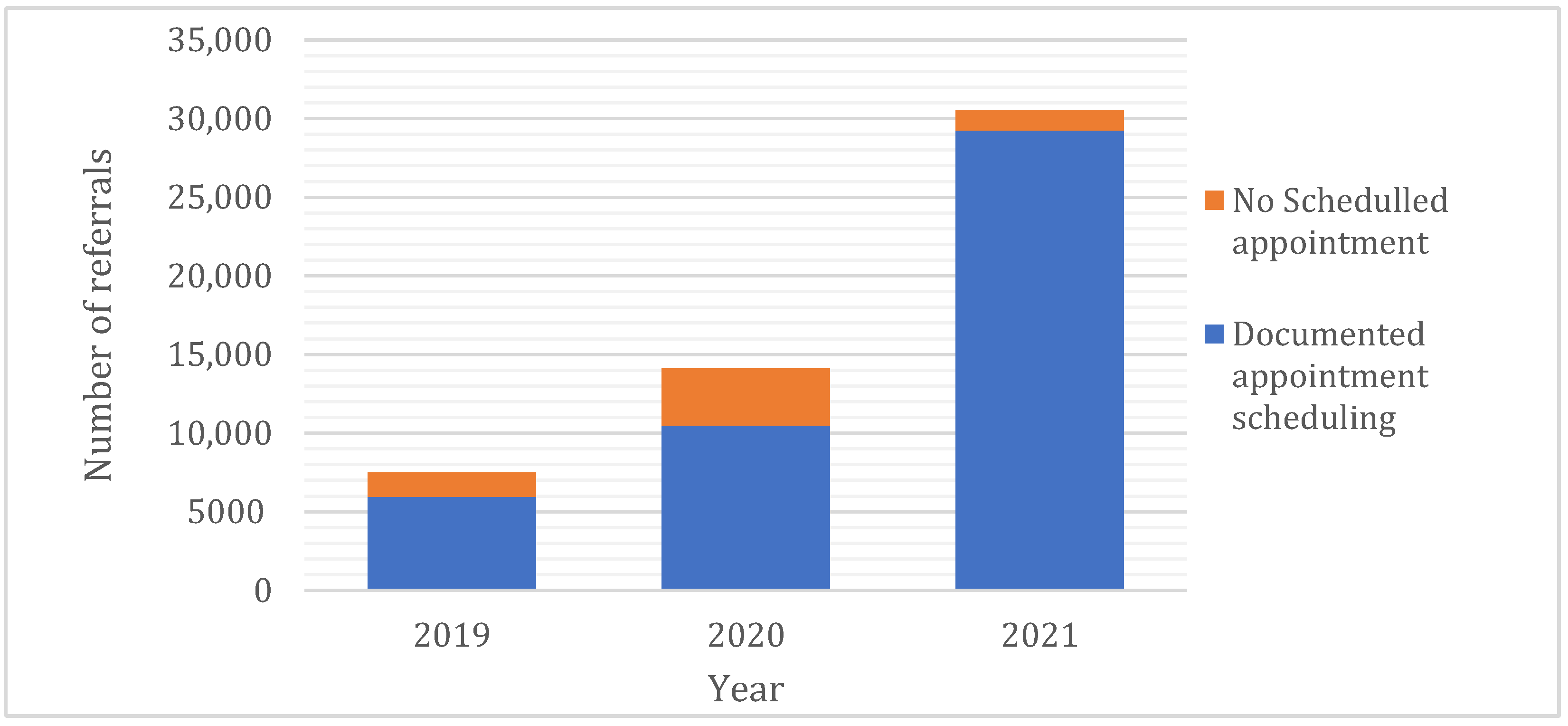
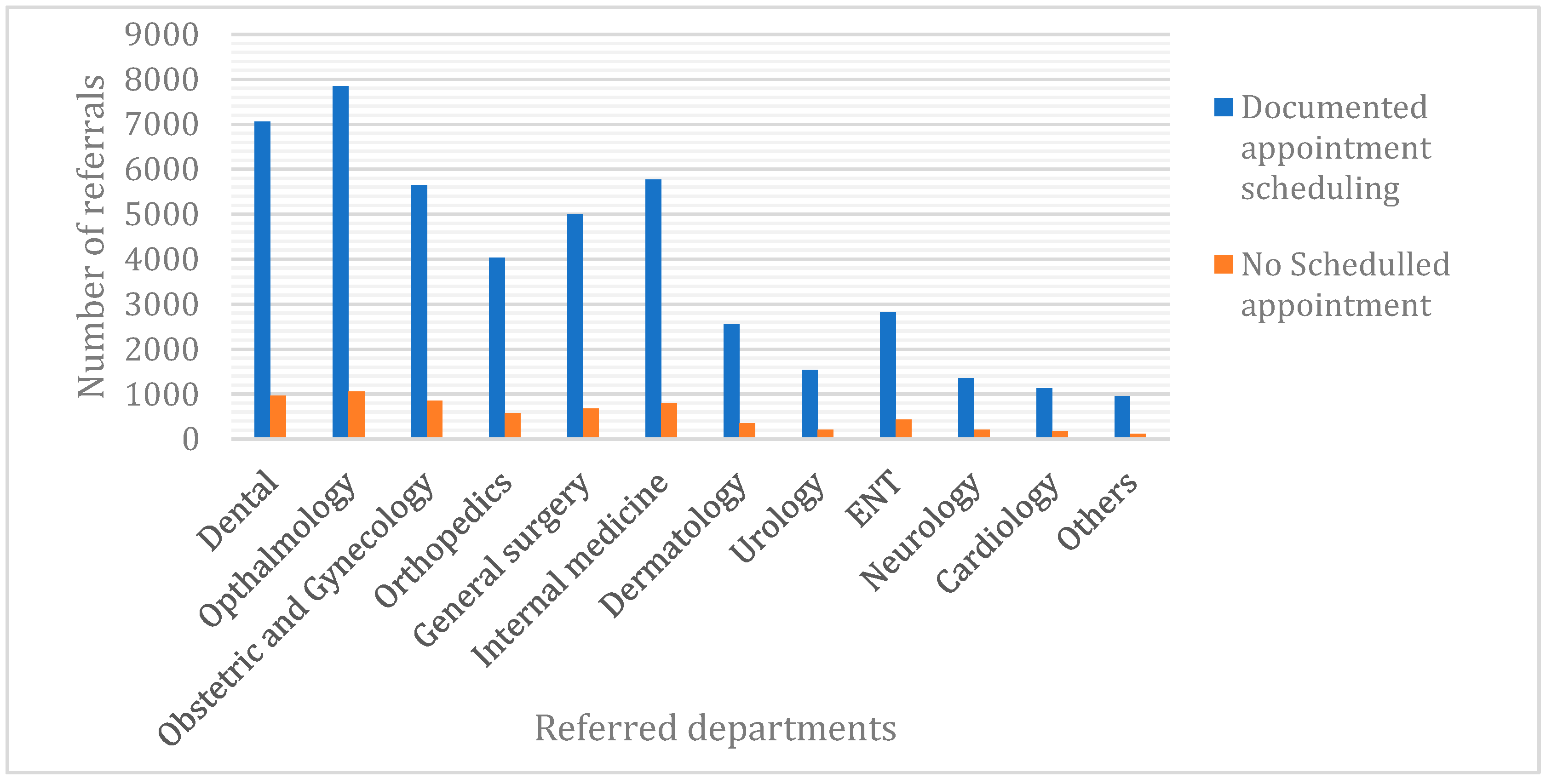
3.2. Referral Characteristics
3.3. Patients’ Characteristics
4. Discussion
5. Limitations
6. Implications and Recommendations
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Van Weel, C.; Kidd, M.R. Why strengthening primary health care is essential to achieving universal health coverage. Can. Med. Assoc. J. 2018, 190, E463–E466. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lal, A.; Erondu, N.A.; Heymann, D.L.; Gitahi, G.; Yates, R. Fragmented health systems in COVID-19: Rectifying the misalignment between global health security and universal health coverage. Lancet 2021, 397, 61–67. [Google Scholar] [CrossRef]
- Kiourtis, A.; Mavrogiorgou, A.; Kyriazis, D. A Comparative Study of Bluetooth SPP, PAN and GOEP for Efficient Exchange of Healthcare Data. Emerg. Sci. J. 2021, 5, 279–293. [Google Scholar] [CrossRef]
- WHO. Referral Systems [Internet]. 2021. Available online: https://www.who.int/ (accessed on 9 February 2021).
- Jarallah, J.S. Referral from primary care to hospitals in Saudi Arabia: 1) quality of referral letters and feedback reports. J. Fam. Community Med. 1998, 5, 15–22. [Google Scholar]
- Alshami, M.; Almutairi, S.; Househ, M. The implementation experience of an electronic referral system in saudi arabia: A case study. Stud. Health Technol. Inform. 2014, 202, 138–141. [Google Scholar] [PubMed]
- Bashar, M.A.; Bhattacharya, S.; Tripathi, S.; Sharma, N.; Singh, A. Strengthening primary health care through e-referral system. J. Fam. Med. Prim. Care 2019, 8, 1511–1513. [Google Scholar]
- Saudi Health Council. Saudi eHealth eReferral and eTransfer Interoperability Use Case. 2016. Available online: https://nhic.gov.sa/eServices/STD/Documents/UC0010%20Saudi%20eHealth%20eReferral%20and%20eTransfer%20Interoperability%20Use%20Case%20v1.0.pdf (accessed on 9 February 2021).
- Senitan, M.; Alhaiti, A.H.; Gillespie, J.; Alotaibi, B.F.; Lenon, G.B. The Referral System between Primary and Secondary Health Care in Saudi Arabia for Patients with Type 2 Diabetes: A Systematic Review. J. Diabetes Res. 2017, 2017, 4183604. [Google Scholar] [CrossRef]
- Saudi Ministry of Health. (Mawid) Service. 2021. Available online: https://www.moh.gov.sa/en/eServices/Pages/cassystem.aspx (accessed on 9 May 2022).
- Saudi Ministry of Health. Saudi eHealth eReferral and eTransfare Interoperability Use Case Version 1. 2015. Available online: https://www.moh.gov.sa/en/Ministry/ehealthstd/Documents/eHealth%20Standards%20Files/eReferral%20and%20eTransfer%201/UC0010%20Saudi%20eHealth%20eReferral%20and%20eTransfer%20Interoperability%20Use%20Case%20v1.0.pdf (accessed on 9 May 2022).
- Patel, M.P.; Schettini, P.; O’Leary, C.P.; Bosworth, H.B.; Anderson, J.B.; Shah, K.P. Closing the Referral Loop: An Analysis of Primary Care Referrals to Specialists in a Large Health System. J. Gen. Intern. Med. 2018, 33, 715–721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Donnell, C.A. Variation in GP referral rates: What can we learn from the literature? Fam. Pract. 2000, 17, 462–471. [Google Scholar] [CrossRef] [PubMed]
- Disler, R.; Glenister, K.; Wright, J. Rural chronic disease research patterns in the United Kingdom, United States, Canada, Australia and New Zealand: A systematic integrative review. BMC Public Health 2020, 20, 770. [Google Scholar] [CrossRef] [PubMed]
- Burke, F.J.; Goodall, C.A.; Hayes, F. Appropriate and inappropriate referrals to a unit of conservative dentistry. Prim. Dent. Care 1999, 6, 141–144. [Google Scholar] [PubMed]
- Kourkouta, S.; Darbar, U.R. An audit of the quality and content of periodontal referrals and the effect of implementing referral criteria. Prim. Dent. Care 2006, 13, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Pierscionek, T.J.; Moore, J.E.; Pierscionek, B.K. Referrals to ophthalmology: Optometric and general practice comparison. Ophthalmic Physiol. Opt. 2009, 29, 32–40. [Google Scholar] [CrossRef]
- Davey, C.J.; Scally, A.J.; Green, C.; Mitchell, E.S.; Elliott, D. Factors influencing accuracy of referral and the likelihood of false positive referral by optometrists in Bradford, United Kingdom. J. Optom. 2016, 9, 158–165. [Google Scholar] [CrossRef] [Green Version]
- Khou, V.; Ly, A.; Moore, L.; Markoulli, M.; Kalloniatis, M.; Yapp, M.; Hennessy, M.; Zangerl, B. Review of referrals reveal the impact of referral content on the triage and management of ophthalmology wait lists. BMJ Open 2021, 11, e047246. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographic and Referrals Characteristics | Total N(%) | Distance of the Referred Hospital N (%) or m ± SD a | p-Value | ||
|---|---|---|---|---|---|
| ≤13 km Zone | >13 km Zone | ||||
| No. of Primary healthcare centres | 9 (100) | 5(55.6) | 4 (44.4) | - | |
| PHC visits to referrals ratio | 16:1 | 14.5:1 | 20.4:1 | - | |
| Number of referrals | 52,143 (100) | 40,060 (76.8) | 12,083 (23.2) | - | |
| Documented scheduled appointment | Yes | 45,697 (87.6) | 35,305 (67.7) | 10,392 (20) | 0.001 * |
| No | 6446 (12.4) | 4755 (9) | 1691 (3.2) | ||
| Referral’s urgency | Urgent | 10,384 (20) | 7237 (14) | 3147 (6) | 0.001 * |
| Non-urgent | 41,759 (80) | 32,823(63) | 8936 (17) | ||
| Patient’s age (years) b | 40.5 ± 18.4 | 41.5 ± 18.4 | 37.3 ± 17.8 | 0.001 * | |
| Gender | Males | 22,869 (44) | 17,553 (33.7) | 5316 (10.2) | 0.728 |
| Females | 29,273 (56) | 22,507 (43.2) | 6767 (13) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alabbasi, K.H.; Kruger, E.; Tennant, M. Strengthening Saudi Arabia’s Primary Health Care through an e-Referral System: A Case Study. Clin. Pract. 2022, 12, 374-382. https://doi.org/10.3390/clinpract12030042
Alabbasi KH, Kruger E, Tennant M. Strengthening Saudi Arabia’s Primary Health Care through an e-Referral System: A Case Study. Clinics and Practice. 2022; 12(3):374-382. https://doi.org/10.3390/clinpract12030042
Chicago/Turabian StyleAlabbasi, Khalid H., Estie Kruger, and Marc Tennant. 2022. "Strengthening Saudi Arabia’s Primary Health Care through an e-Referral System: A Case Study" Clinics and Practice 12, no. 3: 374-382. https://doi.org/10.3390/clinpract12030042
APA StyleAlabbasi, K. H., Kruger, E., & Tennant, M. (2022). Strengthening Saudi Arabia’s Primary Health Care through an e-Referral System: A Case Study. Clinics and Practice, 12(3), 374-382. https://doi.org/10.3390/clinpract12030042