


Developing and Implementing a Narration of Care Framework to Teach Nurses When and How to Narrate Care


{kind=link}
Abstract
1. Introduction
2. Methods
2.1. Developing a Framework
- Conducting a Data Review and Literature Review
- 2.
- Convening a Task Force
- 3.
- Conducting Patient Discussions
- 4.
- Unilateral communication, in which clinical staff speak at or to, rather than with patients, can give the impression that staff are primarily task-oriented rather than person-centered. To address this, NOC must extend beyond one-way patient education and incorporate elements of presence and connection, emphasizing relational engagement over transactional interaction.
- 5.
- NOC would need to include an “uncertainty” component. Anxiety, lack of preparedness, and uncertainty were prominent themes tied to HCAHPS nursing communication scores, particularly questions about “education” and “information”, which suggested that patients viewed nursing staff as being integral to relieving their anxieties and uncertainties through the use of patient education and information, or narration.
- 6.
- NOC would need to include some component of listening. Since our patients noted a perceived lack of attentive behaviors, we knew that non-verbal and verbal behaviors suggesting approachability would need to be incorporated.
- 7.
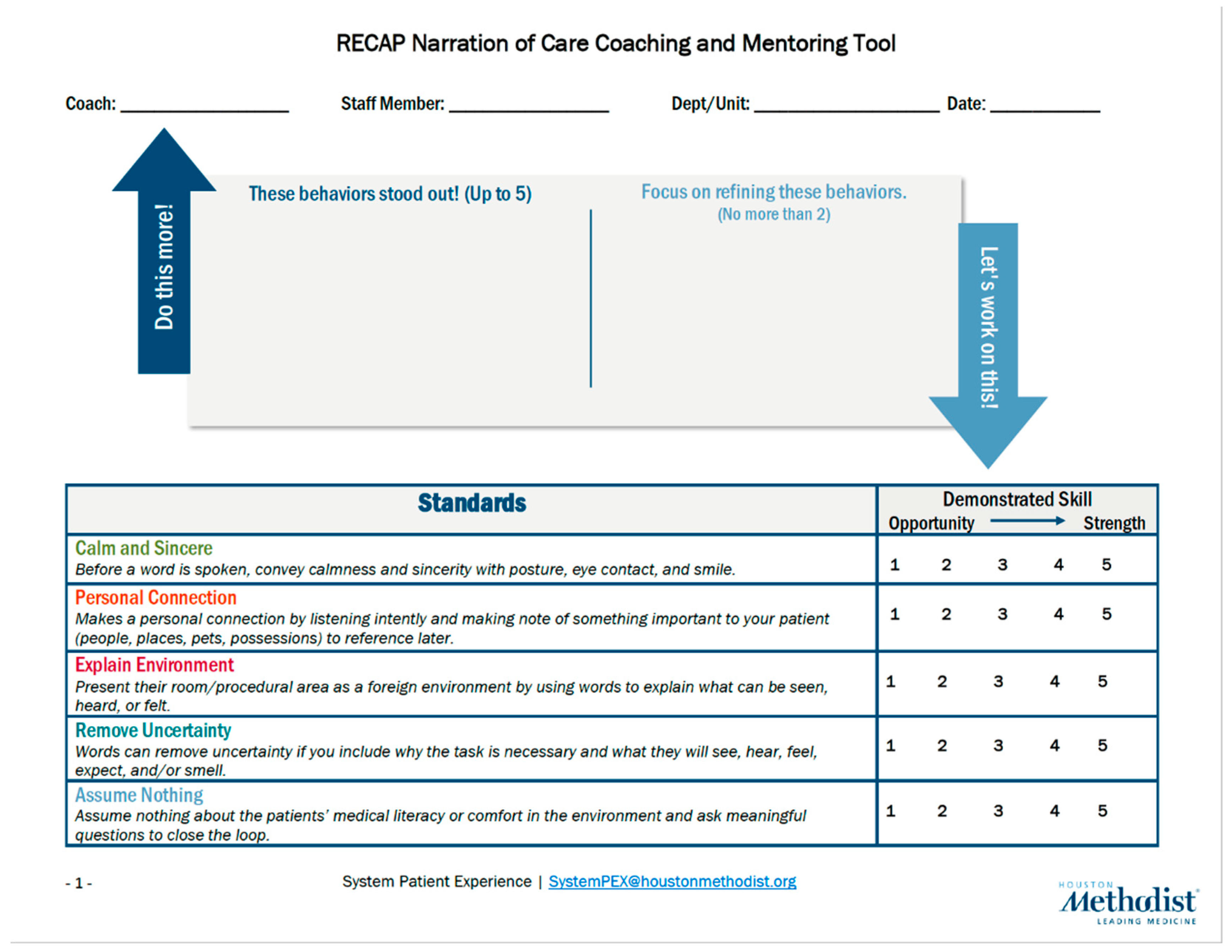
- Formulating a Consensus Framework
- 8.
- Remove Uncertainty: By explaining what we are performing, what the patient can anticipate, and why it is important for their care.
- 9.
- Calm and Sincere: Leave your own negative emotions at the door, including conveying a sense that you are rushed. When speaking with patients, convey calmness in your tone and sincerity with your posture by being open, facing them, moving close, and making eye contact.
- 10.
- Personal Connection: Make a personal connection by making notes of what is important to your patient to reference later and listen intently to matters that concern them. Updating the patient communication board with what they share is most important for them for the day (rest, contacting a family member, etc.). When patients feel cared about, they share concerns and feelings—details that can lead to safer care and better outcomes.
- 11.
- Explain the Environment: By providing the purpose behind equipment, monitor readings, and alarms, and reassuring patients of their safety if an alarm is triggered or readings vary.
- 12.
- Assume Nothing: Just because your patient has been in the hospital before, is a healthcare worker, has higher education, or has chronic conditions, do not assume they are confident and proficient in their state of being or care. Always give clear verbal information to describe what is happening, what to expect, and why it is occurring, so that the patient is able to understand.
- The “R” in RECAP stands for removing uncertainty.
- The “E” in RECAP stands for explaining the environment.
- The “C” in RECAP stands for being calm and sincere.
- The “A” in RECAP stands for assume nothing.
- The “P” in RECAP stands for personal connection.
2.2. Designing the NOC Course
3. Results
Assessing the Outcomes
- Narrate the side effects of medications;
- Narrate why you are turning off alarms, and whether the readings are normal or not;
- Narrate intravenous flushing with saline and potential discomforts it may cause;
- Narrate pain management plans—what you will do to address pain needs, within what timeframes, how you will reassess pain needs, and when you will escalate.
4. Discussion
5. Conclusions and Future Research
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Public Involvement Statement
Guidelines and Standards Statement
Use of Artificial Intelligence
Acknowledgments
Conflicts of Interest
Appendix A
References
- Watson, J. Nursing: The Philosophy and Science of Caring, Revised ed.; Springer Publishing Company: New York, NY, USA, 2008. [Google Scholar] [CrossRef]
- Feo, R.; Conroy, T.; Wiechula, R.; Rasmussen, P.; Frensham, L.; Kitson, A. Instruments Measuring Behavioral Aspects of the Nurse-Patient Relationship. JBI Database Syst. Rev. Implement. Rep. 2018, 16, 1939–1946. [Google Scholar] [CrossRef] [PubMed]
- Peplau, H.E. Peplau’s Theory of Interpersonal Relations. Nurs. Sci. Q. 1997, 10, 162–167. [Google Scholar] [CrossRef] [PubMed]
- Peplau, H.E. Interpersonal Relations: A Theoretical Framework for Application in Nursing Practice. Nurs. Sci. Q. 1992, 5, 13–18. [Google Scholar] [CrossRef] [PubMed]
- Langley, G.L.; Moen, R.; Nolan, K.M.; Nolan, T.W.; Norman, C.L.; Provost, L.P. The Improvement Guide: A Practical Approach to Enhancing Organizational Performance, 2nd ed.; Jossey-Bass Publishers: San Francisco, CA, USA, 2009. [Google Scholar]
- Centers for Medicare & Medicaid Services, Baltimore, MD. Available online: https://www.hcahpsonline.org (accessed on 9 June 2025).
- Strauss, A.; Corbin, J.M. Basics of Qualitative Research: Grounded Theory Procedures and Techniques; Sage Publications: Thousand Oaks, CA, USA, 1990. [Google Scholar]
- Wang, S.; Liu, K.; Shi, Z.; Chen, Q.; Tang, S. Instruments for Measuring Patient Health Education Competence among Nursing Personnel: Protocol for a COSMIN-Based Systematic Review. BMJ Open 2023, 13, e072905. [Google Scholar] [CrossRef] [PubMed]
- Johnson, A.M.; Brimhall, A.S.; Johnson, E.T.; Hodgson, J.; Didericksen, K.; Pye, J.; Harmon, G.J.C.; Sewell, K.B. A Systematic Review of the Effectiveness of Patient Education through Patient Portals. JAMIA Open 2023, 6, ooac085. [Google Scholar] [CrossRef] [PubMed]
- McCabe, C. Nurse-Patient Communication: An Exploration of Patients’ Experiences. J. Clin. Nurs. 2004, 13, 41–49. [Google Scholar] [CrossRef] [PubMed]
- Moy, A.J.; Schwartz, J.M.; Chen, R.; Sadri, S.; Lucas, E.; Cato, K.D.; Rossetti, S.C. Measurement of Clinical Documentation Burden among Physicians and Nurses Using Electronic Health Records: A Scoping Review. J. Am. Med. Inform. Assoc. 2021, 28, 998–1008. [Google Scholar] [CrossRef] [PubMed]
- Grosso, S.; Longhini, J.; Tonet, S.; Bernard, I.; Corso, J.; Marchi, D.; Dorigo, L.; Funes, G.; Lussu, M.; Oppio, N.; et al. Prevalence and Reasons for Non-Nursing Tasks as Perceived by Nurses: Findings from a Large Cross-Sectional Study. J. Nurs. Manag. 2021, 29, 2658–2673. [Google Scholar] [CrossRef] [PubMed]
- Bekker, M.; Coetzee, S.K.; Klopper, H.C.; Ellis, S.M. Non-Nursing Tasks, Nursing Tasks Left Undone and Job Satisfaction among Professional Nurses in South African Hospitals. J. Nurs. Manag. 2014, 23, 1115–1125. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.-Y.; Chao, L.-F.; Xiao, X.; Chien, N.-H. Effects of a Simulation-Based Nursing Process Educational Program: A Mixed-Methods Study. Nurse Educ. Pract. 2021, 56, 103188. [Google Scholar] [CrossRef] [PubMed]
- Vogel, D.; Meyer, M.; Harendza, S. Verbal and Non-Verbal Communication Skills Including Empathy during History Taking of Undergraduate Medical Students. BMC Med. Educ. 2018, 18, 157. [Google Scholar] [CrossRef] [PubMed]
- Shorey, S.; Ang, E.; Yap, J.; Ng, E.D.; Lau, S.T.; Chui, C.K. A Virtual Counseling Application Using Artificial Intelligence for Communication Skills Training in Nursing Education: Development Study. J. Med. Internet Res. 2019, 21, e17064. [Google Scholar] [CrossRef] [PubMed]
- Cortés-Rodríguez, A.E.; López-Rodríguez, M.M.; Roman, P.; Granero-Molina, J.; Fernández-Sola, C.; Hernández-Padilla, J.M. Effect of Two Teaching Methods on Nursing Students’ Acquisition of Patient-Centered Communication Competence in Older People Care: A Cluster Randomized Trial. Front. Public Health 2024, 12, 1510620. [Google Scholar] [CrossRef] [PubMed]
- Young, S.D.; Guo, K.L. Cultural Diversity Training The Necessity of Cultural Competence for Health Care Providers and in Nursing Practice. Health Care Manag. 2020, 39, 100–108. [Google Scholar] [CrossRef] [PubMed]
- Kataoka-Yahiro, M.R.; McFarlane, S.; Koijane, J.; Li, D. Culturally Competent Palliative and Hospice Care Training for Ethnically Diverse Staff in Long-Term Care Facilities. Am. J. Hosp. Palliat. Med. 2017, 34, 335–346. [Google Scholar] [CrossRef] [PubMed]
- Campbell, A.R.; Layne, D.; Scott, E.; Wei, H. Interventions to promote teamwork, delegation and communication among registered nurses and nursing assistants: An integrative review. J. Nurs. Manag. 2020, 28, 1465–1472. [Google Scholar] [CrossRef] [PubMed]
- Hakvoort, L.; Dikken, J.; Cramer-Kruit, J.; van Nieuwenhuyzen, K.M.; van der Schaaf, M.; Schuurmans, M. Factors that influence continuing professional development over a nursing career: A scoping review. Nurse Educ. Pract. 2022, 65, 103481. [Google Scholar] [CrossRef] [PubMed]
- Elwood, W.N. Trust as a Dyadic Mechanism of Action: A Call to Explore Patient-Provider Relationships in the Twenty-First Century. J. Commun. Healthc. 2023, 16, 370–374. [Google Scholar] [CrossRef] [PubMed]
- Allande-Cussó, R.; Fernández-García, E.; Porcel-Gálvez, A.M. Defining and Characterising the Nurse–Patient Relationship: A Concept Analysis. Nurs. Ethics 2021, 29, 462–484. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bruce, C.R.; Zuniga-Georgy, N.N.; Way, N.; Sosa, L.; Javaluyas, E.; Williams, T.L.; Vozzella, G. Developing and Implementing a Narration of Care Framework to Teach Nurses When and How to Narrate Care. Nurs. Rep. 2025, 15, 244. https://doi.org/10.3390/nursrep15070244
Bruce CR, Zuniga-Georgy NN, Way N, Sosa L, Javaluyas E, Williams TL, Vozzella G. Developing and Implementing a Narration of Care Framework to Teach Nurses When and How to Narrate Care. Nursing Reports. 2025; 15(7):244. https://doi.org/10.3390/nursrep15070244
Chicago/Turabian StyleBruce, Courtenay R., Natalie N. Zuniga-Georgy, Nathan Way, Lenis Sosa, Emmanuel Javaluyas, Terrell L. Williams, and Gail Vozzella. 2025. "Developing and Implementing a Narration of Care Framework to Teach Nurses When and How to Narrate Care" Nursing Reports 15, no. 7: 244. https://doi.org/10.3390/nursrep15070244
APA StyleBruce, C. R., Zuniga-Georgy, N. N., Way, N., Sosa, L., Javaluyas, E., Williams, T. L., & Vozzella, G. (2025). Developing and Implementing a Narration of Care Framework to Teach Nurses When and How to Narrate Care. Nursing Reports, 15(7), 244. https://doi.org/10.3390/nursrep15070244