
Nurses’ Engagement in Antimicrobial Stewardship Programmes: A Mapping Review of Influencing Factors Based on Irvine’s Theory



Abstract
1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Types of Sources
2.3. Search Strategy
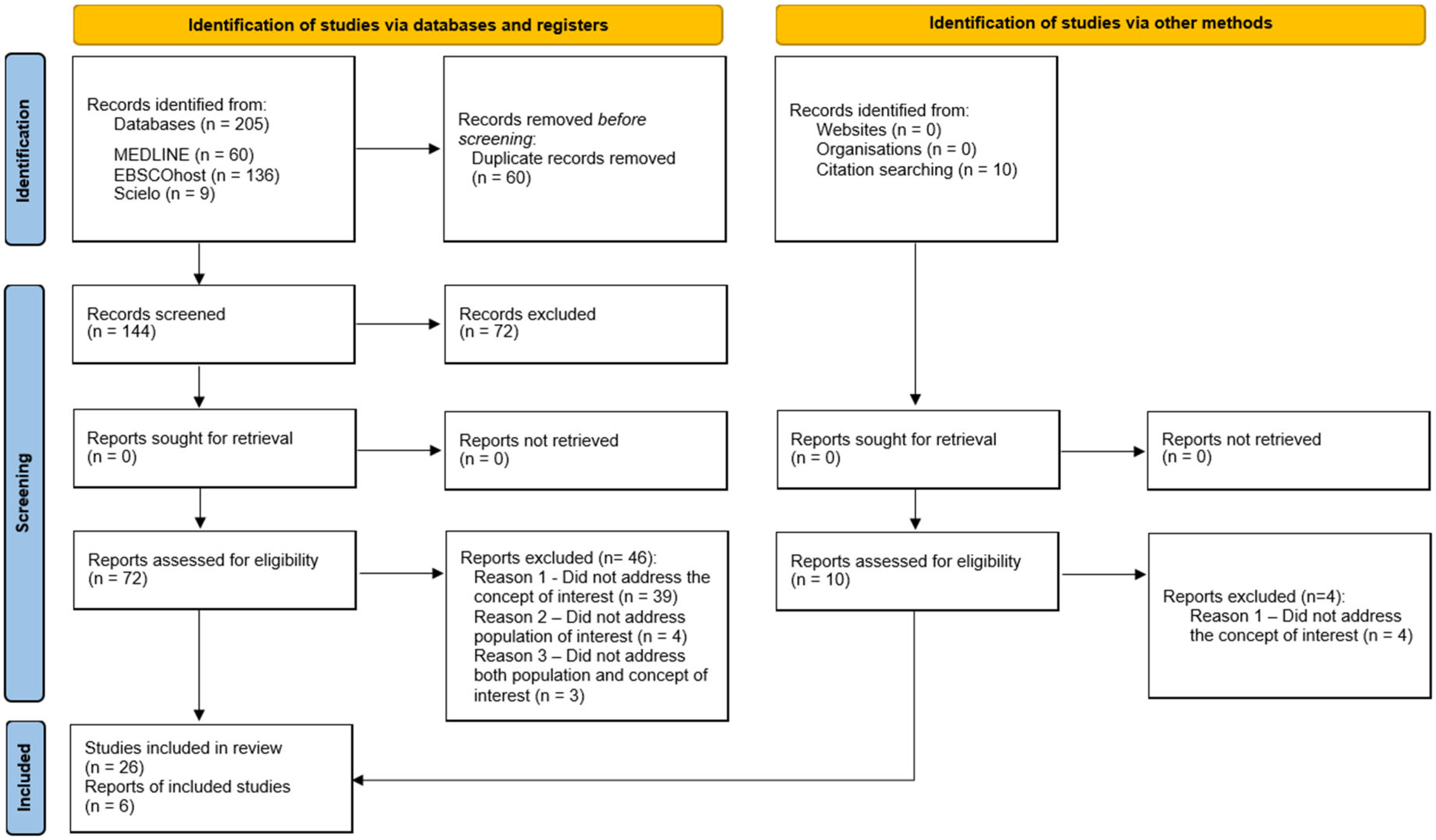
2.4. Source of Evidence Selection
2.5. Data Extraction
2.6. Data Analysis and Presentation
3. Results
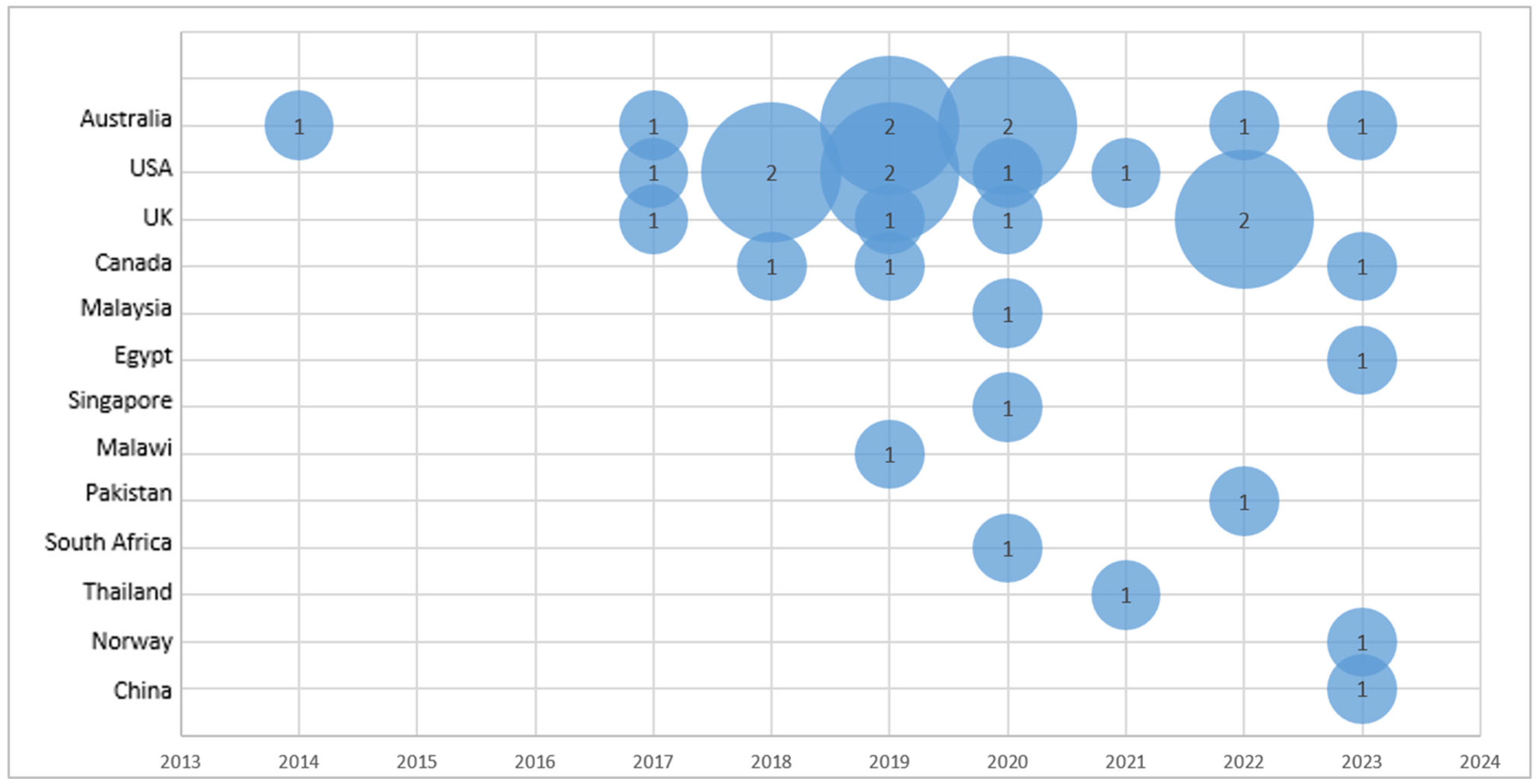
3.1. Characteristics of Included Sources
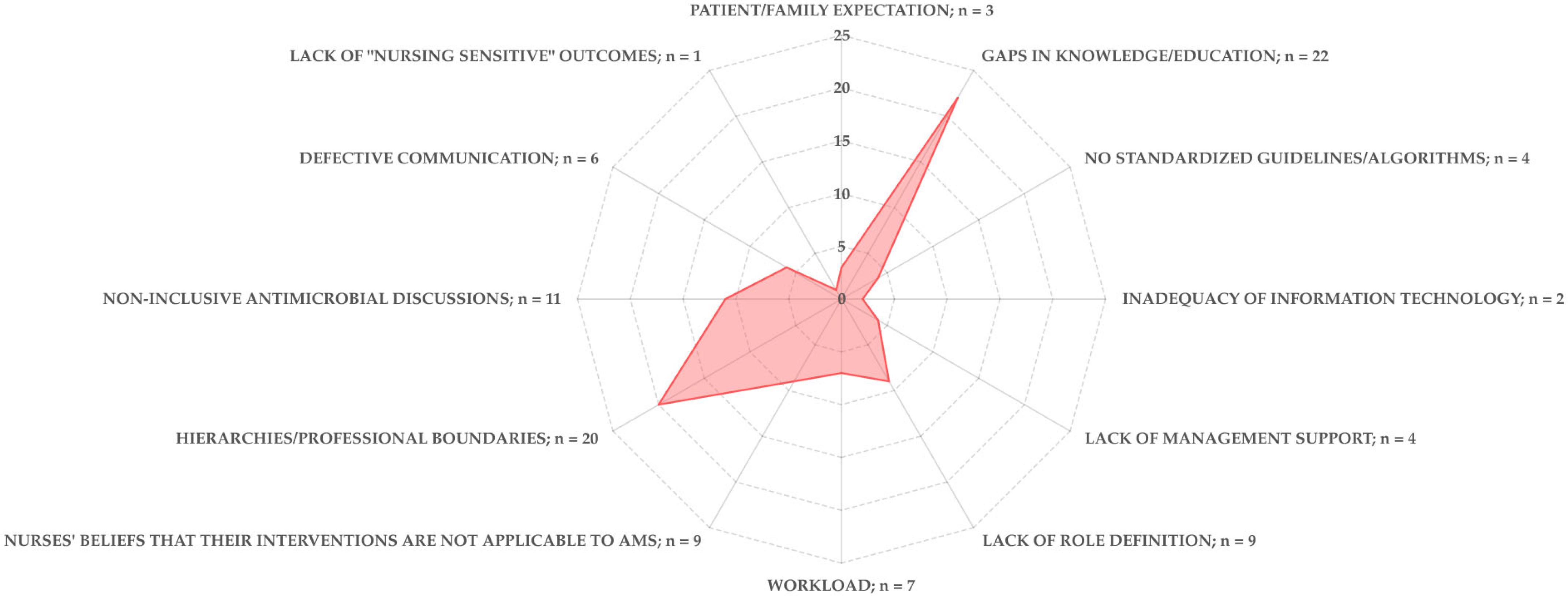
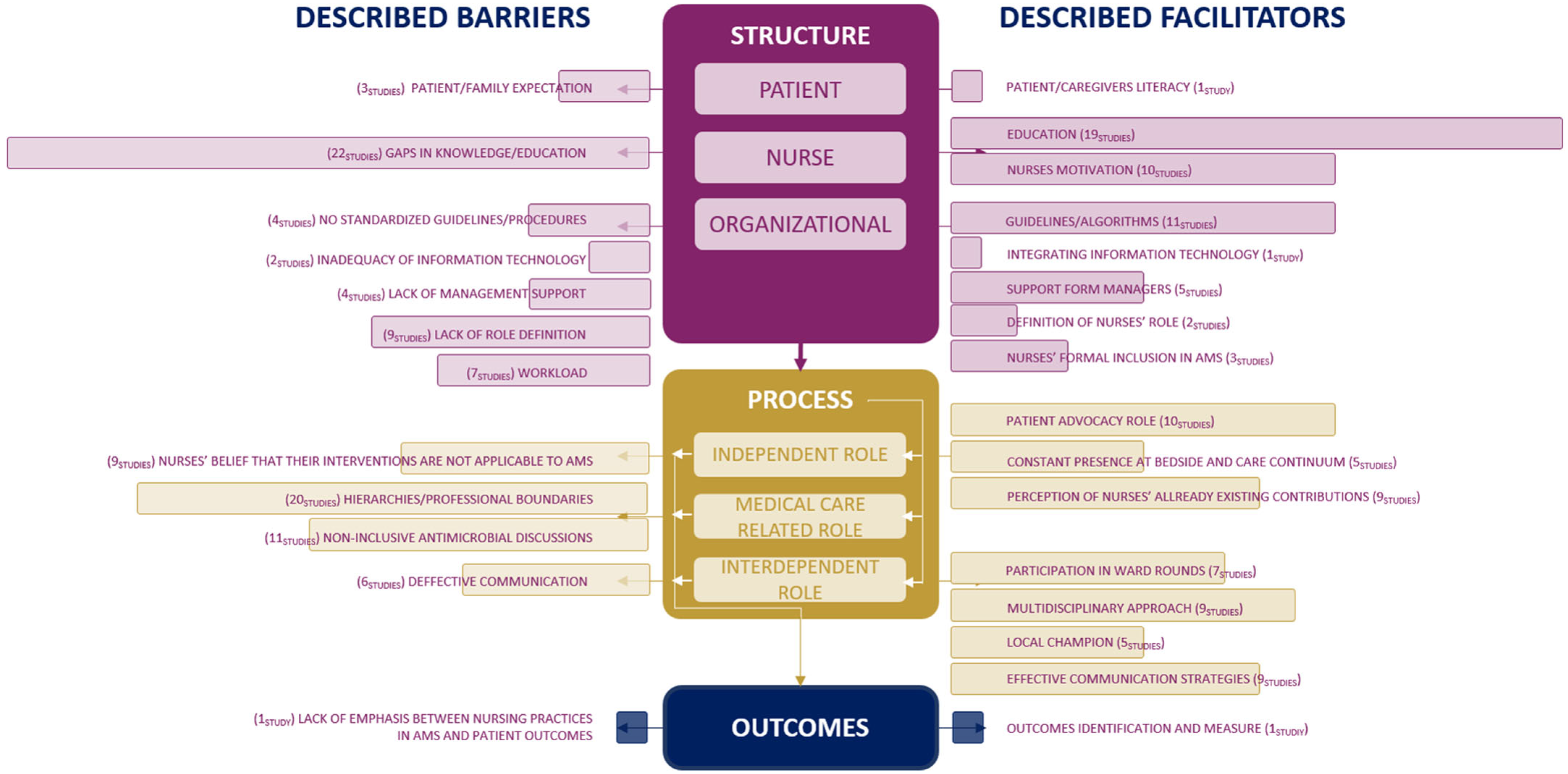
3.2. Barriers to Nurses’ Engagement in AMS Programmes
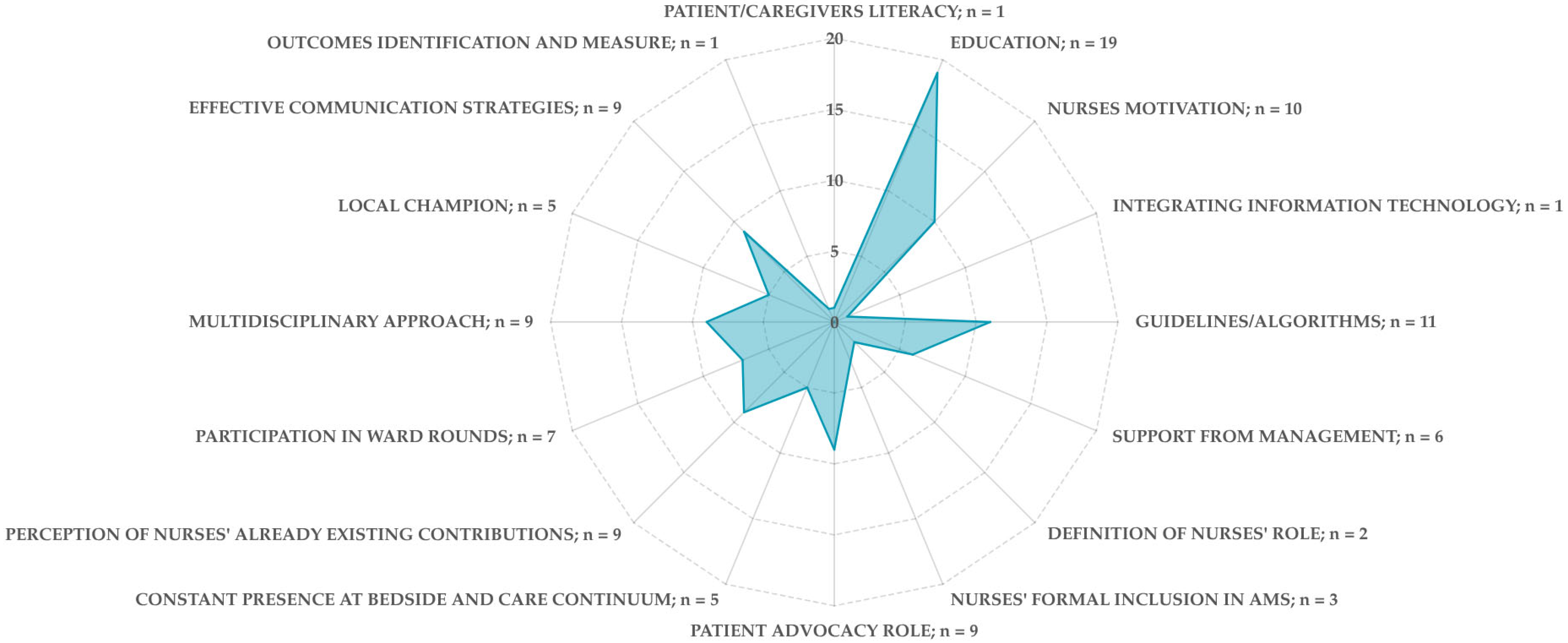
3.3. Facilitators to Nurses’ Engagement in AMS Programmes
3.4. Outcomes Associated with Nurses Engagement in AMS
4. Discussion
4.1. Structure Domain
4.2. Process Domain
4.3. Outcomes
4.4. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Public Involvement Statement
Guidelines and Standards Statement
Conflicts of Interest
References
- WHO. Fact Sheet on Sustainable Development Goals (SDGs): Health Targets—Antimicrobial Resistance; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- Dyar, O.J.; Huttner, B.; Schouten, J.; Pulcini, C. What Is Antimicrobial Stewardship? Clin. Microbiol. Infect. 2017, 23, 793–798. [Google Scholar] [CrossRef] [PubMed]
- Irvine, D.; Sidani, S.; Hall, L.M. Finding Value in Nursing Care: A Framework for Quality Improvement and Clinical Evaluation. Nurs. Econ. 1998, 16, 110. [Google Scholar]
- Sumner, S.; Forsyth, S.; Collette-Merrill, K.; Taylor, C.; Vento, T.; Veillette, J.; Webb, B. Antibiotic Stewardship: The Role of Clinical Nurses and Nurse Educators. Nurse Educ. Today 2018, 60, 157–160. [Google Scholar] [CrossRef] [PubMed]
- Olans, R.N.; Olans, R.D.; DeMaria, A., Jr. The Critical Role of the Staff Nurse in Antimicrobial Stewardship—Unrecognized, but Already There. Clin. Infect. Dis. 2016, 62, 84–89. [Google Scholar] [CrossRef] [PubMed]
- CDC. The Core Elements of Hospital Antibiotic Stewardship Programs; Core Elements of Hospital Antibiotic Stewardship Programs; US Department of Health and Human Services, CDC: Atlanta, GA, USA, 2019.
- Australian Comission on Safety and Quality in Health Care. In Antimicrobial Stewardship in Australian Health Care; ACSQHC: Sydney, Australia, 2018.
- ANA/CDC. Redefining the Antibiotic Stewardship Team: Recommendations from the American Nurses Association/Centers for Disease Control and Prevention Workgroup on the Role of Registered Nurses in Hospital Antibiotic Stewardship Practices. JAC-Antimicrob. Resist. 2017, 1, dlz037. [Google Scholar] [CrossRef]
- Davey, K.; Aveyard, H. Nurses’ Perceptions of Their Role in Antimicrobial Stewardship within the Hospital Environment. An Integrative Literature Review. J. Clin. Nurs. 2022, 31, 3011–3020. [Google Scholar] [CrossRef]
- Irvine, D.; Sidani, S.; Hall, L.M. Linking Outcomes to Nurses’ Roles in Health Care. Nurs. Econ. 1998, 16, 58. [Google Scholar] [PubMed]
- Abbas, S.; Lee, K.; Pakyz, A.; Markley, D.; Cooper, K.; Vanhoozer, G.; Doll, M.; Bearman, G.; Stevens, M.P. Knowledge, Attitudes, and Practices of Bedside Nursing Staff Regarding Antibiotic Stewardship: A Cross-Sectional Study. Am. J. Infect. Control 2019, 47, 230–233. [Google Scholar] [CrossRef]
- Fisher, C.C.; Cox, V.C.; Gorman, S.K.; Lesko, N.; Holdsworth, K.; Delaney, N.; McKenna, C. A Theory-Informed Assessment of the Barriers and Facilitators to Nurse-Driven Antimicrobial Stewardship. Am. J. Infect. Control 2018, 46, 1365–1369. [Google Scholar] [CrossRef] [PubMed]
- Rout, J.; Brysiewicz, P. Perceived Barriers to the Development of the Antimicrobial Stewardship Role of the Nurse in Intensive Care: Views of Healthcare Professionals. S. Afr. J. Crit. Care 2020, 36, 51. [Google Scholar] [CrossRef]
- Danielis, M.; Regano, D.; Castaldo, A.; Mongardi, M.; Buttiron Webber, T. What Are the Nursing Competencies Related to Antimicrobial Stewardship and How They Have Been Assessed? Results from an Integrative Rapid Review. Antimicrob. Resist. Infect. Control 2022, 11, 153. [Google Scholar] [CrossRef] [PubMed]
- Zhao, W.; Guo, W.; Sun, P.; Yang, Y.; Ning, Y.; Liu, R.; Xu, Y.; Li, S.; Shang, L. Bedside Nurses’ Antimicrobial Stewardship Practice Scope and Competencies in Acute Hospital Settings: A Scoping Review. J. Clin. Nurs. 2023, 32, 6061–6088. [Google Scholar] [CrossRef]
- Bonacaro, A.; Solfrizzo, F.G.; Regano, D.; Negrello, F.; Domeniconi, C.; Volpon, A.; Taurchini, S.; Toselli, P.; Baesti, C. Antimicrobial Stewardship in Healthcare: Exploring the Role of Nurses in Promoting Change, Identifying Barrier Elements and Facilitators—A Meta-Synthesis. Healthcare 2024, 12, 2122. [Google Scholar] [CrossRef]
- Campbell, F.; Tricco, A.C.; Munn, Z.; Pollock, D.; Saran, A.; Sutton, A.; White, H.; Khalil, H. Mapping Reviews, Scoping Reviews, and Evidence and Gap Maps (EGMs): The Same but Different—the “Big Picture” Review Family. Syst. Rev. 2023, 12, 45. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Peters, M.D.J.; Godfrey, C.; McInerney, P.; Khalil, H.; Larsen, P.; Marnie, C.; Pollock, D.; Tricco, A.C.; Munn, Z. Best Practice Guidance and Reporting Items for the Development of Scoping Review Protocols. JBI Evid. Synth. 2022, 20, 953–968. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Carter, E.J.; Greendyke, W.G.; Furuya, E.Y.; Srinivasan, A.; Shelley, A.N.; Bothra, A.; Saiman, L.; Larson, E.L. Exploring the Nurses’ Role in Antibiotic Stewardship: A Multisite Qualitative Study of Nurses and Infection Preventionists. Am. J. Infect. Control 2018, 46, 492–497. [Google Scholar] [CrossRef] [PubMed]
- Hamdy, R.F.; Neal, W.; Nicholson, L.; Ansusinha, E.; King, S. Pediatric Nurses’ Perceptions of Their Role in Antimicrobial Stewardship: A Focus Group Study. J. Pediatr. Nurs. 2019, 48, 10–17. [Google Scholar] [CrossRef]
- Hendy, A.; Al-Sharkawi, S.; Hassanein, S.M.A.; Soliman, S.M. Effect of Educational Intervention on Nurses’ Perception and Practice of Antimicrobial Stewardship Programs. Am. J. Infect. Control 2023, 51, 41–47. [Google Scholar] [CrossRef]
- Monsees, E.; Popejoy, L.; Jackson, M.A.; Lee, B.; Goldman, J. Integrating Staff Nurses in Antibiotic Stewardship: Opportunities and Barriers. Am. J. Infect. Control 2018, 46, 737–742. [Google Scholar] [CrossRef] [PubMed]
- Monsees, E.; Lee, B.; Wirtz, A.; Goldman, J. Implementation of a Nurse-Driven Antibiotic Engagement Tool in 3 Hospitals. Am. J. Infect. Control 2020, 48, 1415–1421. [Google Scholar] [CrossRef] [PubMed]
- Mostaghim, M.; Snelling, T.; McMullan, B.J.; Konecny, P. Nurses Are Underutilised in Antimicrobial Stewardship e Results of a Multisite Survey in Paediatric and Adult Hospitals. Infect. Dis. Health 2017, 22, 57–64. [Google Scholar] [CrossRef]
- Mustafa, Z.U.; Manzoor, M.N.; Shahid, A.; Salman, M.; Hayat, K.; Yasmin, K.; Baraka, M.A.; Mathew, S.; Kanwal, M.; Parveen, S.; et al. Nurses’ Perceptions, Involvement, Confidence and Perceived Barriers Towards Antimicrobial Stewardship Program in Pakistan: Findings from a Multi-Center, Cross-Sectional Study. J. Multidiscip. Healthc. 2022, 15, 2553–2562. [Google Scholar] [CrossRef]
- Padigos, J.; Reid, S.; Kirby, E.; Anstey, C.; Broom, J. Nursing Experiences in Antimicrobial Optimisation in the Intensive Care Unit: A Convergent Analysis of a National Survey. Aust. Crit. Care 2023, 36, 769–781. [Google Scholar] [CrossRef]
- Tangeraas Hansen, M.J.; Storm, M.; Syre, H.; Dalen, I.; Husebø, A.M.L. Attitudes and Self-Efficacy towards Infection Prevention and Control and Antibiotic Stewardship among Nurses: A Mixed-Methods Study. J. Clin. Nurs. 2023, 32, 6268–6286. [Google Scholar] [CrossRef]
- Wilcock, M.; Harding, G.; Moore, L.; Nicholls, I.; Powell, N.; Stratton, J. What Do Hospital Staff in the UK Think Are the Causes of Penicillin Medication Errors? Int. J. Clin. Pharm. 2013, 35, 72–78. [Google Scholar] [CrossRef]
- Wong, L.H.; Bin Ibrahim, M.A.; Guo, H.; Kwa, A.L.H.; Lum, L.H.W.; Ng, T.M.; Chung, J.S.; Somani, J.; Lye, D.C.B.; Chow, A. Empowerment of Nurses in Antibiotic Stewardship: A Social Ecological Qualitative Analysis. J. Hosp. Infect. 2020, 106, 473–482. [Google Scholar] [CrossRef]
- Groumoutis, J.Y.; Gorman, S.K.; Beach, J.E. Identifying Opportunities for Antimicrobial Stewardship in a Tertiary Intensive Care Unit: A Qualitative Study. Can. J. Crit. Care Nurs. 2023, 34, 8–14. [Google Scholar] [CrossRef]
- Lim, C.J.; Kwong, M.; Stuart, R.L.; Buising, K.L.; Friedman, N.D.; Bennett, N.; Cheng, A.C.; Peleg, A.Y.; Marshall, C.; Kong, D.C. Antimicrobial Stewardship in Residential Aged Care Facilities: Need and Readiness Assessment. BMC Infect. Dis. 2014, 14, 410. [Google Scholar] [CrossRef]
- Black, E.K.; MacDonald, L.; Neville, H.L.; Abbass, K.; Slayter, K.; Johnston, L.; Sketris, I. Health Care Providers’ Perceptions of Antimicrobial Use and Stewardship at Acute Care Hospitals in Nova Scotia. Can. J. Hosp. Pharm. 2019, 72, 263–270. [Google Scholar] [CrossRef] [PubMed]
- Broom, J.; Broom, A.; Kirby, E.; Gibson, A.F.; Post, J.J. How Do Hospital Respiratory Clinicians Perceive Antimicrobial Stewardship (AMS)? A Qualitative Study Highlighting Barriers to AMS in Respiratory Medicine. J. Hosp. Infect. 2017, 96, 316–322. [Google Scholar] [CrossRef]
- Charani, E.; Smith, I.; Skodvin, B.; Perozziello, A.; Lucet, J.-C.; Lescure, F.-X.; Birgand, G.; Poda, A.; Ahmad, R.; Singh, S.; et al. Investigating the Cultural and Contextual Determinants of Antimicrobial Stewardship Programmes across Low-, Middle-and High-Income Countries—A Qualitative Study. PLoS ONE 2019, 14, e0209847. [Google Scholar] [CrossRef] [PubMed]
- Currie, K.; Laidlaw, R.; Ness, V.; Gozdzielewska, L.; Malcom, W.; Sneddon, J.; Seaton, R.A.; Flowers, P. Mechanisms Affecting the Implementation of a National Antimicrobial Stewardship Programme; Multi-Professional Perspectives Explained Using Normalisation Process Theory. Antimicrob. Resist. Infect. Control 2020, 9, 99. [Google Scholar] [CrossRef]
- Ierano, C.; Rajkhowa, A.; Gotterson, F.; Marshall, C.; Peel, T.; Ayton, D.; Thursky, K. Opportunities for Nurse Involvement in Surgical Antimicrobial Stewardship Strategies: A Qualitative Study. Int. J. Nurs. Stud. 2022, 128, 104186. [Google Scholar] [CrossRef] [PubMed]
- Mula, C.T.; Solomon, V.; Muula, A.S. The Examination of Nurses’ Adherence to the ‘Five Rights’ of Antibiotic Administration and Factors Influencing Their Practices: A Mixed Methods Case Study at a Tertiary Hospital, Malawi. Malawi Med. J. 2019, 31, 126–132. [Google Scholar] [CrossRef]
- Nampoothiri, V.; Bonaconsa, C.; Surendran, S.; Mbamalu, O.; Nambatya, W.; Ahabwe Babigumira, P.; Ahmad, R.; Castro-Sanchez, E.; Broom, A.; Szymczak, J.; et al. What Does Antimicrobial Stewardship Look like Where You Are? Global Narratives from Participants in a Massive Open Online Course. JAC Antimicrob. Resist. 2022, 4, dlab186. [Google Scholar] [CrossRef]
- Ren-Zhang, L.; Chee-Lan, L.; Hui-Yin, Y. The Awareness and Perception on Antimicrobial Stewardship among Healthcare Professionals in a Tertiary Teaching Hospital Malaysia. Arch. Pharm. Pract. 2020, 11, 50–59. [Google Scholar]
- van Gulik, N.; Hutchinson, A.; Considine, J.; Driscoll, A.; Malathum, K.; Botti, M. Perceived Roles and Barriers to Nurses’ Engagement in Antimicrobial Stewardship: A Thai Qualitative Case Study. Infect. Dis. Health 2021, 26, 218–227. [Google Scholar] [CrossRef]
- Wilcock, M.; Powell, N.; Underwood, F. Antimicrobial Stewardship and the Hospital Nurse and Midwife: How Do They Perceive Their Role? Eur. J. Hosp. Pharm. 2019, 26, 89–92. [Google Scholar] [CrossRef]
- Goulopoulos, A.; Rofe, O.; Kong, D.; Maclean, A.; O’Reilly, M. Attitudes and Beliefs of Australian Emergency Department Clinicians on Antimicrobial Stewardship in the Emergency Department: A Qualitative Study. Emerg. Med. Australas. 2019, 31, 787–796. [Google Scholar] [CrossRef] [PubMed]
- Monsees, E.; Goldman, J.; Popejoy, L. Staff Nurses as Antimicrobial Stewards: An Integrative Literature Review. Am. J. Infect. Control 2017, 45, 917–922. [Google Scholar] [CrossRef] [PubMed]
- Monsees, E.A.; Tamma, P.D.; Cosgrove, S.E.; Miller, M.A.; Fabre, V. Integrating Bedside Nurses into Antibiotic Stewardship: A Practical Approach. Infect. Control Hosp. Epidemiol. 2019, 40, 579–584. [Google Scholar] [CrossRef]
- Fitzpatrick, E.R.; Pogorzelska-Maziarz, M.; Manning, M.; Gleason, V.M. The Effect of an Educational Program on Nursing Knowledge and Empowerment in Antimicrobial Stewardship in a Surgical Intensive Care Unit. Dimens. Crit. Care Nurs. 2021, 40, 21–28. [Google Scholar] [CrossRef]
- Greendyke, W.G.; Carter, E.J.; Salsgiver, E.; Bernstein, D.; Simon, M.S.; Saiman, L.; Calfee, D.P.; Furuya, E.Y. Exploring the Role of the Bedside Nurse in Antimicrobial Stewardship: Survey Results From Five Acute-Care Hospitals. Infect. Control Hosp. Epidemiol. 2018, 39, 360–362. [Google Scholar] [CrossRef]
- Gotterson, F.; Buising, K.; Manias, E. Nurse Role and Contribution to Antimicrobial Stewardship: An Integrative Review. Int. J. Nurs. Stud. 2021, 117, 103787. [Google Scholar] [CrossRef]
- van Huizen, P.; Kuhn, L.; Russo, P.L.; Connell, C.J. The Nurses’ Role in Antimicrobial Stewardship: A Scoping Review. Int. J. Nurs. Stud. 2021, 113, 103772. [Google Scholar] [CrossRef] [PubMed]
- Chater, A.M.; Family, H.; Abraao, L.M.; Burnett, E.; Castro-Sanchez, E.; Du Toit, B.; Gallagher, R.; Gotterson, F.; Manias, E.; McEwen, J.; et al. Influences on Nurses’ Engagement in Antimicrobial Stewardship Behaviours: A Multi-Country Survey Using the Theoretical Domains Framework. J. Hosp. Infect. 2022, 129, 171–180. [Google Scholar] [CrossRef]
- Mittal, N.; Deswal, H.; Mittal, R.; Sharma, S.; Kaushik, P. An Educational Program on Antimicrobial Resistance and Stewardship for Staff Nurses in a Public Tertiary Care Hospital in India. Infect. Dis. Health 2023, 28, 202–210. [Google Scholar] [CrossRef]
- Gillespie, E.; Rodrigues, A.; Wright, L.; Williams, N.; Stuart, R.L. Improving Antibiotic Stewardship by Involving Nurses. Am. J. Infect. Control 2013, 41, 365–367. [Google Scholar] [CrossRef]
- Castro-Sánchez, E.; Gilchrist, M.; Ahmad, R.; Courtenay, M.; Bosanquet, J.; Holmes, A.H. Nurse Roles in Antimicrobial Stewardship: Lessons from Public Sectors Models of Acute Care Service Delivery in the United Kingdom. Antimicrob. Resist. Infect. Control 2019, 8, 162. [Google Scholar] [CrossRef] [PubMed]
- Wentzel, J.; van Drie-Pierik, R.; Nijdam, L.; Geesing, J.; Sanderman, R.; van Gemert-Pijnen, J.E.W.C. Antibiotic Information Application Offers Nurses Quick Support. Am. J. Infect. Control 2016, 44, 677–684. [Google Scholar] [CrossRef] [PubMed]
- International Council of Nurses. Antimicrobial Resistance Position Statement. Available online: https://www.icn.ch/sites/default/files/inline-files/PS_A_Antimicrobial_resistance_0.pdf (accessed on 27 May 2023).
- Filipe, S.; Martins, T.; Santos-Costa, P.; Paiva-Santos, F.; Castilho, A.; Bastos, C. Effectiveness of A Nurse-Led Multimodal Intervention in Preventing Blood Culture Contamination: A Before-and-After Study. Healthcare 2024, 12, 1735. [Google Scholar] [CrossRef] [PubMed]
- Ajzen, I. The Theory of Planned Behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Raybardhan, S.; Kan, T.; Chung, B.; Ferreira, D.; Bitton, M.; Shin, P.; Das, P. Nurse Prompting for Prescriber-Led Review of Antimicrobial Use in the Critical Care Unit. Am. J. Crit. Care 2020, 29, 71–76. [Google Scholar] [CrossRef]
- Ha, D.R.; Forte, M.B.; Olans, R.D.; OYong, K.; Olans, R.N.; Gluckstein, D.P.; Kullar, R.; Desai, M.; Catipon, N.; Ancheta, V.; et al. A Multidisciplinary Approach to Incorporate Bedside Nurses into Antimicrobial Stewardship and Infection Prevention. Jt. Comm. J. Qual. Patient Saf. 2019, 45, 600–605. [Google Scholar] [CrossRef]
- Pombo, M.H.R.; Gandra, S.; Thompson, D.; Lamkang, A.S.; Pulcini, C.; Laxminarayan, R. Global Core Standards for Hospital Antimicrobial Stewardship Programs: International Perspectives and Future Directions. 2018. Available online: https://onehealthtrust.org/wp-content/uploads/2018/12/Global-Core-Standards-for-Hospital-Antimicrobial-Stewardship-Programs.pdf (accessed on 5 April 2024).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Database | Search | Results Retrieved |
|---|---|---|
| MEDLINE via PubMed | ((Nurses) AND (antimicrobial stewardship) AND (acute care OR healthcare)) AND ((facilitators AND barriers) OR (perception*)) | 60 |
| EBSCOhost Research | (“antimicrobial stewardship” AND nurs*) AND engage* OR (“nurs* perception*” AND “antimicrobial stewardship”) OR “nurs* behaviour*” AND “nurs* role” AND (antibiotic* OR antimicrob*) NOT (patient* OR psyc* OR veterin* OR dent* OR disinfect*) AND (barrier* and facilitator* or enabler*) | 136 |
| Scielo | (*Antibiotic OR Antimicrobial) AND (stewardship OR management) AND (nurses OR nurse OR nursing) AND NOT (veterinary) | 9 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Filipe, S.; Santos-Costa, P.; Bastos, C.; Castilho, A. Nurses’ Engagement in Antimicrobial Stewardship Programmes: A Mapping Review of Influencing Factors Based on Irvine’s Theory. Nurs. Rep. 2025, 15, 216. https://doi.org/10.3390/nursrep15060216
Filipe S, Santos-Costa P, Bastos C, Castilho A. Nurses’ Engagement in Antimicrobial Stewardship Programmes: A Mapping Review of Influencing Factors Based on Irvine’s Theory. Nursing Reports. 2025; 15(6):216. https://doi.org/10.3390/nursrep15060216
Chicago/Turabian StyleFilipe, Susana, Paulo Santos-Costa, Celeste Bastos, and Amélia Castilho. 2025. "Nurses’ Engagement in Antimicrobial Stewardship Programmes: A Mapping Review of Influencing Factors Based on Irvine’s Theory" Nursing Reports 15, no. 6: 216. https://doi.org/10.3390/nursrep15060216
APA StyleFilipe, S., Santos-Costa, P., Bastos, C., & Castilho, A. (2025). Nurses’ Engagement in Antimicrobial Stewardship Programmes: A Mapping Review of Influencing Factors Based on Irvine’s Theory. Nursing Reports, 15(6), 216. https://doi.org/10.3390/nursrep15060216