
Design, Implementation, and Adaptation of a Tutoring Program for the Competency Development of New Nurses in a Hospital Emergency Department

 , , ,
, , ,
Abstract
1. Introduction
1.1. Problem Description
1.2. Available Knowledge
1.3. Rationale
1.4. Aim
2. Materials and Methods
2.1. Context
2.2. Interventions and Study of the Interventions
2.2.1. Define the Competency Profile of the Figure of the Tutor
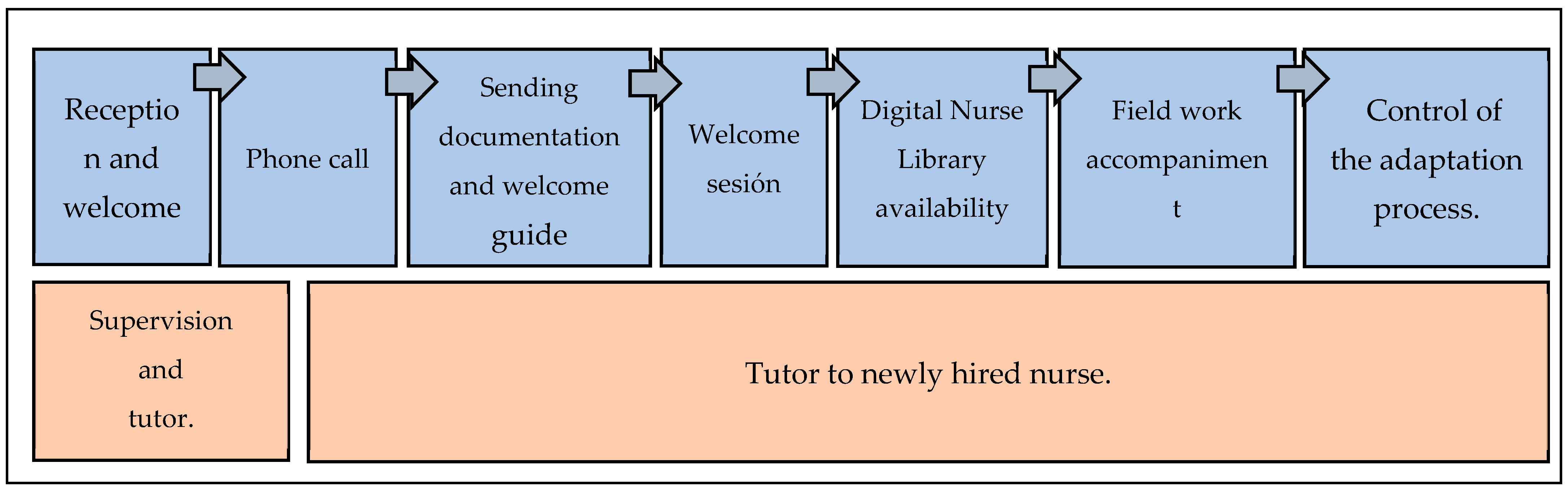
2.2.2. Reception and Tutoring Program Aimed at New Nurses in Hospital Emergency Department
2.3. Measures
2.4. Analysis
2.5. Ethical Considerations
3. Results
- -
- Initiative Autonomy: Initiative autonomy is the ability to act proactively and devise and implement solutions to new problems and/or challenges, with decisiveness and independence of judgment. It implies the ability to respond quickly, effectively, and efficiently to new requirements. All this is achieved by making the most of the resources and opportunities that arise in the environment.
- -
- Effective Communication: Effective communication is the ability to actively listen and clearly transmit to users, family members, and professionals the appropriate information for their needs and demands and to maintain open communication channels that guarantee their rights and duties dictated by the organization.
- -
- Pressure Tolerance: Pressure tolerance is the ability to respond and work effectively under adverse conditions, weather, or overload, in situations of high demand and pressure. It involves the ability to relieve stress in a way that is acceptable to the individual, other people, and the organization. It is the ability to control personal emotions and avoid negative reactions to provocations, opposition, or hostility from others or when working under stressful conditions.
- -
- Teamwork: Teamwork is the ability to collaborate with others, be part of a group, and work with other areas of the organization in order to achieve, together, the organizational strategy, subordinating personal interests to group objectives. It involves having positive expectations of others, understanding others, and creating and maintaining a good work environment.
Technical Competencies and Skills Assessment Rubrics
- -
- All rubrics will be applied with reference to the test for which they have been designed and to the activity that the assessed staff develops in front of the assessor in terms of practical skills.
- -
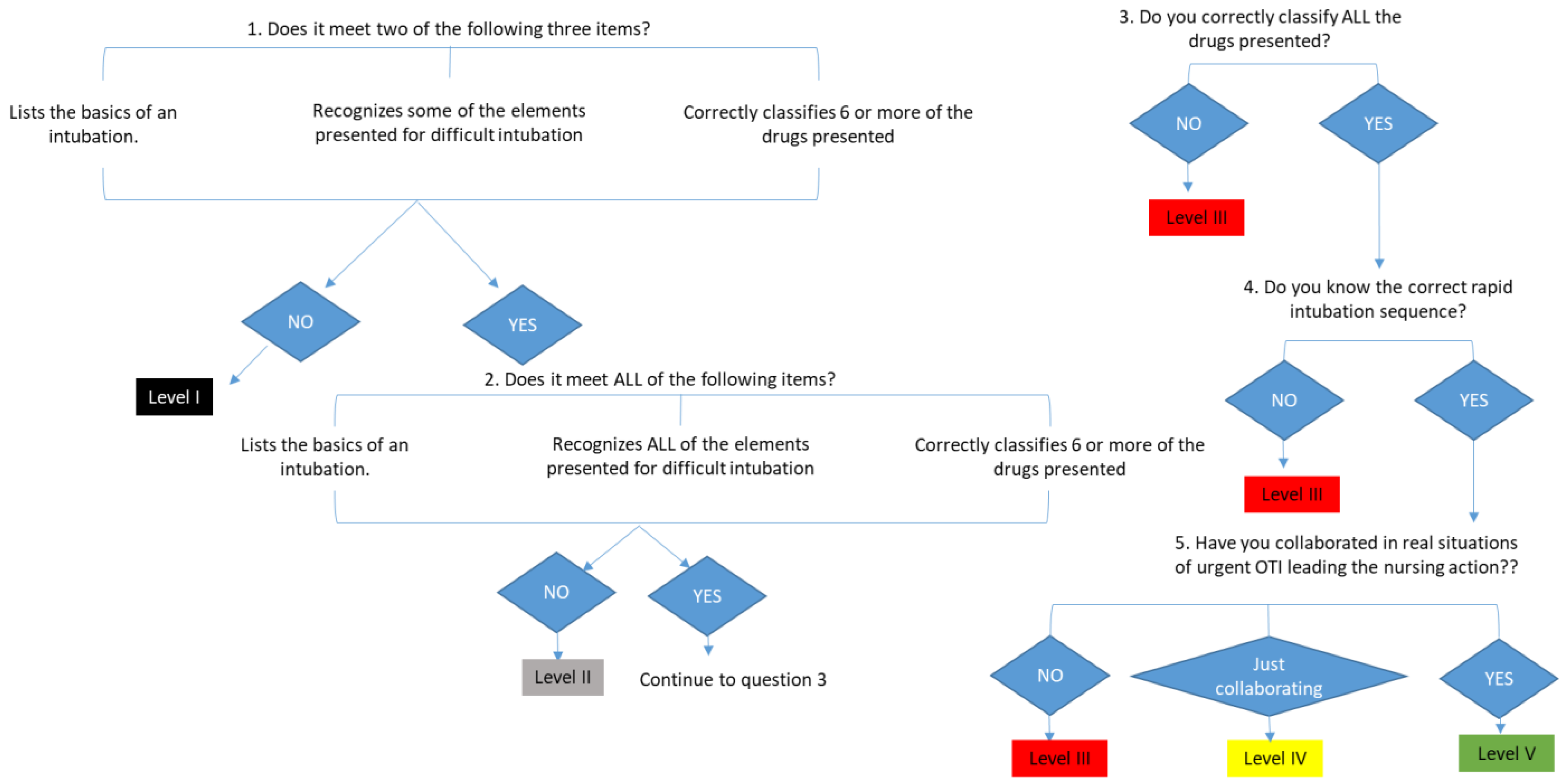
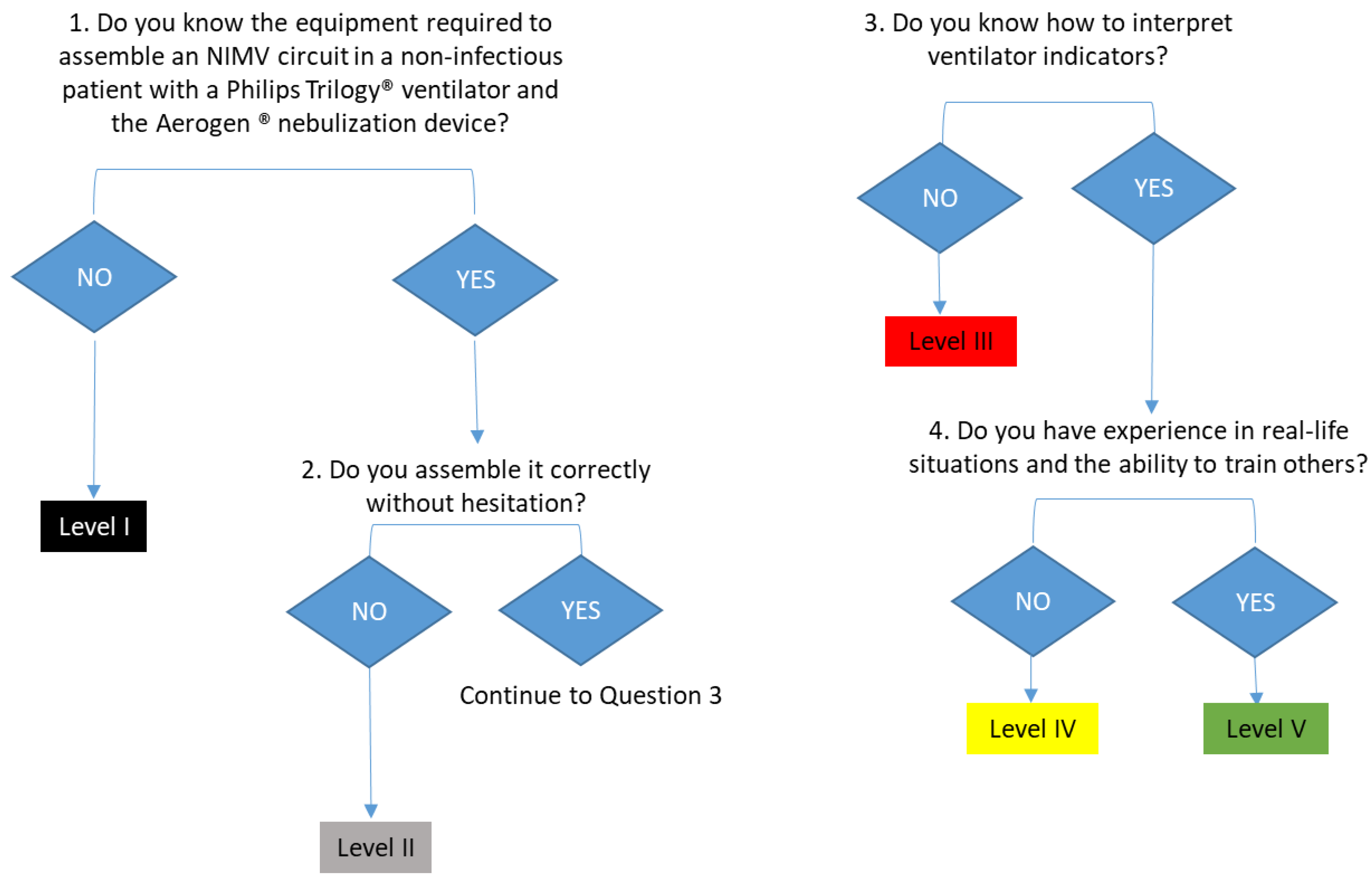
- Competency level assignment diagrams have been developed to help in the application of the evaluation rubric for each technique. In its implementation, it is clarified that the competency level of competence is acquired when one has the theoretical knowledge and is able to imitate a pattern in the simulated test. One is considered to reach the level of efficiency when, in addition, one presents competence and adds an intuitive and general vision of the test one faces, anticipating complications and showing skill in the competencies and skills to be evaluated. And finally, to acquire an expert level, one must have experienced a real situation in a work environment, and have the ability to train other colleagues.
- -
- One must go through all the scenarios that make up the test, keeping the numerical order reflected in each section of the evaluation diagram.
- -
- If all the requirements necessary to assign a competency level accurately are not met, the immediately preceding level will be assigned.
- 2.
4. Discussion
- -
- Detect both individual and group learning needs, taking into account the cognitive, psychomotor, and affective abilities and characteristics of individuals.
- -
- Include in education programs specific aspects related to the prevention of complications and detection of signs and symptoms, as well as the essential initial action.
- -
- Develop teaching activities aimed at nurses and other professionals aimed at strengthening competencies in care aspects in the field of urgencies and emergencies.
5. Strengths and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Public Involvement Statement
Guidelines and Standards Statement
Use of Artificial Intelligence
Conflicts of Interest
References
- Bernués, L.; Peya, M. Libro Blanco. Título de Grado de Enfermería; Agencia Nacional de Evaluación de la Calidad y la Acreditación (ANECA): Madrid, Spain, 2004.
- Benner, P. From Novice to Expert: Excellence and Power in Clinical Nursing Practice; Adisson-Wesley: Menlo Park, CA, USA, 1984. [Google Scholar]
- Benner, P.; Tanner, C.A.; Chesla, C.A. Entering the Field: Advanced beginner practice. In Expertise in Nursing Practice: Caring, Clinical Judgment, and Ethics; Benner, P., Tanner, C.A., Chesla, C.A., Eds.; Springer: New York, NY, USA, 1996; pp. 44–77. [Google Scholar]
- Shearer, J.; Lasonen, J. Critical Practice Study of Nursing Evaluated by Teachers. Int. J. Res. Vocat. Educ. Train. (IJRVET) 2018, 5, 130–139. [Google Scholar] [CrossRef]
- Nielsen, K.; Finderup, J.; Brahe, L.; Elgaard, R.; Elsborg, A.M.; Engell-Soerensen, V.; Holm, L.; Juul, H.; Sommer, I. The art of preceptorship. A qualitative study. Nurse Educ. Pract. 2017, 26, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Myers, S.; Reidy, P.; French, B.; McHale, J.; Chisholm, M.; Griffin, M. Safety concerns of hospital-based new-to-practice registered nurses and their preceptors. J. Contin. Educ. Nurs. 2010, 41, 163–171. [Google Scholar] [CrossRef]
- Arrowsmith, V.; Lau-Walker, M.; Norman, I.; Maben, J. Nurses’ perceptions and experiences of work role transitions: A mixed methods systematic review of the literature. J. Adv. Nurs. 2016, 72, 1735–1750. [Google Scholar] [CrossRef] [PubMed]
- Colina, L.; Sawatzky, J.A.V. Transitioning into the Nurse Practitioner Role through Mentorship. J. Prof. Nurs. 2011, 27, 161–167. [Google Scholar]
- Kumaran, S.; Carney, M. Role transition from student nurse to staff nurse: Facilitating the transition period. Nurse Educ. Pr. 2014, 14, 605–611. [Google Scholar] [CrossRef]
- Marrero, C.M.; García, A.M. Narratives belonging to nurses graduated from the University of La Laguna on how to improve their incorporation into the world of work in Tenerife. Ene 2017, 11, 2–10. [Google Scholar]
- Ten Hoeve, Y.; Kunnen, S.; Brouwer, J.; Roodbol, P.F. The voice of nurses: Novice nurses’ first experiences in a clinical setting. A longitudinal diary study. J. Clin. Nurs. 2018, 27, 1612–1626. [Google Scholar] [CrossRef]
- Jaime-Baron, L.E.; Reyes-vargas, L.I.; Paredes-casas, L.I. Diagnosis of the onboarding process of personnel at E.S.E. Santiago de Tunja. Rev. Pens Acc. Pedagog. Technol. Univ. Colomb. 2022, 32, 2–19. [Google Scholar] [CrossRef]
- Guardado López, S.C.; Martínez Flores, J.; Tapia Torres, D.E. Talent retención: Onboarding proposal in a manufacturing company in Estado de Mexico. Iberoam. Bus. J. 2023, 6, 76–94. [Google Scholar] [CrossRef]
- Onboarding in a Box. Onboarding Kit. Company Linkedin. Available online: https://onx.la/31f7c (accessed on 16 June 2023).
- Camacho, R.; García, Y.; Calvo, G.; Carrasco, A.L.; Gómez, J. Clinical mentoring in the development of nursing professionals’ competencies: A view from the United Kingdom. Index Enferm. 2011, 20, 101–105. [Google Scholar] [CrossRef]
- Lleixà, M.; Gisbert, M.; Marqués, L.; Espuny, C. Diseño de un programa de e-tutoría para favorecer la inserción laboral de los profesionales noveles de enfermería. Pixel-Bit. Rev. Medios Educ. 2011, 38, 23–34. Available online: https://www.researchgate.net/publication/50997431 (accessed on 13 June 2019).
- El Haddad, M.; Moxham, L.; Broadbent, M. Graduate nurse practice readiness: A conceptual understanding of an age old debate. Collegian 2017, 24, 391–396. [Google Scholar] [CrossRef]
- Regan, S.; Wong, C.; Laschinger, H.K.; Cummings, G.; Leiter, M.; MacPhee, M.; Rhéaume, A.; Ritchie, J.A.; Wolff, A.C.; Jeffs, L.; et al. Starting Out: Qualitative perspectives of new graduate nurses and nurse leaders on transition to practice. J. Nurs. Manag. 2017, 25, 246–255. [Google Scholar] [CrossRef] [PubMed]
- Anderson, N.E.; Kent, B.; Owens, R.G. Experiencing patient death in clinical practice: Nurses’ recollections of their earliest memorable patient death. Int. J. Nurs. Stud. 2015, 52, 695–704. [Google Scholar] [CrossRef] [PubMed]
- Lleixá, M.; Gisbert, M.; Marqués, L.; Albacar, N.; Monteso, P. ¿Qué piensan los futuros profesionales de enfermería sobre la inserción laboral? Metas Enfermería 2010, 13, 50–60. Available online: https://dialnet.unirioja.es/servlet/articulo?codigo=3240537http://search.ebscohost.com.roble.unizar.es:9090/login.aspx?drect=true&db=edsdnp&AN=edsdnp.3240537ART&lang=es&site=eds-live (accessed on 13 June 2019).
- Ferrer, F. Estrés en profesionales de enfermería de nueva incorporación. Rev. Rol. Enfermería 2001, 24, 177–180. [Google Scholar]
- Winslow, S.; Almarode, M.; Cottingham, S.; Lowry, K.; Walker, K. New graduates in the emergency department: Could you, would you, should you? J. Emerg. Nurs. 2009, 35, 521–524. [Google Scholar] [CrossRef]
- Freeling, M.; Parker, S. Exploring experienced nurses’ attitudes, views and expectations of new graduate nurses: A critical review, Australia, 2014. Nurse Educ. Todday 2015, 35, e42–e49. [Google Scholar] [CrossRef]
- North, A.; Johnson, J.; Knotts, K.; Whelan, L. Ground instability with mentoring. Nurs Manag. 2006, 37, 16–18. [Google Scholar] [CrossRef]
- Jones, S.J. Establishing a Nurse Mentor Program to Improve Nurse Satisfaction and Intent to Stay. J. Nurses Prof. Dev. 2017, 33, 76–78. [Google Scholar] [CrossRef] [PubMed]
- Burr, S.; Stichler, J.F.; Poeltler, D. Establishing a Mentoring Program: Transforming Organizational Culture and Improving Nurse Retention. Nurs. Womens Health. 2011, 15, 214–224. [Google Scholar] [CrossRef] [PubMed]
- Sánchez, J.; Bueno, A. Factores asociados al uso inadecuado de un servicio de urgencias hospitalario. Emergencias 2005, 17, 138–144. [Google Scholar]
- Lafuente-Robles, N.; Fernández-Salazar, S.; Rodríguez Gómez, S.; Casado-Mora, M.; Morales Asencio, J.M.; Ramos-Morcillo, A. Desarrollo competencial de las enfermeras en el sistema sanitario público de Andalucía. Enfermeria Clin. 2019, 29, 83–89. [Google Scholar] [CrossRef]
- International Council of Nurses. Advanced Practice Nursing Guidelines 2020. Available online: http://www.icn.ch (accessed on 7 February 2023).
- Alles, M. Dictionary of Competencies: The Trilogy—Vol 1: The 60 Most Used Competencies in Competency Management; Gránica: Buenos Aires, Argentina, 2015. [Google Scholar]
- Erickson, M.; Yee, A.M.; Krauter, R.; Hoffman, T. The impact of a structured onboarding program for newly hired nurse practitioners and physician assistants. J. Am. Assoc. Nurse Pract. 2023, 35, 265–271. [Google Scholar] [CrossRef]
- Valdes, E.G.; Sembar, M.C.; Sadler, F. Onboarding New Graduate Nurses Using Assessment-Driven Personalized Learning to Improve Knowledge, Critical Thinking, and Nurse Satisfaction. J. Nurses Prof. Dev. 2023, 39, 18–23. [Google Scholar] [CrossRef]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Remor, E. Psychometric properties of the Spanish version of the Perceived Stress Scale (PSS). Span. J. Psychol. 2006, 9, 86–93. [Google Scholar] [CrossRef]
- Calderón, C.; Gómez, N.; López, F.; Otárola, N.; Briceño, M. Factorial structure of the perceived stress scale (PSS) in a sample of Chilean workers. Salud Soc. 2017, 8, 218–226. [Google Scholar]
- Cabezas, C. Burnout syndrome, work-related stress and professional quality of life. Form. Méd. Cont. Pri. 1998, 5, 491–492. [Google Scholar]
- Grimaldo, Μ.; Reyes, M.A. Quality of life and sleep in professionals in Lima. Rev. Latinoam. Psicol. 2015, 47, 50–57. [Google Scholar]
- Martín, J.; Cortés, J.A.; Morente, M.; Caboblanco, M.; Garijo, J.; Rodriguez, A. Metric characteristics of the Professional Quality of Life Questionnaire (CVP-35). Gac. Sanit. 2004, 18, 129–136. [Google Scholar] [CrossRef] [PubMed]
- Fernández, A.M.; Santa Clotilde, E.; Casado del Olmo, M.I. Quality of Professional Life of Nursing Professionals in Primary Care in Soria. Bibl. Las. Casas 2007, 3, 3–30. Available online: http://www.index-f.com/lascasas/documentos/lc0213.php (accessed on 24 January 2020).
- Lluch-Molins, L.; Cano-García, E. Design and validation of an instrument for the assessment of competencies within the framework of teacher professional development. Interuniv. Electron. J. Teach. Educ. 2022, 25, 79–91. [Google Scholar]
- Spanish Institute for Nursing Research and General Nursing Council of Spain. Nurses’ Actions in the Field of Care in Urgent and Emergency Situations; Spanish Institute for Nursing Research and General Nursing Council of Spain: Madrid, Spain, 2020; ISBN 978-84-09-22538-5. [Google Scholar]
- Resolution no. 11/2019, of 18 December 2019, Which Regulates Certain Aspects of the Professional Practice of Nurses in the Field of Urgencies and Emergencies. BOE no. 24, of “28 January 2020”. Available online: https://www.ieinstituto.es/component/rsfiles/descargar-archivo/archivos?path=resoluciones%252Fresol_11-2019-urgencias-emergencias.pdf&Itemid=3712 (accessed on 17 June 2020).
- Gayrama-Borines, Z.; Coffman, S. Effectiveness of Mentorship Program in the Emergency Department. J. Nurses Prof. Dev. 2021, 37, 107–111. [Google Scholar] [CrossRef]
- Hussein, R.; Everett, B.; Ramjan, L.M.; Hu, W.; Salamonson, Y. New graduate nurses’ experiences in a clinical specialty: A follow up study of newcomer perceptions of transitional support. BMC Nurs. 2017, 16, 42. [Google Scholar] [CrossRef]
- Rush, K.L.; Adamack, M.; Gordon, J.; Lilly, M.; Janke, R. Best practices of formal new graduate nurse transition programs: An integrative review. Int. J. Nurs. Stud. 2013, 50, 345–356. [Google Scholar] [CrossRef]
- Edwards, D.; Hawker, C.; Carrier, J.; Rees, C. A systematic review of the effectiveness of strategies and interventions to improve the transition from student to newly qualified nurse. Int. J. Nurs. Stud. 2015, 52, 1254–1268. [Google Scholar] [CrossRef] [PubMed]
- Alvarez, M. Teacher profile in the competency-based approach. Rev. Electrónica Educ. 2011, 15, 99–107. [Google Scholar] [CrossRef]
- Kaiser, G.; Busse, A.; Hoth, J. About the Complexities of Video-Based Assessments:Theoretical and Methodological Approaches to Overcoming Shortcomings ofResearch on Teachers’ Competence. Int. J. Sci. Math. Educ. 2015, 13, 369–387. [Google Scholar] [CrossRef]
- Ross, J.y.; Bruce, C. Teacher Self-Assessment: A Mechanism for Facilitating Professional Growth. AERA Meeting. 2005. Available online: https://tspace.library.utoronto.ca/handle/1807/30029 (accessed on 17 June 2020).
- Manero-Solanas, M.; Garcés-Horna, S.; Gascón-Catalán, A. Competency development of novice nurses in emergencies with the implementation of a tutoring program. Emergency 2022, 34, 230–233. [Google Scholar]
- Piccinini, C.J.; Hudlun, N.; Branam, K.; Moore, J.M. The effects of preceptor training on new graduate registered nurse transition experiences and organizational outcomes. J. Contin. Educ. Nurs. 2018, 49, 216–220. [Google Scholar] [CrossRef] [PubMed]
- Quek, G.J.H.; Shorey, S. Perceptions, Experiences, and Needs of Nursing Preceptors and Their Preceptees on Preceptorship: An Integrative Review. J. Prof. Nurs. 2018, 34, 417–428. [Google Scholar] [CrossRef] [PubMed]
- Brook, J.; Aitken, L.; Webb, R.; MacLaren, J.; Salmon, D. Characteristics of successful interventions to reduce turnover and increase retention of early career nurses: A systematic review. Int. J. Nurs. Stud. 2019, 91, 47–59. [Google Scholar] [CrossRef] [PubMed]
- Joswiak, M.E. Transforming orientation through a tiered skills acquisition model. J. Nurses Prof. Dev. 2018, 3, 118–122. [Google Scholar] [CrossRef]
- Mínguez Moreno, I.; González de la Cuesta, D.; Barrado Narvión, M.J.; Arnaldos Esteban, M.; González Cantalejo, M. Nurse Mentoring: A Scoping Review. Healthcare 2023, 11, 2302. [Google Scholar] [CrossRef]
- Latham, C.L.; Ringl, K.; Hogan, M. Professionalization and Retention Outcomes of a University–Service Mentoring Program Partnership. J. Prof. Nurs. 2011, 27, 344–353. [Google Scholar] [CrossRef]
- Hoover, J.; Koon, A.D.; Rosser, E.N.; Rao, K.D. Mentoring the working nurse: A scoping review. Hum. Resour. Health 2020, 18, 52. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Level I: Beginner | Level II: Advanced Beginner | Level III: Proficient | Level IV: Efficient | Level V: Expert | |
|---|---|---|---|---|---|
| Orotracheal intubation in emergency situations | Does not list all the necessary elements of a basic intubation. Does not recognize all the elements presented for difficult intubation. Does not correctly classify all necessary drugs. Does not know the correct intubation sequence (premedication → sedation → relaxation). | Meets two of these criteria: Lists all the necessary elements of a basic intubation. Recognizes some elements presented for difficult intubation. Correctly classifies six or more of the drugs needed. Does not know the correct intubation sequence (premedication → sedation → relaxation). | Lists all the necessary elements of a basic intubation (OTI). Recognizes all of the elements presented for difficult intubation. Correctly classifies six or more of the drugs needed. Does not know the correct intubation sequence (premedication → sedation → relaxation). | Lists all the necessary elements of a basic intubation. Recognizes all of the elements presented for difficult intubation. Correctly classifies all necessary drugs. Knows the correct intubation sequence. Has collaborated in real situations but not leading the nursing role. | Lists the necessary elements of a basic intubation and even takes into account those necessary in case of complication. Recognizes all of the elements presented for difficult intubation. Correctly classifies all necessary drugs. Knows the correct intubation sequence. Has experience in real-world situations as a nurse leader in these situations. Is able to train others. |
| Level I: Beginner | Level II: Advanced Beginner | Level III: Proficient | Level IV: Efficient | Level V: Expert | |
|---|---|---|---|---|---|
| Non-invasive mechanical ventilation + Aerogen® nebulization | Does not know the Aerogen® device or how it is assembled. Does not know the material needed to assemble a NIMV circuit or how to assemble it. Does not know how to interpret indicators from the ventilator monitor or solve the incidents shown. | Knows the Aerogen® device and the material required for its use but not its assembly. Knows the material needed to assemble a VMNI circuit but does not know how to assemble it or has any doubts during assembly. Does not know how to interpret indicators from the ventilator monitor or solve the incidents shown. | Knows the Aerogen® device. Capable of assembling it without instructions properly. Knows the material needed to assemble a VMNI circuit. Assembles it without hesitation. Does not know how to interpret indicators from the ventilator monitor or solve the incidents shown. | Knows the Aerogen® device. Capable of assembling it without instructions properly. Knows the material needed to assemble an NIMV circuit. Carries out the assembly properly autonomously. Knows how to interpret indicators from the ventilator monitor and solve incidents shown. | Knows the Aerogen® device. Capable of assembling it without instructions properly. Knows the material needed to assemble an NIMV circuit. Assembles properly autonomously. Interprets the indicators present in the ventilator monitor. Troubleshoots and interprets simple issues. Has experience in real situations. Is able to train others. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Manero-Solanas, M.; Navamuel-Castillo, N.; Garcés-Horna, S.; López-Ibort, N.; Gómez-Baca, C.A.; Gascón-Catalán, A. Design, Implementation, and Adaptation of a Tutoring Program for the Competency Development of New Nurses in a Hospital Emergency Department. Nurs. Rep. 2024, 14, 2370-2384. https://doi.org/10.3390/nursrep14030176
Manero-Solanas M, Navamuel-Castillo N, Garcés-Horna S, López-Ibort N, Gómez-Baca CA, Gascón-Catalán A. Design, Implementation, and Adaptation of a Tutoring Program for the Competency Development of New Nurses in a Hospital Emergency Department. Nursing Reports. 2024; 14(3):2370-2384. https://doi.org/10.3390/nursrep14030176
Chicago/Turabian StyleManero-Solanas, Marta, Noelia Navamuel-Castillo, Silvia Garcés-Horna, Nieves López-Ibort, Carmen Angustias Gómez-Baca, and Ana Gascón-Catalán. 2024. "Design, Implementation, and Adaptation of a Tutoring Program for the Competency Development of New Nurses in a Hospital Emergency Department" Nursing Reports 14, no. 3: 2370-2384. https://doi.org/10.3390/nursrep14030176
APA StyleManero-Solanas, M., Navamuel-Castillo, N., Garcés-Horna, S., López-Ibort, N., Gómez-Baca, C. A., & Gascón-Catalán, A. (2024). Design, Implementation, and Adaptation of a Tutoring Program for the Competency Development of New Nurses in a Hospital Emergency Department. Nursing Reports, 14(3), 2370-2384. https://doi.org/10.3390/nursrep14030176