
Mentoring Support Quality in Group and Individual Mentoring Approaches during Nursing Clinical Training: A Quasi-Experimental Study



Abstract
1. Introduction
2. Materials and Methods
2.1. Sampling
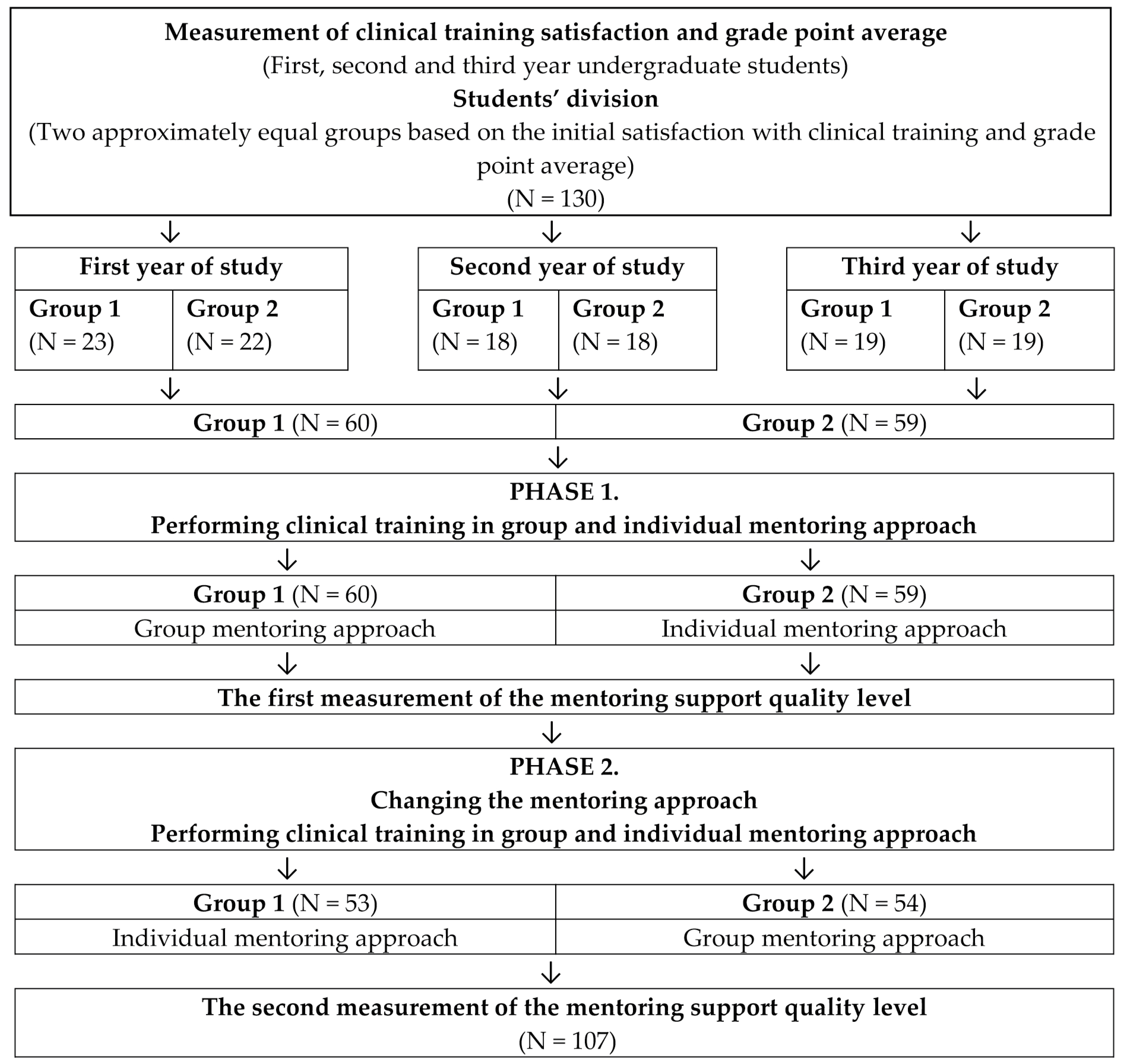
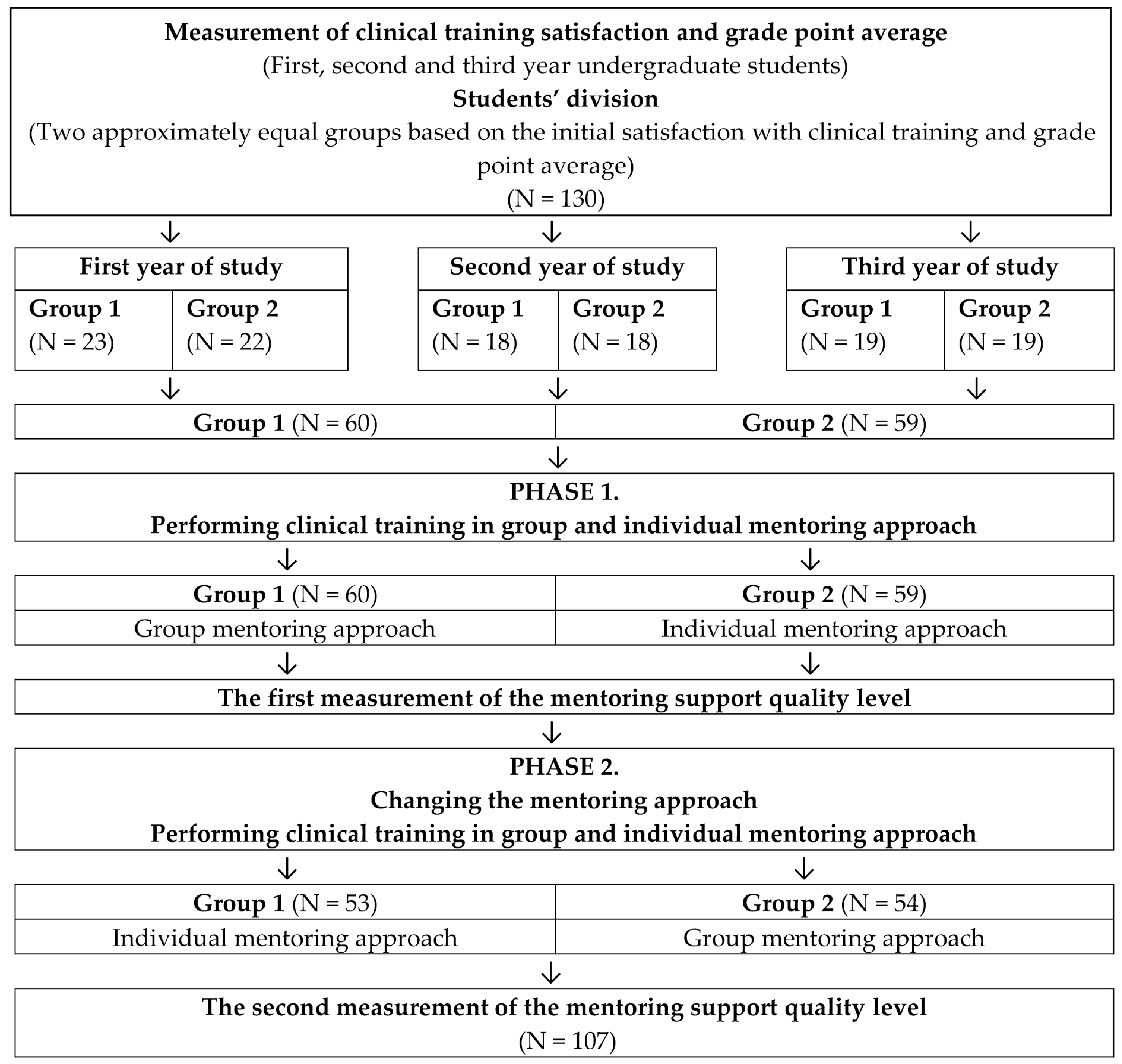
2.2. Study Design
2.3. Participants
2.4. Interventions
2.5. Data Collection Procedures
2.6. Instrument
2.7. Ethical Considerations and Procedures
2.8. Data Analysis
3. Results
3.1. Sociodemographic Characteristics of the Respondents
3.2. Quality Levels of Mentoring Support in Group and Individual Mentoring Approaches
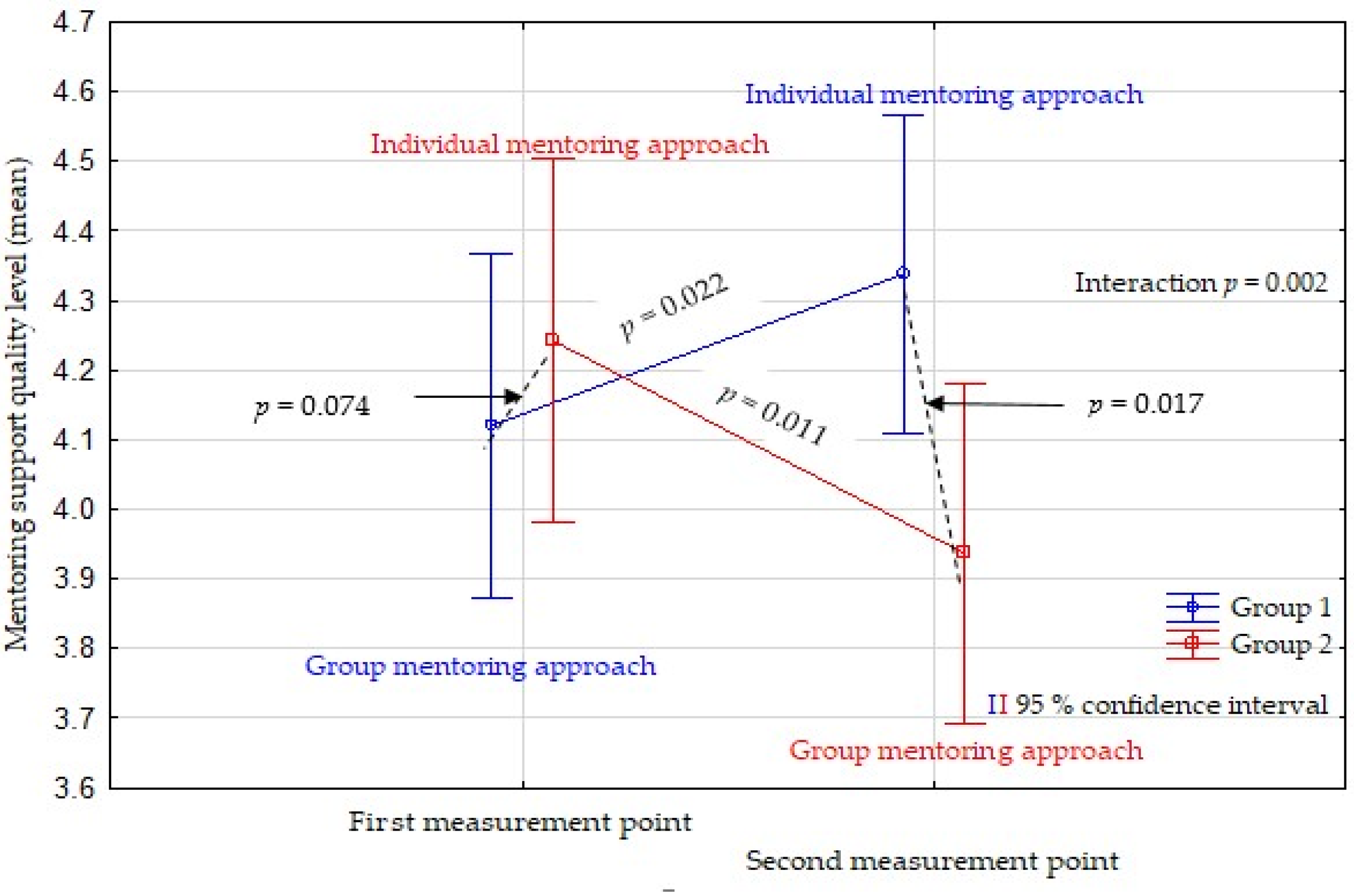
3.3. Differences in the Quality Level of Mentoring Support in the Group and Individual Mentoring Approaches
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Public Involvement Statement
Guidelines and Standards Statement
Acknowledgments
Conflicts of Interest
References
- Mlaba, Z.P.; Emmamally, W. Describing the perceptions of student nurses regarding barriers and benefits of a peer-mentorship programme in a clinical setting in kwazulunatal. Health SA Gesondheid 2019, 24. [Google Scholar] [CrossRef] [PubMed]
- Gusar, I.; Bačkov, K.; Tokić, A.; Dželalija, B.; Lovrić, R. Nursing student evaluations on the quality of mentoring support in individual, dual, and group approaches during clinical training: A prospective cohort study. Aust. J. Adv. Nurs. 2020, 37, 28–36. [Google Scholar] [CrossRef]
- European Parliament and the Council of the European Union. Directive 2013/55/EU of the European parliament and of the council of 20 November 2013 amending Directive 2005/36/EC on the recognition of professional qualifications and Regulation (EU) No 1024/2012 on administrative cooperation through the Internal Mark. Off. J. Eur. Union 2013, 55, 132–169. [Google Scholar]
- Franklin, N. Clinical Supervision in Undergraduate Nursing Students: A Review of the Literature. E-J. Bus. Educ. Scholarsh. Teach. 2013, 7, 34–42. [Google Scholar]
- Kenny, P.; Reeve, R.; Hall, J. Satisfaction with nursing education, job satisfaction, and work intentions of new graduate nurses. Nurse Educ. Today 2016, 36, 230–235. [Google Scholar] [CrossRef] [PubMed]
- Nowell, L.; Norris, J.M.; Mrklas, K.; White, D.E. A literature review of mentorship programs in academic nursing. J. Prof. Nurs. 2017, 33, 334–344. [Google Scholar] [CrossRef] [PubMed]
- Jokelainen, M.; Turunen, H.; Tossavainen, K.; Jamookeeah, D.; Coco, K. A systematic review of mentoring nursing students in clinical placements. J. Clin. Nurs. 2011, 20, 2854–2867. [Google Scholar] [CrossRef] [PubMed]
- Pollock, A.; Campbell, P.; Deery, R.; Fleming, M.; Rankin, J.; Sloan, G.; Cheyne, H. A systematic review of evidence relating to clinical supervision for nurses, midwives and allied health professionals. J. Adv. Nurs. 2017, 73, 1825–1837. [Google Scholar] [CrossRef] [PubMed]
- Walker, S.; Dwyer, T.; Moxham, L.; Broadbent, M.; Sander, T. Facilitator versus preceptor: Which offers the best support to undergraduate nursing students? Nurse Educ. Today 2013, 33, 530–535. [Google Scholar] [CrossRef]
- Ntho, T.A.; Pienaar, A.J.; Sehularo, L.A. Peer-mentees’ challenges in an undergraduate peer-group clinical mentoring programme in a nursing education institution. Health SA Gesondheid 2020, 25. [Google Scholar] [CrossRef]
- Antohe, I.; Riklikiene, O.; Tichelaar, E.; Saarikoski, M. Clinical education and training of student nurses in four moderately new European Union countries: Assessment of students’ satisfaction with the learning environment. Nurse Educ. Pract. 2016, 17, 139–144. [Google Scholar] [CrossRef] [PubMed]
- Saarikoski, M.; Marrow, C.; Abreu, W.; Riklikiene, O.; Özbicakçi, S. Student nurses’ experience of supervision and Mentorship in clinical practice: A cross cultural perspective. Nurse Educ. Pract. 2007, 7, 407–415. [Google Scholar] [CrossRef] [PubMed]
- Kostovich, C.T.; Thurn, K.E. Group mentoring: A story of transition for undergraduate baccalaureate nursing students. Nurse Educ. Today 2013, 33, 413–418. [Google Scholar] [CrossRef] [PubMed]
- Mikkonen, K.; Elo, S.; Miettunen, J.; Saarikoski, M.; Kaatiainen, M. Development and testing of the CALD s and CLES+T scales for international nursing students clinical learning environments. J. Adv. Nurs. 2017, 73, 1977–2011. [Google Scholar] [CrossRef]
- Pitkänena, S.; Kääriäinen, M.; Oikarainena, A.; Tuomikoski, A.M.; Elo, S.; Ruotsalainen, H.; Saarikoski, M.; Kärsämänoja, T.; Mikkonen, K. Healthcare students’ evaluation of the clinical learning environment and supervision—A cross-sectional study. Nurse Educ. Today 2018, 62, 143–149. [Google Scholar] [CrossRef] [PubMed]
- Phillips, K.F.; Mathew, L.; Aktan, N.; Catano, B. Clinical education and student satisfaction: An integrative literature review. Int. J. Nurs. Sci. 2017, 4, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Ayalew, F.; Kibwana, S.; Shawula, S.; Misganaw, E.; Abosse, Z.; Van Roosmalen, J.; Stekelenburg, J.; Kim, Y.M.; Teshome, M.; Mariam, D.W. Understanding job satisfaction and motivation among nurses in public health facilities of Ethiopia: A cross-sectional study. BMC Nurs. 2019, 18, 46. [Google Scholar] [CrossRef] [PubMed]
- Mažionienė, A.; Staniulienė, V.; Gerikienė, V. The Clinical Learning Environment: The Attitude of Undergraduate Student Nurses Towards Mentorship At Hospitals in Lithuania. CBU Int. Conf. Proc. 2018, 6, 659–666. [Google Scholar] [CrossRef]
- Lilja Andersson, P.; Edberg, A.K. Swedish nursing students’ experience of aspects important for their learning process and their ability to handle the complexity of the nursing degree program. Nurse Educ. Today 2012, 32, 453–457. [Google Scholar] [CrossRef]
- Crombie, A.; Brindley, J.; Harris, D.; Marks-Maran, D.; Thompson, T.M. Factors that enhance rates of completion: What makes students stay? Nurse Educ. Today 2013, 33, 1282–1287. [Google Scholar] [CrossRef]
- Lovrić, R.; Milutinović, D.; Žvanut, B. Psychometric evaluation and cross-cultural adaptation of the Croatian version of Nursing student perceptions of dishonesty scale. J. Prof. Nurs. 2020, 36, 432–442. [Google Scholar] [CrossRef]
- Salamonson, Y.; Everett, B.; Halcomb, E.; Hutchinson, M.; Jackson, D.; Mannix, J.; Peters, K.; Weaver, R. Unravelling the complexities of nursing students’ feedback on the clinical learning environment: A mixed methods approach. Nurse Educ. Today 2015, 35, 206–211. [Google Scholar] [CrossRef]
- Drennan, V.M.; Ross, F. Global nurse shortages-the facts, the impact and action for change. Br. Med. Bull. 2019, 19, 25–37. [Google Scholar] [CrossRef] [PubMed]
- Vidović, V.V.; Vuković, M.B.; Matić, J. IDIZ-ov Priručnik za Mentoriranje Mladih Istraživača; Institut za Društvena Istraživanja u Zagrebu: Zagreb, Croatia, 2014; pp. 1–36. Available online: https://www.ffri.uniri.hr/files/dokumentifakulteta/IDIZ-ov_prirucnik_za_mentoriranje.pdf (accessed on 11 November 2023).
- Canet-Vélez, O.; Botigué, T.; Lavedán Santamaría, A.; Masot, O.; Cemeli, T.; Roca, J. The perception of training and professional development according to nursing students as health workers during COVID-19: A qualitative study. Nurse Educ. Pract. 2021, 53, 103072. [Google Scholar] [CrossRef] [PubMed]
- Gusar, I.; Gabrilo, K.; Tokić, A. Online teaching during COVID-19 pandemic: Attitudes of Croatian nursing students. Cent. Eur. J. Nurs. Midwifery 2023, 14, 815–822. [Google Scholar] [CrossRef]
- Papastavrou, E.; Lambrinou, E.; Tsangari, H.; Saarikoski, M.; Leino-Kilpi, H. Student nurses experience of learning in the clinical environment. Nurse Educ. Pract. 2010, 10, 176–182. [Google Scholar] [CrossRef] [PubMed]
- Crawford, M.J.; Dresen, S.E.; Tschikota, S.E. From “getting to know you” to “soloing”: The preceptor-student relationship. Nt Res. 2000, 5, 5–19. [Google Scholar] [CrossRef]
- Woo, M.W.J.; Li, W. Nursing students’ views and satisfaction of their clinical learning environment in Singapore. Nurs. Open 2020, 7, 1909–1919. [Google Scholar] [CrossRef]
- Tuomikoski, A.M.; Ruotsalainen, H.; Mikkonen, K.; Miettunen, J.; Juvonen, S.; Sivonen, P.; Kääriäinen, M. How mentoring education affects nurse mentors’ competence in mentoring students during clinical practice—A quasi-experimental study’. Scand. J. Caring Sci. 2020, 34, 230–238. [Google Scholar] [CrossRef]
- Jack, K.; Hamshire, C.; Harris, W.E.; Langan, M.; Barrett, N.; Wibberley, C. “My mentor didn’t speak to me for the first four weeks”: Perceived Unfairness experienced by nursing students in clinical practice settings. J. Clin. Nurs. 2018, 27, 929–938. [Google Scholar] [CrossRef] [PubMed]
- Lovrić, R.; Farčić, N.; Mikšić, Š.; Včev, A. Studying During the COVID-19 Pandemic: A Qualitative Inductive Content Analysis of Nursing Students’ Perceptions and Experiences. Educ. Sci. 2020, 10, 188. [Google Scholar] [CrossRef]
- Mbakaya, B.C.; Kalembo, F.W.; Zgambo, M.; Konyani, A.; Lungu, F.; Tveit, B.; Kaasen, A.; Simango, M.; Bvumbwe, T. Nursing and midwifery students’ experiences and perception of their clinical learning environment in Malawi: A mixed-method study. BMC Nurs. 2020, 19, 87. [Google Scholar] [CrossRef] [PubMed]
- Tang, C.Y. Learning Experience of Chinese Nursing Students during Clinical Practicum: A Descriptive Qualitative Study. Nurs. Rep. 2021, 11, 495–505. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Group | n | First Round | n | Second Round | ||
|---|---|---|---|---|---|---|
| Mentoring Approach | Mean (SD) | Mentoring Approach | Mean (SD) | |||
| Group 1 | 60 | GMA | 4.12 (0.94) | 53 | IMA | 4.34 (0.91) |
| Group 2 | 59 | IMA | 4.24 (0.66) | 54 | GMA | 3.94 (1.04) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gusar, I.; Tokić, A.; Lovrić, R. Mentoring Support Quality in Group and Individual Mentoring Approaches during Nursing Clinical Training: A Quasi-Experimental Study. Nurs. Rep. 2024, 14, 838-848. https://doi.org/10.3390/nursrep14020065
Gusar I, Tokić A, Lovrić R. Mentoring Support Quality in Group and Individual Mentoring Approaches during Nursing Clinical Training: A Quasi-Experimental Study. Nursing Reports. 2024; 14(2):838-848. https://doi.org/10.3390/nursrep14020065
Chicago/Turabian StyleGusar, Ivana, Andrea Tokić, and Robert Lovrić. 2024. "Mentoring Support Quality in Group and Individual Mentoring Approaches during Nursing Clinical Training: A Quasi-Experimental Study" Nursing Reports 14, no. 2: 838-848. https://doi.org/10.3390/nursrep14020065
APA StyleGusar, I., Tokić, A., & Lovrić, R. (2024). Mentoring Support Quality in Group and Individual Mentoring Approaches during Nursing Clinical Training: A Quasi-Experimental Study. Nursing Reports, 14(2), 838-848. https://doi.org/10.3390/nursrep14020065