
Pain Assessment in Patients during Hemodialysis Treatment: Quality Improvement Project



Abstract
1. Introduction
1.1. Pain Context
1.2. Pain in Patients with Chronic Kidney Disease
1.3. Pain Management and Treatment
2. Materials and Methods
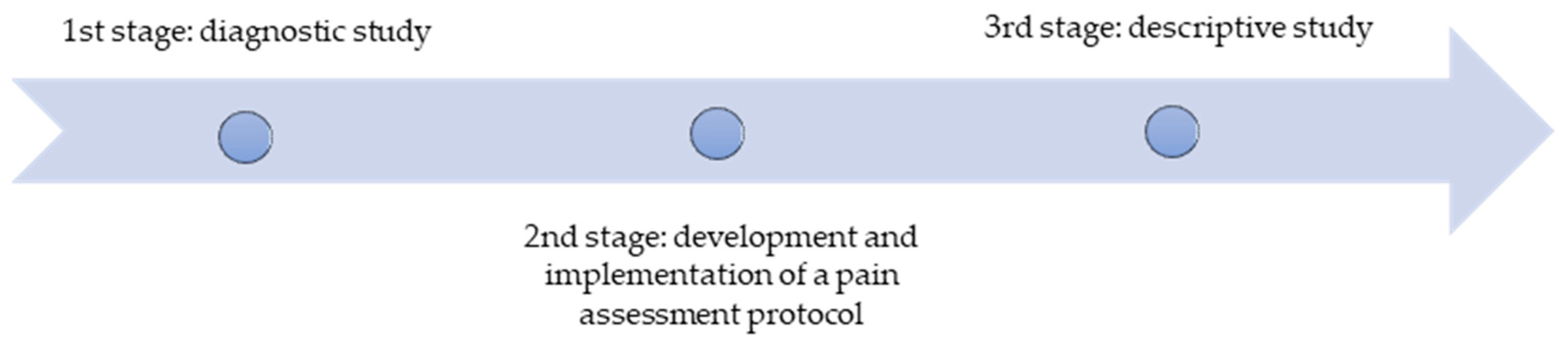
2.1. Study Design
- (i)
- Assess the patient’s ability to evaluate their pain.
- (ii)
- If the patient can assess their pain, instruments such as the Numerical Rating Pain Scale (NRPS), Visual Analogue Scale (VAS), or qualitative self-report scales should be used, as suggested by evidence, respecting the patient’s preference.
- (iii)
- If the patient is unable to verbally assess their pain, use the Pain Assessment in Advanced Dementia (PAINAD) and Behavior Pain Scale (BPS) instruments.
- (iv)
- If the patient reports feeling pain, the nurse should implement non-pharmacological pain relief strategies (e.g., positioning or optimizing the environment such as light, noise, and temperature control) and begin administering painkillers based on WHO recommendations and medical prescriptions. If necessary, contact the physician to readjust pharmacological prescriptions.
- (v)
- Document nursing records, including pain characteristics (i.e., type, intensity, location, irradiation, and previous effective management strategies) and interventions performed.
- (vi)
- Reassess pain frequently (ten minutes after administering painkillers).
- (vii)
- During these procedures, the nurse should monitor the patient’s condition, promote comfort and well-being, and provide reassurance to the patient.
2.2. Setting of Study
2.3. Population and Sample
Inclusion and Exclusion Criteria
2.4. Data Collection Instruments
2.5. Data Analysis
2.6. Ethical Procedures
3. Results
3.1. Sociodemographic and Clinical Characterization of HD Treatments

{kind=link}
| M | SD | Max | Min | ||
|---|---|---|---|---|---|
| Age * (years) | 71.48 | 12.70 | 93 | 35 | |
| n | % | ||||
| Gender * | Male | 48 | 64.00 | ||
| Female | 27 | 36.00 | |||
| Residence * | Countryside | 61 | 81.30 | ||
| Urban | 14 | 18.70 | |||
| Qualification (by Portuguese classification) * | Illiterate (not able to read or write) | 11 | 14.70 | ||
| Elementary School (1st–4rd year) | 45 | 60.00 | |||
| 1st Basic Education (5th–7th year) | 7 | 9.30 | |||
| 2nd Basic Education (7th–9th year) | 6 | 8.00 | |||
| Secondary Education (10th–12nd year) | 3 | 4.00 | |||
| Higher Education | 3 | 4.00 |
| M | SD | Max | Min | ||
|---|---|---|---|---|---|
| Average time since starting dialysis treatment * (years) | 4.72 | 3.91 | 18 | 1 | |
| n | % | ||||
| Number of treatments per week * | 3 times a week | 74 | 98.70 | ||
| 4 times a week | 1 | 1.30 | |||
| Type of vascular access * | Arteriovenous fistulae (AVF) | 65 | 86.70 | ||
| Polytetrafluoroethylene -PTFE | 6 | 8.00 | |||
| Central venous catheter (CVC) | 4 | 5.30 | |||
| Vascular access localization * | Left upper limb | 58 | 77.30 | ||
| Right upper limb | 13 | 17.30 | |||
| Central venous catheter (CVC) | 4 | 5.30 |
| M | SD | Max | Min | ||
|---|---|---|---|---|---|
| Average Time with Pain (years) | 3.64 | 2.7 | 10 | 1 | |
| Questions: | n | % | |||
| Do you usually have pain? | Yes | 48 | 64.00 | ||
| No | 27 | 36.00 | |||
| How is your pain duration? | Intermittent | 46 | 61.30 | ||
| Continued | 2 | 2.70 | |||
| Where do you feel your pain? | Lower limbs | 15 | 20.00 | ||
| Lower back | 15 | 20.00 | |||
| Bones and muscles | 14 | 18.70 | |||
| Head | 3 | 4.00 | |||
| Other | 1 | 1.30 | |||
| Does the pain irradiate? | No | 38 | 50.70 | ||
| Yes ** | 10 | 13.30 | |||
| ** Where is the place where it radiates? | Lower limbs | 7 | 9.30 | ||
| Lower backlight shoulder | 2 | 2.70 | |||
| Right shoulder | 1 | 1.30 | |||
| How could you define your pain? | “Crushing” | 24 | 32.00 | ||
| “Cramp” | 14 | 18.70 | |||
| “Stabbing” | 6 | 8.00 | |||
| “Tingling” | 2 | 2.70 | |||
| “Burning” | 2 | 2.70 | |||
| What is the pain assessment tool used? | Qualitative Pain Scale | 35 | 46.70 | ||
| Numerical Rating Pain Scale (NRPS) [0–10] | 13 | 17.30 | |||
| Do you usually do pain control medication? | Yes | 27 | 36.00 | ||
| No | 21 | 28.00 | |||
| What medication do you usually take? | Paracetamol | 13 | 17.30 | ||
| Magnesium-metamizole | 3 | 4.00 | |||
| Tramadol | 3 | 4.00 | |||
| Pregabalin | 2 | 2.70 | |||
| Dot Know or remember the name | 6 | 8.00 | |||
| Does your pain limit your Activities of Daily Living (ADLs)? | Yes ** | 24 | 32.00 | ||
| No | 24 | 32.00 | |||
| ** What are the mostly affected ADLs? | Mobility | 22 | 29.30 | ||
| Sleep | 2 | 2.70 | |||
| Are you followed by a Chronic Pain Unit team? | No | 34 | 45.30 | ||
| Yes | 2 | 2.70 |
| n | % | ||
|---|---|---|---|
| Do you usually have pain during your HD treatment? | No | 39 | 52.00 |
| Yes | 36 | 48.00 | |
| Where you usually have more pain? | Lower limbs | 14 | 18.70 |
| Lower back | 14 | 18.70 | |
| Upper limbs | 3 | 4.00 | |
| Headaches | 3 | 4.00 | |
| Bones/muscles | 1 | 1.30 | |
| Other | 1 | 1.30 | |
| How can you define your pain? | “Crushing” | 15 | 20.00 |
| “Cramp” | 9 | 12.00 | |
| “Stabbing” | 8 | 10.70 | |
| “Tingling” | 2 | 2.70 | |
| “Burning” | 2 | 2.70 | |
| Does your pain get worse during a HD treatment? | Yes ** | 28 | 37.30 |
| No | 8 | 10.70 | |
| ** What is your pain relief strategy? | Positioning | 24 | 32.00 |
| Medication | 11 | 14.70 | |
| Other | 1 | 1.30 | |
| Do you usually take painkillers during HD treatment? | No | 25 | 33.30 |
| Yes ** | 11 | 14.70 | |
| ** What painkiller(s) you usually do in HD treatment? | Paracetamol | 8 | 10.70 |
| Magnesium-metamizole | 3 | 4.00 |
3.2. Characterization of Pain in Patients with CKD
3.3. Nurses’ Characterization
3.4. Assessment of Nurses’ Satisfaction with Strategies Implemented
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Public Involvement Statement
Use of Artificial Intelligence
Guidelines and Standards Statement
Acknowledgments
Conflicts of Interest
Appendix A
| Text Section and Item Name | Section or Item Description | Page No |
|---|---|---|
| Title and Abstract | ||
| Indicate that the manuscript concerns an initiative to improve healthcare (broadly defined to include the quality, safety, effectiveness, patient-centeredness, timeliness, cost, efficiency, and equity of healthcare) | 1 |
| a. Provide adequate information to aid in searching and indexing b. Summarize all key information from various sections of the text using the abstract format of the intended publication or a structured summary such as: background, local problem, methods, interventions, results, conclusions | 1 |
| Introduction | Why did you start? | |
| Nature and significance of the local problem | 1–3 |
| Summary of what is currently known about the problem, including relevant previous studies | 1–3 |
| Informal or formal frameworks, models, concepts, and/or theories used to explain the problem, any reasons or assumptions that were used to develop the intervention(s), and reasons why the intervention(s) was expected to work | 2 |
| Purpose of the project and of this report | 4 |
| Methods | What did you do? | |
| Contextual elements considered important at the outset of introducing the intervention(s) | 3 |
| a. Description of the intervention(s) in sufficient detail that others could reproduce it b. Specifics of the team involved in the work | 4 |
| a. Approach chosen for assessing the impact of the intervention(s) b. Approach used to establish whether the observed outcomes were due to the intervention(s) | 4 |
| a. Measures chosen for studying processes and outcomes of the intervention(s), including rationale for choosing them, their operational definitions, and their validity and reliability b. Description of the approach to the ongoing assessment of contextual elements that contributed to the success, failure, efficiency, and cost c. Methods employed for assessing completeness and accuracy of data | 4 |
| a. Qualitative and quantitative methods used to draw inferences from the data b. Methods for understanding variation within the data, including the effects of time as a variable | 5 |
| Ethical aspects of implementing and studying the intervention(s) and how they were addressed, including, but not limited to, formal ethics review and potential conflict(s) of interest | 6 |
| Results | What did you find? | |
| a. Initial steps of the intervention(s) and their evolution over time (e.g., time-line diagram, flow chart, or table), including modifications made to the intervention during the project b. Details of the process measures and outcome c. Contextual elements that interacted with the intervention(s) d. Observed associations between outcomes, interventions, and relevant contextual elements e. Unintended consequences such as unexpected benefits, problems, failures, or costs associated with the intervention(s). f. Details about missing data | 6–12 |
| Discussion | What does it mean? | |
| a. Nature of the association between the intervention(s) and the outcomes b. Comparison of results with findings from other publications c. Impact of the project on people and systems d. Reasons for any differences between observed and anticipated outcomes, including the influence of context e. Costs and strategic trade-offs, including opportunity costs | 12–15 |
| a. Limits to the generalizability of the work b. Factors that might have limited internal validity such as confounding, bias, or imprecision in the design, methods, measurement, or analysis. c. Efforts made to minimize and adjust for limitations | 15 |
| a. Usefulness of the work b. Sustainability c. Potential for spread to other contexts d. Implications for practice and further study in the field e. Suggested next steps | 15–16 |
References
- World Health Organization. World Health Statistics 2023: Monitoring Health for the SDGs, Sustainable Development Goals; World Health Organization: Geneva, Switzerland, 2023; Available online: https://www.who.int/publications/i/item/9789240074323 (accessed on 1 May 2023).
- Almeida, E.A.F.; Raimundo, M.; Coelho, A.; Sá, H. Incidence, prevalence and crude survival of patients starting dialysis in Portugal (2010–2016): Analysis of the National Health System individual registry. Clin. Kidney J. 2021, 14, 869–875. [Google Scholar] [CrossRef]
- National Kidney Foundation. NKFKDOQI Clinical Pratice Guidelines 2021. Available online: https://www.kidney.org/professionals/guidelines (accessed on 5 May 2023).
- Jesus, N.M.; Souza, G.F.; Mendes-Rodrigues, C.; Neto, O.P.A.; Rodrigues, D.D.M.; Cunha, C.M. Quality of life of individuals with chronic kidney disease on dialysis. J. Bras. Nefrol. 2019, 41, 364–374. [Google Scholar] [CrossRef]
- Galvão, A. Abordagem da DRC avançada: Estado da arte e controvérsias. Sociedade Portuguesa de Nefrologia. 2022. Available online: https://www.spnefro.pt/assets/relatorios/tratamento_doenca_terminal/er2023_registo.pdf (accessed on 1 May 2023).
- Evaristo, L.S.; Cunha, A.P.; Morais, C.G.; Samselski, B.J.L.; Esposito, E.P.; Miranda, M.K.V.; Gouvêa-e-Silva, L.F. Complicaciones durante la sesión de hemodiálisis. av.enferm. [online] 2020, 38, 316–324. [Google Scholar] [CrossRef]
- Barros, A.; Borges, S.; Lemos, K. Doença renal crônica e cuidado paliativo: Avaliação dos sintomas, estado nutricional, funcionalidade e perceção do tratamento dialítico. Braz. J. Dev. 2022, 8, 16655–16673. [Google Scholar] [CrossRef]
- Vides, M.C.; Martins, M.R.I. Avaliação da dor óssea em pacientes renais crônicos em hemodiálise. Revista Dor. 2017, 18, 245–249. [Google Scholar]
- Lambourg, E.; Colvin, L.; Guthrie, G.; Murugan, K.; Lim, M.; Walker, H.; Boon, G.; Bell, S. The prevalence of pain among patients with chronic kidney disease using systematic review and meta-analysis. Kidney Int. 2021, 100, 636–649. [Google Scholar] [CrossRef]
- International Association for the Study of Pain. Available online: https://www.iasp-pain.org/resources/terminology/#pain (accessed on 10 May 2023).
- Afonso, M. Controlo Farmacológico da Dor. Master’s Degree, Universidade Fernando Pessoa, Porto, Portugal, 2021. [Google Scholar]
- Cohen, S.P.; Vase, L.; Hooten, W.M. Chronic pain: An update on burden, best pratices, and new advances. Lancet 2021, 397, 2082–2097. [Google Scholar] [CrossRef]
- Moreno, A.F.C.; Silva, G.O.; Ferreira, E.D.F. Analysis of chronic pain in users of primary health care units in Maringá-PR. Braz. J. Dev. 2023, 9, 15160–15177. [Google Scholar] [CrossRef]
- Rocha, J.R.O.; Uhlig, S.; Karloh, M.; Santos, A.R.S.; Sousa, T.R. Characterization of biopsychosocial factors of patients with chronic nonspecific low back pain. BrJP 2021, 4, 332–338. [Google Scholar] [CrossRef]
- Ashmawi, H.A. Programa de Educação Continuada em Fisiopatologia e Terapêutica da Dor. Available online: https://www.anestesiologiausp.com.br/wp-content/uploads/epidemiologia-da-dor_2020.pdf (accessed on 15 May 2023).
- Figueira, A.I.R.; Amaral, G.M.M.S.; Carmo, T.I.G. A avaliação e registo da dor no serviço de urgência: Um estudo transversal. Enfermería Cuid. Humaniz. 2022, 11, e2712. [Google Scholar] [CrossRef]
- Santos, P.R.; Mendonça, C.R.; Noll, M.; Borges, C.C.; Alves, P.M.; Dias, N.T.; Romeiro, A.M.S.; Barbosa, M.A.; Porto, C.C. Pain in hemodialysis patients: Prevalence, intensity, location and functional interference in daily activities. Healthcare 2021, 9, 1375. [Google Scholar] [CrossRef]
- Silva, F.; Melo, G.; Santos, R.; Silva, R.; Aguiar, L.; Caetano, J. Avaliação da dor em pacientes com insuficiência renal crónica em hemodiálise. Rev. Rene. 2020, 21, e43685. [Google Scholar] [CrossRef]
- Dionísio, G.H.; Salermo, V.Y.; Padilha, A. Central sensitization and beliefs among patients with chronic pain in a primary health care unit. BrJP 2020, 3, 42–47. [Google Scholar] [CrossRef]
- Direção-Geral da Saúde. A Dor como 5° sinal vital. Registo sistemático da intensidade da Dor. Available online: https://www.aped-dor.org/documentos/DGSdor_como_5_sinal_vital_-_2003.pdf (accessed on 21 May 2023).
- Ordem dos Enfermeiros. Dor—Guia Orientador de Boa Prática. Available online: https://www.ordemenfermeiros.pt/arquivo/publicacoes/Documents/cadernosoe-dor.pdf (accessed on 21 May 2023).
- Fink, R.M.; Brant, J.M. Complex cancer pain assessment. Hematol. Oncol. Clin. N. Am. 2018, 32, 353–369. [Google Scholar] [CrossRef]
- Nagoor, S.; Sathiya, M. Efficacy of muscle relaxation technique on pain perception among patients undergoing hemodialysis. Indian J. Palliat. Care 2019, 25, 566–570. [Google Scholar]
- Aboul-Fotouh, A.; El-Sayed, R.; Hegazy, N. Non-pharmacological interventions for reducing fatigue in adults undergoing maintenance hemodialysis: A systematic review. Clin. Nurs. Res. 2018, 27, 797–817. [Google Scholar]
- Lee, Y.; Lin, K.; Lin, C. Effectiveness of Warm Compress Application on Pain among Hemodialysis Patients. J. Ren. Care 2020, 46, 88–95. [Google Scholar]
- Dutton, J.; Forni, L.G.; Keogh, B.E. Renal replacement therapy and the management of pain in acute kidney injury. Anaesthesia 2017, 72, 1092–1101. [Google Scholar]
- Direção-Geral da Saúde. Programa Nacional para a Prevenção e Controlo da Dor. Available online: https://www.google.com.hk/search?client=firefox-b-d&q=DGS-Programa_Nacional_para_a_Prevenção_e_Controlo_da_Dor_-_2017.pdf(aped-dor.org) (accessed on 25 May 2023).
- Sociedade Portuguesa de Nefrologia. Evolução Temporal da Incidência da DRC em TSFR: Implicações Clínico-Epidemiológicas. Sociedade Portuguesa de Nefrologia, Gabinete do Registo da Doença Renal Crónica. Available online: https://www.spnefro.pt/assets/relatorios/tratamento_doenca_terminal/dados-gerais-do-registo-2022.pdf (accessed on 25 May 2023).
- Pires, S.; Carrão, J.; Mota, M.; Cunha, M. Determinantes do ganho de peso interdialítico em pessoas em hemodiálise. Servir 2022, 2, e26229. [Google Scholar]
- Sociedade Portuguesa de Nefrologia. Portuguese Regestry of Dialysis and Transplantation 2021. Sociedade Portuguesa de Nefrologia, Gabinete do Registo da Doença Renal Crónica. Available online: https://www.spnefro.pt/assets/relatorios/tratamento_doenca_terminal/er2022-final.pdf (accessed on 25 May 2023).
- Sousa, L.M.M.; Marques-Vieira, C.M.A.; Marques, M.C.; Reis, M.G.M.; Bule, M.J.; José, H.M.G. Avaliação e Efetividade da Analgesia em Pessoas Submetidas a Hemodiálise. Rev. Ibero-Am. De Saúde E Envelhec. 2019, 5, 1832–1844. [Google Scholar] [CrossRef]
- Kusztal, M.; Trafidto, E.; Madziarska, K.; Augustyniak-Bartosik, H.; Karczewski, M.; Weyde, W.; Krajewska, M.; Rymaszewska, J.; Klinger, M. Depressive symptoms but not chronic pain have an impact on the survival of patients undergoing maintance hemodialysis. Arch. Med. Sci. 2018, 14, 265–275. [Google Scholar] [CrossRef]
- Komann, M.; Weinmann, C.; Schwenkglenks, M.; Meissner, W. Non-Pharmacological Methods and Post-Operative Pain Relief: An observational study. Anesth Pain Med. 2019, 9, e84674. [Google Scholar] [CrossRef]
- Ritto, C.; Rocha, F.D. Avaliação da Dor. No Manual da Dor Crónica; Instituto Português de Oncologia: Lisboa, Portugal, 2012. [Google Scholar]
- Allen, E.; Williams, A.; Jennings, D.; Stomski Goucke, R.; Toyce, C.; Slatyer, S.; Clarke, T.; Mc Cullough, K. Revisiting the pain resource nurse role in sustaining evidence-based changes for pain assessment and management. Worldviews Evid. Based Nurs. 2018, 15, 368–376. [Google Scholar] [CrossRef]
- Lemos, B.O.; Cunha, A.M.R.; Cesarino, C.B.; Martins, M.R.I. The impact of chronic pain on functionality and quality of life of the elderly. BrJP 2019, 2, 237–241. [Google Scholar] [CrossRef]
- Dantas, J.; Martins, M.R.I. Correlation between pain and quality of life of patients under hemodialysis. Rev. Dor. 2017, 18, 124–127. [Google Scholar] [CrossRef]
- Pozo, M.G.; Parrado, M.C.R.; Garrido, M.C.; López, V.E.G.; Montero, R.C. Caracterizacion del dolor en el paciente en hemodiálisis. Enferm Nefrol. 2017, 20, 295–304. [Google Scholar] [CrossRef]
- Andrade, A.F.S.M.; Teles, W.S.; Silva, M.C.; Torres, R.C.; Azevedo, M.V.C.; Debbo, A.; Silva, M.H.S.; Barros, A.M.M.; Junior, P.C.C.S.; Calasans, T.A.S. Assistência de enfermagem ao paciente em hemodiálise: Investigação completiva. Res. Soc. Dev. 2021, 10, e522101119890. [Google Scholar] [CrossRef]
- Fleishman, T.T.; Dreiher, J.; Shvartzman, P. Pain in Maintenanc Hemodialysis Patients: A Multicenter Study. J. Pain Symptom Manag. 2018, 56, 178–184. [Google Scholar] [CrossRef]
- Coluzzi, F. Assessing and treating chronic pain in patients with end-stage renal disease. Drogas 2018, 78, 1459–1479. [Google Scholar] [CrossRef]
- Marzouq, M.K.; Samoudi, A.F.; Samara, A.; Zyoud, S.H.; Al-Jabi, S.W. Exploring factors associated with pain in hemodialysis patients: A multicenter cross-sectional study from Palestine. BMC Nephrol. 2021, 22, 96. [Google Scholar] [CrossRef]
- Lucas, G.N.C.; Leitão, A.C.C.; Alencar, R.L.; Xavier, R.M.F.; Daher, E.F.; Junior, G.B.S. Pathophysiological aspects of nephropathy caused by non-steroidal anti-inflammatory drugs. Braz. J. Nephrol. 2019, 41, 124–130. [Google Scholar] [CrossRef] [PubMed]
- Nagar, V.R.; Nascimentos, P.; Salles, S.; Sloan, P.A. Opioid use in chronic pain patients with chronic kidney disease: A systematic review. Pain Med. 2017, 18, 1416–1449. [Google Scholar] [CrossRef] [PubMed]
- Dreiher, J.; Fleishman, T.T.; Shvartzman, P. Pain management evaluation in maintenance hemodialysis patients. Pain Med. 2021, 22, 1946–1953. [Google Scholar] [CrossRef] [PubMed]
- Raina, R.K. Management of pain in end-stage renal disease patients: Short review. Hemodial. Int. 2017, 22, 290–296. [Google Scholar] [CrossRef] [PubMed]
- Ceballos, K.; Lagos, L.; Aragon, E.; Ocampo, C.; Sandoval, R. Impact of relaxation techniques in the reduction of pain in hemodialysis patients: A randomized clinical trial. Pain Manag. Nurs. 2019, 20, 146–152. [Google Scholar]
- Heidari, M.; Gorji, M.A.H.; Farajzadeh, Z.; Shahgholian, N. Effect of guided imagery on pain and anxiety in patients undergoing hemodialysis: A randomized controlled trial. J. Caring Sci. 2017, 6, 247–256. [Google Scholar]
- Kesik, G.; Ozdemir, L.; Yildirim, T.; Jabrayilov, J.; Çeliksoz, G. Effects of warm or cold compresses applied to the legs during hemodialysis on cramps, fatigue, and patient comfort: A placebo-controlled randomized trial. Hemodial. Int. 2023, 2, 117–125. [Google Scholar] [CrossRef]
- Dinis, M.; Sousa, J. A pilot randomised controlled trial on the effectiveness of an anti-stress ball technique for pain reduction during vascular access cannulation in haemodialysis patients. Nurs. Rep. 2023, 13, 731–739. [Google Scholar] [CrossRef] [PubMed]
- Ordem dos Enfermeiros. Anuário Estatístico 2022. Available online: https://www.ordemenfermeiros.pt/estat%C3%ADstica-de-enfermeiros/ (accessed on 25 June 2023).
- Instituto Nacional de Estatística. Estatísticas da Saúde—2022. Lisboa. Available online: https://www.ine.pt/xportal/xmain?xpid=INE&xpgid=ine_indicadores&contecto=pi&indOcorrCod=0008198&selTab=tab0 (accessed on 25 June 2023).
- Sutherland, R. Dying well-informed: The need for better clinical education surrounding facilitating end-of-life conversations. Yale J. Biol. Med. 2019, 92, 757–764. [Google Scholar]
- Ordem dos Enfermeiros. Sistemas de Informação de Enfermagem—Princípios Básicos da Arquitetura e Principais Requisitos Técnico—Funcionais. Available online: https://www.ordemenfermeiros.pt/arquivo/documentosoficiais/Documents/SIE-PrincipiosBasicosArq_RequisitosTecFunc-Abril2007.pdf (accessed on 28 June 2023).
- Bailas, C.M. Impacto do uso de sistemas de informação informatizados na carga global de trabalho dos enfermeiros. Master’s Degree, Escola Superior de Enfermagem do Porto, Porto, Portugal, 2016. [Google Scholar]
- Moyo, N.; Madzimbamuto, F. Teaching of chronic pain management in a low-and-middle-income setting: A needs assessment survey. Pain Rep. 2019, 4, e708. [Google Scholar] [CrossRef]
| M | SD | Max | Min | ||
|---|---|---|---|---|---|
| Age (years) | 38.38 | 3.86 | 49 | 35 | |
| Nursing experience (years) | 15.54 | 4.18 | 26 | 10 | |
| n | % | ||||
| Gender | Female | 11 | 84.60 | ||
| Male | 2 | 15.40 | |||
| Professional category | General Nurse | 10 | 76.90 | ||
| Nurse Specialist | 3 | 23.10 | |||
| Did you have some train in pain assessment/ management before this participation? | No | 10 | 76.90 | ||
| Yes | 3 | 23.10 | |||
| Do you believe it is important to receive training in pain management? | Yes | 13 | 100.00 |
| M | SD | Max | Min | ||
|---|---|---|---|---|---|
| How is your satisfaction level from (0–10), with the protocol implemented? | 7.92 | 1.32 | 10 | 5 | |
| n | % | ||||
| Do you believe it is important to assess pain during the HD treatment? | Important | 5 | 38.50 | ||
| Very Important | 8 | 61.50 | |||
| Do you agree it is important to have a pain assessment protocol during the HD treatment? | Yes | 13 | 100.00 | ||
| How do you rate the suitability of the protocol implemented for the clinical context? | Not Suitable | 2 | 15.40 | ||
| Suitable | 9 | 69.20 | |||
| Very Suitable | 2 | 15.40 | |||
| In your opinion, is patients’ pain management more effective after protocol implementation? | Yes | 13 | 100.00 | ||
| Do you think your approach to patients with pain has improved since the protocol implementation? | Yes | 12 | 92.30 | ||
| No | 1 | 7.70 | |||
| Was the protocol able to give visibility to pain assessment during the HD treatment? | Yes | 13 | 100.00 | ||
| Did you find the protocol easy to apply during the HD treatment? | Yes | 12 | 92.30 | ||
| No | 1 | 7.70 | |||
| Do you agree that the protocol is effective for assessing pain during the HD treatment? | Yes | 12 | 92.30 | ||
| No | 1 | 7.70 | |||
| Do you agree that the protocol has been properly implemented? | Yes | 12 | 92.30 | ||
| No | 1 | 7.70 | |||
| Do you agree that adequate training/support has been given during the protocol implementation? | Yes | 11 | 84,60 | ||
| No | 2 | 15.40 | |||
| Do you believe that the protocol has contributed to improving patient care? | Yes | 13 | 100.00 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodrigues, R.; Costeira, C. Pain Assessment in Patients during Hemodialysis Treatment: Quality Improvement Project. Nurs. Rep. 2024, 14, 1370-1387. https://doi.org/10.3390/nursrep14020103
Rodrigues R, Costeira C. Pain Assessment in Patients during Hemodialysis Treatment: Quality Improvement Project. Nursing Reports. 2024; 14(2):1370-1387. https://doi.org/10.3390/nursrep14020103
Chicago/Turabian StyleRodrigues, Rita, and Cristina Costeira. 2024. "Pain Assessment in Patients during Hemodialysis Treatment: Quality Improvement Project" Nursing Reports 14, no. 2: 1370-1387. https://doi.org/10.3390/nursrep14020103
APA StyleRodrigues, R., & Costeira, C. (2024). Pain Assessment in Patients during Hemodialysis Treatment: Quality Improvement Project. Nursing Reports, 14(2), 1370-1387. https://doi.org/10.3390/nursrep14020103