
Clinical Trial for Cartilage Conduction Hearing Aid in Indonesia

 ,
,
Abstract
:1. Introduction
2. Method
2.1. Participants
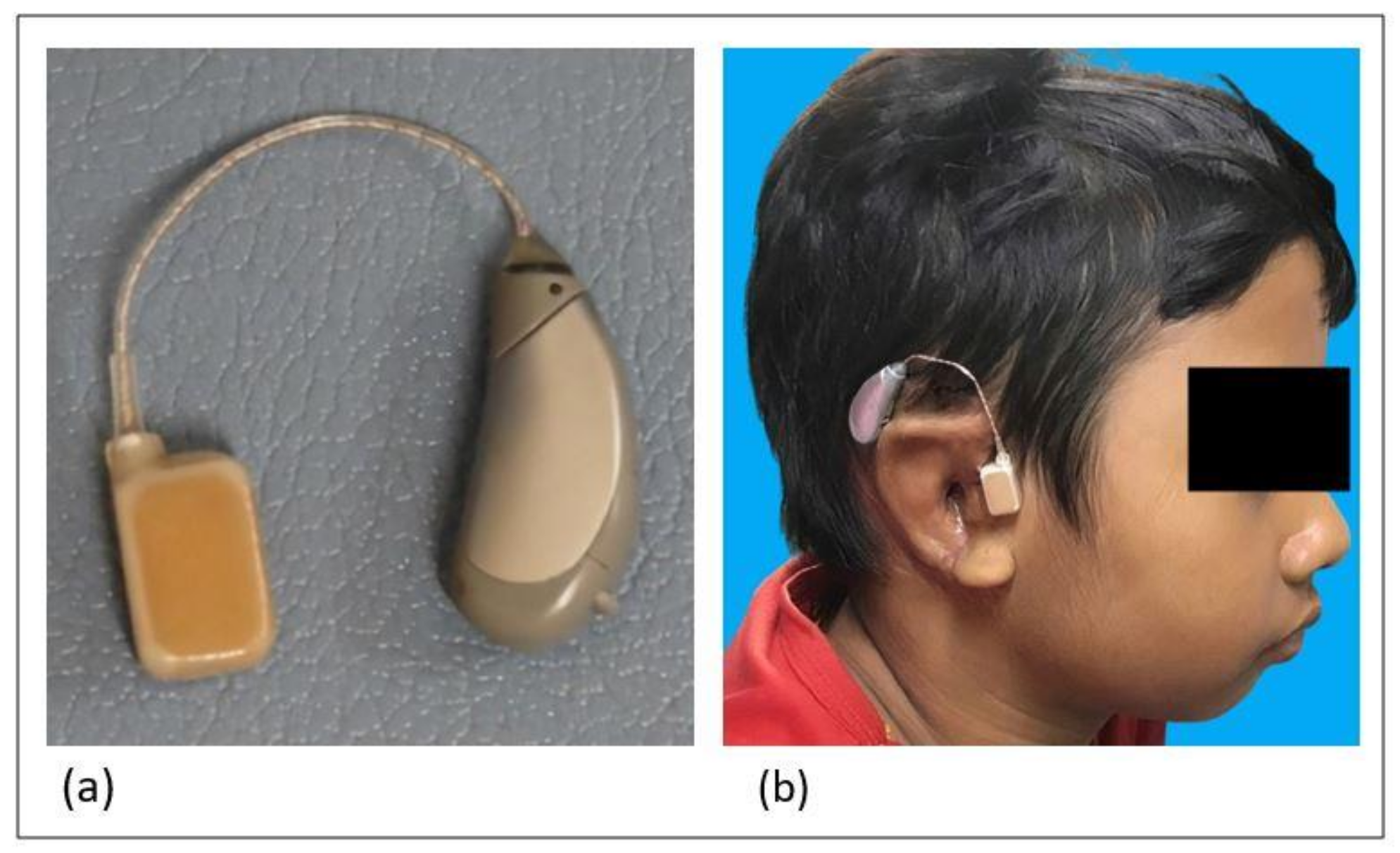
2.2. CCHA Fitting and Evaluations
3. Results
4. Discussions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sanjib, T.; Meng, X. Treatment of Microtia: Past, Present and Future. J. Southeast Univ. 2015, 34, 485–488. [Google Scholar] [CrossRef]
- Pellinen, J.; Vasama, J.P.; Kivekäs, I. Long-term Results of Atresiaplasty in Patients with Congenital Aural Atresia. Acta Oto-Laryngol. 2018, 138, 1–4. [Google Scholar] [CrossRef] [Green Version]
- Håkansson, B.; Tjellström, A.; Rosenhall, U. Hearing Thresholds with Direct Bone Conduction Versus Conventional Bone Conduction. Scand Audiol. 1984, 13, 3–13. [Google Scholar] [CrossRef] [PubMed]
- House, J.W.; Kutz, J.W. Bone-anchored Hearing Aids: Incidence and Management of Postoperative Complications. Otol. Neurotol. 2007, 28, 213–217. [Google Scholar] [CrossRef] [PubMed]
- Hobson, J.C.; Roper, A.J.; Andrew, R.; Rothera, M.P.; Hill, P.; Green, K.M. Complications of Bone-anchored Hearing Aid Implantation. J. Laryngol. Otol. 2010, 124, 132–136. [Google Scholar] [CrossRef]
- Chang, S.O.; Choi, B.Y.; Hur, D.G. Analysis of the Long-Term Hearing Results After the Surgical Repair of Aural Atresia. Laryngoscope 2006, 116, 1835–1841. [Google Scholar] [CrossRef] [PubMed]
- Başerer, N. The Experience Outcomes of the Cosmetic and Functional Surgery in Congenital Aural Atresia. Clin. Surg. 2017, 2, 1–5. [Google Scholar]
- Hosoi, H.; Yanai, S.; Nishimura, T.; Sakaguchi, T.; Iwakura, T.; Yoshino, K. Development of cartilage con-duction hearing aid. Arch. Mat. Sci. Eng. 2010, 42, 104–110. [Google Scholar]
- Nishimura, T.; Hosoi, H.; Saito, O.; Miyamae, R.; Shimokura, R.; Matsui, T.; Iwakura, T. Benefit of a New Hearing Device Utilizing Cartilage Conduction. Auris Nasus Larynx 2013, 40, 440–446. [Google Scholar] [CrossRef]
- Shimokura, R.; Hosoi, H.; Iwakura, T.; Nishimura, T.; Matsui, T. Development of monaural and binaural behind-the-ear cartilage conduction hearing aids. Appl. Acoust. 2013, 74, 1234–1240. [Google Scholar] [CrossRef]
- Nishimura, T.; Hosoi, H.; Sugiuchi, T.; Matsumoto, N.; Nishiyama, T.; Takano, K.; Sugimoto, S.; Yazama, H.; Sato, T.; Komori, M. Cartilage conduction hearing aid fitting in clinical practice. J. Am. Acad. Audiol. 2021, in press. [Google Scholar]
- Nishimura, T.; Hosoi, H.; Saito, O.; Shimokura, R.; Yamanaka, T.; Kitahara, T. Cartilage Conduction Hearing Aids for Severe Conduction Hearing Loss. Otol. Neurotol. 2018, 39, 65–72. [Google Scholar] [CrossRef]
- Nishimura, T.; Hosoi, H.; Saito, O.; Miyamae, R.; Shimokura, R.; Matsui, T.; Yamanaka, T.; Levitt, H. Is cartilage conduction classified into air or bone conduction? Laryngoscope. 2014, 124, 1214–1219. [Google Scholar] [CrossRef] [PubMed]
- Shimokura, R.; Hosoi, H.; Nishimura, T.; Yamanaka, T.; Levitt, H. Cartilage conduction hearing. J. Acoust Soc. Am. 2014, 135, 1959–1966. [Google Scholar] [CrossRef] [PubMed]
- Nishimura, T.; Hosoi, H.; Saito, O.; Miyamae, R.; Shimokura, R.; Yamanaka, T.; Kitahara, T.; Levitt, H. Cartilage conduction is characterized by vibrations of the cartilaginous portion of the ear canal. PLoS ONE 2015, 10, e0120135. [Google Scholar] [CrossRef]
- Nishimura, T.; Hosoi, H.; Saito, O.; Miyamae, R.; Shimokura, R.; Matsui, T.; Yamanaka, T.; Kitahara, T.; Levitt, H. Cartilage conduction efficiently generates airborne sound in the ear canal. Auris Nasus Larynx. 2015, 42, 15–19. [Google Scholar] [CrossRef] [Green Version]
- Miyamae, R.; Nishimura, T.; Hosoi, H.; Saito, O.; Shimokura, R.; Yamanaka, T.; Kitahara, T. Perception of speech in cartilage conduction. Auris Nasus Larynx. 2017, 44, 26–32. [Google Scholar] [CrossRef]
- Nishimura, T.; Miyamae, R.; Hosoi, H.; Saito, O.; Shimokura, R.; Yamanaka, T.; Kitahara, T. Frequency characteristics and speech recognition in cartilage conduction. Auris Nasus Larynx. 2019, 46, 709–715. [Google Scholar] [CrossRef]
- Nishimura, T.; Hosoi, H.; Saito, O.; Akasaka, S.; Shimokura, R.; Yamanaka, T.; Kitahara, T. Effect of fixation place on airborne sound in cartilage conduction. J. Acoust. Soc. Am. 2020, 148, 469. [Google Scholar] [CrossRef]
- Nishimura, T.; Hosoi, H.; Shimokura, R.; Morimoto, C.; Kitahara, T. Cartilage Conduction Hearing and Its Clinical Application. Audiol. Res. 2021, 11, 254–262. [Google Scholar] [CrossRef]
- Hosoi, H.; Nishimura, T.; Shimokura, R.; Kitahara, T. Cartilage conduction as the third pathway for sound transmission. Auris Nasus Larynx. 2019, 46, 151–159. [Google Scholar] [CrossRef] [Green Version]
- Nishimura, T.; Hosoi, H.; Saito, O.; Shimokura, R.; Yamanaka, T.; Kitahara, T. Sound localisation ability using cartilage conduction hearing aids in bilateral aural atresia. Int. J. Audiol. 2020, 59, 891–896. [Google Scholar] [CrossRef]
- Morimoto, C.; Nishimura, T.; Hosoi, H.; Saito, O.; Fukuda, F.; Shimokura, R.; Yamanaka, T. Sound transmis-sion by cartilage conduction in ear with fibrotic aural atresia. J. Rehabil. Res. Dev. 2014, 51, 325–332. [Google Scholar] [CrossRef] [PubMed]
- Nishiyama, T.; Oishi, N.; Ogawa, K. Who are good adult candidates for cartilage conduction hearing aids? Eur. Arch. Otorhinolaryngol. 2020, in press. [Google Scholar] [CrossRef] [PubMed]
- Nishiyama, T.; Oishi, N.; Ogawa, K. Efficacy of cartilage conduction hearing aids in children. Int. J. Pediatr Otorhinolaryngol. 2021, 142, 110628. [Google Scholar] [CrossRef]
- Komune, N.; Higashino, Y.; Ishikawa, K.; Tabuki, T.; Masuda, S.; Koike, K.; Hongo, T.; Sato, K.; Uchi, R.; Miyazaki, M.; et al. Management of Residual Hearing with Cartilage Conduction Hearing Aid after Lateral Temporal Bone Resection: Our Institutional Experience. Audiol. Res. 2021, 11, 263–274. [Google Scholar] [CrossRef] [PubMed]
- Akasaka, S.; Nishimura, T.; Hosoi, H.; Saito, O.; Shimokura, R.; Morimoto, C.; Kitahara, T. Benefits of Cartilage Conduction Hearing Aids for Speech Perception in Unilateral Aural Atresia. Audiol. Res. 2021, 11, 284–290. [Google Scholar] [CrossRef] [PubMed]
- Li, D.; Chin, W.; Wu, J.; Zhang, Q.; Xu, F.; Zhang, R. Psychosocial Outcomes Among Microtia Patients of Different Ages and Genders Before Ear Reconstruction. Aesthetic Plast. Surg. 2010, 34, 570–576. [Google Scholar] [CrossRef] [PubMed]
- Sleifer, P.; Didoné, D.D.; Keppeler, Í.B.; Bueno, C.D.; Riesgo, R.D.S. Air and Bone Conduction Frequency-specific Auditory Brainstem Response in Children with Agenesis of the External Auditory Canal. Int. Arch. Otorhinolaryngol. 2017, 21, 318–322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gazia, F.; Galletti, B.; Portelli, D.; Alberti, G.; Freni, F.; Bruno, R.; Galletti, F. Real ear measurement (REM) and auditory performances with open, tulip and double closed dome in patients using hearing aids. Eur. Arch. Otorhinolaryngol. 2020, 277, 1289–1295. [Google Scholar] [CrossRef] [PubMed]
- Shimokura, R.; Hosoi, H.; Nishimura, T.; Iwakura, T.; Yamanaka, T. Simulating cartilage conduction sound to estimate the sound pressure level in the external auditory canal. J. Sound. Vib. 2015, 20, 261–268. [Google Scholar] [CrossRef]
- Shimokura, R.; Nishimura, T.; Hosoi, H. Vibrational and Acoustical Characteristics of Ear Pinna Simulators that Differ in Hardness. Audiol. Res. 2021, 11, 327–334, in press. [Google Scholar] [CrossRef]

{kind=link}
| Patient | Sex | Age (Year) | Pure Tone/Behavioral Audiometry (dB HL) [500, 1000, 2000, 4000 Hz] | TB Bone ABR (dB nHL) | Degree of Conductive Hearing Loss | |||
|---|---|---|---|---|---|---|---|---|
| R | L | R | L | R | L | |||
| 1 | F | 13 | 107.5/ 67.5 | 101.3/ 68.8 | - | - | Profound/ Severe | Profound/ Severe |
| 2 | M | 9 | NA/ 50 | NA/ 50 | - | - | - Moderate | - Moderate |
| 3 | F | 14 | 66.3/ 62.5 | 62.5/ 53.8 | - | - | Severe/ Severe | Severe/ Moderate |
| 4 | F | 10 | NA | NA | 60 | 60 | Severe | Severe |
| 5 | M | 9 | NA | NA | 55 | 65 | Moderate | Severe |
| 6 | M | 12 | 60.0/ 51.3 | 61.3/ 56.3 | - | - | Severe/ Moderate | Severe/ Moderate |
| 7 | F | 13 | 70.0/ 32.5 | 58.8/ 28.8 | - | - | Severe/ Mild | Moderate/ Mild |
| 8 | F | 19 | Normal/ Normal | 68.8/ 70.0 | - | - | Normal/ Normal | Severe/ Severe |
| 9 | F | 15 | Normal/ Normal | 82.5/ 82.5 | - | - | Normal/Normal | Severe/Severe |
| 10 | F | 10 | 61.3/ 68.8 | 65.0/ 65.0 | - | - | Severe/ Severe | Severe/ Severe |
| Patient | Ear-Chip | DFT | Ear | Unaided/ Aided Thresholds (dB HL) | Functional Gain (dB) | Unaided/ Aided SRTs (dB HL) | SRT-I (dB) | Unaided/ Aided SDLs (dB HL) | SDL-I (dB) |
|---|---|---|---|---|---|---|---|---|---|
| 1 | No | Yes | R | NC/90 | NC | NC | NC | NC | NC |
| No | Yes | L | NC/68.8 | NC | NC | NC | NC | NC | |
| 2 | No | Yes | R | 50/27.5 | 22.5 | 68/46 | 22 | 100/60 | 40 |
| No | Yes | L | 50.0/28.8 | 21.3 | 72/47 | 25 | 100/60 | 40 | |
| 3 | No | Yes | R | 52.5/31.3 | 21.3 | 93/49 | 44 | NC/90 | - |
| Yes | No | L | 48.8/37.5 | 11.3 | 82/60 | 22 | 100/80 | 20 | |
| 4 | No | Yes | R | 66.3/31.3 | 35.0 | NC | NC | NC | NC |
| No | Yes | L | 63.8/25.0 | 38.8 | NC | NC | NC | NC | |
| 5 | Yes | No | R | NC | NC | NC | NC | NC | NC |
| Yes | No | L | NC | NC | NC | NC | NC | NC | |
| 6 | No | Yes | R | 50.0/27,5 | 22.5 | 75/30 | 45 | ?/60 | - |
| No | Yes | L | 50.0/28.8 | 21.3 | 92/28 | 64 | 100/60 | 40 | |
| 7 | No | Yes | R | 65.0/38.8 | 26.3 | 81/42 | 39 | 90/50 | 40 |
| No | Yes | L | 56.3/30.0 | 26.3 | 73/37 | 36 | 80/50 | 30 | |
| 8 | - | - | R | Normal | - | - | - | - | - |
| No | Yes | L | 68.8/38.8 | 30.0 | 74/50 | 24 | 90/60 | 30 | |
| 9 | - | - | R | Normal | - | - | - | - | - |
| No | Yes | L | 76.3/30.0 | 46.3 | 85/50 | 35 | 90/60 | 30 | |
| 10 | No | Yes | R | 57.5/32.5 | 25.0 | 76/28 | 48 | 90/50 | 40 |
| No | Yes | L | 61.3/32.5 | 28.8 | 75/42 | 33 | 90/50 | 40 |
| Unaided Threshold (n = 14) | Aided Threshold (n = 14) | Functional Gain (95% Confidence Interval) | P Value (Paired T-Test) |
|---|---|---|---|
| 58.3 ± 2.3 dB HL | 31.4 ± 1.1 dB HL | 26.9 ± 2.3 dB | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Suwento, R.; Widodo, D.W.; Airlangga, T.J.; Alviandi, W.; Watanuki, K.; Nakanowatari, N.; Hosoi, H.; Nishimura, T. Clinical Trial for Cartilage Conduction Hearing Aid in Indonesia. Audiol. Res. 2021, 11, 410-417. https://doi.org/10.3390/audiolres11030038
Suwento R, Widodo DW, Airlangga TJ, Alviandi W, Watanuki K, Nakanowatari N, Hosoi H, Nishimura T. Clinical Trial for Cartilage Conduction Hearing Aid in Indonesia. Audiology Research. 2021; 11(3):410-417. https://doi.org/10.3390/audiolres11030038
Chicago/Turabian StyleSuwento, Ronny, Dini Widiarni Widodo, Tri Juda Airlangga, Widayat Alviandi, Keisuke Watanuki, Naoko Nakanowatari, Hiroshi Hosoi, and Tadashi Nishimura. 2021. "Clinical Trial for Cartilage Conduction Hearing Aid in Indonesia" Audiology Research 11, no. 3: 410-417. https://doi.org/10.3390/audiolres11030038
APA StyleSuwento, R., Widodo, D. W., Airlangga, T. J., Alviandi, W., Watanuki, K., Nakanowatari, N., Hosoi, H., & Nishimura, T. (2021). Clinical Trial for Cartilage Conduction Hearing Aid in Indonesia. Audiology Research, 11(3), 410-417. https://doi.org/10.3390/audiolres11030038