
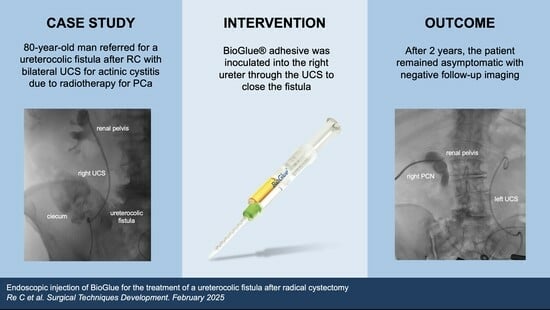
Endoscopic Injection of BioGlue for the Treatment of a Ureterocolic Fistula After Radical Cystectomy

 , , ,
, , ,
Abstract
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
1. Introduction
2. Case Presentation
2.1. Patient Characteristics and Clinical Findings
2.2. Treatment
2.3. Outcome and Follow-Up
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Smith, Z.L.; Johnson, S.C.; Golan, S.; McGinnis, J.R.; Steinberg, G.D.; Smith, N.D. Fistulous Complications following Radical Cystectomy for Bladder Cancer: Analysis of a Large Modern Cohort. J. Urol. 2018, 199, 663–668. [Google Scholar] [CrossRef] [PubMed]
- Mastromichalis, M.H.; Frazzini, P.; Newall, P.M. Successful endoscopic management of a chronic transplant ureterocutaneous fistula. Urology 2011, 78, 952–953. [Google Scholar] [PubMed]
- Bahouth, Z.; Moskovitz, B.; Halachmi, S.; Nativ, O. Bovine serum albumin-glutaraldehyde (BioGlue®) tissue adhesive versus standard renorrhaphy following renal mass enucleation: A retrospective comparison. Ther. Adv. Urol. 2017, 9, 67–72. [Google Scholar] [PubMed]
- Msezane, L.; Reynolds, W.S.; Mhapsekar, R.; Gerber, G.; Steinberg, G. Open surgical repair of ureteral strictures and fistulas following radical cystectomy and urinary diversion. J. Urol. 2008, 179, 1428–1431. [Google Scholar] [CrossRef]
- Scozzari, G.; Arezzo, A.; Morino, M. Enterovesical fistulas: Diagnosis and management. Tech. Coloproctol. 2010, 14, 293–300. [Google Scholar] [CrossRef] [PubMed]
- Ng, C.S.; Klein, E.A. Conservative management of an ileal neobladder-enteric fistula. Urology 1999, 54, 366. [Google Scholar] [CrossRef] [PubMed]
- El Khader, K.; Karmouni, T.; Guillé, F.; Lobel, B. Ureteroileal fistula: An unusual complication of Crohn’s disease. Acta Gastroenterol. Belg. 2000, 63, 312–313. [Google Scholar] [PubMed]
- Leicht, W.; Thomas, C.; Thüroff, J.; Roos, F. Colovesical fistula caused by diverticulitis of the sigmoid colon: Diagnosis and treatment. Urologe A 2012, 51, 971–974. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.K.; Chang, S.D.; Roche, C.J.; Duddalwar, V.A.; Rowley, V.A.; McLoughlin, M.G. Spontaneous ureterocolic fistula secondary to calculous pyohydroureteronephrosis. Br. J. Radiol. 2005, 78, 954–955. [Google Scholar] [CrossRef] [PubMed]
- Bioglue CryoLife Inc. BioGlue Surgical Adhesive; Medical Information; IFU for BioGlue Surgical Adhesive (USA). Available online: https://www.accessdata.fda.gov/cdrh_docs/pdf/p010003b.pdf (accessed on 2 February 2020).
- Mitrev, Z.; Belostotskii, V.; Hristov, N. Suture line reinforcement using suction-assisted bioglue application during surgery for acute aortic dissection. Interact. Cardiovasc. Thorac. Surg. 2007, 6, 147–149. [Google Scholar] [CrossRef] [PubMed]
- Garcia, S.; Dissanaike, S. Case report: Treatment of rectovaginal fistula with Bioglue(®). Int. J. Surg. Case Rep. 2012, 3, 327–329. [Google Scholar] [CrossRef] [PubMed]
- Van Koperen, P.J.; Bemelman, W.A.; Gerhards, M.F.; Janssen, L.W.; van Tets, W.F.; van Dalsen, A.D.; Slors, J.F.M. The anal fistula plug treatment compared with the mucosal advancement flap for cryptoglandular high transsphincteric perianal fistula: A double-blinded multicenter randomized trial. Dis. Colon. Rectum. 2011, 54, 387–393. [Google Scholar] [CrossRef] [PubMed]
- Hidas, G.; Kastin, A.; Mullerad, M.; Shental, J.; Moskovitz, B.; Nativ, O. Sutureless nephron-sparing surgery: Use of albumin glutaraldehyde tissue adhesive (BioGlue). Urology 2006, 67, 697–700; discussion 700. [Google Scholar] [CrossRef] [PubMed]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Re, C.; Scilipoti, P.; Rosiello, G.; Leggio, N.; Avesani, G.; Matloob, R.; Salonia, A.; Montorsi, F.; Bertini, R. Endoscopic Injection of BioGlue for the Treatment of a Ureterocolic Fistula After Radical Cystectomy. Surg. Tech. Dev. 2025, 14, 11. https://doi.org/10.3390/std14020011
Re C, Scilipoti P, Rosiello G, Leggio N, Avesani G, Matloob R, Salonia A, Montorsi F, Bertini R. Endoscopic Injection of BioGlue for the Treatment of a Ureterocolic Fistula After Radical Cystectomy. Surgical Techniques Development. 2025; 14(2):11. https://doi.org/10.3390/std14020011
Chicago/Turabian StyleRe, Chiara, Pietro Scilipoti, Giuseppe Rosiello, Nicola Leggio, Giulio Avesani, Rayan Matloob, Andrea Salonia, Francesco Montorsi, and Roberto Bertini. 2025. "Endoscopic Injection of BioGlue for the Treatment of a Ureterocolic Fistula After Radical Cystectomy" Surgical Techniques Development 14, no. 2: 11. https://doi.org/10.3390/std14020011
APA StyleRe, C., Scilipoti, P., Rosiello, G., Leggio, N., Avesani, G., Matloob, R., Salonia, A., Montorsi, F., & Bertini, R. (2025). Endoscopic Injection of BioGlue for the Treatment of a Ureterocolic Fistula After Radical Cystectomy. Surgical Techniques Development, 14(2), 11. https://doi.org/10.3390/std14020011