Abstract
Background: Facial features are the first basic sign of medical knowledge of children and adults with congenital malformations. Children born with multiple contractures almost always receive the misdiagnosis of arthrogryposis multiplex. Larsen syndrome can easily be diagnosed at birth via the proper interpretations of its characteristic facial features and multiple dislocations. Comprehensive clinical diagnosis can facilitate an orthopedic strategy for early treatment and can enhance the recognition of unreported craniocervical malformation complexes. Material and Methods: Six children (four boys and two girls, with ages ranging from a few months to 7 years old) were referred to our department for diagnosis and treatment. All children received their first misdiagnosis by the pediatricians as manifesting arthrogryposis multiplex congenita. The clinical phenotype was our first decisive tool for diagnosis. All children exhibited the classical phenotype of dish-like facies associated with multiple joint dislocations. Radiological phenotypic characteristics confirmed our clinical diagnosis of Larsen syndrome. Three children out of six showed unpleasant cervical spine deformities. The first child, a 2-year-old, became tetraplegic after minor trauma. One child presented with progressive rigid cervical kyphosis. The third child was a product of a first-relative marriage and was born with congenital tetraplegia. A genotype was carried out for confirmation. Results: Three children underwent open reduction for congenital hip and knee dislocations. One child underwent spinal fusion CO-C7 because of tetraplegia. A 3D-reformatted and reconstruction CT scan of the craniocervical junction showed two forms of unusual dys-segmentation, firstly along C2-3 effectively causing the development of acute-angle cervical kyphosis. Secondly, an infant with congenital tetraplegia showed a serious previously undescribed atlanto–axial malformation complex. Namely, atlanto–axial maldevelopment (dys-segmentation) of (C1/C2) was associated with hypoplasia of the anterior and the posterior rings of the atlas. Genetic tests of these children were compatible with the autosomal dominant type of Larsen syndrome and manifested a heterozygous mutation in FLNB mapped 3p14.3, encoding an actin-binding protein, filamin B. The child with congenital tetraplegia showed no mutations in FLNB, though his clinical and radiological phenotype and his family history of first-relative marriage were totally compatible with the diagnosis of the autosomal recessive type of Larsen syndrome. Conclusions: Our strategy was and still is based on a coherent clinical and radiological diagnosis, which is based on comprehensive clinical and radiological phenotypic characterizations. We implemented a 3D-reformatted CT scan to further understand the craniocervical junction pathology in three children. Strikingly, prenatal onset of lethal maldevelopment (dys-segmentation) of the atlanto–axial spine segments has been diagnosed in an infant with congenital tetraplagia. A less serious cervical spine malformation was detected in two children who presented with progressive acute-angle cervico and cervico-thoracic kyphosis. Our clinical strategy can form the basis for a thorough clinical assessment for infants and children born with multiple malformation complexes and can lead to recognition of novel understandings.
1. Introduction
Larsen et al. (OMIM: 150250) described multiple congenital large joint dislocations associated with a distinctive facial phenotypic characterization in six unrelated patients [1]. The most striking findings were a typical flattened “dish-like” facies, bilateral dislocations of multiple joints, and equinovarus deformities of the feet. Larsen syndrome is characterized by distinctive facies (flat face, hypertelorism, depressed nasal bridge, prominent forehead, cleft palate, and cleft uvula). Ligamentous hyperlaxity of the joints is associated with dislocated elbows, hips, and knees (genu recurvatum) [1,2,3]. The phenotype of the hands is characteristic cylindrical fingers, spatulate-like thumbs, and short and broad fingertips, and in some cases multiple wrist ossification centers can be encountered. The foot is characterized by a resistant type of clubfoot deformity, though the radiological phenotype can be diagnostic via the presence of a juxta-calcaneal accessory bone or bifid calcaneus [3,4,5,6]. A remarkable number of children with Larsen syndrome present with sensorineural or mixed hearing loss associated with abnormal ear anatomy. Other forms of dislocations have been encountered such as dislocation of the malleus and incus [6,7]. Abnormalities of the central nervous system were part of the syndrome in some patients (neurological impairment in connection with cord compression, hydrocephalus, intellectual disability, and subependymal glial proliferation of the lateral ventricle can mimic tuberous sclerosis) [8]. The joint deformities associated with ligamentous hyperlaxity include dislocations of the hip, anterior dislocations of the knee, dislocations of the radial head, and dislocation of the patella as well as the wrist, shoulder, the carpometacarpal joint of the thumb, and even the superior tibio-fibular joint [9,10]. Congenital talipes equinovarus is not an uncommon occurrence in children with Larsen syndrome [11]. Life-threatening congenital heart defects of aortic dilatation and valvular insufficiency and aneurysm of the ductus arteriosus have been described [12,13]. Spine abnormalities include dys-segmentation and craniocervical instability [14,15,16]. The progressive spine deformities may lead to progressive kyphosis and lordosis and eventually in some cases death [17]. At the lumbo–sacral junction, the neural arches may show maldevelopment associated with narrow interpedicular distances. Scoliosis develops in early childhood and can be progressive (fusion is preferably performed by the age of 10 years). The gene has been located—it is filamin B, and children showed heterozygosity for de novo mutations in FLNB gene (OMIM 603381) [18], though the same mutated gene has been diagnosed in children with atelosteogenesis types I and III and in spondylocarpotarsal syndromes. Mutations seem to cluster in about 5 of the 46 exons [19]. Autosomal recessive-type Larsen syndrome has been diagnosed in children with a CHST3 gene mutation [20].
2. Materials and Methods
The study protocol was approved by the Ethics Committee of the (Ilizarov Scientific Research Institute, No. 4(50)/13.12.2016, Kurgan, Russia). Informed consents were obtained from the patients’ guardians. Six children (four boys and two girls, age range of a few months to 7 years) were referred to our departments for diagnosis and treatment. In Larsen syndrome, pediatricians as well as orthopedic surgeons may be confronted with one of the most confusing and challenging constellations of musculo-skeletal deformities. The first and foremost clinical confusion is the initiation of the false diagnosis of arthrogryposis multiplex congenita (AMC). AMC when seen in children with generalized ligamentous hyperlaxity associated with alterations in muscle tone can easily be misunderstood as hypotonia. This sort of misconception drove the medical group to direct their clinical potential toward listing these children within the category of floppy infant syndrome. Untrained pediatricians have immense difficulties differentiating between hypotonia and ligamentous hyperlaxity. Similarly, Downs syndrome (trisomy 21) and endocrinopathies are the common false diagnoses for infants with dysmorphic facial features. Therefore, unnecessary investigations are implemented to confirm or rule out neuromuscular disorders. The outcome of false diagnosis with subsequent irrelevant investigations can represent a heavy burden on parents. Structured questionnaires and history taking are the fundamental elements of diagnosis. In particular, information on maternal gestational history of miscarriages, bleeding in the first trimester, feeble in utero movement, stillbirths, eclampsia, hydro/oligo-hydraminious and history of difficulties with conceiving such as history of primary or secondary sterility is collected. Unusual events in gestational histories such as infections (toxoplasmosis, cytomegalovirus, AIDS virus, and so forth) are also collected. Full details regarding the labor circumstances (history of breech delivery, fetal distress, and cyanosis) and measurements of the baby’s growth parameters are other data collected. Family history of medical pathologies, operations, interventions, skeletal dysplasia, metabolic bone disorders, and syndromic association complexes are also collected. A careful clinical inspection is conducted for craniofacial abnormalities, general physique and build, upper limbs, lower limbs, contractures, and the spine in conjunction with comprehensive radiological phenotypic characterization to detect additional pathologic features. DNA is extracted from whole blood using standard procedures. FLNB exons and exon–intron boundaries are amplified using a polymerase chain reaction as described by previous studies [20]. We recognized a heterozygous mutation in FLNB mapped on 3p14.3, encoding an actin-binding protein, and missense mutations in four children have been encountered (all showed pathological changes with point mutations suggesting amin acid substitution). It is well known that mutations in FLNB can also be encountered in other disorders of skeletal dysplasia, such as spondylocarpotarsal, atelosteogenesis I and III, and Boomerang syndrome. The aforementioned disorders can easily be distinguished from Larsen syndrome, through the distinctive craniofacial features and the associated multiple joint dislocations.
We identified a causative FLNB mutation in each of the five unrelated patients and the mother-son duo with LS. All alterations are point mutations predicting an amino acid substitution.
3. Results
3.1. The Classical Clinical and Radiological Phenotype in Children with Larsen Syndrome
In these children, dysmorphic facial features were evident, which encompassed distinctive facial features, frontal bossing, and a flattened nasal bridge giving the facial phenotype of a dish-like facies. Our orthopedic strategy is based upon detailed clinical and radiological phenotypic characterization. Radiological phenotypic interpretations have been organized for all children by referring to 3D CT scan. In a lateral skull radiograph of a 7-month-old boy with Larsen syndrome, one can note brachycephaly, frontal bossing, and marked disproportionate small facial bones in comparison with a large cranium and dysplastic cervical spine, osteopenia of the lambdoid bones causing downward bulging, and prominence of the occipital bone associated with progressive thinning of the squamous part of the occipital bone (arrow). One can also note the cervical kyphosis (arrow) AP hand radiograph of a 3-year-old boy with Larsen syndrome showing retarded bone age, expansion of the distal ends of the shortened metacarpals, a thumb proximally placed, and the presence of accessory bone adjacent to the distal third metacarpal-phalangeal bone (arrow). One can also see the delta phalanx of the middle metacarpophalangeal bone of the fifth finger (arrow) (b) (Figure 1a,b). The AP pelvis radiograph of a 7-month-old girl with Larsen syndrome showed bilateral hip dislocation associated with maldevelopment of a severely dysplastic acetabulum and dysplastic capital femoral epiphysis (a). The AP pelvis radiograph of a 3-year-old boy with Larsen syndrome showed bilateral hip dislocations (severe acetabulo-femoral dysplasia) (Figure 2a). The AP pelvis radiograph of a 7-month-old girl with Larsen syndrome showed bilateral hip dislocation associated with maldevelopment of a severely dysplastic acetabulum and dysplastic capital femoral epiphysis (a). The AP pelvis radiograph of a 3-year-old boy with Larsen syndrome showed bilateral hip dislocations (severe acetabulo-femoral dysplasia) (Figure 2b). AP knees radiograph of a 5-month-old boy with Larsen syndrome showing bilateral knee dislocations (arrows) associated with under tubulation of the tibae and fibulae. Note the fragmented/deformed epiphyses and that the right tibia is medially subluxated. Note bilateral talipes equinivarus associated with double ossifications of the calcaneus (arrows) (Figure 3).
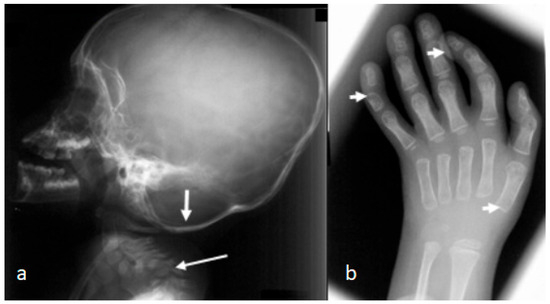
Figure 1.
(a,b): Lateral skull radiograph of a 7-month-old boy with Larsen syndrome. Note brachycephaly, frontal bossing, and marked disproportionate small facial bones in comparison with a large cranium and dysplastic cervical spine, osteopenia of the lambdoid bones causing downward bulging, and prominence of the occipital bone associated with progressive thinning of the squamous part of the occipital bone (arrow). Note the cervical kyphosis (arrow) AP hand radiograph of a 3-year-old boy with Larsen syndrome showing retarded bone age, expansion of the distal ends of the shortened metacarpals, a thumb proximally placed, and the presence of accessory bone adjacent to the distal third metacarpal-phalangeal bone (arrow). Delta phalanx of the middle metacarpophalangeal bone of the fifth finger (arrow) (b).
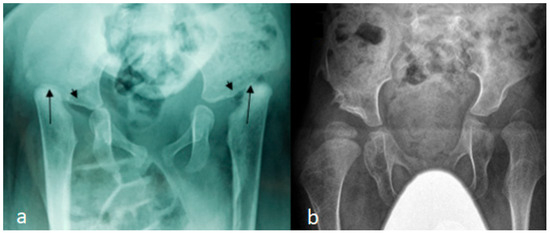
Figure 2.
(a,b): AP pelvis radiograph of a 7-month-old girl with Larsen syndrome showing bilateral hip dislocation associated with maldevelopment of severely dysplastic acetabulum and dysplastic capital femoral epiphysis (arrows) (a). AP pelvis radiograph of a 3-year-old boy with Larsen syndrome showing bilateral hip dislocations (severe acetabulo-femoral dysplasia) (b).
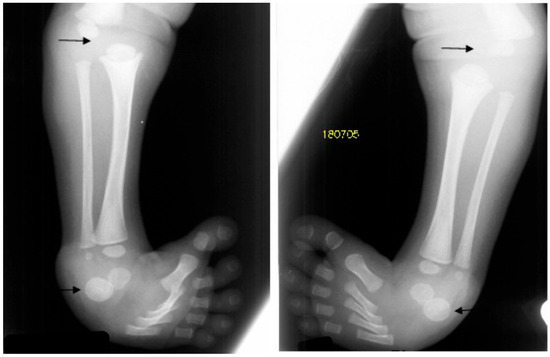
Figure 3.
AP knees radiograph of a 5-month-old boy with Larsen syndrome showing bilateral knee dislocations (arrows) associated with under tubulation of the tibae and fibulae. Note the fragmented/deformed epiphyses and that the right tibia is medially subluxated. Note bilateral talipes equinivarus associated with double ossifications of the calcaneus (arrows).
3.2. Congenital Tetraplegia in a Child with Larsen Syndrome
Congenital tetraplegia has been never described in children with Larsen syndrome. The overall clinical criteria of the lethal type of Larsen syndrome, which is characterized by immediate death after birth, is not consistent with our current child. However, no CT scan studies for the craniocervical junctions have been described in the lethal type of Larsen syndrome.
A 3D-reformatted sagittal CT scan of the cranium shows a six-month-old-child who was born with congenital tetraplegia. Maldevelopment of the anterior ring of the atlas C1, which has been displaced along the superior surface of the clivus, is also evident. Also, the (odontoid process is hypoplastic and dislocated and 9s located between the maldeveloped anterior rings) (arrow head). Fusion of the fragmented anterior and posterior rings of C1 and fusion of these fragments effect the development of a bifurcation-like structure (Figure 4a). An axial 3D-reformatted CT scan shows congenital maldevelopment of the anterior arch of the atlas and fusion of the remnants of anterior ring with the lateral mass of C1 (forming a Y-shaped deformity) (arrow head). The posterior ring of C1 is hypoplastic, resembling a Jefferson fracture (arrow head) (Figure 4b).
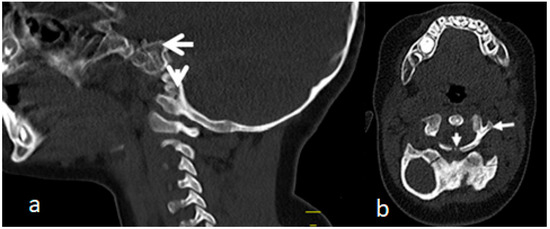
Figure 4.
(a,b). A 3D-reformatted sagittal CT scan of the cranium in a six-month-old child with Larsen syndrome who was born with congenital tetraplagia. Note the maldevelopment of the anterior ring of the atlas C1, which has been displaced along the superior surface of the clivus. Also, the odontoid process is hypoplastic and dislocated and displaced between the defectively developed anterior rings (arrow head). Fusion of the fragmented anterior and posterior rings of C1 and fusion of these fragments causing effectively the development of a Y-shaped deformity (a). Axial 3D-reformatted CT scan showing congenital maldevelopment of the anterior arch of the atlas and fusion of the remnants of the anterior ring with the lateral mass of C1 (forming a Y-shaped bone deformity) (arrow head). The posterior ring of C1 is hypoplastic resembling a Jefferson fracture (arrow head) (b).
3.3. Acute-Angle Cervico-Thoracic Kyphosis in a Child with Larsen Syndrome
Acute-angle kyphosis (sharp angulation) presenting at birth or later on is almost always due to a congenital vertebral malformation. In this child, the deformity is purely kyphotic. Conservative treatment alone is of limited value in the management of congenital kyphosis, though some restrictions have to be considered to perform surgical interventions, especially when there is cardiopulmonary dysfunction, associated kidney anomalies, and neurological pathologies such as an Arnold–Chiari lesion, filum terminale syndrome, or diastematomyelia.
A sagittal cervico-thoracic MRI of a 2-year-old boy with Larsen syndrome showed cervico-thoracic kyphosis (Cobb’s angle of 90°) (Figure 5a). A sagittal cervico-thoracic 3D-reformatted CT scan of a 7-year-old child with Larsen syndrome showed hypoplastic anterior and posterior arches of the atlas fusion of C2-3 and hypoplasia and fragmentation of the seventh cervical spine (arrow) (Figure 5b). A 3D reconstruction CT scan of the same child showed fusion of C2-3 associated with hypoplastic vertebral bodies causing the development of acute cervico-thoracic kyphosis (Figure 5c).
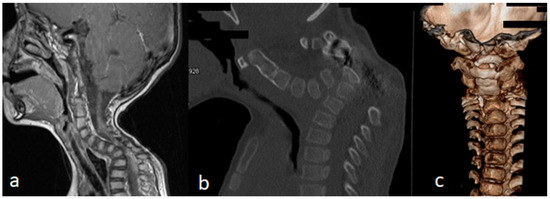
Figure 5.
(a–c): A sagittal cervico-thoracic MRI of a 2-year-old boy with Larsen syndrome showed cervico-thoracic kyphosis (Cobb’s angle of 90°) (a). Sagittal cervico thoracic 3D-reformatted CT scan of a 7-year-old child with Larsen syndrome showed hypoplastic anterior and posterior arch of the atlas associated with fusion of C2-3, hypoplasia and fragmentation of the 7th cervical spine (arrow) (b). A 3D reconstruction CT scan of the same child showed fusion of C2-3 associated with hypoplastic vertebral bodies causing the development of acute cervico-thoracic kyphosis (c).
3.4. Surgical Interventions to Correct Hip/Knee Dislocations and Talipes Equinovarus
Congenital multiple dislocations often prove a difficult task for pediatric orthopedic surgeons. Skeletal deformities in Larsen syndrome can recur. The dislocated hip joints must be treated as early as possible. Since at the same time, there is often hyperlaxity of the knee joints with anterior dislocation of the tibia, conservative treatment with physiotherapy and a Pavlik harness must primarily be carried out. While it is usually possible to reduce the knee joints through slow repression, the hip joints have to be openly reduced, which is technically difficult because they are due to the Larsen syndrome’s extremely unstable joints. In order to achieve sufficient joint stability, the open reduction must be combined with a bony procedure in which the dysplastic acetabulum is corrected. The surgical method according to Pemberton/Dega has proven successful in our hands, in which a slightly curved chisel is inserted in the cranial area to the edge of the acetabulum, the ileum is severed to just above the Y joint, and a triangular bone graft inserted into the osteotomy gap is fixed with a K wire. Depending on the existing anatomical conditions, an intertrochanteric osteotomy may also be indicated—for example, in the case of increased ante torsion of the femoral neck—in order to achieve optimal centering and stability of the femoral head in the joint socket. Because of the bony procedures, the surgery is not indicated before the age of 12 months. We performed it simultaneously combined proximal femoral varus osteotomy, and shelf acetabuloplasty has been performed in a 14-month-old girl with Larsen syndrome. The aim of these surgical procedures is to assure good containment of the bilateral hip dislocation. A double incision was used for this type of surgery (Figure 6a). Proximal femoral osteotomy for varization and de-rotation was performed at the intertrochanteric level (Figure 6b). In the postoperative period, neck-shaft angles were never reduced to less than 110°, and the de-rotation angle was less than 20° (Figure 6c).
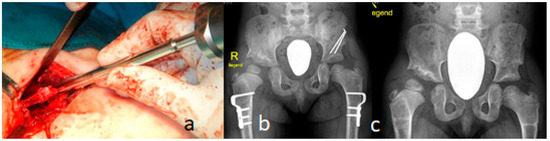
Figure 6.
(a–c): A double incision was used for this type of surgery in a 14-month-old girl with Larsen syndrome (a). Proximal femoral osteotomy for varization osteotomy and de-rotation was performed at the intertrochanteric level (b). In the postoperative period, neck-shaft angles were never reduced to less than 110°, and the de-rotation angle was less than 20° (c).
Regarding knee dislocations, we primarily started gentle manipulation soon after birth with traction and flexion of the knees. A long leg cast fixation was applied to restore knee flexion at 90° concomitantly with application of a Pavlik harness. The severe shortening of the quadriceps warranted operative corrections. The incision was made extending from the lateral parapatellar proximal to the crossing of the midline distally to the patella ending at the medial tibial tuberosity. Arthrotomy through mobilization of the quadriceps and hamstrings was applied. VY plasty and shortening osteotomy of the femur with plate fixation (preservation of extensor mechanism) was applied by a reverse McIntosh soft tissue plasty for joint stabilization associated with posterior capsulorrhaphy and cruciate plasty (the aim was shortening of the elongated anterior cruciate ligament). Postoperatively, we applied a plaster cast in 30–45° flexion. The first change of the plaster was on the second day after surgery; this was followed by plaster fixation for 4–6 weeks, and finally, with splints and physiotherapy, and orthotic management was achieved successfully.
Talipes equinovarus of the foot was corrected via soft tissue release (when the child was older than 1 year of age). The deformity in some children was very resistant, even to aggressive release. Postoperative bracing with ankle-foot orthoses was applied in an attempt to delay recurrence, though a recurrent deformity required repeated surgeries. In some children, we were able to achieve and maintain a plantigrade foot. Talectomy and talar de-cancellation were attempted in some children. V-Y quadriceps plasty with a shortening osteotomy of the femur with plate fixation (Figure 7a) was also attempted. The periodical clinical examinations and the follow ups showed dramatic improvement in his locomotor system (Figure 7b).
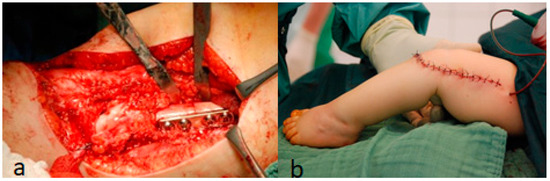
Figure 7.
(a,b): V-Y quadriceps plasty with shortening osteotomy of the femur with plate fixation (a) The periodical clinical examinations and the follow ups showed dramatic improvement in his locomotor system.
3.5. Surgical Intervention to Correct Traumatic Tertaplagia
A 2-year-old boy with Larsen syndrome became tetraplegic after minor trauma (jumping down from the sofa). Halo traction with 1 kg was used in the local emergency trauma center, and then after 1 week he was transferred to Ilizarov Center with minor neurological improvement. The lateral skull and spine radiograph showed hypoplastic and maldevelopment of the cervical spine associated with C1-2 instability and apparent kyphotic deformity with C4 body hypoplasia. The size of the cervical spinal canal was normal. So SCIWORA (spinal cord injury without radiographic-like) was a bit confusing due to laxity. But nevertheless, the kyphotic deformity was highly evident, and therefore the mechanism of cord trauma was expected (Figure 8a). An axial reformatted CT scan confirmed the hypoplasia of the vertebral body of C4 (Figure 8b).
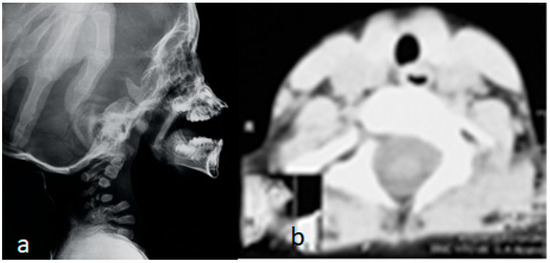
Figure 8.
(a,b): Lateral skull and spine radiograph showed hypoplastic and maldevelopment of the cervical spine associated with C1–2 instability and apparent kephotic deformity with C4 body hypoplasia. The size of the cervical spinal canal is normal. So SCIWORA (spinal cord injury without radiographic-like) was a bit confusing due to laxity. But nevertheless, the kyphotic deformity was so evident. and therefore, the mechanism of cord trauma was expected (Figure 6a). Axial reformatted CT scan confirmed the hypoplasia of the vertebral body of C4 (b).
According to the photo (intraoperative), at the end of the surgery 10, 3, and 5 mm screws were inserted in the lateral masses of C3-6 and intralaminar in C7 as well as two standard screws were applied to the occipital plate (Figure 9a). The surgery was followed by breath problems due to chest softness. Therefore, we were obliged to stop the operation every 30 min in order to give the child better oxygenation through lifting the child in our hands. Good neurological recovery was noticeable 2 weeks after surgery. A lateral cervical spine radiograph, ten years after surgery, showed good bone fusion, and the hardware is still stable (Figure 9b). He manifested remarkable improvement.
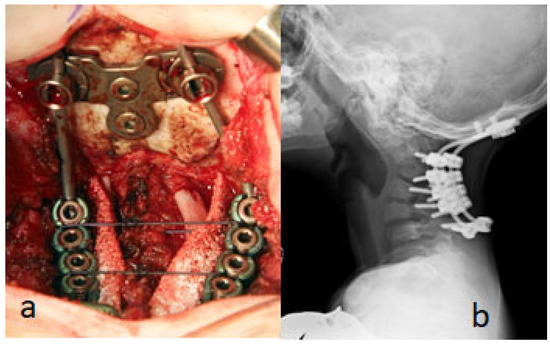
Figure 9.
(a,b). As shown in the photo (intraoperative), at the end of the surgery 10, 3, and 5 mm screws were inserted in the lateral masses of C3-6 and intralaminar in C7 as well as two standard screws that were applied to the occipital plate (Figure 7a). A lateral cervical spine radiograph, ten years after surgery, showed good bone fusion, and the hardware is still stable (b). Follow up after10 years (2014–2024) showed no neurological deficits. The foot surgery (talipes equinovarus) was made in another hospital. The implants are stable and have good glance, so we decided not to do anterior decompression and fixation.
4. Discussion
Larsen syndrome is characterized by multiple joint dislocations. The most frequent association (45%) is with developmental dysplasia of the hips, which can be diagnosed clinically at birth. The ossification of the femoral head occurs earlier than normal [21].
Children with Larsen syndrome may require many operations to fulfill some sort of corrections. These corrections are needed to approach sufficient success to ameliorate the locomotor system. The knees are particularly difficult to stabilize, and, in spite of prolonged splint age, instability can occur. In some patients, bilateral knee disarticulation in some instances can be problematic [22]. The hips are usually irreducible except by operative release, but, if this is the only solution, it is better performed during the first years of life. The dislocated elbows cause effectively total disruption for both the radio-capitulars and humero-ulnar joints because of the dysplasia of the distal humerus and condylar underdevelopment [23]. Talipes equinovarus or equinovalgus, or hindfoot valgus with forefoot adduction, can occur. These deformities warrant surgical corrections. A constellation of foot deformities have been described such as adductus, valgus, cavus, and equinovarus [24,25]. Cervical spine deformities in Larsen syndrome have been described in the literature as being the most serious life-threatening manifestation. A combination of cervical spine defects can cause morbid impingement on the spinal cord, which can include vertebral body hypoplasia, posterior element dysraphism, and craniocervical/cervical spine dys-segmentations [26]. All the aforementioned vertebral anomalies can result in C1-2 instability and/or leads to the development of acute-angle cervical kyphosis.
Acute-angle cervical spine kyphosis (spine malformation resulting in sharp angulation) has been diagnosed in three children; the first developed sudden insult to the spinal cord, which exposed the spinal cord to suffer severe damage, especially when progressive traumatic injury at the apex of the acute kyphosis occurred. The second was successfully operated. The third manifested a craniocervical malformation complex in congenital quadriplegia (tetraplegia). He manifested more severe skeletal and extraskeletal manifestations than the classical type of Larsen [27,28]. The dys-segmentation of the atlanto–axial spine can be considered as a novel finding consistent with the diagnosis of the lethal type of Larsen syndrome. On the one hand, a 3D-reformatted CT scan showed maldevelopment of the anterior ring of the atlas C1, which has been displaced along the superior surface of the clivus. On the other hand, the odontoid process was hypoplastic and dislocated and was displaced and impacted between the defectively developed anterior rings. In our patient, neither brain dysplasia nor pulmonary pathologies were encountered, and death occurred in his first year of life. The family history in this tetraplegic infant showed first-cousin marriage, compatible with an autosomal recessive pattern of inheritance. A lethal variant of Larsen syndrome is described in the literature. Apart from neonatal death due to pulmonary hypoplasia and laryngotracheomalacia, the main distinguishing feature appears to be serious congenital respiratory pathology [29,30,31,32,33]. Larsen syndrome in its classical presentation and/or in the lethal form have been a core of extensively studied disorders as a constellation of malformation complexes [34,35,36,37]. None of these studies compared the classical type and/or the lethal type of Larsen syndrome craniocervical malformations.
The differential diagnosis of Larsen syndrome is mandatory, and other disorders with multiple dislocations have to be considered. Hall et al. described three unrelated patients with an unusual form of spondyloepimetaphyseal dysplasia with multiple joint dislocations. Skeletal surveys revealed small flattened and irregular and fragmented epiphyses with wide and irregular metaphyses. There was also streaky sclerosis of the metaphyses [38]. Idaho syndrome is another disorder characterized by multiple joint dislocations and craniosynostosis. The limb abnormalities are diagnostically important, in that there is a complete anterior dislocation of the tibia and fibula, and the patellae are absent. The thumbs are proximally implanted, and there is camptodactyly at the interphalangeal joints [39].
5. Conclusions
The orthopedic strategy for patients with Larsen syndrome should be based upon early and precise clinical diagnosis. Cervical spine deformities can be divided into two categories. Firstly, with the lethal atlanto–axial maldevelopment (dys-segmentation), this form can be considered the most serious deformity and, meanwhile, as a novel understanding in infants with the lethal type of Larsen syndrome. Secondly, the progressive impingement on the spinal cord at the apex of the acute-angle kyphosis is another type. The early recognition of the nature of deformities can facilitate the diagnostic process. The precise clinical assessment and analysis of these children can lead to much better management. We continue to express our clinical expertise as a multidisciplinary team with different orthopedic specialties toward the best possible outcome, which is almost always based on our clinical merit. Finally, we wish to stress that in our registry we have more than a dozen patients with Larsen syndrome. Unfortunately, five adult patients remain physically handicapped because of misdiagnosis by other medical practitioners. The aim of this paper is to sensitize pediatricians, orthopedic surgeons, radiologists, and geneticists to the fact that arthrogryposis multiplex is a symptom complex rather than a diagnostic clinical entity and to differentiate between generalized ligamentous hyperlaxity as a component of a countless number of heritable bone disorders, and the floppy infant syndrome is mandatory.
Author Contributions
A.A.K. conceptualization and methodology; validation, A.A.K., F.G., A.G. and V.D.; formal analysis, A.A.K., A.G., S.R., H.A.K. and S.G.K.; investigation, S.G.K.; data curation, H.A.K., S.R. and F.G.; writing—original draft preparation, A.A.K.; writing—review and editing, F.G.; visualization, A.A.K.; supervision, F.G. and A.A.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study protocol was approved by Ethics Committee of the (Ilizarov Scientific Research Institute, No. 4(50)/13.12.2016, Kurgan, Russia). Informed consents were obtained from the patients’ guardians. Informed Consent Statement: A signed consent form was obtained from the patients’ guardians.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data is contained within the article.
Acknowledgments
We wish to thank and acknowledge the collaboration of the families and the guardians of the patients.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Larsen, L.J.; Schottstaedt, E.R.; Bost, F.C. Multiple congenital dislocations associated with characteristic facial abnormality. J. Pediatr. 1950, 37, 574–581. [Google Scholar] [PubMed]
- Klenn, P.J.; Iozzo, R.V. Larsen’s syndrome with novel congenital anomalies. Hum. Pathol. 1991, 22, 1055–1057. [Google Scholar] [PubMed]
- Latta, R.J.; Graham, C.B.; Aase, J.; Scham, S.M.; Smith, D.W. Larsen’s syndrome: A skeletal dysplasia with multiple joint dislocations and unusual facies. J. Pediatr. 1971, 78, 291–298. [Google Scholar] [PubMed]
- Kozlowski, K.; Robertson, F.; Middleton, R. Radiographic findings in Larsen’s syndrome. Australas. Radiol. 1974, 18, 336–344. [Google Scholar]
- De Smet, L.; Legius, E.; Fabry, G.; Fryns, J.P. The Larsen syndrome. The diagnostic contribution of the analysis of the metacarpophalangeal pattern profile. Genet. Couns. 1993, 4, 157–164. [Google Scholar]
- Maack, R.W.; Muntz, H.R. Ossicular abnormality in Larsen’s syndrome: A case report. Am. J. Otolaryngol. 1991, 12, 51–53. [Google Scholar]
- Kaga, K.; Suzuki, J.I.; Kimizuka, M. Temporal bone pathology of two infants with Larsen’s syndrome. Int. J. Pediatr. Otorhinolaryngol. 1991, 22, 257. [Google Scholar]
- Henriksson, P.; Ivarsson, S.; Theander, G. Larsen syndrome and glial profileration in the brain. Acta Paediatr. Scand. 1977, 66, 653. [Google Scholar]
- Goldberg, M.J. The Dysmorphic Child: An Orthopedic Perspective; Raven Press: New York, NY, USA, 1986. [Google Scholar]
- Steel, H.H.; Kohl, E.J. Multiple congenital dislocations associated with other skeletal anomalies (Larsen syndrome) in three siblings. J. Bone Jt. Surg. 1972, 54A, 75–82. [Google Scholar]
- Silverman, F.N. Larsen’s syndrome: Congenital dislocation of the knees and other joints, distinctive facies, and frequently, cleft palate. Ann. Radiol. 1972, 15, 297–328. [Google Scholar]
- Strisciuglio, P.; Sebastio, G.; Andria, G. Severe cardiac anomalies in sibs with Larsen syndrome. J. Med. Genet. 1983, 20, 422–424. [Google Scholar] [PubMed]
- Eletta, R.; Pandey, A.; Dharmasaputra, T.; Moreno, M.; Oparaugo, Y.; Kumar, T.S.; Beker, S. Severe Aortic Root Dilatation in a Patient With Larsen Syndrome. World J. Pediatr. Congenit. Heart Surg. 2023, 14, 532–535. [Google Scholar] [PubMed]
- Micheli, L.J.; Hall, J.E.; Watts, H.G. Spinal instability in Larsen’s syndrome: Report of three cases. J. Bone Jt. Surg. 1976, 58, 562–565. [Google Scholar]
- Weisenbach, J.; Melegh, B. Vertebral anomalies in Larsen‘s syndrome. Pediatr. Radiol. 1996, 26, 682–683. [Google Scholar] [PubMed]
- Lutter, L.D. Larsen syndrome: Clinical features and treatment—A report of two cases. J. Pediatr. Orthop. 1990, 10, 270–274. [Google Scholar]
- Johnston, C.E.; Birch, J.G.; Daniels, J.L. Cervical kyphosis in patients who have Larsen syndrome. J. Bone Jt. Surg. 1996, 78, 538–545. [Google Scholar]
- Zhang, D.; Herring, J.A.; Swaney, S.S.; McClendon, T.B.; Gao, X.; Browne, R.H.; Rathjen, K.E.; Johnston, C.E.; Harris, S.; Cain, N.M.; et al. Mutations responsible for Larsen syndrome cluster in the FLNB protein. J. Med. Genet. 2006, 43, e24. [Google Scholar]
- Hermanns, P.; Unger, S.; Rossi, A.; Perez-Aytes, A.; Cortina, H.; Bonafé, L.; Boccone, L.; Setzu, V.; Dutoit, M.; Sangiorgi, L.; et al. Congenital joint dislocations caused by carbohydrate sulfotransferase 3 deficiency in recessive Larsen syndrome and humero-spinal dysostosis. Am. J. Hum. Genet. 2008, 82, 1368–1374. [Google Scholar]
- Krakow, D.; Robertson, S.P.; King, L.M.; Morgan, T.; Sebald, E.T.; Bertolotto, C.; Wachsmann-Hogiu, S.; Acuna, D.; Shapiro, S.S.; Takafuta, T.; et al. Mutations in the gene encoding filamin B disrupt vertebral segmentation, joint formation and skeletogenesis. Nat. Genet. 2004, 36, 405–410. [Google Scholar]
- De La Rocha, A.; Birch, J.G.; Schiller, J.R. Precocious appearance of the capital femoral nucleus in Larsen Syndrome. J. Bone Jt. Surg. 2012, 94, pe55. [Google Scholar]
- Curtis, B.H.; Fisher, R.L. Congenital hyperextension with anterior subluxation of the knee. Surgical treatment and long-term observations. J. Bone Jt. Surg. 1969, 51, 255–1969. [Google Scholar] [PubMed]
- Rodríguez, A.; Asenjo, B.; Dominguez, R.; Lemaire, R. Larsen syndrome: Multicenter study of 12 new cases. Diagnosis, planning and results of treatment. Acta Orthop. Belg. 1994, 60, 259–273. [Google Scholar] [PubMed]
- Morcuende, J.A.; Dolan, L.A.; Dietz, F.R.; Ponseti, I.V. Radical reduction in the rate of extensive corrective surgery for clubfoot using the Ponseti method. Pediatrics 2004, 113, 376–380. [Google Scholar] [PubMed]
- Gerlach, D.J.; Gurnett, C.A.; Limpaphayom, N.; Alaee, F.; Zhang, Z.; Porter, K.; Kirchhofer, M.; Smyth, M.D.; Dobbs, M.B. Early results of the Ponseti method for the treatment of clubfoot associated with myelomeningocele. J. Bone Jt. Surg. 2009, 91, 1350–1359. [Google Scholar]
- Merrill, R.K.; Ishmael, T.G.; Samdani, A.F.; Hwang, S.W.; Pahys, J.M. Severe Cervical Kyphosis and Spondyloptosis with Myelopathy in Larsen Syndrome: A Report of 2 Cases. JBJS Case Connect. 2021, 11, e21. [Google Scholar]
- McKay, S.D.; Al-Omari, A.; Tomlinson, L.A.; Dormans, J.P. Review of cervical spine anomalies in genetic syndromes. Spine 2012, 37, E269–E277. [Google Scholar]
- Armouti, M.; Hirbawi, H.; Jadaan, M.; Hashem, H.; Muhsen, B.A. Surgical management of cervical kyphosis in larsen syndrome. Case report and review of literature. Ann. Med. Surg. 2022, 75, 103372. [Google Scholar]
- Unger, S.; Lausch, E.; Rossi, A.; Mégarbané, A.; Sillence, D.; Alcausin, M.; Aytes, A.; Mendoza-Londono, R.; Nampoothiri, S.; Afroze, B.; et al. Phenotypic features of carbohydrate sulfotransferase 3 (CHST3) deficiency in 24 patients: Congenital dislocations and vertebral changes as principal diagnostic features. Am. J. Med. Genet. A 2010, 152A, 2543–2549. [Google Scholar]
- Chen, H.; Chang, C.H.; Perrin, E.; Perrin, J.; Opitz, J.M. A lethal, Larsen-like multiple joint dislocation syndrome. Am. J. Med. Genet. 1982, 13, 149–161. [Google Scholar]
- Clayton-Smith, J.; Donnai, D. A further patient with the lethal type of Larsen syndrome. J. Med. Genet. 1988, 25, 499–500. [Google Scholar]
- Kulkarni, M.L.; Mohammed, Z.; Kulkarni, P.M. Larsen syndrome—Lethal variety. Indian J. Pediatr. 2005, 72, 1053–1054. [Google Scholar] [CrossRef] [PubMed]
- Caksen, H.; Kurtoglu, S. Larsen syndrome associated with severe congenital hydrocephalus. Genet. Couns. 2001, 12, 369–372. [Google Scholar] [PubMed]
- Siafaka, A.; Angelis, S.; Piagkou, M.; Apostolopoulos, A.; Troupis, T.; Filippou, D. Larsen Syndrome and Associated Spinal Deformities. Cureus 2023, 15, e41655. [Google Scholar] [CrossRef]
- Furuya, M.; Takeoka, Y.; Yurube, T.; Ito, M.; Suzuki, T.; Kakutani, K.; Uno, K. Two-Staged Surgery for Kyphoscoliosis in Larsen Syndrome with A 30-Year Follow-Up: A Case Report. Spine Surg. Relat. Res. 2023, 8, 338–341. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Sardhara, J.; Raiyani, V.; Saxena, D.; Kumar, A.; Bhaisora, K.S.; Das, K.K.; Mehrotra, A.; Srivastava, A.K.; Behari, S. Craniovertebral junction instability in Larsen syndrome: An institutional series and review of literature. J. Craniovertebr Junction Spine 2020, 11, 276–286. [Google Scholar]
- Deora, H.; Singh, S.; Sardhara, J.; Behari, S. A 360-Degree Surgical Approach for Correction of Cervical Kyphosis and Atlantoaxial Dislocation in the Case of Larsen Syndrome. J. Neurosci. Rural. Pract. 2020, 11, 196–201. [Google Scholar] [CrossRef]
- Hall, C.M.; Elcioglu, N.H.; MacDermot, K.D.; Offiah, A.C.; Winter, R.M. Spondyloepimetaphyseal dysplasia with multiple dislocations (Hall type): Three further cases and evidence of autosomal dominant inheritance. J. Med. Genet. 2002, 39, 666–670. [Google Scholar] [CrossRef][Green Version]
- Escobar, L.F.; Bixler, D.; Weaver, D.D.; Bull, M.J.; Bader, P. Larsen syndrome and craniosynostosis: Idaho syndrome? Dysmorph. Clin. Genet. 1989, 3, 24–27. [Google Scholar]









Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).