


Phase II Trial of Romidepsin as Consolidation Therapy after Gemcitabine, Dexamethasone, and Cisplatin in Elderly Transplant-Ineligible Patients with Relapsed/Refractory Peripheral T-Cell Lymphoma

 ,
,  , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Prospective and Retrospective Study Design
2.2. Treatment Protocol of the Prospective Study
2.3. Efficacy Evaluation
2.4. Efficacy Evaluation Following the Conclusion of Treatment
2.5. Statistical Analysis
3. Results
3.1. Patient and Clinical Characteristics
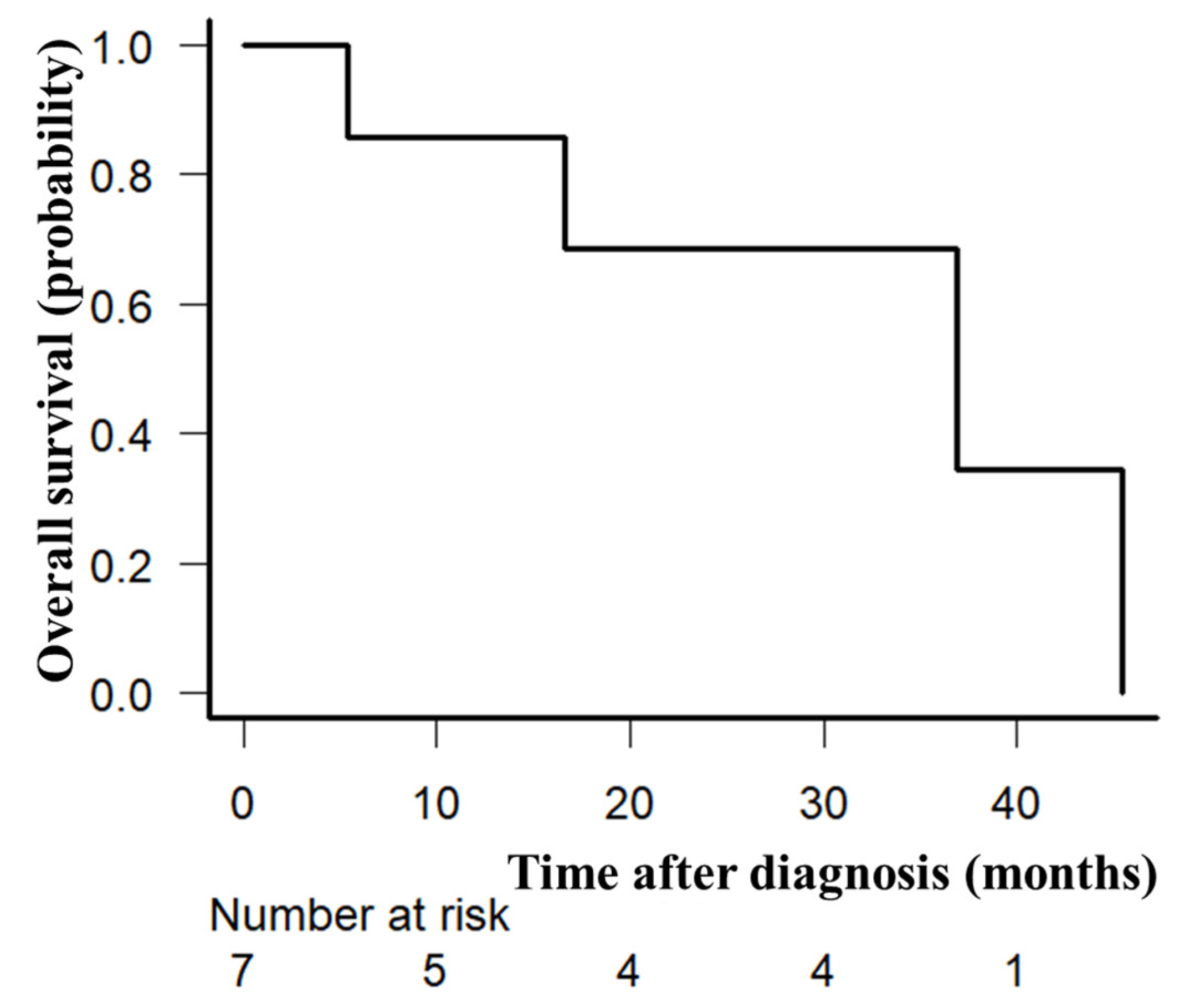
3.2. Treatment Outcomes
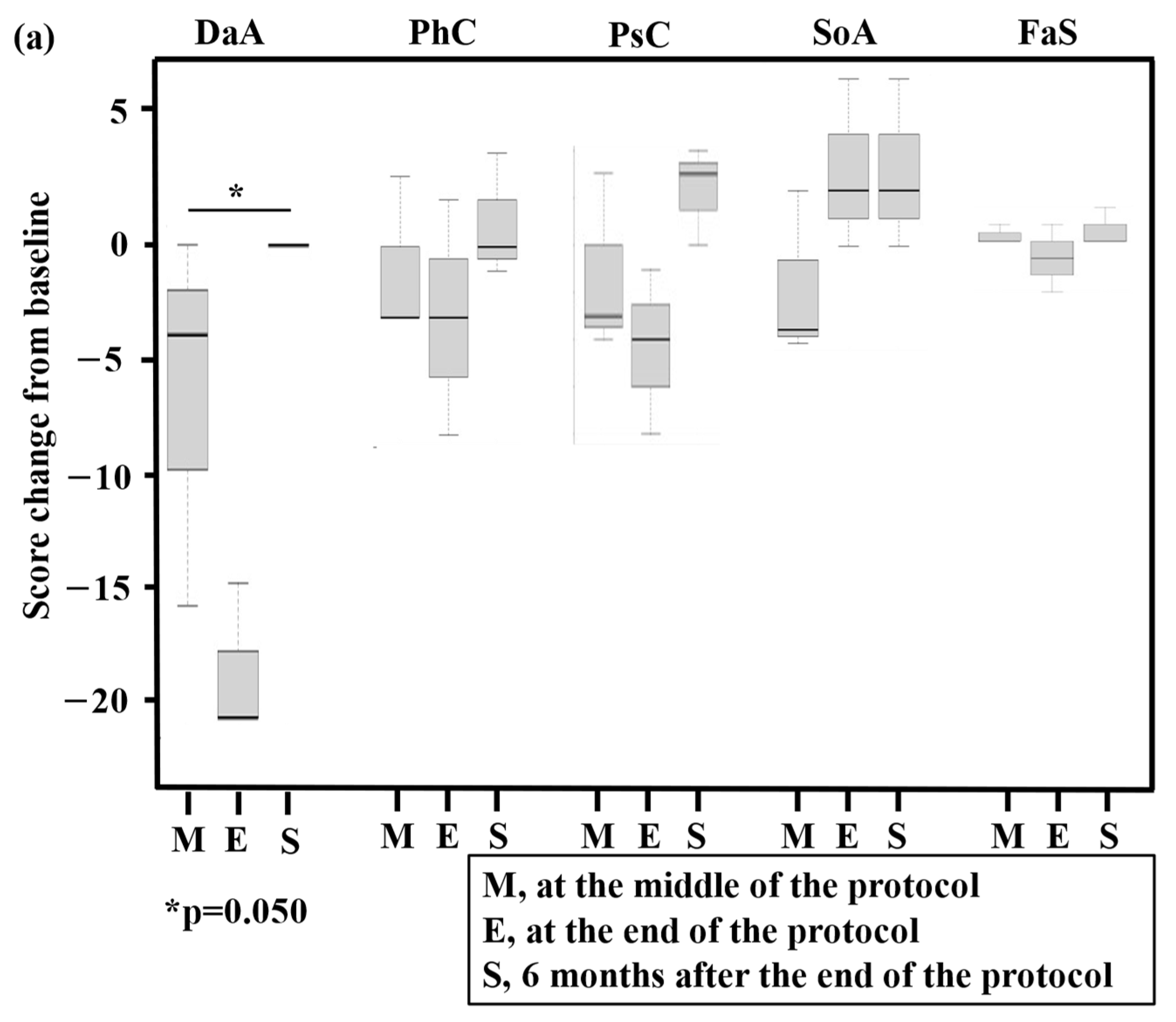
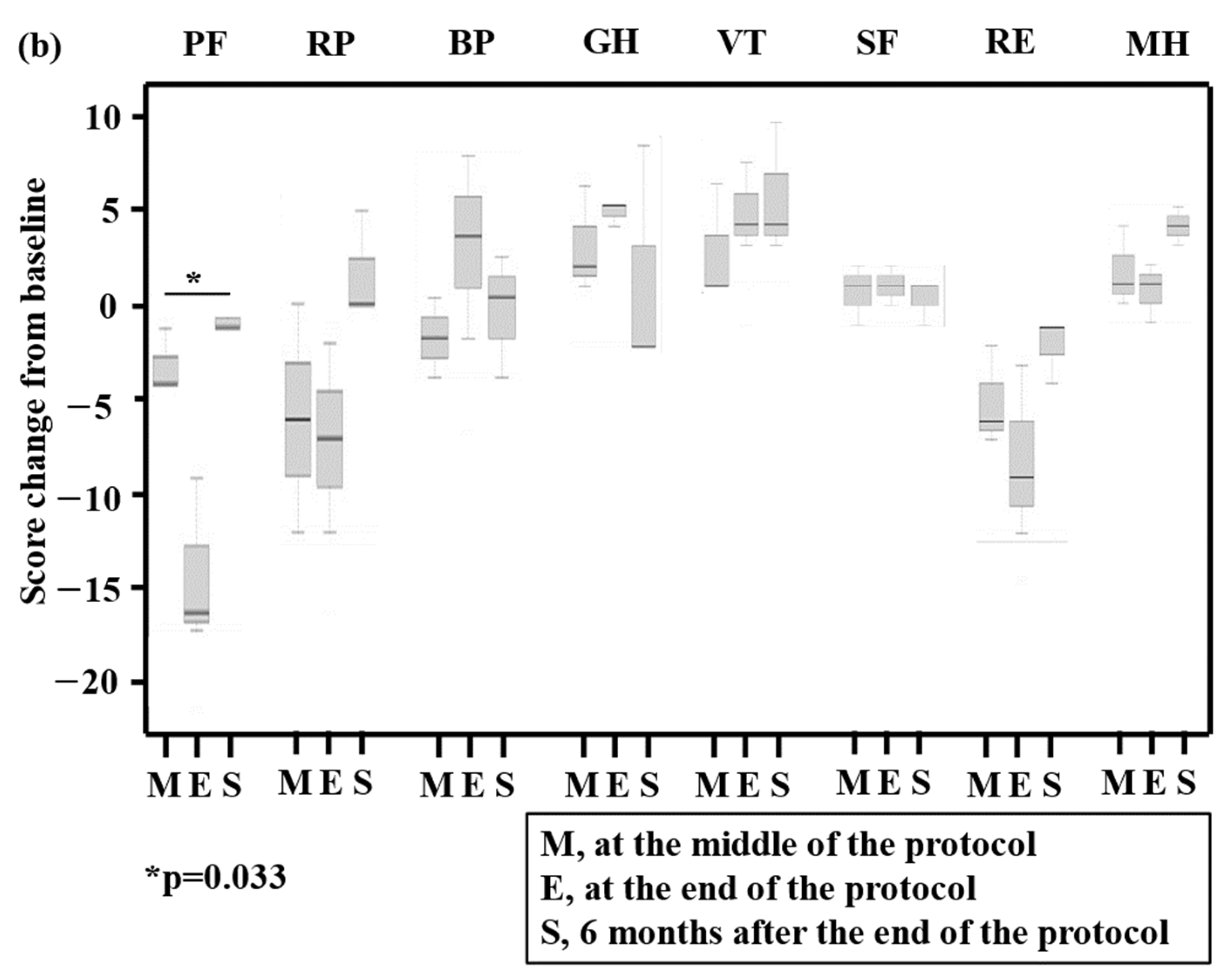
3.3. Toxicity Assessments, QOL, and Cost
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Swerdlow, S.H.; Campo, E.; Harris, N.L.; Jaffe, E.S.; Pileri, S.A.; Stein, H.; Thiele, J.; Vardiman, J.W. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues; IARC Press: Lyon, France, 2017. [Google Scholar]
- Horwitz, S.; O’Connor, O.A.; Pro, B.; Trümper, L.; Iyer, S.; Advani, R.; Bartlett, N.L.; Christensen, J.H.; Morschhauser, F.; Domingo-Domenech, E.; et al. The ECHELON-2 Trial: 5-year results of a randomized, phase III study of brentuximab vedotin with chemotherapy for CD30-positive peripheral T-cell lymphoma. Ann. Oncol. 2022, 33, 288–298. [Google Scholar] [CrossRef] [PubMed]
- Horwitz, S.; O’Connor, O.A.; Pro, B.; Illidge, T.; Fanale, M.; Advani, R.; Bartlett, N.L.; Christensen, J.H.; Morschhauser, F.; Domingo-Domenech, E.; et al. Brentuximab vedotin with chemotherapy for CD30-positive peripheral T-cell lymphoma (ECHELON-2): A global, double-blind, randomised, phase 3 trial. Lancet 2019, 393, 229–240. [Google Scholar] [CrossRef] [PubMed]
- Park, B.B.; Kim, W.S.; Suh, C.; Shin, D.Y.; Kim, J.A.; Kim, H.G.; Lee, W.S. Salvage chemotherapy of gemcitabine, dexamethasone, and cisplatin(GDP) for patients with relapsed o rrefractory peripheral T-Cell lymphomas:A consortium for improving survival of lymphoma(CISL) trial. Ann. Hematol. 2015, 94, 1845–1851. [Google Scholar] [CrossRef] [PubMed]
- Qi, F.; Dong, M.; He, X.; Li, Y.; Wang, W.; Liu, P.; Yang, J.; Gui, L.; Zhang, C.; Yang, S.; et al. Gemcitabine, dexamethasone, Andcisplatin (GDP) as salvage chemotherapy for patients with relapsed or refractory peripheral T cell lymphoma-Not otherwisespecified. Ann. Hematol. 2017, 96, 245–251. [Google Scholar] [CrossRef] [PubMed]
- Maruyama, D.; Tobinai, K.; Ogura, M.; Uchida, T.; Hatake, K.; Taniwaki, M.; Ando, K.; Tsukasaki, K.; Ishida, T.; Kobayashi, N.; et al. Romidepsin in Japanese patients with relapsed or refractory peripheral T-Cell lymphoma. A phase I/II and pharmacokinetics study. Int. J. Hematol. 2017, 106, 655–665. [Google Scholar] [CrossRef] [PubMed]
- Shustov, A.; Coiffier, B.; Horwitz, S.; Sokol, L.; Pro, B.; Wolfson, J.; Balser, B.; Eisch, R.; Popplewell, L.; Prince, H.M.; et al. Romidepsin is effective and well tolerated in older patients with peripheral T-cell lymphoma: Analysis of two phase II trials. Leuk. Lymphoma 2017, 58, 2335–2341. [Google Scholar] [CrossRef] [PubMed]
- Hosing, C.; McLaughlin, E.; Braunstein, Z.; Valdez, B.C.; Wei, L.; Popat, U.R.; Andersson, B.S.; Vasu, S.; Larkin, K.T.; Jaglowski, S.; et al. Post-Allograft Romidepsin Maintenance Mitigates Relapse Risk and Stimulates the Graft-Versus-Malignancy Effect through Enhanced NK-Cell Cytotoxicity in Patients with Aggressive T-Cell Malignancies in a Phase I/II Trial. Blood 2022, 140 (Suppl. 1), 1885–1886. [Google Scholar] [CrossRef]
- Stuver, R.; Moskowitz, A.J. Therapeutic Advances in Relapsed and Refractory Peripheral T-Cell Lymphoma. Cancers 2023, 15, 589. [Google Scholar] [CrossRef] [PubMed]
- Yamasaki, S.; Iida, H.; Yoshida, I.; Komeno, T.; Sawamura, M.; Matsumoto, M.; Sekiguchi, N.; Hishita, T.; Sunami, K.; Shimomura, T.; et al. Comparison of prognostic scores in transplant-ineligible patients with peripheral T-cell lymphoma not otherwise specified and angioimmunoblastic T-cell lymphoma: A retrospective study from the national hospital organization in Japan. Leuk. Lymphoma 2021, 62, 819–827. [Google Scholar] [CrossRef] [PubMed]
- Swerdlow, S.H.; Campo, E.; Pileri, S.A.; Harris, N.L.; Stein, H.; Siebert, R.; Advani, R.; Ghielmini, M.; Salles, G.A.; Zelenetz, A.D.; et al. The 2016 revision of the World Health Organization classification of lymphoid neoplasms. Blood 2016, 127, 2375–2390. [Google Scholar] [CrossRef] [PubMed]
- Cheson, B.D.; Pfistner, B.; Juweid, M.E.; Gascoyne, R.D.; Specht, L.; Horning, S.J.; Coiffier, B.; Fisher, R.I.; Hagenbeek, A.; Zucca, E.; et al. International Harmonization Project on Lymphoma Revised response criteria for malignant lymphoma. J. Clin. Oncol. 2007, 25, 579–586. [Google Scholar] [CrossRef] [PubMed]
- Yamasaki, S.; Kada, A.; Nagai, H.; Yoshida, I.; Choi, I.; Saito, A.M.; Iwasaki, H. Phase II Trial Using Romidepsin after Gemcitabine, Dexamethasone, and Cisplatin Therapy in Elderly Transplant-Ineligible Patients with Relapsed/Refractory Peripheral T-Cell Lymphoma: Study Protocol. Acta Med. Okayama 2019, 73, 469–474. [Google Scholar] [PubMed]
- Kurihara, M.; Shimizu, H.; Tsuboi, K.; Kobayashi, K.; Murakami, M.; Eguchi, K.; Shimozuma, K. Development of quality of life questionnaire in Japan: Quality of life assessment of cancer patients receiving chemotherapy. Psychooncology 1999, 8, 355–363. [Google Scholar] [CrossRef]
- Fukuhara, S.; Bito, S.; Green, J.; Hsiao, A.; Kurokawa, K. Translation, adaptation, and validation of the SF-36 Health Survey for use in Japan. J. Clin. Epidemiol. 1998, 51, 1037–1044. [Google Scholar] [CrossRef] [PubMed]
- Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant. 2013, 48, 452–458. [Google Scholar] [CrossRef]
- Coiffier, B.; Pro, B.; Prince, H.M.; Foss, F.; Sokol, L.; Greenwood, M.; Caballero, D.; Borchmann, P.; Morschhauser, F.; Wilhelm, M.; et al. Results from a pivotal, open-label, phase II study of romidepsin in relapsed or refractory peripheral T-cell lymphoma after prior systemic therapy. J. Clin. Oncol. 2012, 30, 631–636. [Google Scholar] [CrossRef] [PubMed]
- Pellegrini, C.; Dodero, A.; Chiappella, A.; Monaco, F.; Degl’Innocenti, D.; Salvi, F.; Vitolo, U.; Argnani, L.; Corradini, P.; Zinzani, P.L.; et al. A phase II study on the role of gemcitabine plus romidepsin (GEMRO regimen) in the treatment of relapsed/refractory peripheral T-cell lymphoma patients. J. Hematol. Oncol. 2016, 9, 38. [Google Scholar] [CrossRef] [PubMed]
- Cheung, L.C.; Cruickshank, M.N.; Hughes, A.M.; Singh, S.; Chua, G.A.; Ford, J.; Ferrari, E.; Oommen, J.; Malinge, S.; Lock, R.B.; et al. Romidepsin enhances the efficacy of cytarabine in vivo, Revealing histonedeacetylase inhibition as apromising therapeutic strategy for KMT2Ar earranged infant acute lymphoblastic leukemia. Haematologica 2019, 104, e300–e303. [Google Scholar] [CrossRef] [PubMed]
- Gisselbrecht, C.; Sibon, D. New perspectives in the therapeutic approach of peripheral T-cell lymphoma. Curr. Opin. Oncol. 2018, 30, 285–291. [Google Scholar] [CrossRef] [PubMed]
- Mead, M.; Cederleuf, H.; Björklund, M.; Wang, X.; Relander, T.; Jerkeman, M.; Gaut, D.; Larson, S.; Ellin, F. Impact of comorbidity in older patients with peripheral T-cell lymphoma: An international retrospective analysis of 891 patients. Blood Adv. 2022, 6, 2120–2128. [Google Scholar] [CrossRef] [PubMed]
- Bachy, E.; Camus, V.; Thieblemont, C.; Sibon, D.; Casasnovas, R.-O.; Ysebaert, L.; Damaj, G.; Guidez, S.; Pica, G.M.; Kim, W.S.; et al. Romidepsin Plus CHOP versus CHOP in Patients with Previously Untreated Peripheral T-Cell Lymphoma: Results of the Ro-CHOP Phase III Study (Conducted by LYSA). J. Clin. Oncol. 2022, 40, 242–251. [Google Scholar] [CrossRef] [PubMed]
- Kharfan-Dabaja, M.A.; Kumar, A.; Ayala, E.; Hamadani, M.; Reimer, P.; Gisselbrecht, C.; d’Amore, F.; Jantunen, E.; Ishida, T.; Bazarbachi, A.; et al. Clinical practice recommendations on indication and timing of hematopoietic cell transplantation in mature T cell and NK/T cell lymphomas: An international collaborative effort on behalf of the Guidelines Committee of the American Society for Blood and Marrow Transplantation. Biol. Blood Marrow Transplant. 2017, 23, 1826–1838. [Google Scholar] [PubMed]
- Yamasaki, S.; Yoshida, S.; Kato, K.; Choi, I.; Imamura, Y.; Kohno, K.; Henzan, H.; Tanimoto, K.; Ogawa, R.; Suehiro, Y.; et al. Effects of stem cell transplantation in patients with peripheral T-cell lymphoma not otherwise specified and angioimmunoblastic T-cell lymphoma. Int. J. Hematol. 2020, 112, 74–83. [Google Scholar] [CrossRef] [PubMed]
- Falchi, L.; Ma, H.; Klein, S.; Lue, J.K.; Montanari, F.; Marchi, E.; Deng, C.; Kim, H.A.; Rada, A.; Jacob, A.T.; et al. Combined oral 5-azacytidine and romidepsin are highly effective in patients with PTCL: A multicenter phase 2 study. Blood 2021, 137, 2161–2170. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | n = 7 | |
| Median age (range), years | 74 (72–82) | |
| ≥75 years of age, n (%) | 3 (43) | |
| Sex, n (%) | male | 7 (100) |
| female | 0 | |
| ECOG PS, n (%) | 0 | 2 (29) |
| 1 | 5 (71) | |
| 2 | 0 | |
| Ann Arbor stage, n (%) | I | 0 |
| II | 0 | |
| III | 4 (57) | |
| IV | 3 (43) | |
| BM involvement, n (%) | 2 (29) | |
| IPI, n (%) | low | 0 |
| low–intermediate | 1 (14) | |
| high–intermediate | 5 (71) | |
| high | 1 (14) | |
| Median No. (range) of cycles of initial CHOP | 6 (1–6) | |
| Radiotherapy after initial CHOP, n (%) | 0 | |
| Best response after initial CHOP, n (%) | CR | 5 (71) |
| PR | 1 (14) | |
| SD | 1 (14) | |
| PTCL-GDPR | |||||||||||
| GDP | Romidepsin | ||||||||||
| Toxicities/Cycles | 1 | 2 | 3 | 4 | 1 | 2 | 3 | 5 | 7 | 10 | 12 |
| n = 7 | n = 5 | n = 4 | n = 4 | n = 5 | n = 5 | n = 5 | n = 3 | n = 3 | n = 3 | n = 3 | |
| Hematological toxicities, n (%) | |||||||||||
| WBC decreased | 5 (71) | 3 (60) | 2 (50) | 2 (50) | 3 (60) | 2 (40) | 2 (40) | 1 (33) | 1 (33) | 0 | 0 |
| Neutrophil count decreased | 5 (71) | 3 (60) | 2 (50) | 2 (50) | 3 (60) | 2 (40) | 2 (40) | 1 (33) | 1 (33) | 0 | 0 |
| Anemia | 2 (29) | 2 (40) | 0 | 0 | 1 (20) | 0 | 1 (20) | 0 | 0 | 0 | 0 |
| Thrombocytopenia | 0 | 3 (60) | 1 (25) | 1 (25) | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| VZV infections, n (%) | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 (33) | 0 |
| Non-hematological toxicities, n (%) | |||||||||||
| Gastrointestinal | |||||||||||
| Anorexia | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 (33) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yamasaki, S.; Iida, H.; Saito, A.; Matsumoto, M.; Kuroda, Y.; Izumi, T.; Saito, A.M.; Miyoshi, H.; Ohshima, K.; Nagai, H.; et al. Phase II Trial of Romidepsin as Consolidation Therapy after Gemcitabine, Dexamethasone, and Cisplatin in Elderly Transplant-Ineligible Patients with Relapsed/Refractory Peripheral T-Cell Lymphoma. Hematol. Rep. 2024, 16, 336-346. https://doi.org/10.3390/hematolrep16020034
Yamasaki S, Iida H, Saito A, Matsumoto M, Kuroda Y, Izumi T, Saito AM, Miyoshi H, Ohshima K, Nagai H, et al. Phase II Trial of Romidepsin as Consolidation Therapy after Gemcitabine, Dexamethasone, and Cisplatin in Elderly Transplant-Ineligible Patients with Relapsed/Refractory Peripheral T-Cell Lymphoma. Hematology Reports. 2024; 16(2):336-346. https://doi.org/10.3390/hematolrep16020034
Chicago/Turabian StyleYamasaki, Satoshi, Hiroatsu Iida, Akio Saito, Morio Matsumoto, Yoshiaki Kuroda, Tohru Izumi, Akiko M. Saito, Hiroaki Miyoshi, Koichi Ohshima, Hirokazu Nagai, and et al. 2024. "Phase II Trial of Romidepsin as Consolidation Therapy after Gemcitabine, Dexamethasone, and Cisplatin in Elderly Transplant-Ineligible Patients with Relapsed/Refractory Peripheral T-Cell Lymphoma" Hematology Reports 16, no. 2: 336-346. https://doi.org/10.3390/hematolrep16020034
APA StyleYamasaki, S., Iida, H., Saito, A., Matsumoto, M., Kuroda, Y., Izumi, T., Saito, A. M., Miyoshi, H., Ohshima, K., Nagai, H., & Iwasaki, H. (2024). Phase II Trial of Romidepsin as Consolidation Therapy after Gemcitabine, Dexamethasone, and Cisplatin in Elderly Transplant-Ineligible Patients with Relapsed/Refractory Peripheral T-Cell Lymphoma. Hematology Reports, 16(2), 336-346. https://doi.org/10.3390/hematolrep16020034