
Impact of Skeletal Muscle Depletion on Patients with Myelodysplastic Syndrome Treated with Azacitidine

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
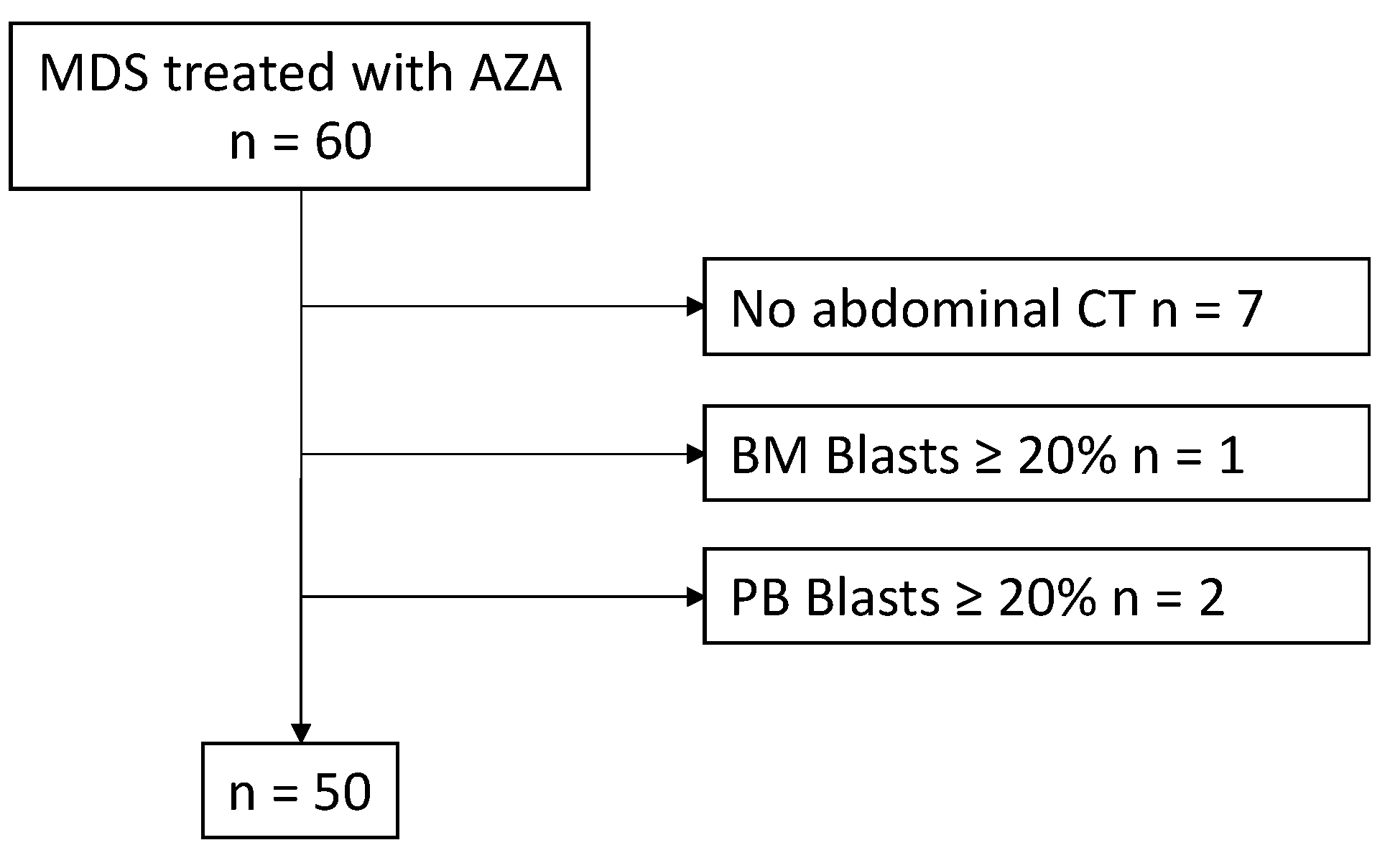
2.1. Patient Cohort and Treatment
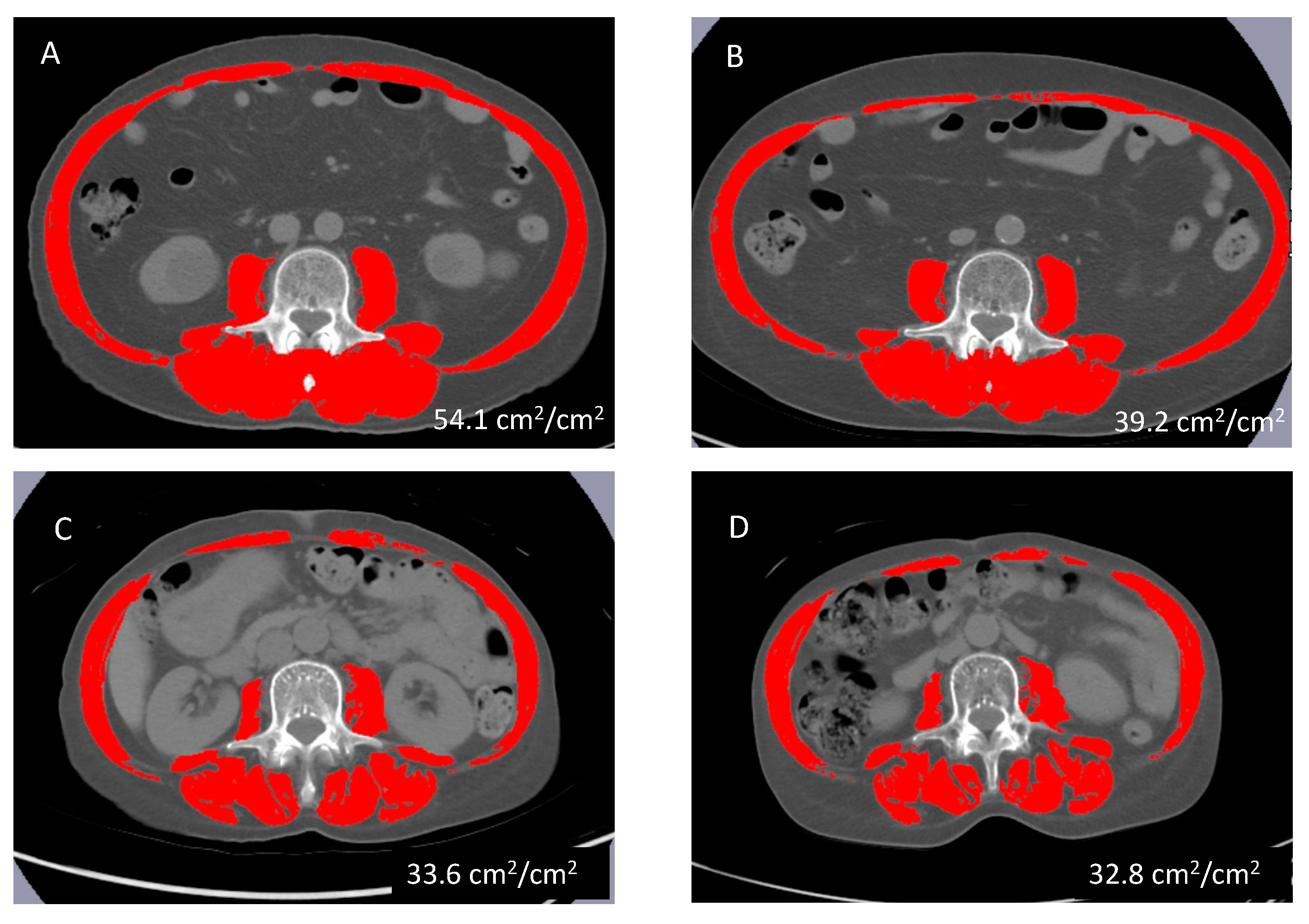
2.2. Definition of Skeletal Muscle Depletion
2.3. Statistical Analysis
3. Results
3.1. Patients’ Characteristics and Comparisons between SMD and Non-SMD Group Patients
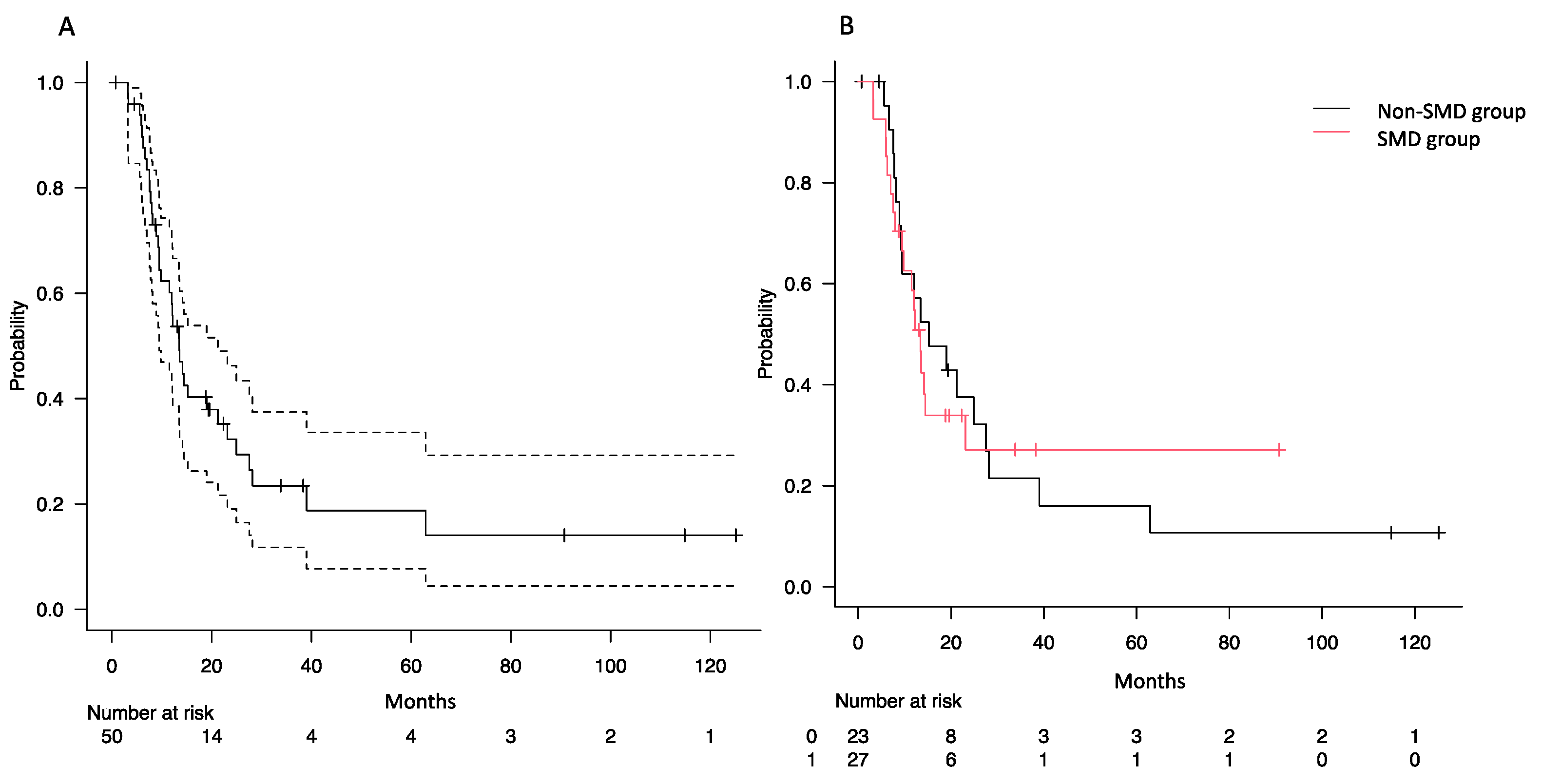
3.2. Impact of SMD on Overall Survival
3.3. Associations of SMD with Response Rates and Adverse Events
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Walter, M.J.; Shen, D.; Ding, L.; Shao, J.; Koboldt, D.C.; Chen, K.; Larson, D.E.; McLellan, M.D.; Dooling, D.; Abbott, R.; et al. Clonal Architecture of Secondary Acute Myeloid Leukemia. N. Engl. J. Med. 2012, 366, 1090–1098. [Google Scholar] [CrossRef] [PubMed]
- Kuendgen, A.; Strupp, C.; Aivado, M.; Hildebrandt, B.; Haas, R.; Gattermann, N.; Germing, U. Myelodysplastic Syndromes in Patients Younger than Age 50. J. Clin. Oncol. 2006, 24, 5358–5365. [Google Scholar] [CrossRef] [PubMed]
- Ma, X.; Does, M.; Raza, A.; Mayne, S.T. Myelodysplastic Syndromes: Incidence and Survival in the United States. Cancer 2007, 109, 1536–1542. [Google Scholar] [CrossRef]
- Keating, G.M. Azacitidine: A Review of Its Use in the Management of Myelodysplastic Syndromes/Acute Myeloid Leukaemia. Drugs 2012, 72, 1111–1136. [Google Scholar] [CrossRef]
- Zeidan, A.M.; Joshi, N.; Kale, H.; Wang, W.-J.; Corman, S.; Salimi, T.; Epstein, R.S. Impact of Hypomethylating Agent Use on Hospital and Emergency Room Visits, and Predictors of Early Discontinuation in Patients With Higher-Risk Myelodysplastic Syndromes. Clin. Lymphoma Myeloma Leuk. 2022, 22, 670–679. [Google Scholar] [CrossRef]
- Greenberg, P.; Cox, C.; LeBeau, M.M.; Fenaux, P.; Morel, P.; Sanz, G.; Sanz, M.; Vallespi, T.; Hamblin, T.; Oscier, D.; et al. International Scoring System for Evaluating Prognosis in Myelodysplastic Syndromes. Blood 1997, 89, 2079–2088. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, P.L.; Tuechler, H.; Schanz, J.; Sanz, G.; Garcia-Manero, G.; Solé, F.; Bennett, J.M.; Bowen, D.; Fenaux, P.; Dreyfus, F.; et al. Revised International Prognostic Scoring System for Myelodysplastic Syndromes. Blood 2012, 120, 2454–2465. [Google Scholar] [CrossRef]
- Sieber, C.C. Malnutrition and Sarcopenia. Aging Clin. Exp. Res. 2019, 31, 793–798. [Google Scholar] [CrossRef]
- Zhang, X.; Edwards, B.J. Malnutrition in Older Adults with Cancer. Curr. Oncol. Rep. 2019, 21, 80. [Google Scholar] [CrossRef]
- Surov, A.; Wienke, A. Sarcopenia Predicts Overall Survival in Patients with Malignant Hematological Diseases: A Meta-Analysis. Clin. Nutr. 2021, 40, 1155–1160. [Google Scholar] [CrossRef]
- Nakamura, N.; Hara, T.; Shibata, Y.; Matsumoto, T.; Nakamura, H.; Ninomiya, S.; Kito, Y.; Kitagawa, J.; Kanemura, N.; Goto, N.; et al. Sarcopenia Is an Independent Prognostic Factor in Male Patients with Diffuse Large B-Cell Lymphoma. Ann. Hematol. 2015, 94, 2043–2053. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, N.; Ninomiya, S.; Matsumoto, T.; Nakamura, H.; Kitagawa, J.; Shiraki, M.; Hara, T.; Shimizu, M.; Tsurumi, H. Prognostic Impact of Skeletal Muscle Assessed by Computed Tomography in Patients with Acute Myeloid Leukemia. Ann. Hematol. 2019, 98, 351–359. [Google Scholar] [CrossRef] [PubMed]
- Kanehira, D.; Koinuma, M.; Kato, T.; Abe, T.; Sagara, A.; Sato, F.; Yumoto, T. Relationship between Low Pretreatment Geriatric Nutritional Risk Index and Poor Tolerability of Azacitidine in Patients with Myelodysplastic Syndromes. Ann. Nutr. Metab. 2020, 76, 405–412. [Google Scholar] [CrossRef]
- Fenaux, P.; Mufti, G.J.; Hellstrom-Lindberg, E.; Santini, V.; Finelli, C.; Giagounidis, A.; Schoch, R.; Gattermann, N.; Sanz, G.; List, A.; et al. Efficacy of Azacitidine Compared with That of Conventional Care Regimens in the Treatment of Higher-Risk Myelodysplastic Syndromes: A Randomised, Open-Label, Phase III Study. Lancet Oncol. 2009, 10, 223–232. [Google Scholar] [CrossRef] [PubMed]
- Gao, C.; Wang, J.; Li, Y.; Zhao, H.; Li, R.; Hou, L.; Zhang, Y.; Tian, S.; Liang, H.; Wang, C.; et al. Incidence and Risk of Hematologic Toxicities with Hypomethylating Agents in the Treatment of Myelodysplastic Syndromes and Acute Myeloid Leukopenia: A Systematic Review and Meta-Analysis. Medicine 2018, 97, e11860. [Google Scholar] [CrossRef] [PubMed]
- Arber, D.A.; Orazi, A.; Hasserjian, R.; Thiele, J.; Borowitz, M.J.; Le Beau, M.M.; Bloomfield, C.D.; Cazzola, M.; Vardiman, J.W. The 2016 Revision to the World Health Organization Classification of Myeloid Neoplasms and Acute Leukemia. Blood 2016, 127, 2391–2405. [Google Scholar] [CrossRef] [PubMed]
- Bennett, J.M.; Catovsky, D.; Daniel, M.T.; Flandrin, G.; Galton, D.A.; Gralnick, H.R.; Sultan, C. Proposals for the Classification of the Myelodysplastic Syndromes. Br. J. Haematol. 1982, 51, 189–199. [Google Scholar] [CrossRef]
- Bouillanne, O.; Morineau, G.; Dupont, C.; Coulombel, I.; Vincent, J.-P.; Nicolis, I.; Benazeth, S.; Cynober, L.; Aussel, C. Geriatric Nutritional Risk Index: A New Index for Evaluating at-Risk Elderly Medical Patients. Am. J. Clin. Nutr. 2005, 82, 777–783. [Google Scholar] [CrossRef]
- Kenis, C.; Decoster, L.; Van Puyvelde, K.; De Grève, J.; Conings, G.; Milisen, K.; Flamaing, J.; Lobelle, J.-P.; Wildiers, H. Performance of Two Geriatric Screening Tools in Older Patients with Cancer. J. Clin. Oncol. 2014, 32, 19–26. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A New Method of Classifying Prognostic Comorbidity in Longitudinal Studies: Development and Validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Nishikawa, H.; Shiraki, M.; Hiramatsu, A.; Moriya, K.; Hino, K.; Nishiguchi, S. Japan Society of Hepatology Guidelines for Sarcopenia in Liver Disease (1st Edition): Recommendation from the Working Group for Creation of Sarcopenia Assessment Criteria. Hepatol. Res. 2016, 46, 951–963. [Google Scholar] [CrossRef]
- Cheson, B.D.; Greenberg, P.L.; Bennett, J.M.; Lowenberg, B.; Wijermans, P.W.; Nimer, S.D.; Pinto, A.; Beran, M.; de Witte, T.M.; Stone, R.M.; et al. Clinical Application and Proposal for Modification of the International Working Group (IWG) Response Criteria in Myelodysplasia. Blood 2006, 108, 419–425. [Google Scholar] [CrossRef]
- Kanda, Y. Investigation of the Freely Available Easy-to-Use Software “EZR” for Medical Statistics. Bone Marrow Transplant. 2013, 48, 452–458. [Google Scholar] [CrossRef]
- Oliva, E.N.; Schey, C.; Hutchings, A.S. A Review of Anemia as a Cardiovascular Risk Factor in Patients with Myelodysplastic Syndromes. Am. J. Blood Res. 2011, 1, 160–166. [Google Scholar]
- Basood, M.; Oster, H.S.; Mittelman, M. Thrombocytopenia in Patients with Myelodysplastic Syndromes: Still an Unsolved Problem. Mediterr. J. Hematol. Infect. Dis. 2018, 10, e2018046. [Google Scholar] [CrossRef]
- Cesari, M.; Penninx, B.W.J.H.; Lauretani, F.; Russo, C.R.; Carter, C.; Bandinelli, S.; Atkinson, H.; Onder, G.; Pahor, M.; Ferrucci, L. Hemoglobin Levels and Skeletal Muscle: Results from the InCHIANTI Study. J. Gerontol. A Biol. Sci. Med. Sci. 2004, 59, 249–254. [Google Scholar] [CrossRef]
- Takata, T.; Mae, Y.; Yamada, K.; Taniguchi, S.; Hamada, S.; Yamamoto, M.; Iyama, T.; Isomoto, H. Skeletal Muscle Mass Is Associated with Erythropoietin Response in Hemodialysis Patients. BMC Nephrol. 2021, 22, 134. [Google Scholar] [CrossRef]
- Lucijanic, M.; Galusic, D.; Soric, E.; Sedinic, M.; Cubela, M.; Huzjan Korunic, R.; Pejsa, V.; Kusec, R. Ruxolitinib Treatment Improves Muscle Mass in Patients with Myelofibrosis. Ann. Hematol. 2021, 100, 1105–1106. [Google Scholar] [CrossRef] [PubMed]
- Cho, K.-M.; Park, H.; Oh, D.-Y.; Kim, T.-Y.; Lee, K.H.; Han, S.-W.; Im, S.-A.; Kim, T.-Y.; Bang, Y.-J. Skeletal Muscle Depletion Predicts Survival of Patients with Advanced Biliary Tract Cancer Undergoing Palliative Chemotherapy. Oncotarget 2017, 8, 79441–79452. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Cho, Y.; Park, S.; Kim, J.W.; Lee, I.J. Skeletal Muscle Depletion Predicts the Prognosis of Patients With Hepatocellular Carcinoma Treated With Radiotherapy. Front. Oncol. 2019, 9, 1075. [Google Scholar] [CrossRef] [PubMed]
- Huh, J.; Park, B.; Lee, H.; An, Y.-S.; Jung, Y.; Kim, J.Y.; Kang, D.K.; Kim, K.W.; Kim, T.H. Prognostic Value of Skeletal Muscle Depletion Measured on Computed Tomography for Overall Survival in Patients with Non-Metastatic Breast Cancer. J. Breast Cancer 2020, 23, 80–92. [Google Scholar] [CrossRef]
- Armenian, S.H.; Xiao, M.; Berano Teh, J.; Lee, B.; Chang, H.A.; Mascarenhas, K.; Lee, S.; Iukuridze, A.; Xie, J.J.; Scott, J.M.; et al. Impact of Sarcopenia on Adverse Outcomes After Allogeneic Hematopoietic Cell Transplantation. J. Natl. Cancer Inst. 2019, 111, 837–844. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Tan, S.; Wu, G. Oral Nutritional Supplements, Physical Activity, and Sarcopenia in Cancer. Curr. Opin. Clin. Nutr. Metab. Care 2021, 24, 223–228. [Google Scholar] [CrossRef] [PubMed]
- Knips, L.; Bergenthal, N.; Streckmann, F.; Monsef, I.; Elter, T.; Skoetz, N. Aerobic Physical Exercise for Adult Patients with Haematological Malignancies. Cochrane Database Syst. Rev. 2019, 1, CD009075. [Google Scholar] [CrossRef]
- Yilmaz, M.; Atilla, F.D.; Sahin, F.; Saydam, G. The Effect of Malnutrition on Mortality in Hospitalized Patients with Hematologic Malignancy. Support. Care Cancer 2020, 28, 1441–1448. [Google Scholar] [CrossRef]
- Hall, C.C.; Skipworth, R.J.E.; Blackwood, H.; Brown, D.; Cook, J.; Diernberger, K.; Dixon, E.; Gibson, V.; Graham, C.; Hall, P.; et al. A Randomized, Feasibility Trial of an Exercise and Nutrition-Based Rehabilitation Programme (ENeRgy) in People with Cancer. J. Cachexia Sarcopenia Muscle 2021, 12, 2034–2044. [Google Scholar] [CrossRef]
- Ahmadi, B.M.; Noori, A.; Ashtiani, M.K.; Rajabi, S.; Talkhabi, M. 5-Azacytidine Incorporated Skeletal Muscle-Derived Hydrogel Promotes Rat Skeletal Muscle Regeneration. Cells Dev. 2023, 173, 203826. [Google Scholar] [CrossRef] [PubMed]
- Uchida, T.; Ogawa, Y.; Kobayashi, Y.; Ishikawa, T.; Ohashi, H.; Hata, T.; Usui, N.; Taniwaki, M.; Ohnishi, K.; Akiyama, H.; et al. Phase I and II Study of Azacitidine in Japanese Patients with Myelodysplastic Syndromes. Cancer Sci. 2011, 102, 1680–1686. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Factor | Group | Overall | SMD | Non-SMD | p-Value |
|---|---|---|---|---|---|
| (n = 50) | (n = 27) | (n = 23) | |||
| Female, n (%) | 11 (22.0) | 7 (25.9) | 4 (17.4) | 0.515 | |
| Age at AZA start, y, median (range) | 69.5 (17–82) | 71.0 (28.0–82.0) | 67.00 (17.0–79.0) | 0.067 | |
| Duration between diagnosis to AZA start, days, median (range) | 32.5 (0-1405) | 31 (0–781) | 36 (4–1405) | 0.495 | |
| BMI, kg/m2, median (range) | 22.65 (16.0–28.9) | 21.0 (16.0–27.1) | 24.4 (19.3–28.9) | <0.001 | |
| SMI, cm2/m2, median (range) | 40.0 (27.0–59.7) | 37.38 (27.0–41.9) | 46.8 (38.2–59.7) | <0.001 | |
| GNRI, median (range) | 102.2 (67.0–123.8) | 99.5 (67.0–123.8) | 106.1 (83.5–120.5) | 0.029 | |
| CCI, n (%) | 0–1 | 30 (60.0) | 15 (55.6) | 15 (65.2) | 0.569 |
| ≥2 | 20 (40.0) | 12 (44.4) | 8 (34.8) | ||
| fTRST, n (%) | 0 | 22 (44.0) | 10 (37.0) | 12 (52.2) | 0.199 |
| 1 | 22 (44.0) | 15 (55.6) | 7 (30.4) | ||
| 2 | 6 (12.0) | 2 (7.4) | 4 (17.4) | ||
| ECOG PS, n (%) | 0–1 | 45 (90.0) | 22 (81.5) | 23 (100.0) | 0.054 |
| ≥2 | 5 (10.0) | 5 (18.5) | 0 (0.0) | ||
| Neutrophil count, ×103/μL, median (range) | 1.1 (0.89–388.64) | 1.58 (0.52–388.64) | 0.92 (0.89–19.58) | 0.018 | |
| Hemoglobin, g/dL, median (range) | 8.2 (4.7–12.40) | 8.1 (4.7–12.1) | 8.3 (5.0–12.4) | 0.884 | |
| Platelet count, ×103/μL, median (range) | 66.5 (7.0–579.0) | 54.0 (7.0–280.0) | 101.0 (17.0–579.0) | 0.090 | |
| BM percentage blasts, median (range) | 9.45 (1.7–18.3) | 9.4 (1.9–18.3) | 9.5(1.7–17.9) | 0.846 | |
| Red cell transfusion dependence, n (%) | 11 (22.0) | 5 (18.5) | 6 (26.1) | 0.733 | |
| FAB classification, n (%) | RA | 5 (10.0) | 3 (11.1) | 2 (8.7) | 1.000 |
| RAEB | 45 (90.0) | 24 (88.9) | 21 (91.3) | ||
| WHO classification, n (%) | SLD | 2 (4.0) | 0 (0.0) | 2 (8.7) | 0.402 |
| MLD | 1 (2.0) | 1 (3.7) | 0 (0.0) | ||
| RS-MLD | 1 (2.0) | 1 (3.7) | 0 (0.0) | ||
| MDS-U | 1 (2.0) | 1 (3.7) | 0 (0.0) | ||
| EB-1 | 19 (38.0) | 9 (33.3) | 10 (43.5) | ||
| EB-2 | 26 (52.0) | 15 (55.6) | 11 (47.8) | ||
| IPSS-R, n (%) | Low | 1 (2.0) | 0 (0.0) | 1 (4.3) | 0.518 |
| Intermediate | 5 (10.0) | 4 (14.8) | 1 (4.3) | ||
| High | 17 (34.0) | 9 (33.3) | 8 (34.8) | ||
| Very high | 27 (54.0) | 14 (51.9) | 13 (56.5) | ||
| AZA ≥ 4 cycles, n (%) | 29 (58.0) | 18 (66.7) | 11 (47.8) | 0.252 | |
| Dose of AZA, n (%) | 75 mg/m2 | 25 (50.0) | 10 (37.0) | 15 (65.2) | 0.167 |
| 100 mg/body | 16 (32.0) | 11 (40.7) | 5 (21.7) | ||
| other | 9 (18.0) | 6 (22.2) | 3 (13.0) | ||
| Days of AZA treatment, n (%) | 7 days | 15 (30.0) | 7 (25.9) | 8 (34.8) | |
| 5–7 days | 35 (70.0) | 20 (74.1) | 15 (65.2) | ||
| Allo-HSCT, n (%) | 17 (34.0) | 5 (18.5) | 12 (52.1) | 0.012 |
| Univariate Analysis | Multivariable Analysis | |||
|---|---|---|---|---|
| Factor | HR (95% CI) | p-Value | HR (95% CI) | p-Value |
| ECOG PS ≥ 2 | 2.73 (0.91–8.16) | 0.073 | 3.15 (0.98–10.17) | 0.055 |
| SMD | 1.05 (0.54–2.03) | 0.897 | 0.75 (0.36–1.56) | 0.456 |
| IPSS-R score | 1.19 (0.96–1.48) | 0.116 | 1.21 (0.96–1.53) | 0.098 |
| Allo-HSCT | 0.59 (0.28–1.25) | 0.167 | 0.56 (0.26–1.26) | 0.162 |
| Factor | Group | All Patients | SMD | Non SMD | p-Value |
|---|---|---|---|---|---|
| (n = 50) | (n = 27) | (n = 23) | |||
| Response, n (%) | CR | 6 (14.6) | 4 (19.0) | 2 (10.0) | 0.714 |
| PR | 3 (7.3) | 2 (9.5) | 1 (5.0) | ||
| Marrow CR | 9 (22.0) | 4 (19.0) | 5 (25.0) | ||
| SD | 15 (36.6) | 6 (28.6) | 9 (45.0) | ||
| PD | 8 (19.5) | 5 (23.8) | 3 (15.0) | ||
| Hematological improvement, n (%) | HI-E | 18 (40.9) | 9 (37.5) | 9 (45.0) | 0.760 |
| HI-P | 16 (50.0) | 12 (57.1) | 4 (36.4) | 0.458 | |
| HI-N | 10 (50.0) | 3 (42.9) | 7 (53.8) | 1.000 | |
| Severe hematological adverse event, n (%) | Neutropenia | 29 (58.0) | 17 (63.0) | 12 (52.2) | 0.567 |
| Thrombocytopenia | 24 (48.0) | 17 (63.0) | 7 (30.4) | 0.027 | |
| Anemia | 17 (34.0) | 13 (48.1) | 4 (17.4) | 0.036 | |
| FN | 21 (42.0) | 13 (48.1) | 8 (34.8) | 0.398 | |
| Severe non-hematological adverse event, n (%) | Infection | 16 (32.0) | 10 (37.0) | 6 (26.1) | 0.546 |
| Other | 6 (12.0) | 5 (18.5) | 1 (4.3) | 0.199 |
| Neutropenia | Thrombocytopenia | Anemia | ||||
|---|---|---|---|---|---|---|
| Factor | OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value |
| Dose of AZA: 75 mg/m2 | 0.91 (0.28–3.01) | 0.882 | 1.48 (0.40–5.43) | 0.557 | 0.77 (0.21–2.85) | 0.698 |
| Days of AZA treatment: 7 days | 0.53 (0.15–1.83) | 0.317 | 0.28 (0.07–1.14) | 0.076 | 0.39 (0.09–1.74) | 0.216 |
| SMD | 1.45 (0.44–4.78) | 0.544 | 4.36 (1.17–16.20) | 0.028 | 4.00 (1.01–15.80) | 0.048 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Takada, E.; Nakamura, N.; Kaneda, Y.; Fukuno, K.; Lee, S.; Fujita, K.; Morishita, T.; Ikoma, Y.; Matsumoto, T.; Nakamura, H.; et al. Impact of Skeletal Muscle Depletion on Patients with Myelodysplastic Syndrome Treated with Azacitidine. Hematol. Rep. 2024, 16, 114-124. https://doi.org/10.3390/hematolrep16010012
Takada E, Nakamura N, Kaneda Y, Fukuno K, Lee S, Fujita K, Morishita T, Ikoma Y, Matsumoto T, Nakamura H, et al. Impact of Skeletal Muscle Depletion on Patients with Myelodysplastic Syndrome Treated with Azacitidine. Hematology Reports. 2024; 16(1):114-124. https://doi.org/10.3390/hematolrep16010012
Chicago/Turabian StyleTakada, Eri, Nobuhiko Nakamura, Yuto Kaneda, Kenji Fukuno, Shin Lee, Kei Fujita, Tetsuji Morishita, Yoshikazu Ikoma, Takuro Matsumoto, Hiroshi Nakamura, and et al. 2024. "Impact of Skeletal Muscle Depletion on Patients with Myelodysplastic Syndrome Treated with Azacitidine" Hematology Reports 16, no. 1: 114-124. https://doi.org/10.3390/hematolrep16010012
APA StyleTakada, E., Nakamura, N., Kaneda, Y., Fukuno, K., Lee, S., Fujita, K., Morishita, T., Ikoma, Y., Matsumoto, T., Nakamura, H., Kitagawa, J., Kanemura, N., Kasahara, S., Hara, T., Tsurumi, H., & Shimizu, M. (2024). Impact of Skeletal Muscle Depletion on Patients with Myelodysplastic Syndrome Treated with Azacitidine. Hematology Reports, 16(1), 114-124. https://doi.org/10.3390/hematolrep16010012