

Primary Bone Lymphoma of the Scapula


Abstract
1. Introduction
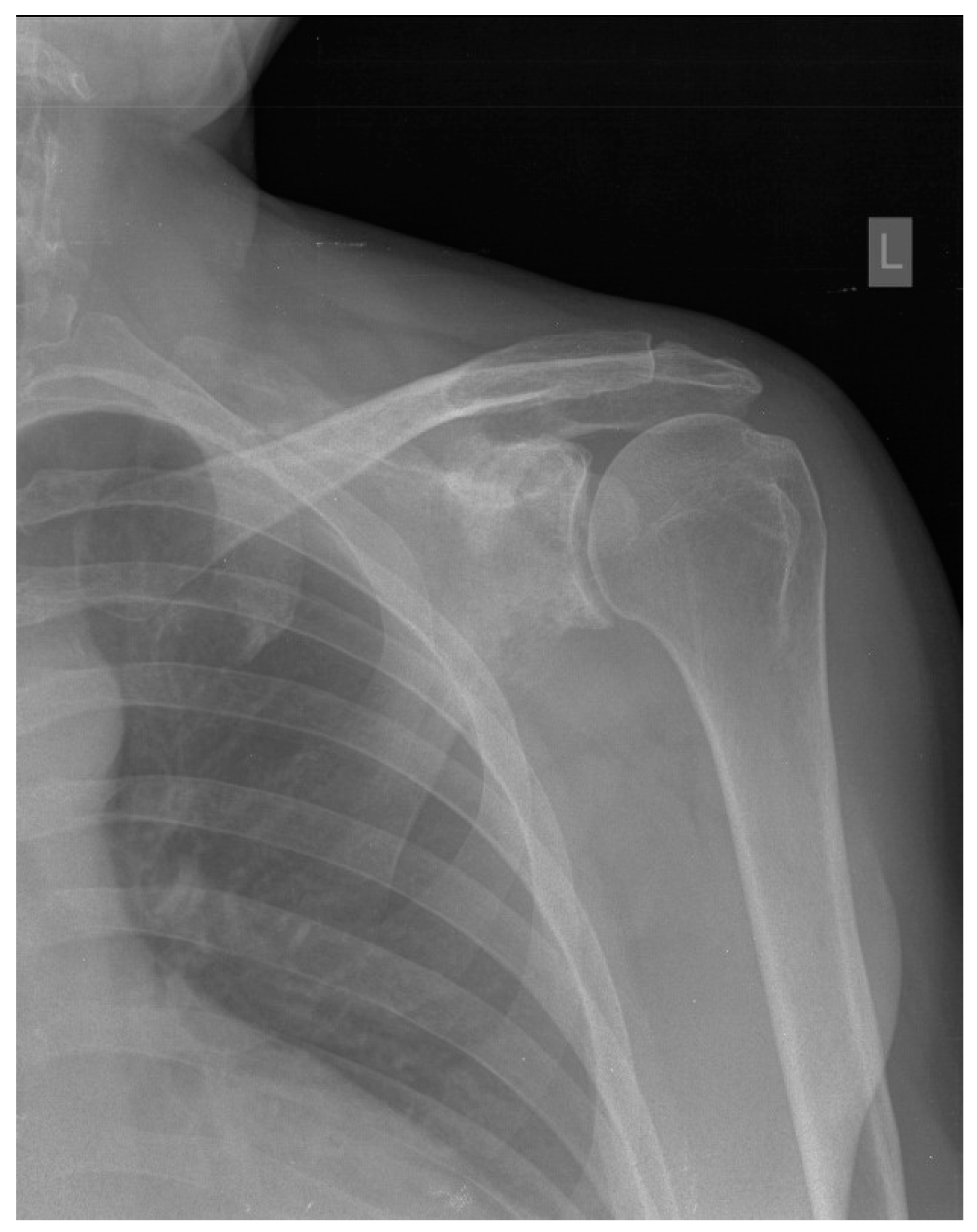
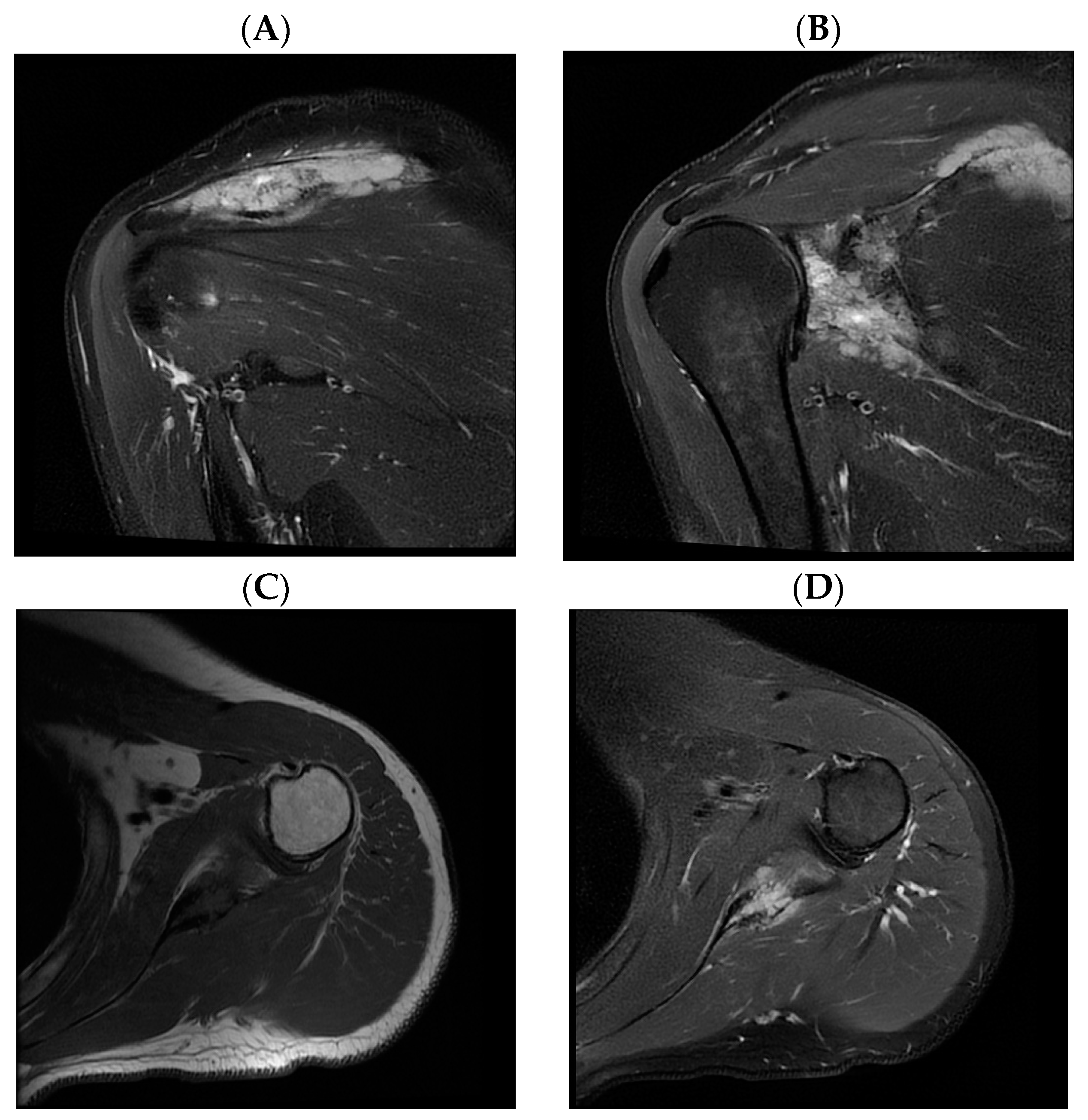
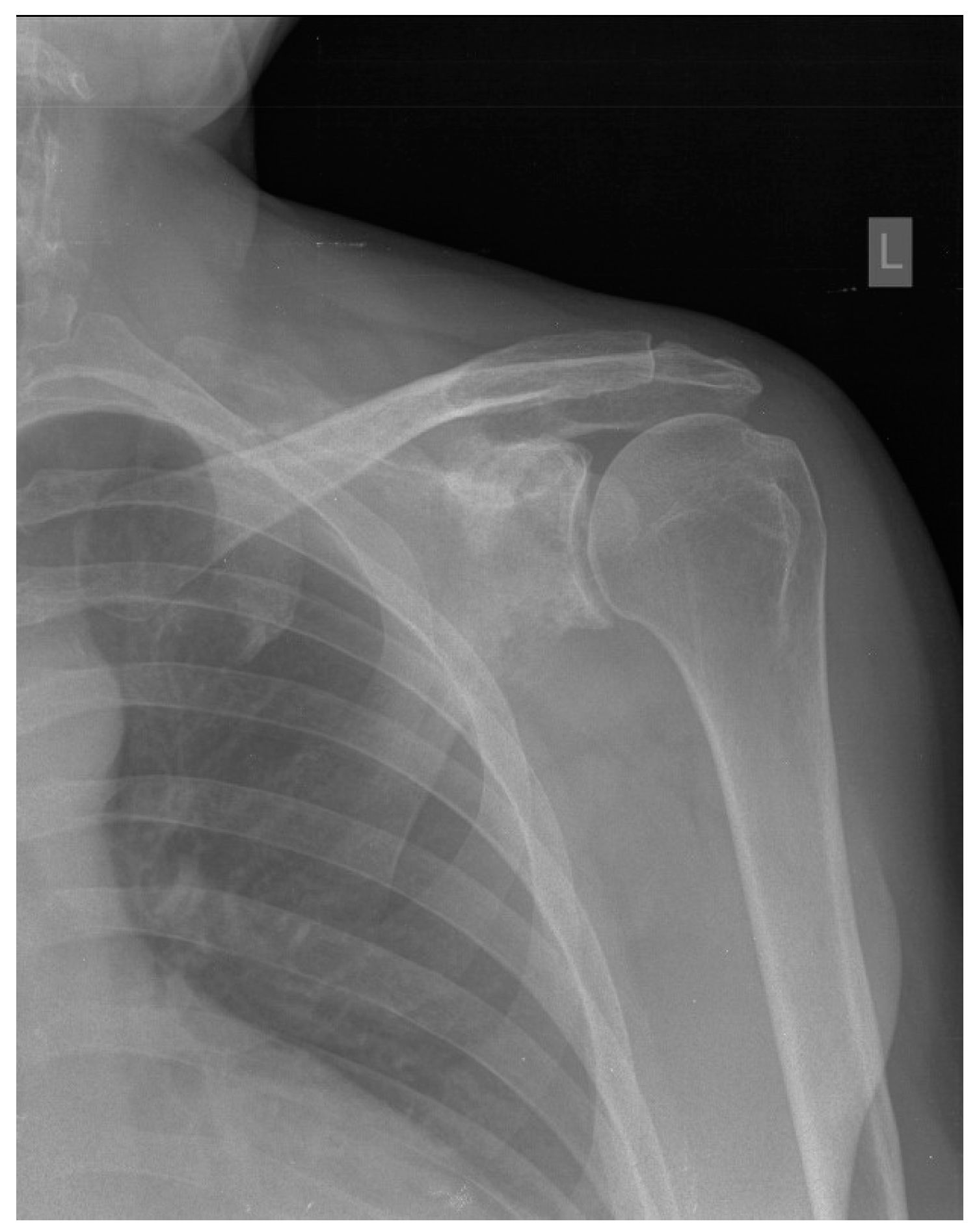
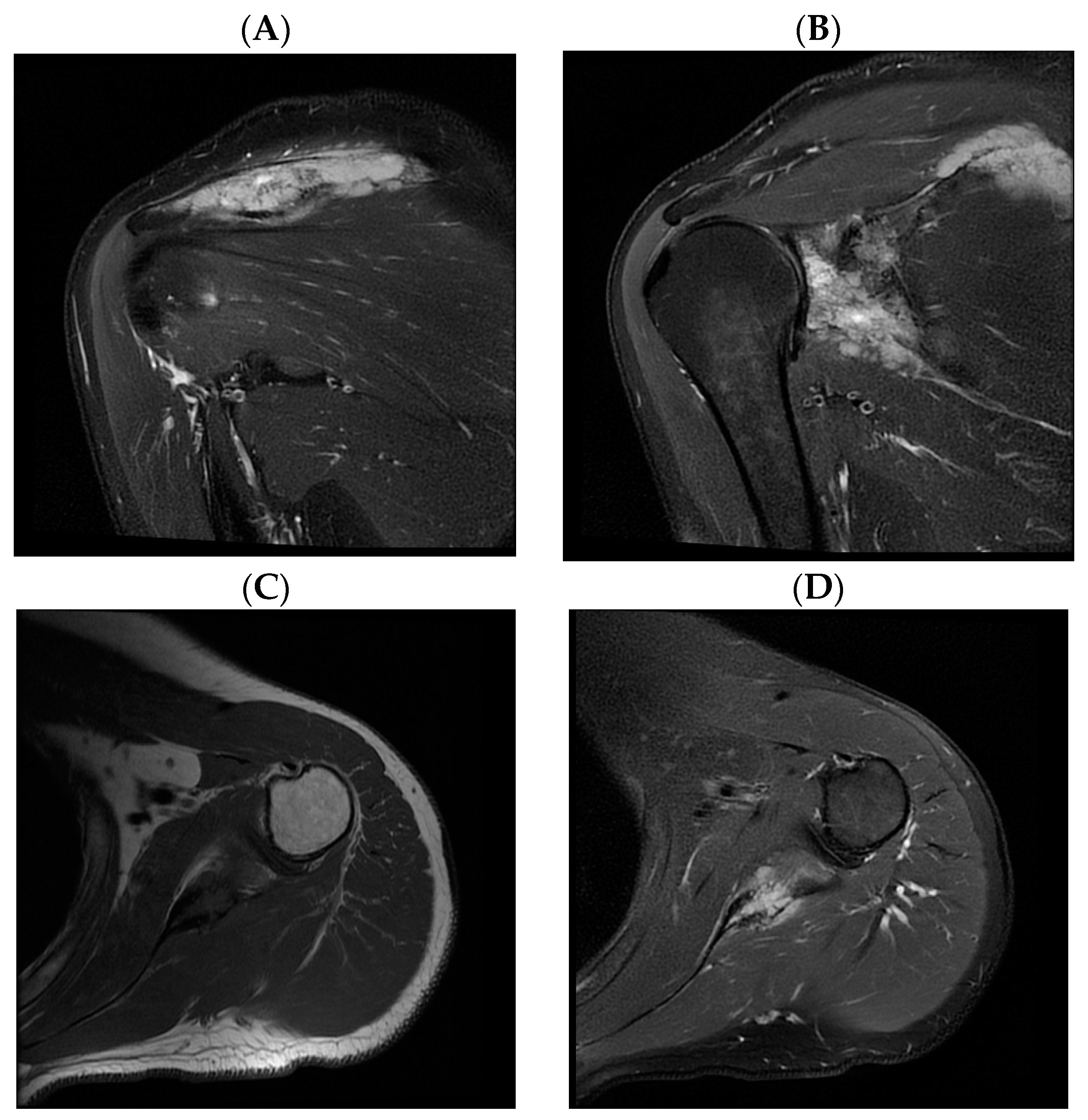
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vitolo, U.; Seymour, J.F.; Martelli, M.; Illerhaus, G.; Illidge, T.; Zucca, E.; Campo, E.; Ladetto, M. Extranodal diffuse large B-cell lymphoma (DLBCL) and primary mediastinal B-cell lymphoma: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2016, 27, 91–102. [Google Scholar] [CrossRef]
- 2. Diffuse Large B-Cell Lymphoma—Cancer Stat Facts [Internet]. SEER. Available online: https://seer.cancer.gov/statfacts/html/dlbcl.html (accessed on 24 April 2021).
- Morton, L.M.; Slager, S.L.; Cerhan, J.R.; Wang, S.S.; Vajdic, C.M.; Skibola, C.F.; Bracci, P.M.; de Sanjosé, S.; Smedby, K.E.; Chiu, B.C.; et al. Etiologic heterogeneity among non-hodgkin lymphoma subtypes: The interLymph non-hodgkin lymphoma subtypes project. J. Natl. Cancer Inst. Monogr. 2014, 2014, 130–144. [Google Scholar] [CrossRef]
- Padala, S.A.; Kallam, A. Diffuse Large B-Cell Lymphoma. In StatPearls[Internet]; StatPearlsPublishing: Treasure Island, FL, USA, 2024. Available online: https://www.ncbi.nlm.nih.gov/books/NBK557796/ (accessed on 24 April 2021).
- Marotta, D.; Sgambato, A.; Cerciello, S.; Magarelli, N.; Martini, M.; Maria, L.M.; Maccauro, G. Soft tissue non-Hodgkin lymphoma of shoulder in a HIV patient: A report of a case and review of the literature. World J. Surg. Oncol. 2008, 6, 1–6. [Google Scholar] [CrossRef]
- Arredondo, J.; Worland, R.L.; Sinnenberg, R.J.J.; Qureshi, G. Non-Hodgkin’s Lymphoma as an Unexpected Diagnosis in a Shoulder Arthroplasty. J. Arthroplast. Vol. 1999, 14, v108–v111. [Google Scholar] [CrossRef]
- Chauhan, N.R.; Chick, J.F.B.; Khurana, B. Annihilation of the acromion: A rare case of primary scapular lymphoma. J. Emerg. Med. 2013, 44, e389–e390. [Google Scholar] [CrossRef]
- Carroll, G.; Breidahl, W.; Robbins, P. Musculoskeletal lymphoma: MRI of bone or soft tissue presentations. J. Med. Imaging Radiat Oncol. 2013, 57, 663–673. [Google Scholar] [CrossRef]
- Boulytcheva, I.V.; Sciotto, C.; Soloviev, Y.; Kushlinskii, N.E. Diffuse large B-cell lymphoma presented as bone lesions. A study of 21 cases and review of the literature. Mol. Meditsina 2013, 11, 44–47. [Google Scholar]
- Das, D.K.; Pathan, S.K.; Al-Waheeb, S.K.M.; Ali, A.E.; Joneja, M.; Al-Kanderi, M.G.; John, B.; Mallik, M.K. Chest wall lymphomas: Fine needle aspiration cytodiagnosis and review of the literature. Cytopathology 2017, 28, 364–370. [Google Scholar] [CrossRef]
- Yousef, M.H.A.H.; Audat, Z.; Al-Shorafat, D.M.; Al-Khatib, S.; Daoud, A.K. Primary Diffuse Large B Cell Lymphoma of Bone: A Single-Center Experience. J. Blood Med. 2022, 13, 143–149. [Google Scholar] [CrossRef]
- Nikonova, A.; Guirguis, H.R.; Buckstein, R.; Cheung, M.C. Predictors of delay in diagnosis and treatment in diffuse large B-cell lymphoma and impact on survival. Br. J. Haematol. 2015, 168, 492–500. [Google Scholar] [CrossRef]
- Messina, C.; Christie, D.; Zucca, E.; Gospodarowicz, M.; Ferreri, A.J.M. Primary and secondary bone lymphomas. Cancer Treat Rev. 2015, 41, 235–246. [Google Scholar] [CrossRef]
- Zelenetz, A.D.; Gordon, L.I.; Chang, J.E.; Christian, B.; Abramson, J.S.; Advani, R.H.; Bartlett, N.L.; Budde, E.L.; Caimi, P.F.; De Vos, S.; et al. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) B-Cell Lymphomas Version 4.2021—5 May 2021. J. Natl. Compr. Cancer Netw 2021, 19, 1227–1230. [Google Scholar]
- Bhagavathi, S.; Fu, K. Primary Bone Lymphoma. Arch. Pathol. Lab. Med. 2009, 133, 1868–1871. [Google Scholar] [CrossRef]
- Subramanian, S.; Viswanathan, V.K. Lytic Bone Lesions—StatPearls—NCBI Bookshelf [Internet]. NCBI. 2018. Available online: https://www.ncbi.nlm.nih.gov/books/NBK539837/ (accessed on 21 May 2021).
- Haussler, M.D.; Fenstermacher, M.J.; Johnston, D.A.; Harle, T.S. MRI of primary lymphoma of bone: Cortical disorder as a criterion for differential diagnosis. J. Magn. Reson. Imaging 1999, 9, 93–100. [Google Scholar] [CrossRef]
- Mengiardi, B.; Honegger, H.; Hodler, J.; Exner, U.G.; Csherhati, M.D.; Brühlmann, W. Primary lymphoma of bone: MRI and CT characteristics during and after successful treatment. Am. J. Roentgenol. 2005, 184, 185–192. [Google Scholar] [CrossRef]
- Dabaja, B.S.; Vanderplas, A.M.; Crosby-Thompson, A.L.; Abel, G.A.; Czuczman, M.S.; Friedberg, J.W.; Gordon, L.I.; Kaminski, M.; Niland, J.; Millenson, M.; et al. Radiation for diffuse large B-cell lymphoma in the rituximab era: Analysis of the National Comprehensive Cancer Network lymphoma outcomes project. In Cancer [Internet]; John Wiley and Sons Inc.: Hoboken, NJ, USA, 2015; pp. 1032–1039. [Google Scholar]
- Huang, H.; Li, X.; Zhu, J.; Ye, S.; Zhang, H.; Wang, W. Entecavir vs Lamivudine for Prevention of Hepatitis B Virus Reactivation Among Patients With Untreated Diffuse Large B-Cell Lymphoma Receiving R-CHOP Chemotherapy A Randomized Clinical Trial. JAMA 2015, 312, 2521–2530. [Google Scholar] [CrossRef]
- Dong, H.J.; Ni, L.N.; Sheng, G.F.; Song, H.L.; Xu, J.Z.; Ling, Y. Risk of hepatitis B virus (HBV) reactivation in non-Hodgkin lymphoma patients receiving rituximab-chemotherapy: A meta-analysis. J. Clin. Virol. 2013, 57, 209–214. [Google Scholar] [CrossRef]
- Yu, S.; Luo, H.; Pan, M.; Luis, A.P.; Xiong, Z.; Shuai, P.; Zhang, Z. Comparison of entecavir and lamivudine in preventing HBV reactivation in lymphoma patients undergoing chemotherapy: A meta-analysis. Int. J. Clin. Pharm. 2016, 38, 1035–1043. [Google Scholar] [CrossRef]
- Lampertico, P.; Agarwal, K.; Berg, T.; Buti, M.; Janssen, H.L.A.; Papatheodoridis, G.; Zoulim, F.; Tacke, F. EASL 2017 Clinical Practice Guidelines on the management of hepatitis B virus infection. J. Hepatol. 2017, 67, 370–398. [Google Scholar] [CrossRef]
- Gutfreund, K.S.; Williams, M.; George, R.; Bain, V.G.; Ma, M.M.; Yoshida, E.M.; Yoshida, E.M.; Villeneuve, J.P.; Fischer, K.P.; Tyrrell, D.L. Genotypic succession of mutations of the hepatitis B virus polymerase associated with lamivudine resistance. Microbiology 2000, 33, 469–475. [Google Scholar] [CrossRef]
- Santini, D.; Vincenzi, B.; Dicuonzo, G.; Avvisati, G.; Massacesi, C.; Battistoni, F.; Gavasci, M.; Rocci, L.; Tirindelli, M.C.; Altomare, V.; et al. Zoledronic acid induces significant and long-lasting modifications of circulating angiogenic factors in cancer patients. Clin. Cancer Res. 2003, 9, 2893–2897. [Google Scholar] [PubMed]
- Winter, M.C.; Holen, I.; Coleman, R.E. Exploring the anti-tumour activity of bisphosphonates in early breast cancer. Cancer Treat Rev. 2008, 34, 453–475. [Google Scholar] [CrossRef] [PubMed]
- Inoue, N.; Nishimura, N.; Takahashi, A.; Kusano, Y.; Yamauchi, H.; Ueda, K. Negative impact of Zolendronic acid in R-CHOP treated DLBCL with bone metastsis. Hematol. Oncol. 2017, 3, 340–341. [Google Scholar] [CrossRef]
- Valachis, A.; Polyzos, N.P.; Coleman, R.E.; Gnant, M.; Eidtmann, H.; Brufsky, A.M.; Aft, R.; Tevaarwerk, A.J.; Swenson, K.; Lind, P.; et al. Adjuvant therapy with zoledronic acid in patients with breast cancer: A systematic review and meta-analysis. Oncologist 2013, 1, 84–101. [Google Scholar] [CrossRef]
- Himelstein, A.L.; Foster, J.C.; Khatcheressian, J.L.; Roberts, J.D.; Seisler, D.K.; Novotny, P.J.; Qin, R.; Go, R.S.; Grubbs, S.S.; O’Connor, T.; et al. Effect of longer-interval vs standard dosing of zoledronic acid on skeletal events in patients with bone metastases: A randomized clinical trial. JAMA—J. Am. Med. Assoc. 2017, 317, 48–58. Available online: https://jamanetwork.com/ (accessed on 25 May 2021). [CrossRef]
- Iversen, P.O.; Negaard, H.; Østenstad, B.; Sandset, P.M.; Kolset, S.O. Evidence for long-term hypercoagulopathy, but normalization of markers of extracellular matrix turnover, in patients with non-Hodgkin lymphoma. Leuk. Lymphoma 2015, 56, 2479–2481. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| 1st Author and Year of Publication | Sex/Age | Presentation | Time between Symptom Onset and Diagnosis/ Time between First Hospital Visit and Diagnosis | Involvement of Other Sites | Treatment | Outcome |
|---|---|---|---|---|---|---|
| Chauhan [7], 2013 | F/84 y | Pain | Two months/ days-weeks | Surrounding soft tissue | R-CHOP chemotherapy | Remission |
| Carroll [8], 2013 | M/29 y | Lump | Nd/Nd | Nd | Nd | Nd |
| Boulytcheva [9], 2013 | F/73 y | Nd | Nd | Nd | Radiotherapy | Death |
| Das [10], 2017 | M/73 y | Nd | Nd | Nd | Nd | Nd |
| Ayesh Haj Yousef [11], 2022 | F/46 y | Mass | Two months/Nd | Nd | R-CHOP chemotherapy + radiotherapy | Remission |
| Our patient | M/45 y | Paresthesia, tingling, numbness and edema of the little and ring fingers | Two years/ two years | Surrounding soft tissue | R-CHOP chemotherapy + radiotherapy | Remission |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lovaković, J.; Mandac Smoljanović, I.; Matković, A.; Smoljanović, T. Primary Bone Lymphoma of the Scapula. Hematol. Rep. 2024, 16, 106-113. https://doi.org/10.3390/hematolrep16010011
Lovaković J, Mandac Smoljanović I, Matković A, Smoljanović T. Primary Bone Lymphoma of the Scapula. Hematology Reports. 2024; 16(1):106-113. https://doi.org/10.3390/hematolrep16010011
Chicago/Turabian StyleLovaković, Josip, Inga Mandac Smoljanović, Andro Matković, and Tomislav Smoljanović. 2024. "Primary Bone Lymphoma of the Scapula" Hematology Reports 16, no. 1: 106-113. https://doi.org/10.3390/hematolrep16010011
APA StyleLovaković, J., Mandac Smoljanović, I., Matković, A., & Smoljanović, T. (2024). Primary Bone Lymphoma of the Scapula. Hematology Reports, 16(1), 106-113. https://doi.org/10.3390/hematolrep16010011