

Oral Manifestations: A Warning-Sign in Children with Hematological Disease Acute Lymphocytic Leukemia

 ,
, {kind=link}
{kind=link}
Abstract
1. Introduction
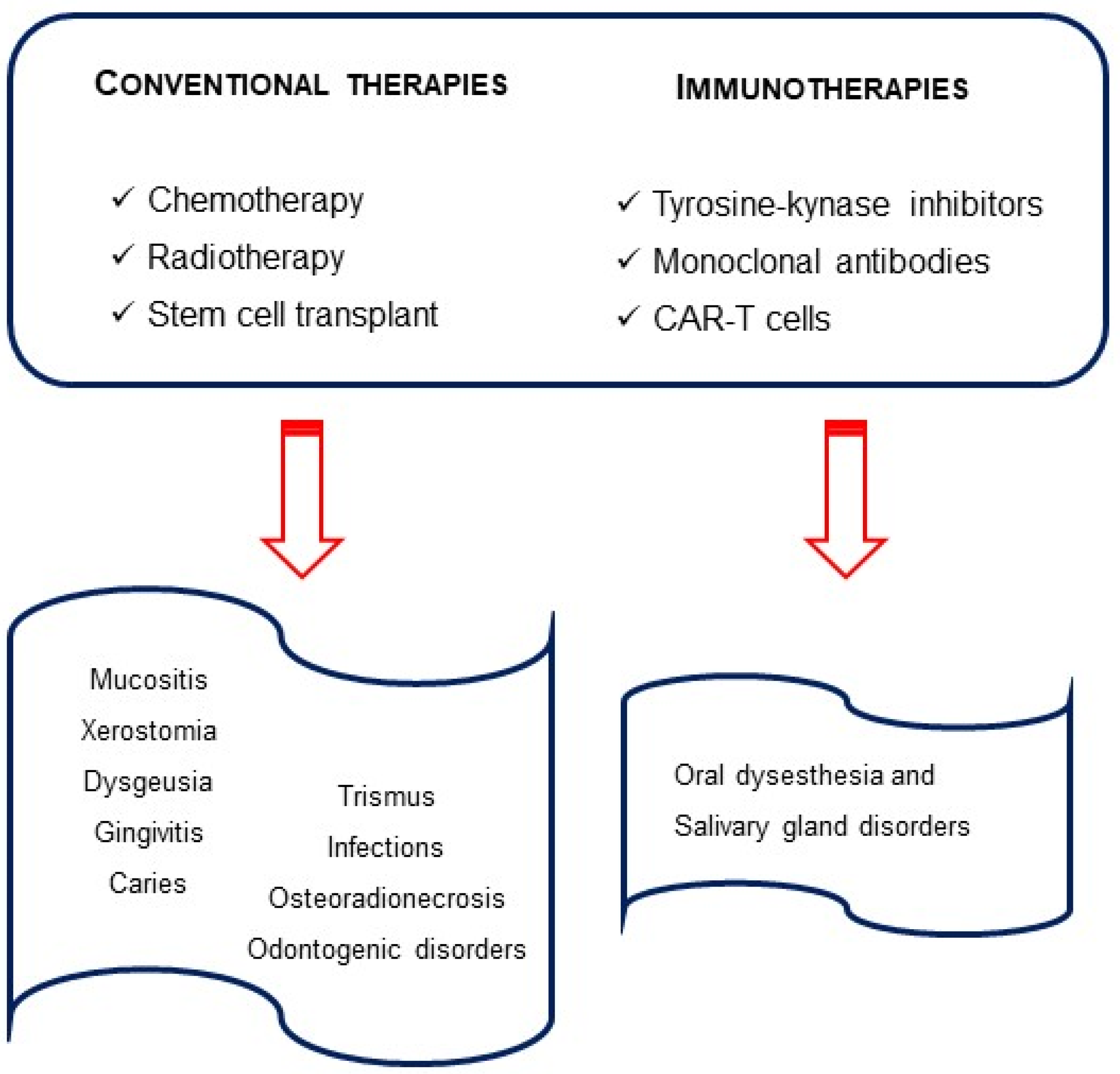
2. Oral Complications in Children with Acute Lymphoblastic Leukemia
- Primary complications, which occur mainly due to the disease itself; these result from the infiltration of malignant cells into oral structures, such as the gum and bone, and gingival edema or tooth pain due to pulp infiltration.
- Secondary complications are usually associated with a direct effect of radiation therapy or chemotherapy, such as thrombocytopenia, anemia and granulocytopenia. These include a tendency to bleed or susceptibility to infections.
- Tertiary complications usually occur due to the complex interactions of therapy and its side effects, such as immunosuppression. They include ulcerations, inflammation of the mucous membranes, osteoradionecrosis, xerostomia, taste alterations, trismus or carious lesions [26].
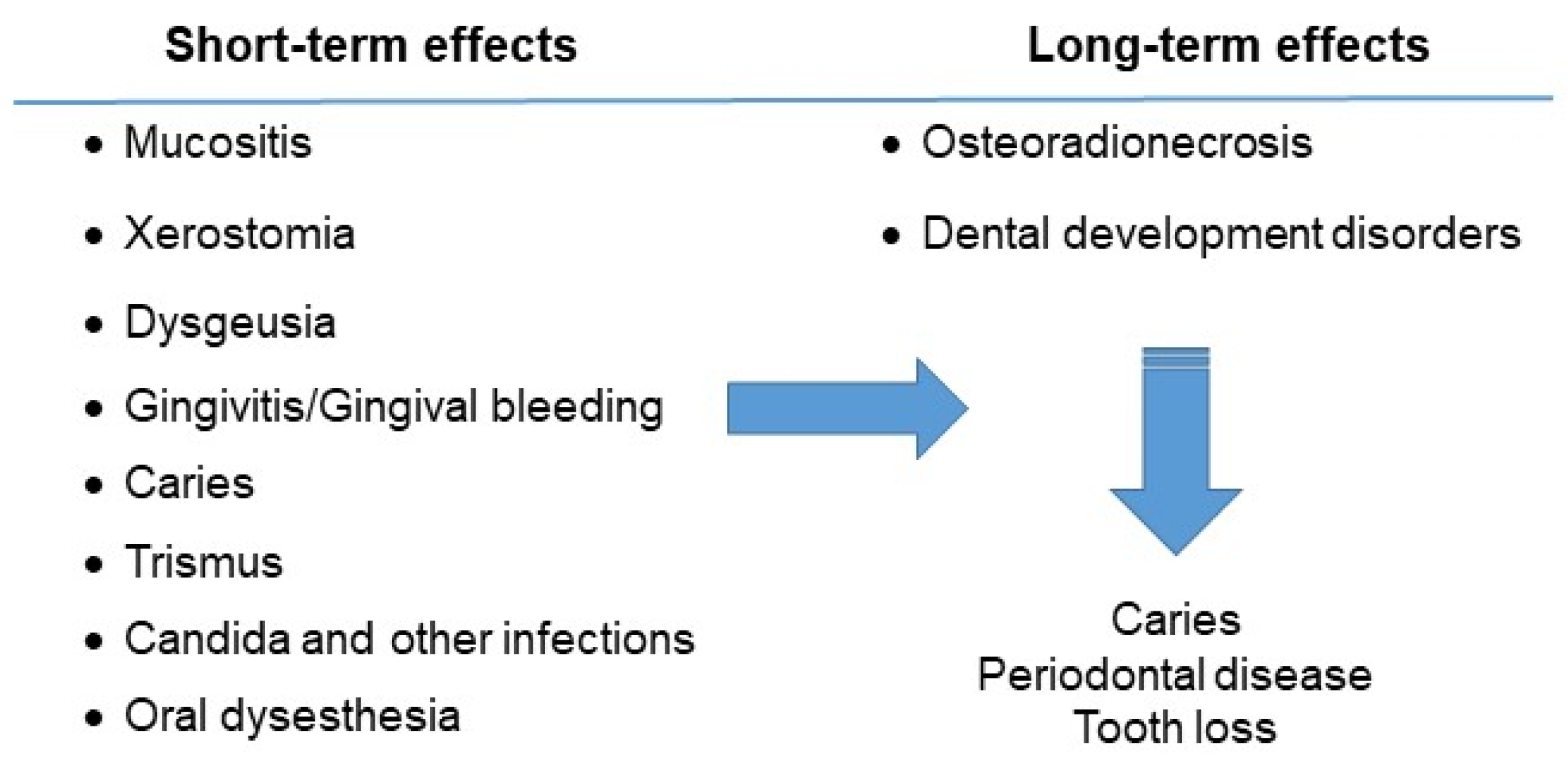
2.1. Mucositis
2.2. Xerostomia
2.3. Dysgeusia
2.4. Gingivitis and Gingival Bleeding
2.5. Caries
2.6. Trismus
2.7. Candida and Other Infections
2.8. Osteoradionecrosis
2.9. Oral Dysesthesia
2.10. Dental Developmental Disorders
3. Dental Care and Management of the Child Patient
3.1. Before Chemotherapy
- (a)
- To identify and stabilize or eliminate possible sources of infection and local irritants in the oral cavity in order to avoid delaying cancer treatment or inducing other complications. Any existing lesions that might normally lie dormant can flare up and become life threatening once the child is immunosuppressed.
- (b)
- To educate patients and parents about the importance of optimal oral care to minimize oral problems and discomfort before, during and after cancer treatment.
- (c)
3.2. During Chemotherapy
- (a)
- To maintain optimal oral health during cancer therapy.
- (b)
- To manage any oral side effects that may develop because of the cancer therapy.
- (c)
3.3. After Chemotherapy
- (a)
- To maintain optimal oral health.
- (b)
- To reinforce the importance of optimal oral and dental care for life to the patient/parents [66].
4. Concluding Remarks
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Madhusoodhan, P.P.; Carroll, W.L.; Bhatla, T. Progress and Prospects in Pediatric Leukemia. Curr. Probl. Pediatr. Adolesc. Health Care 2016, 46, 229–241. [Google Scholar] [CrossRef] [PubMed]
- Fathi, A.; Mirzarahimi, M.; Farajkhah, H. Réponse à un schéma chimiothérapeutique administré à des enfants atteints de LAL à cellules pré-B à risque élevé selon le protocole COG. Can. Oncol. Nurs. J. 2021, 31, 334–338. [Google Scholar] [CrossRef] [PubMed]
- Lim, H.-C.; Kim, C.-S. Oral signs of acute leukemia for early detection. J. Periodontal Implant. Sci. 2014, 44, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Global Cancer Observatory (iarc.fr). 2022. Available online: https://gco.iarc.fr/today/home (accessed on 20 December 2022).
- Seth, R.; Singh, A. Leukemias in Children. Indian J. Pediatr. 2015, 82, 817–824. [Google Scholar] [CrossRef] [PubMed]
- Tarlock, K.; Dahl, G.; Lacayo, N. Acute myeloid leukemia in children. In Wintrobe’s Clinical Hematology, 14th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2018; pp. 5016–5095. [Google Scholar]
- Zimmermann, C.; Meurer, M.I.; Grando, L.J.; Del Moral, J.G.; Rath, I.B.d.S.; Tavares, S.S. Dental Treatment in Patients with Leukemia. J. Oncol. 2015, 2015, 571739. [Google Scholar] [CrossRef]
- Babu, K.L.G.; Mathew, J.; Doddamani, G.M.; Narasimhaiah, J.K.; Naik, L.R.K. Oral health of children with acute lymphoblastic leukemia: A review. J. Orofac. Sci. 2016, 8, 3. [Google Scholar] [CrossRef]
- Svsg, N. Dental Care of Children with Leukemia—An Overview. J. Pediatr. Neonatal Care 2016, 4, 00157. [Google Scholar] [CrossRef]
- Imbach, P.; Kuhne, T.; Arceci, R. Pediatric Oncology Book 2011; Springer: Berlin/Heidelberg, Germany, 2011. [Google Scholar]
- Baytan, B.; Evim, M.S.; Güler, S.; Güneş, A.M.; Okan, M. Acute Central Nervous System Complications in Pediatric Acute Lymphoblastic Leukemia. Pediatr. Neurol. 2015, 53, 312–318. [Google Scholar] [CrossRef]
- Deak, D.; Gorcea-Andronic, N.; Sas, V.; Teodorescu, P.; Constantinescu, C.; Iluta, S.; Pasca, S.; Hotea, I.; Turcas, C.; Moisoiu, V.; et al. A narrative review of central nervous system involvement in acute leukemias. Ann. Transl. Med. 2021, 9, 68. [Google Scholar] [CrossRef]
- Del Principe, M.I.; Maurillo, L.; Buccisano, F.; Sconocchia, G.; Cefalo, M.; De Santis, G.; Di Veroli, A.; Ditto, C.; Nasso, D.; Postorino, M.; et al. Central nervous system involvement in adult acute lymphoblastic leukemia: Diagnostic tools, prophylaxis, and therapy. Mediterr. J. Hematol. Infect. Dis. 2014, 6, e2014075. [Google Scholar] [CrossRef]
- Johnston, D.L.; Alonzo, T.A.; Gerbing, R.B.; Aplenc, R.; Woods, W.G.; Meshinchi, S.; Gamis, A.S. Central nervous system disease in pediatric acute myeloid leukemia: A report from the Children’s Oncology Group. Pediatr. Blood Cancer 2017, 64, e26612. [Google Scholar] [CrossRef] [PubMed]
- Tebbi, C.K. Etiology of Acute Leukemia: A Review. Cancers 2021, 13, 2256. [Google Scholar] [CrossRef] [PubMed]
- Van Delft, F.W.; Saha, V. Molecular Techniques to Improve Outcome in Childhood ALL pp111-12. In Pediatric Hematology Methods and Protocols; Goulden, N.J., Steward, C.G., Eds.; Humana Press: Totowa, NJ, USA, 2004. [Google Scholar]
- Cho, S.Y.; Cheng, A.C.; Cheng, M.C. Oral care for children with leukaemia. Hong Kong Med. J. 2018, 6, 203–208. [Google Scholar]
- Valéra, M.-C.; Noirrit-Esclassan, E.; Pasquet, M.; Vaysse, F. Oral complications and dental care in children with acute lymphoblastic leukaemia. J. Oral Pathol. Med. 2015, 44, 483–489. [Google Scholar] [CrossRef]
- Lowal, K.; Alaizari, N.; Tarakji, B.; Petro, W.; Hussain, K.; Altamimi, M. Dental Considerations for Leukemic Pediatric Patients: An Updated Review for General Dental Practitioner. Mater. Socio Medica 2015, 27, 359–362. [Google Scholar] [CrossRef] [PubMed]
- Francisconi, C.F.; Caldas, R.J.; Martins, L.J.O.; Rubira, C.M.F.; Santos, P.S.d.S. Leukemic Oral Manifestations and their Management. Asian Pac. J. Cancer Prev. 2016, 17, 911–915. [Google Scholar] [CrossRef]
- Rafei, H.; Daher, M.; Rezvani, K. Chimeric antigen receptor (CAR) natural killer (NK)-cell therapy: Leveraging the power of innate immunity. Br. J. Haematol. 2020, 193, 216–230. [Google Scholar] [CrossRef]
- Packer, R.J.; Pfister, S.; Bouffet, E.; Avery, R.; Bandopadhayay, P.; Bornhorst, M.; Bowers, D.C.; Ellison, D.; Fangusaro, J.; Foreman, N.; et al. Pediatric low-grade gliomas: Implications of the biologic era. Neuro-Oncology 2016, 19, 750–761. [Google Scholar] [CrossRef]
- Shen, C.J.; Terezakis, S.A. The Evolving Role of Radiotherapy for Pediatric Cancers with Advancements in Molecular Tumor Characterization and Targeted Therapies. Front. Oncol. 2021, 11, 679701. [Google Scholar] [CrossRef]
- Ritwik, P.; Chrisentery-Singleton, T.E. Oral and dental considerations in pediatric cancers. Cancer Metastasis Rev. 2020, 39, 43–53. [Google Scholar] [CrossRef]
- Mathur, V.P.; Kalra, G.; Dhillon, J.K. Oral health in children with leukemia. Indian J. Palliat. Care 2012, 18, 12–18. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Zeng, X.; Yang, X.; Que, J.; Du, Q.; Zhang, Q.; Zou, J. Oral Health, Caries Risk Profiles, and Oral Microbiome of Pediatric Patients with Leukemia Submitted to Chemotherapy. BioMed Res. Int. 2021, 2021, 6637503. [Google Scholar] [CrossRef] [PubMed]
- Lula, E.C.d.O.; Lula, C.E.d.O.; Alves, C.M.C.; Lopes, F.F.; Pereira, A.L.A. Chemotherapy-induced oral complications in leukemic patients. Int. J. Pediatr. Otorhinolaryngol. 2007, 71, 1681–1685. [Google Scholar] [CrossRef] [PubMed]
- Brown, T.J.; Gupta, A. Management of Cancer Therapy–Associated Oral Mucositis. J. Oncol. Pract. 2015, 16, 103–109. [Google Scholar] [CrossRef] [PubMed]
- American Academy of Pediatric Dentistry (AAPD). Dental Management of Pediatric Patients Receiving Immunosuppressive Therapy and/or Head and Neck Radiation; The Reference Manual of Pediatric Dentistry: American Academy of Pediatric Dentistry: Chicago, IL, USA, 2022; pp. 507–516. [Google Scholar]
- Stolze, J.; Vlaanderen, K.C.E.; Holtbach, F.C.E.D.; Teepen, J.C.; Kremer, L.C.M.; Loonen, J.J.; Broeder, E.v.D.-D.; Heuvel-Eibrink, M.M.v.D.; van der Pal, H.J.H.; Versluys, B.; et al. Long-Term Effects of Childhood Cancer Treatment on Dentition and Oral Health: A Dentist Survey Study from the DCCSS LATER 2 Study. Cancers 2021, 13, 5264. [Google Scholar] [CrossRef] [PubMed]
- Jensen, S.; Pedersen, A.; Reibel, J.; Nauntofte, B. Xerostomia and hypofunction of the salivary glands in cancer therapy. Support. Care Cancer 2003, 11, 207–225. [Google Scholar] [CrossRef] [PubMed]
- Stolze, J.; Teepen, J.C.; Raber-Durlacher, J.E.; Loonen, J.J.; Kok, J.L.; Tissing, W.J.E.; de Vries, A.C.H.; Neggers, S.J.C.M.M.; Broeder, E.v.D.-D.; Heuvel-Eibrink, M.M.v.D.; et al. Prevalence and Risk Factors for Hyposalivation and Xerostomia in Childhood Cancer Survivors Following Different Treatment Modalities—A Dutch Childhood Cancer Survivor Study Late Effects 2 Clinical Study (DCCSS LATER 2). Cancers 2022, 14, 3379. [Google Scholar] [CrossRef]
- Jensen, S.B.; Vissink, A.; Limesand, K.H.; E Reyland, M. Salivary Gland Hypofunction and Xerostomia in Head and Neck Radiation Patients. J. Natl. Cancer Inst.–Monogr. 2019, 53, 95–106. [Google Scholar] [CrossRef]
- Silva, I.M.; Donaduzzi, L.C.; Perini, C.C.; Couto, S.A.; Werneck, R.I.; de Araújo, M.R.; Kurahashi, M.; Johann, A.C.; Azevedo-Alanis, L.R.; Vieira, A.R.; et al. Association of xerostomia and taste alterations of patients receiving antineoplastic chemotherapy: A cause for nutritional concern. Clin. Nutr. ESPEN 2021, 43, 532–535. [Google Scholar] [CrossRef]
- Villa, A.; Connell, C.L.; Abati, S. Diagnosis and management of xerostomia and hyposalivation. Ther. Clin. Risk Manag. 2014, 11, 45–51. [Google Scholar] [CrossRef]
- Johnson, J.T.; Ferretti, G.A.; Nethery, W.J.; Valdez, I.H.; Fox, P.C.; Ng, D.; Muscoplat, C.C.; Gallagher, S.C. Oral pilocarpine for post-irradiation xerostomia in patients with head and neck cancer. New Engl. J. Med. 1993, 329, 390–395. [Google Scholar] [CrossRef]
- Brink, M.v.D.; Ijpma, I.; van Belkom, B.; Fiocco, M.; Havermans, R.C.; Tissing, W.J.E. Smell and taste function in childhood cancer patients: A feasibility study. Support. Care Cancer 2021, 29, 1619–1628. [Google Scholar] [CrossRef] [PubMed]
- Munankarmi, D. Management of Dysgeusia related to Cancer. J. Lumbini Med. Coll. 2017, 5, 10. [Google Scholar] [CrossRef][Green Version]
- Ponce-Torres, E.; Ruíz-Rodríguez, M.d.S.; Alejo-González, F.; Hernández-Sierra, J.F.; de Pozos-Guillén, A. Oral Manifestations in Pediatric Patients Receiving Chemotherapy for Acute Lymphoblastic Leukemia. J. Clin. Pediatr. Dent. 2010, 34, 275–279. [Google Scholar] [CrossRef] [PubMed]
- Kaskova, L.F.; Yanko, N.V.; Vashchenko, I.Y. Gingival health in children in the different phases of acute lymphoblastic leukemia. Curr. Issues Pharm. Med. Sci. 2019, 32, 134–137. [Google Scholar] [CrossRef]
- Shayani, A.; Aravena, P.C.; Rodríguez-Salinas, C.; Escobar-Silva, P.; Diocares-Monsálvez, Y.; Angulo-Gutiérrez, C.; Rivera, C. Chemotherapy as a risk factor for caries and gingivitis in children with acute lymphoblastic leukemia: A retrospective cohort study. Int. J. Paediatr. Dent. 2021, 32, 538–545. [Google Scholar] [CrossRef]
- Gawade, P.L.; Hudson, M.M.; Kaste, S.C.; Neglia, J.P.; Constine, L.S.; Robison, L.L.; Ness, K.K. A systematic review of dental late effects in survivors of childhood cancer. Pediatr. Blood Cancer 2014, 61, 407–416. [Google Scholar] [CrossRef]
- Al Humaid, J. Sweetener content and cariogenic potential of pediatric oral medications: A literature. Int. J. Health Sci. 2018, 12, 75–82. [Google Scholar]
- American Academy of Pediatric Dentistry (AAPD). Guideline on Dental Management of Pediatric Patients Receiving Chemotherapy, Hematopoietic Cell Transplantation, and/or Radiation Therapy; American Academy of Pediatric Dentistry: Chicago, IL, USA, 2013. [Google Scholar]
- Katz, J.; Peretz, B. Trismus in a 6 year old child: A manifestation of leukemia? J. Clin. Pediatr. Dent. 2002, 26, 337–339. [Google Scholar] [CrossRef]
- Satheeshkumar, P.; Mohan, M.P.; Jacob, J. Restricted mouth opening and trismus in oral oncology. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2014, 117, 709–715. [Google Scholar] [CrossRef]
- Yigit, M.; Bilir, A.; Yüksek, S.K.; Kaçar, D.; Özbek, N.Y.; Yarali, H.N. Antifungal Therapy in Pediatric Acute Lymphoblastic Leukemia. J. Pediatr. Hematol./Oncol. 2022, 44, e653–e657. [Google Scholar] [CrossRef] [PubMed]
- Brivio, E.; Cossio, A.; Borra, D.; Silvestri, D.; Prunotto, G.; Colombini, A.; Verna, M.; Rizzari, C.; Biondi, A.; Conter, V.; et al. Osteonecrosis in paediatric acute lymphoblastic leukaemia: Incidence, risk factors, radiological patterns and evolution in a single-centre cohort. Br. J. Haematol. 2022, 197, 602–608. [Google Scholar] [CrossRef] [PubMed]
- Kuhlen, M.; Kunstreich, M.; Gökbuget, N. Osteonecrosis in Adults with Acute Lymphoblastic Leukemia: An Unmet Clinical Need. Hemasphere 2021, 5, e544. [Google Scholar] [CrossRef]
- Pui, C.-H. Precision medicine in acute lymphoblastic leukemia. Front. Med. 2020, 14, 689–700. [Google Scholar] [CrossRef]
- Lejman, M.; Kuśmierczuk, K.; Bednarz, K.; Ostapińska, K.; Zawitkowska, J. Targeted Therapy in the Treatment of Pediatric Acute Lymphoblastic Leukemia—Therapy and Toxicity Mechanisms. Int. J. Mol. Sci. 2021, 22, 9827. [Google Scholar] [CrossRef] [PubMed]
- Ribera, J.-M.; Chiaretti, S. Modern Management Options for Ph+ ALL. Cancers 2022, 14, 4554. [Google Scholar] [CrossRef] [PubMed]
- Vigarios, E.; Epstein, J.B.; Sibaud, V. Oral mucosal changes induced by anticancer targeted therapies and immune checkpoint inhibitors. Support. Care Cancer 2017, 25, 1713–1739. [Google Scholar] [CrossRef] [PubMed]
- Partanen, M.; Alberts, N.M.; Conklin, H.M.; Krull, K.R.; Pui, C.-H.; Anghelescu, D.A.; Jacola, L.M. Neuropathic pain and neurocognitive functioning in children treated for acute lymphoblastic leukemia. Pain 2022, 163, 1070–1077. [Google Scholar] [CrossRef]
- Jasinski, S.; Reyes, F.A.D.L.; Yametti, G.C.; Pierro, J.; Raetz, E.; Carroll, W.L. Immunotherapy in Pediatric B-Cell Acute Lymphoblastic Leukemia: Advances and Ongoing Challenges. Pediatr. Drugs 2020, 22, 485–499. [Google Scholar] [CrossRef]
- Lv, M.; Liu, Y.; Liu, W.; Xing, Y.; Zhang, S. Immunotherapy for Pediatric Acute Lymphoblastic Leukemia: Recent Advances and Future Perspectives. Front. Immunol. 2022, 13, 921894. [Google Scholar] [CrossRef]
- Malczewska, M.; Kośmider, K.; Bednarz, K.; Ostapińska, K.; Lejman, M.; Zawitkowska, J. Recent Advances in Treatment Options for Childhood Acute Lymphoblastic Leukemia. Cancers 2022, 14, 2021. [Google Scholar] [CrossRef] [PubMed]
- Jodłowska, A.; Postek-Stefańska, L. Systemic Anticancer Therapy Details and Dental Adverse Effects in Children. Int. J. Environ. Res. Public Health 2022, 19, 6936. [Google Scholar] [CrossRef] [PubMed]
- Lupi, S.M.; Baena, A.R.Y.; Cervino, G.; Todaro, C.; Rizzo, S. Long-Term Effects of Acute Myeloid Leukemia Treatment on the Oral System in a Pediatric Patient. Open Dent. J. 2018, 12, 230–237. [Google Scholar] [CrossRef] [PubMed]
- Minicucci, E.M.; Lopes, L.F.; Crocci, A.J. Dental abnormalities in children after chemotherapy treatment for acute lymphoid leukemia. Leuk. Res. 2003, 27, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Lauritano, D.; Petruzzi, M. Decayed, missing and filled teeth index and dental anomalies in long-term survivors leukaemic children: A prospective controlled study. Med. Oral Patol. Oral Cir. Bucal. 2012, 17, e977–e980. [Google Scholar] [CrossRef] [PubMed]
- Proc, P.; Szczepańska, J.; Skiba, A.; Zubowska, M.; Fendler, W.; Młynarski, W. Dental Anomalies as Late Adverse Effect among Young Children Treated for Cancer. Cancer Res. Treat. 2016, 48, 658–667. [Google Scholar] [CrossRef]
- Çetiner, D.; Çetiner, S.; Uraz, A.; Alpaslan, G.H.; Alpaslan, C.; Memikoğlu, T.U.T.; Karadeniz, C. Oral and dental alterations and growth disruption following chemotherapy in long-term survivors of childhood malignancies. Support. Care Cancer 2019, 27, 1891–1899. [Google Scholar] [CrossRef]
- Otmani, N.; Nachef, M.; Alaoui, F.M. Prise en charge bucco-dentaire de l’enfant atteint de leucémie aiguë. Revue d’Odonto-Stomatologie 2004, 33, 17–27. [Google Scholar]
- Ferrández-Pujante, A.; Pérez-Silva, A.; Serna-Muñoz, C.; Fuster-Soler, J.L.; Galera-Miñarro, A.M.; Cabello, I.; Ortiz-Ruiz, A.J. Prevention and Treatment of Oral Complications in Hematologic Childhood Cancer Patients: An Update. Children 2022, 9, 566. [Google Scholar] [CrossRef]
- Padmini, C.; Bai, K.Y. Oral and Dental Considerations in Pediatric Leukemic Patient. ISRN Hematol. 2014, 2014, 895721. [Google Scholar] [CrossRef]
- Gholman, R.R.; El Meligy, O.A.; Felemban, E.H. Dental Rehabilitation of a Child with Acute Lymphocytic Leukemia: A Case Report. Int. J. Clin. Pediatr. Dent. 2019, 12, 582–586. [Google Scholar] [CrossRef] [PubMed]
- Hassan, A.; Manaf, A.; Zikra, A.; Burke, M.; Najla, N. Oral and dental management of people with myelodysplastic syn-dromes and acute myeloid leukemia: A systematic search and evidence based clinical guidance. Spec Care Dent. 2019, 39, 406–420. [Google Scholar]
- Costa, M.T.; Lenza, M.A.; Gosch, C.S.; Costa, I.; Ribeiro-Dias, F. In vitro evaluation of corrosion and cytotoxicity of or-thodontic brackets. J. Dent. Res. 2007, 86, 441–445. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, V.; Davidovitch, Z. Cellular, molecular, and tissue-level reactions to orthodontic force. Am. J. Orthod. Dentofac. Orthop. 2006, 129, 469.e1–469.e32. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Soares, S.C.; Roux, L.J.D.; Castro, A.R.; Silva, C.C.; Rodrigues, R.; Macho, V.M.P.; Silva, F.; Costa, C. Oral Manifestations: A Warning-Sign in Children with Hematological Disease Acute Lymphocytic Leukemia. Hematol. Rep. 2023, 15, 491-502. https://doi.org/10.3390/hematolrep15030051
Soares SC, Roux LJD, Castro AR, Silva CC, Rodrigues R, Macho VMP, Silva F, Costa C. Oral Manifestations: A Warning-Sign in Children with Hematological Disease Acute Lymphocytic Leukemia. Hematology Reports. 2023; 15(3):491-502. https://doi.org/10.3390/hematolrep15030051
Chicago/Turabian StyleSoares, Sandra Clara, Louis J. D. Roux, Ana Rita Castro, Cristina Cardoso Silva, Rita Rodrigues, Viviana M. P. Macho, Fátima Silva, and Céu Costa. 2023. "Oral Manifestations: A Warning-Sign in Children with Hematological Disease Acute Lymphocytic Leukemia" Hematology Reports 15, no. 3: 491-502. https://doi.org/10.3390/hematolrep15030051
APA StyleSoares, S. C., Roux, L. J. D., Castro, A. R., Silva, C. C., Rodrigues, R., Macho, V. M. P., Silva, F., & Costa, C. (2023). Oral Manifestations: A Warning-Sign in Children with Hematological Disease Acute Lymphocytic Leukemia. Hematology Reports, 15(3), 491-502. https://doi.org/10.3390/hematolrep15030051