
Embryo Cryopreservation in a Patient with Sickle Cell Disease Utilizing Letrozole and Enoxaparin: A Case Report

Abstract
1. Introduction
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Assouline, E.; Crocchiolo, R.; Prebet, T.; Broussais, F.; Coso, D.; Gamerre, M.; Vey, N.; Blaise, D.; Courbiere, B. Impact of reduced-intensity conditioning allogeneic stem cell transplantation on women’s fertility. Clin. Lymphoma Myeloma Leuk. 2013, 13, 704–710. [Google Scholar] [CrossRef] [PubMed]
- Ghafuri, D.L.; Stimpson, S.J.; Day, M.E.; James, A.; DeBaun, M.R.; Sharma, D. Fertility challenges for women with sickle cell disease. Expert Rev. Hematol. 2017, 10, 891–901. [Google Scholar] [CrossRef] [PubMed]
- Nickel, R.S.; Maher, J.Y.; Hsieh, M.H.; Davis, M.F.; Hsieh, M.M.; Pecker, L.H. Fertility after Curative Therapy for Sickle Cell Disease: A Comprehensive Review to Guide Care. J. Clin. Med. 2022, 11, 2318. [Google Scholar] [CrossRef] [PubMed]
- Boga, C.; Asma, S.; Ozer, C.; Bulgan Kilicdag, E.; Kozanoglu, I.; Yeral, M.; Korur, A.; Gereklioglu, C.; Ozdogu, H. Gonadal Status and Sexual Function at Long-Term Follow-up after Allogeneic Stem Cell Transplantation in Adult Patients with Sickle Cell Disease. Exp. Clin. Transplant. 2022. [Google Scholar] [CrossRef] [PubMed]
- Nikas, G.; Develioglu, O.H.; Toner, J.P.; Jones, H.W., Jr. Endometrial pinopodes indicate a shift in the window of receptivity in IVF cycles. Hum. Reprod. 1999, 14, 787–792. [Google Scholar] [CrossRef] [PubMed]
- Bonnar, J. Coagulation effects of oral contraception. Am. J. Obstet. Gynecol. 1987, 157, 1042–1048. [Google Scholar] [CrossRef] [PubMed]
- Pecker, L.H.; Maher, J.Y.; Law, J.Y.; Beach, M.C.; Lanzkron, S.; Christianson, M.S. Risks associated with fertility preservation for women with sickle cell anemia. Fertil. Steril. 2018, 110, 720–731. [Google Scholar] [CrossRef] [PubMed]
- Matthews, M.; Pollack, R. Acute pain crisis in a patient with sickle cell disease undergoing ovarian stimulation for fertility preservation prior to curative stem cell transplantation: Case report and literature review. J. Assist. Reprod. Genet. 2017, 34, 1445–1448. [Google Scholar] [CrossRef] [PubMed]
- Dovey, S.; Krishnamurti, L.; Sanfilippo, J.; Gunawardena, S.; McLendon, P.; Campbell, M.; Alway, S.; Efymow, B.; Gracia, C. Oocyte cryopreservation in a patient with sickle cell disease prior to hematopoietic stem cell transplantation: First report. J. Assist. Reprod. Genet. 2012, 29, 265–269. [Google Scholar] [CrossRef] [PubMed]
- Aserlind, A.; Martini, A.; Dong, J.; Zolton, J.; Carpinello, O.; DeCherney, A. Fertility preservation before hematopoetic stem cell transplantation: A case series of women with GATA binding protein 2 deficiency, dedicator of cytokinesis 8 deficiency, and sickle cell disease. FS Rep. 2020, 1, 287–293. [Google Scholar] [CrossRef]
- Cakmak, H.; Rosen, M.P. Ovarian stimulation in cancer patients. Fertil. Steril. 2013, 99, 1476–1484. [Google Scholar] [CrossRef] [PubMed]
- Reddy, J.; Oktay, K. Ovarian stimulation and fertility preservation with the use of aromatase inhibitors in women with breast cancer. Fertil. Steril. 2012, 98, 1363–1369. [Google Scholar] [CrossRef]
- Oktay, K.; Türkçüoğlu, I.; Rodriguez-Wallberg, K.A. GnRH agonist trigger for women with breast cancer undergoing fertility preservation by aromatase inhibitor/FSH stimulation. Reprod. Biomed. Online 2010, 20, 783–788. [Google Scholar] [CrossRef]
- Practice Committee of the American Society for Reproductive Medicine. Prevention and treatment of moderate and severe ovarian hyperstimulation syndrome: A guideline. Fertil. Steril. 2016, 106, 1634–1647. [Google Scholar] [CrossRef] [PubMed]
- Griffin, D.; Benadiva, C.; Kummer, N.; Budinetz, T.; Nulsen, J.; Engmann, L. Dual trigger of oocyte maturation with gonadotropin-releasing hormone agonist and low-dose human chorionic gonadotropin to optimize live birth rates in high responders. Fertil. Steril. 2012, 97, 1316–1320. [Google Scholar] [CrossRef] [PubMed]
- Heindryckx, B. Treatment option for sperm- or oocyte-related fertilization failure: Assisted oocyte activation following diagnostic heterologous ICSI. Hum. Reprod. 2005, 20, 2237–2241. [Google Scholar] [CrossRef] [PubMed]
- Haixia, J.; Xiaoxue, S.; Wenyan, S.; Yan, L.; Lin, Q.; Fuli, Z. Development of Nomograms to Predict Blastulation Rate Following Cycles of In Vitro Fertilization in Patients with Tubal Factor Infertility, Polycystic Ovary Syndrome, or Endometriosis. Front. Endocrinol. 2021, 12, 751373. [Google Scholar]
- Chadid, M.L.; Carpio, J.; Valdivieso, P.; Zambrano, M.; García-Ferreyra, J.; Valdivieso-Mejía, P. Percentage of Blastulation on the Number and Function of Metaphase II Oocytes. JBRA Assist. Reprod. 2015, 19, 111–113. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.Q.; Li, X.L.; Peng, Y.; Guo, X.; Heng, B.C.; Tong, G.Q. Reduction in exposure of human embryos outside the incubator enhances embryo quality and blastulation rate. Reprod. Biomed. Online. 2010, 20, 510–515. [Google Scholar] [CrossRef] [PubMed]



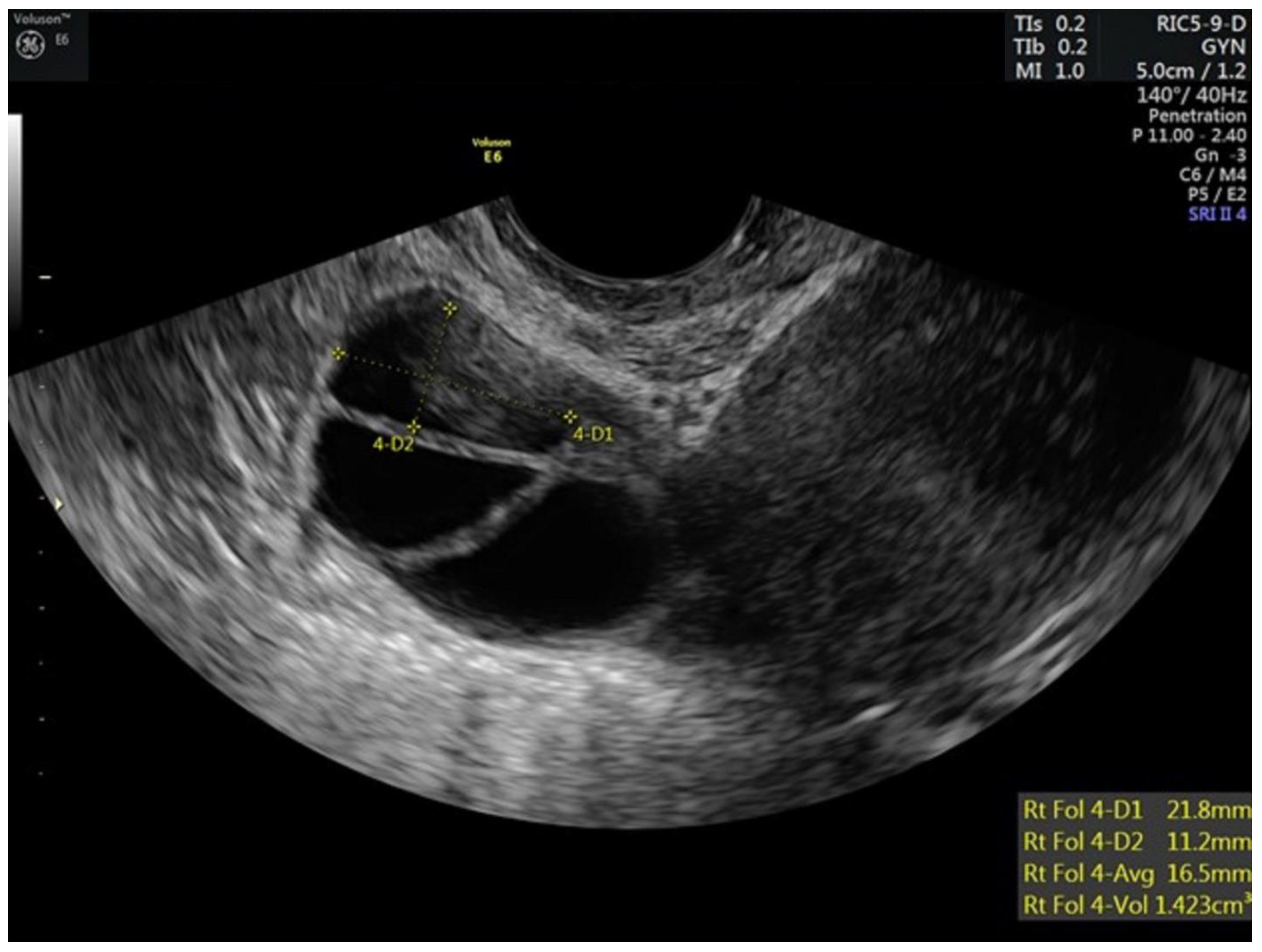{kind=link}
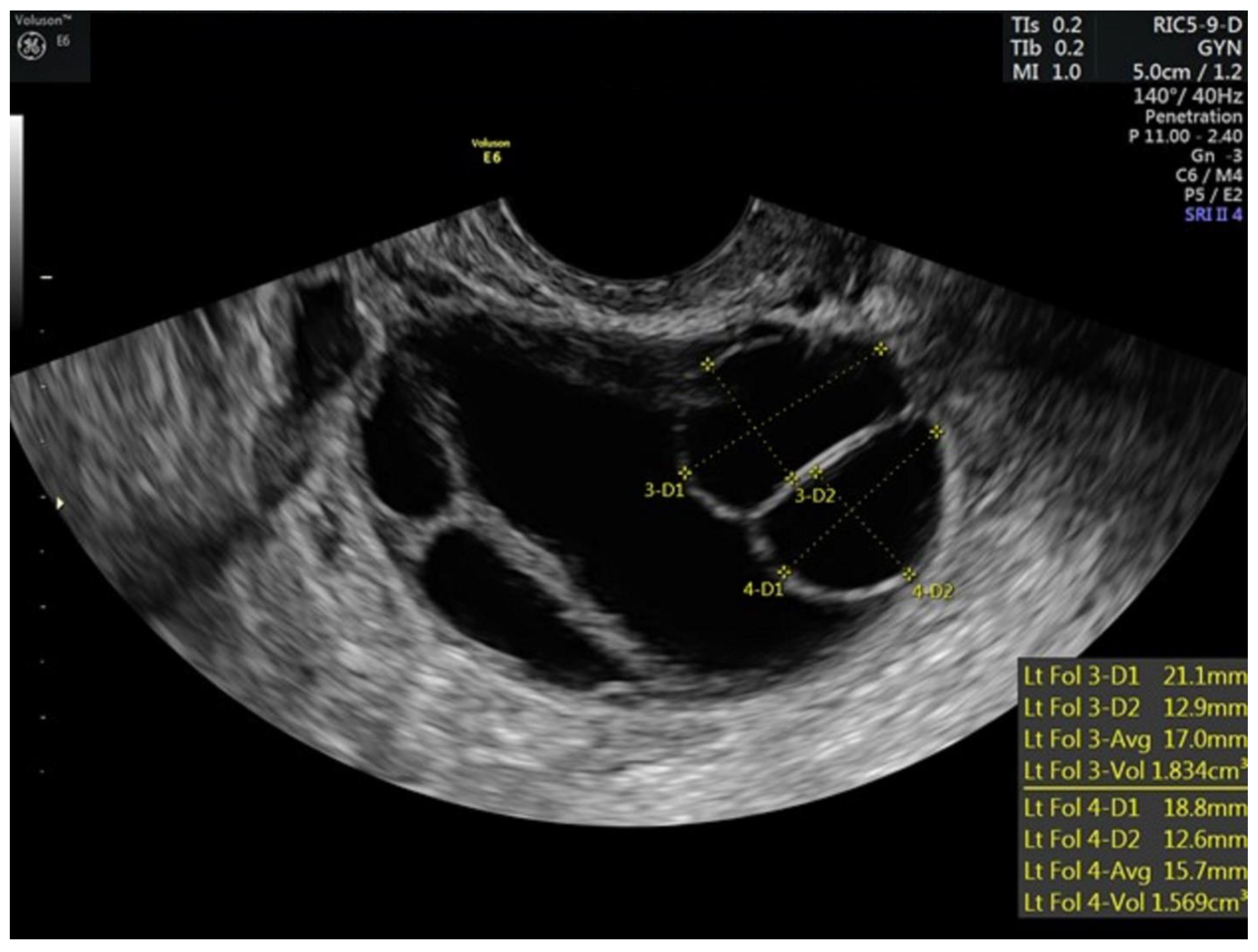{kind=link}
| Cycle Day | Medication Dosing | Serum Testing | Right Ovarian Follicles (mm) | Left Ovarian Follicles (mm) | Endometrial Thickness (mm) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Letrozole (mg) | Enoxaparin (mg) | rFSH (IU) | HMG (IU) | GnRH Antagonist (mcg) | GnRH Agonist(IU) | hCG(IU) | Estradiol (pg/dL) | LH (IU/L) | ||||
| 0 | 5 | |||||||||||
| 1–3 | 5 | 40 | 100 | 75 | 35.5 | 12 < 10 | 9 < 10 | 3.3 | ||||
| 4–6 | 5 | 40 | 100 | 75 | 74.1 | 7 < 10 | 9 < 10 | 4.1 | ||||
| 7 | 5 | 40 | 100 | 75 | 250 | 84 | 12,11,10,9,9,7 | 12,12,11,10,9,8 | 4.7 | |||
| 8–9 | 5 | 40 | 100 | 75 | 250 | 116 | 15,14,13,11,10,9 | 16,14,13,13,12,7 | 5.8 | |||
| 10 | 5 | 40 | 100 | 75 | 250 | 172 | 0.6 | 19,17,17,13,12,12,9,6 | 18,17,16,16,13,4 | 5.3 | ||
| 11 | 5 | 40 | 175 | 0 | 40 | 1500 | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gunderson, S.J.; Snowden, N.; Field, J.J. Embryo Cryopreservation in a Patient with Sickle Cell Disease Utilizing Letrozole and Enoxaparin: A Case Report. Hematol. Rep. 2023, 15, 101-107. https://doi.org/10.3390/hematolrep15010011
Gunderson SJ, Snowden N, Field JJ. Embryo Cryopreservation in a Patient with Sickle Cell Disease Utilizing Letrozole and Enoxaparin: A Case Report. Hematology Reports. 2023; 15(1):101-107. https://doi.org/10.3390/hematolrep15010011
Chicago/Turabian StyleGunderson, Stephanie J., Nina Snowden, and Joshua J. Field. 2023. "Embryo Cryopreservation in a Patient with Sickle Cell Disease Utilizing Letrozole and Enoxaparin: A Case Report" Hematology Reports 15, no. 1: 101-107. https://doi.org/10.3390/hematolrep15010011
APA StyleGunderson, S. J., Snowden, N., & Field, J. J. (2023). Embryo Cryopreservation in a Patient with Sickle Cell Disease Utilizing Letrozole and Enoxaparin: A Case Report. Hematology Reports, 15(1), 101-107. https://doi.org/10.3390/hematolrep15010011