
Influence of Oral Dipping Tombak Smokeless Tobacco on Coagulation Profile and Platelet Counts

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Data Collection
2.2. Inclusion and Exclusion Criteria
2.3. Ethical Consideration
2.4. Statistical Analysis
3. Results
3.1. Demographic Characteristics
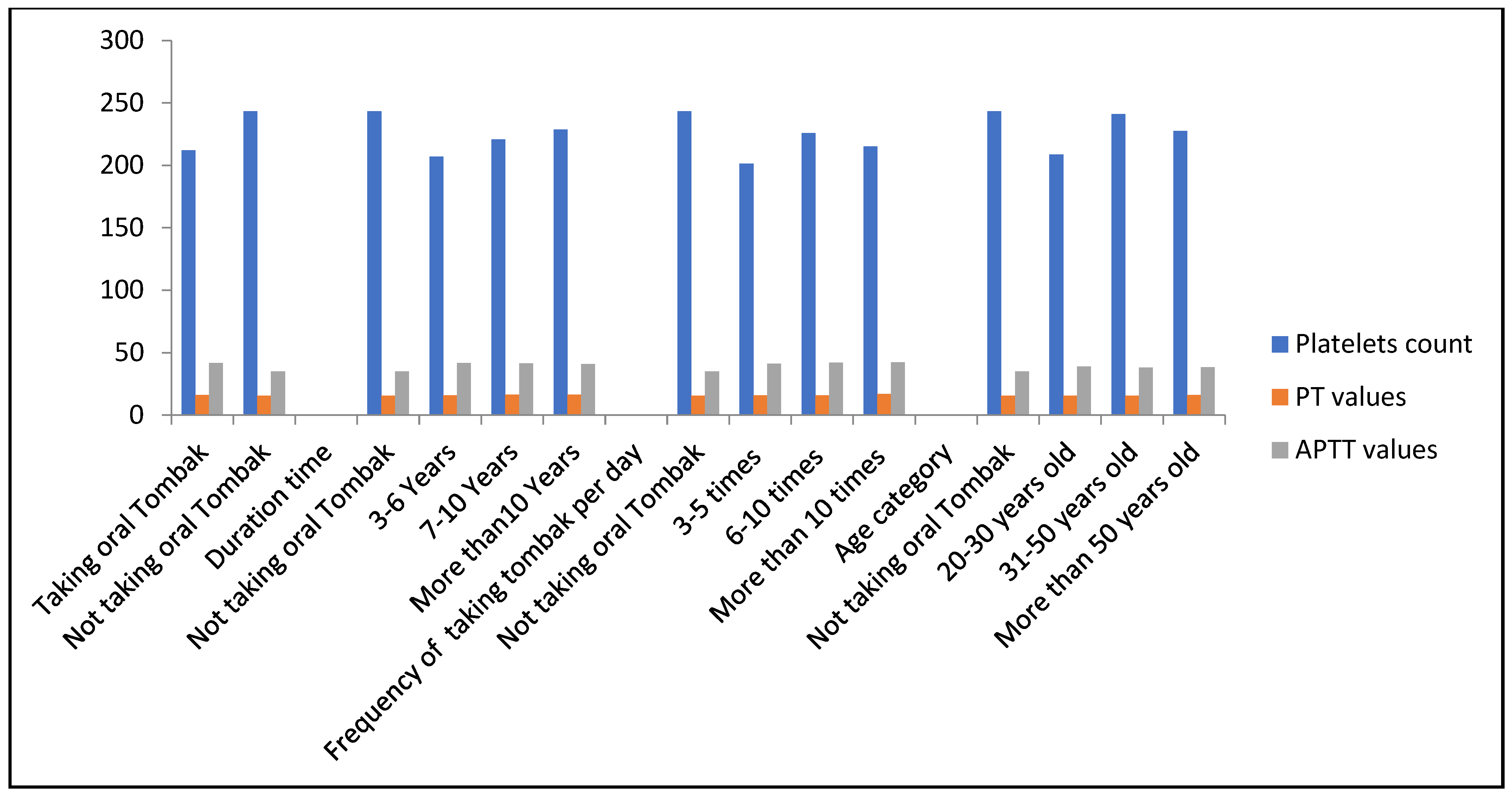
3.2. Effects of Taking Oral Tombak on Platelet Counts
3.3. Effects of Taking Oral Tombak on Prothrombin Time
3.4. Effects of Taking Oral Tombak on Activated Partial Thromboplastin Time
3.5. Effects of Taking Oral Tombak Based on International Normalised Ratio
3.6. Effects of Taking Oral Tombak on PT, APTT, INR, and PLTs (Multiple Linear Regression)
4. Discussion
5. Conclusions
6. Limitation of the Study
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mohammedi, F.; Hazari, M.A.H.; Khatoon, F.; Naeem, K.H.A.; Ali, S.I. Effect of nicotine on platelet function. MedPulse Int. J. Physiol. 2017, 5, 13–16. [Google Scholar] [CrossRef]
- World Health Organization. Report on Global Tobacco Epidemic; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Mohan, P.; Lando, H.A.; Panneer, S. Assessment of tobacco consumption and control in India. IndianJ. Clin. Med. 2018, 9, 1179916118759289. [Google Scholar] [CrossRef]
- National Cancer Institute; Centers for Disease Control and Prevention. Smokeless Tobacco and Public Health: A Global Perspective; NCI: Bethesda, MD, USA, 2014.
- WHO. WHO Report on the Global Tobacco Epidemic, 2017: Monitoring Tobacco Use and Prevention Policies; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Babiker, A.A.; Elhaj, A.; Mohamedahmed, K.A.; Ahmed, E.A. Assessment of Cytological Atypia, AgNOR Count and p53 Protein in Epithelial Oral Mucosa Exposed to Toombak Among Sudanese Snuffers. Assessment 2019, 3, 1–5. [Google Scholar]
- Almahdi, H.M.; Åstrøm, A.N.; Ali, R.W.; Nasir, E.F. School workers’ knowledge, attitude and behaviour related to use of Toombak: A cross sectional study from Khartoum state, Sudan. BMC Oral Health 2017, 17, 160. [Google Scholar] [CrossRef]
- El-Amin, S.E.-T.; Nwaru, B.I.; Ginawi, I.; Pisani, P.; Hakama, M. The role of parents, friends and teachers in adolescents’ cigarette smoking and tombak dipping in Sudan. Tob. Control 2011, 20, 94–99. [Google Scholar] [CrossRef]
- Idris, A.M.; Ibrahim, Y.E.; Warnakulasuriya, K.; Cooper, D.J.; Johnson, N.W.; Nilsen, R. Toombak use and cigarette smoking in the Sudan: Estimates of prevalence in the Nile state. Prev. Med. 1998, 27, 597–603. [Google Scholar] [CrossRef][Green Version]
- Idris, A.M.; Ibrahim, S.O.; Vasstrand, E.N.; Johannessen, A.; Lillehaug, J.; Magnusson, B.; Wallström, M.; Hirsch, J.-M.; Nilsen, R. The Swedish snus and the Sudanese toombak: Are they different? Oral Oncol. 1998, 34, 558–566. [Google Scholar] [CrossRef]
- Costea, D.E.; Lukandu, O.; Bui, L.; Ibrahim, M.J.M.; Lygre, R.; Neppelberg, E.; Ibrahim, S.O.; Vintermyr, O.K.; Johannessen, A.C. Adverse effects of Sudanese toombak vs. Swedish snuff on human oral cells. J. Oral Pathol. Med. 2010, 39, 128–140. [Google Scholar]
- Anand, P.S.; Kamath, K.P.; Shekar, B.R.; Anil, S. Relationship of Smoking and Smokeless Tobacco Use to Tooth Loss in a Central Indian Population. Oral Health Prev. Dent. 2012, 10, 243. [Google Scholar]
- Sinha, D.N.; Abdulkader, R.S.; Gupta, P.C. Smokeless tobacco-associated cancers: A systematic review and meta-analysis of I ndian studies. Int. J. Cancer 2016, 138, 1368–1379. [Google Scholar] [CrossRef]
- Ahmed, H.G. Aetiology of oral cancer in the Sudan. J. Oral Maxillofac. Res. 2013, 4, e3. [Google Scholar] [CrossRef]
- Osman, T.A.; Satti, A.A.; Bøe, O.E.; Yang, Y.-H.; Ibrahim, S.O.; Suleiman, A.M. Pattern of malignant tumors registered at a referral oral and maxillofacial hospital in Sudan during 2006 and 2007. J. Cancer Res. Ther. 2010, 6, 473. [Google Scholar] [CrossRef] [PubMed]
- Pednekar, M.S.; Gupta, P.C.; Yeole, B.B.; Hébert, J.R. Association of tobacco habits, including bidi smoking, with overall and site-specific cancer incidence: Results from the Mumbai cohort study. Cancer Causes Control 2011, 22, 859–868. [Google Scholar] [CrossRef] [PubMed]
- IARC Working Group on the Evaluation of Carcinogenic Risks to Humans. A Review of Human Carcinogens: Personal Habits and Indoor Combustions; World Health Organization: Geneva, Switzerland, 2012; Volume 100. [Google Scholar]
- Bijlani, R.L.; Manjunatha, S. Understanding Medical Physiology: A Textbook for Medical Students; Jaypee Brothers Publishers: New Delhi, India, 2010. [Google Scholar]
- Kerr, R.; Newsome, P.; Germain, L.; Thomson, E.; Dawson, P.; Stirling, D.; Ludlam, C.A. Effects of acute liver injury on blood coagulation. J. Thromb. Haemost. 2003, 1, 754–759. [Google Scholar] [CrossRef]
- Peyvandi, F.; Haertel, S.; Knaub, S.; Mannucci, P.M. Incidence of bleeding symptoms in 100 patients with inherited afibrinogenemia or hypofibrinogenemia. J. Thromb. Haemost. 2006, 4, 1634–1637. [Google Scholar] [CrossRef] [PubMed]
- Elkhalifa, A.M. Effects of cigarette smoking on coagulation screening tests and platelet counts in a Sudanese male adults population. Saudi Med. J. 2018, 39, 897. [Google Scholar] [CrossRef] [PubMed]
- Kumar, D.; Binawara, B.K.; Beniwal, P.; Sharma, P. Effect of chewing tobacco on hematological parameters in Bikaner city population. J. Med. Sci. Clin. Res. 2017, 5, 17721–17727. [Google Scholar] [CrossRef]
- Csordas, A.; Bernhard, D. The biology behind the atherothrombotic effects of cigarette smoke. Nat. Rev. Cardiol. 2013, 10, 219. [Google Scholar] [CrossRef]
- Oaikhena, G.A.; Nwaopara, A.O.; Ugbor, C.; Obami, K.; Uzor, P.U.; Imhoudu, T.; Blackies, H.O.T. The effect of tobacco snuff on blood coagulation parameters in adult Wistar rats. Int. J. Herbs Pharmacol. Res. 2015, 4, 40–45. [Google Scholar]
- Sandhya, M.; Satyanarayana, U.; Mohanty, S.; Basalingappa, D.R. Impact of chronic cigarette smoking on platelet aggregation and coagulation profile in apparently healthy male smokers. Int. J. Clin. Exp. Physiol. 2015, 2, 128–133. [Google Scholar]
- Al-Dahr, M.H.S. Impact of smoking on platelet, coagulation and lipid profile in young male subjects. World Appl. Sci. J. 2010, 11, 118–123. [Google Scholar]
- Akpotuzor, J.O.; Agwunobi, L.E.; Inyama, M.A. Prothrombin time (Pt) and partial thromboplastin time with kaolin (Pttk) of cigarette smokers in Calabar, Cross-river State, Nigeria. Adv. Med. Dent. Sci. 2001, 3, 17–20. [Google Scholar]
- Nascetti, S.; Elosua, R.; Pena, A.; Covas, M.I.; Sentí, M.; Marrugat, J. Variables associated with fibrinogen in a population-based study: Interaction between smoking and age on fibrinogen concentration. Eur. J. Epidemiol. 2001, 17, 953–958. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Independent Variables | n | Mean | SD | t/F | p-Value |
|---|---|---|---|---|---|
| Taking oral Tombak | 100 | 212.1 × 103/mm3 | 74.3 × 103/mm3 | −2.789 | 0.0006 * |
| Not taking oral Tombak | 100 | 243.2 × 103/mm3 | 83.0 × 103/mm3 | ||
| Duration time | |||||
| Not taking oral Tombak | 100 | 243.2 × 103/mm3 | 83.0 × 103/mm3 | −2.87 | 0.037 * |
| 3–6 Years | 66 | 206.9 × 103/mm3 | 85.6 × 103/mm3 | ||
| 7–10 Years | 28 | 220.8 × 103/mm3 | 44.6 × 103/mm3 | ||
| More than 10 Years | 6 | 228.6 × 103/mm3 | 46.8 × 103/mm3 | ||
| Frequency of taking Tombak per day | |||||
| Not taking oral Tombak | 100 | 243.2 × 103/mm3 | 83.0 × 103/mm3 | −3.23 | 0.023 * |
| 3–5 times | 48 | 201.4 × 103/mm3 | 97.1 × 103/mm3 | ||
| 6–10 times | 33 | 225.9 × 103/mm3 | 44.5 × 103/mm3 | ||
| More than 10 times | 19 | 215.1 × 103/mm3 | 39.6 × 103/mm3 | ||
| Age category | |||||
| Not taking oral Tombak | 100 | 243.2 × 103/mm3 | 83.0 × 103/mm3 | ||
| 20–30 years old | 64 | 208.7 × 103/mm3 | 115.3 × 103/mm3 | −3.12 | 0.046 * |
| 31–50 years old | 92 | 240.9 × 103/mm3 | 60.4 × 103/mm3 | ||
| More than 50 years old | 44 | 227.5 × 103/mm3 | 39.5 × 103/mm3 |
| Independent Variables | n | Mean | SD | t/F | p-Value |
|---|---|---|---|---|---|
| Taking oral Tombak | 100 | 16.03 s | 1.22 s | 4.38 | <0.001 * |
| Not taking oral Tombak | 100 | 15.44 s | 0.557 s | ||
| Duration time | |||||
| Not taking oral Tombak | 100 | 15.44 s | 0.557 s | 11.05 | <0.001 * |
| 3–6 Years | 66 | 15.79 s | 1.12 s | ||
| 3–7–10 Years | 28 | 16.50 s | 1.24 s | ||
| More than 10 Years | 6 | 16.41 s | 1.57 s | ||
| Frequency of taking Tombak per day | |||||
| Not taking oral Tombak | 100 | 15.44 s | 0.557 s | 15.03 | <0.001 * |
| 3–5 times | 48 | 15.83 s | 1.06 s | ||
| 6–10 times | 33 | 15.79 s | 1.19 s | ||
| More than 10 times | 19 | 16.93 s | 1.28 s | ||
| Age category | |||||
| Not taking oral Tombak | 100 | 15.44 s | 0.557 s | ||
| 20–30 years old | 64 | 15.60 s | 0.911 s | 5.02 | 0.007 * |
| 31–50 years old | 92 | 15.62 s | 0.927 s | ||
| More than 50 years old | 44 | 16.14 s | 1.14 s |
| Independent Variables | n | Mean | SD | t/F | p-Value |
|---|---|---|---|---|---|
| Taking oral Tombak | 100 | 41.62 s | 7.28 s | 7.96 | <0.001 * |
| Not taking oral Tombak | 100 | 34.99 s | 4.02 s | ||
| Duration time | |||||
| Not taking oral Tombak | 100 | 34.99 s | 4.02 s | 21.02 | <0.001 * |
| 3–6 Years | 66 | 41.75 s | 7.24 s | ||
| 7–10 Years | 28 | 41.51 s | 7.80 s | ||
| More than 10 years | 6 | 40.78 s | 6.13 s | ||
| Frequency of taking Tombak per day | |||||
| Not taking oral Tombak | 100 | 34.99 s | 4.02 s | 21.18 | <0.001 * |
| 3–5 times | 48 | 41.18 s | 6.97 s | ||
| 6–10 times | 33 | 41.96 s | 7.55 s | ||
| More than 10 times | 19 | 42.15 s | 7.88 s | ||
| Age category | |||||
| Not taking oral Tombak | 100 | 34.99 s | 4.02 s | 0.241 | 0.786 |
| 20–30 years old | 64 | 38.77 s | 6.64 s | ||
| 31–50 years old | 92 | 38.01 s | 6.78 s | ||
| More than 50 years old | 44 | 38.25 s | 6.91 s |
| Independent Variables | n | Mean | SD | t/F | p-Value |
|---|---|---|---|---|---|
| Taking oral Tombak | 100 | 1.11 | 0.096 | 3.59 | <0.001 * |
| Not taking oral Tombak | 100 | 1.07 | 0.066 | ||
| Duration time | |||||
| Not taking oral Tombak | 100 | 1.07 | 0.066 | 8.68 | <0.001 * |
| 3–6 Years | 66 | 1.09 | 0.077 | ||
| 7–10 Years | 28 | 1.15 | 0.120 | ||
| More than 10 Years | 6 | 1.14 | 0.108 | ||
| Frequency of taking Tombak per day | |||||
| Not taking oral Tombak | 100 | 1.07 | 0.066 | 12.5 | <0.001 * |
| 3–5 times | 48 | 1.09 | 0.076 | ||
| 6–10 times | 33 | 1.09 | 0.077 | ||
| More than 10 times | 19 | 1.19 | 0.130 | ||
| Age category | |||||
| Not taking oral Tombak | 100 | 1.07 | 0.066 | 4.03 | 0.019 * |
| 20–30 years old | 64 | 1.0806 | 0.06700 | ||
| 31–50 years old | 92 | 1.0863 | 0.08291 | ||
| More than 50 years old | 44 | 1.1243 | 0.10606 |
| Variable | B | T/F | p-Value * | p-Value ** |
|---|---|---|---|---|
| Platelet | 2.77 | 0.043 * | ||
| (Constant) | 206.45 | 13.01 | <0.001 * | |
| Age (category) | 17.73 | 2.165 | 0.032 * | 0.144 |
| Duration time of taking Tombak | −3.908 | −0.188 | 0.851 | 0.061 |
| Frequency of taking Tombak | −11.37 | −0.664 | 0.507 | 0.068 |
| PT | 11.66 | <0.001 * | ||
| (Constant) | 15.25 | 82.47 | <0.001 * | |
| Age (category) | 0.090 | 0.941 | 0.348 | 0.010 ** |
| Duration time of taking Tombak | 0.064 | 0.265 | 0.791 | <0.001 ** |
| Frequency of taking Tombak | 0.306 | 1.531 | 0.127 | <0.001 ** |
| APTT | 19.45 | <0.001 * | ||
| (Constant) | 39.04 | 32.61 | <0.001 * | |
| Age (category) | −1.87 | −3.034 | 0.003 * | 0.641 |
| Duration time of taking Tombak | −0.985 | −0.628 | 0.530 | <0.001 ** |
| Frequency of taking Tombak | 4.11 | 3.182 | 0.002 * | <0.001 ** |
| INR | 8.89 | <0.001 * | ||
| (Constant) | 1.05 | 65.09 | <0.001 * | |
| Age (category) | 0.009 | 1.03 | 0.305 | 0.013 ** |
| Duration time of taking Tombak | 0.004 | 0.200 | 0.842 | <0.001 ** |
| Frequency of taking Tombak | 0.023 | 1.33 | 0.185 | <0.001 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Elkhalifa, A.M.E.; Ali, N.Y.; Tamomh, A.G.; Tabash, M.I.; Mustafa, E.T.A.; Mohammed, Z.A.K.; Ahamed, N.A.S. Influence of Oral Dipping Tombak Smokeless Tobacco on Coagulation Profile and Platelet Counts. Hematol. Rep. 2022, 14, 126-134. https://doi.org/10.3390/hematolrep14020019
Elkhalifa AME, Ali NY, Tamomh AG, Tabash MI, Mustafa ETA, Mohammed ZAK, Ahamed NAS. Influence of Oral Dipping Tombak Smokeless Tobacco on Coagulation Profile and Platelet Counts. Hematology Reports. 2022; 14(2):126-134. https://doi.org/10.3390/hematolrep14020019
Chicago/Turabian StyleElkhalifa, Ahmed M. E., Nada Y. Ali, Abdelhakam G. Tamomh, Mohammed I. Tabash, Esraa T. A. Mustafa, Zenieb A. K. Mohammed, and Nedal A. S. Ahamed. 2022. "Influence of Oral Dipping Tombak Smokeless Tobacco on Coagulation Profile and Platelet Counts" Hematology Reports 14, no. 2: 126-134. https://doi.org/10.3390/hematolrep14020019
APA StyleElkhalifa, A. M. E., Ali, N. Y., Tamomh, A. G., Tabash, M. I., Mustafa, E. T. A., Mohammed, Z. A. K., & Ahamed, N. A. S. (2022). Influence of Oral Dipping Tombak Smokeless Tobacco on Coagulation Profile and Platelet Counts. Hematology Reports, 14(2), 126-134. https://doi.org/10.3390/hematolrep14020019