
Diagnostic Significance of Absence of Post-Feeding Contraction of the Gallbladder in Biliary Atresia: Two Case Reports

 , and
, and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Cases
2.1. Case 1: 4-Day-Old Boy
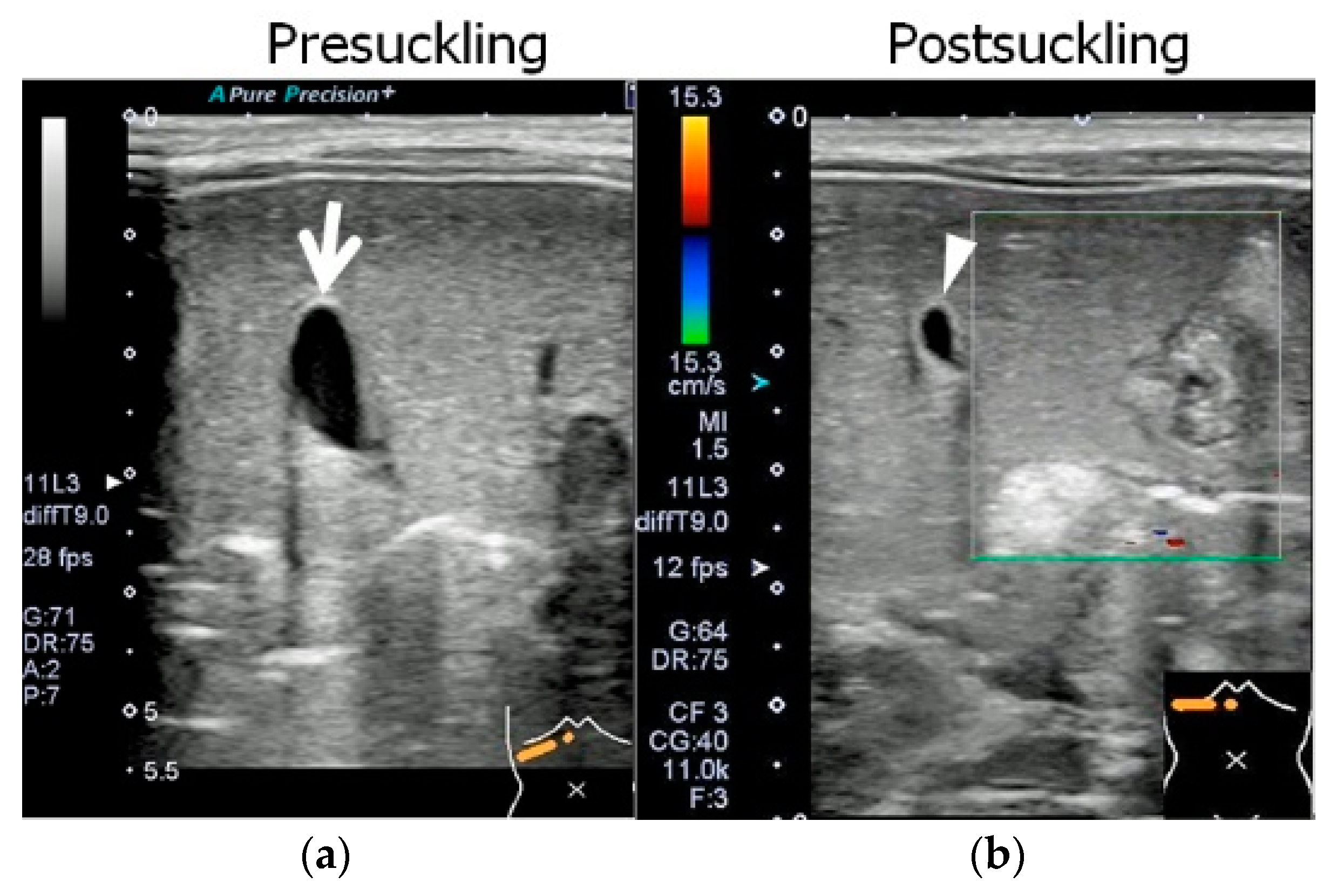
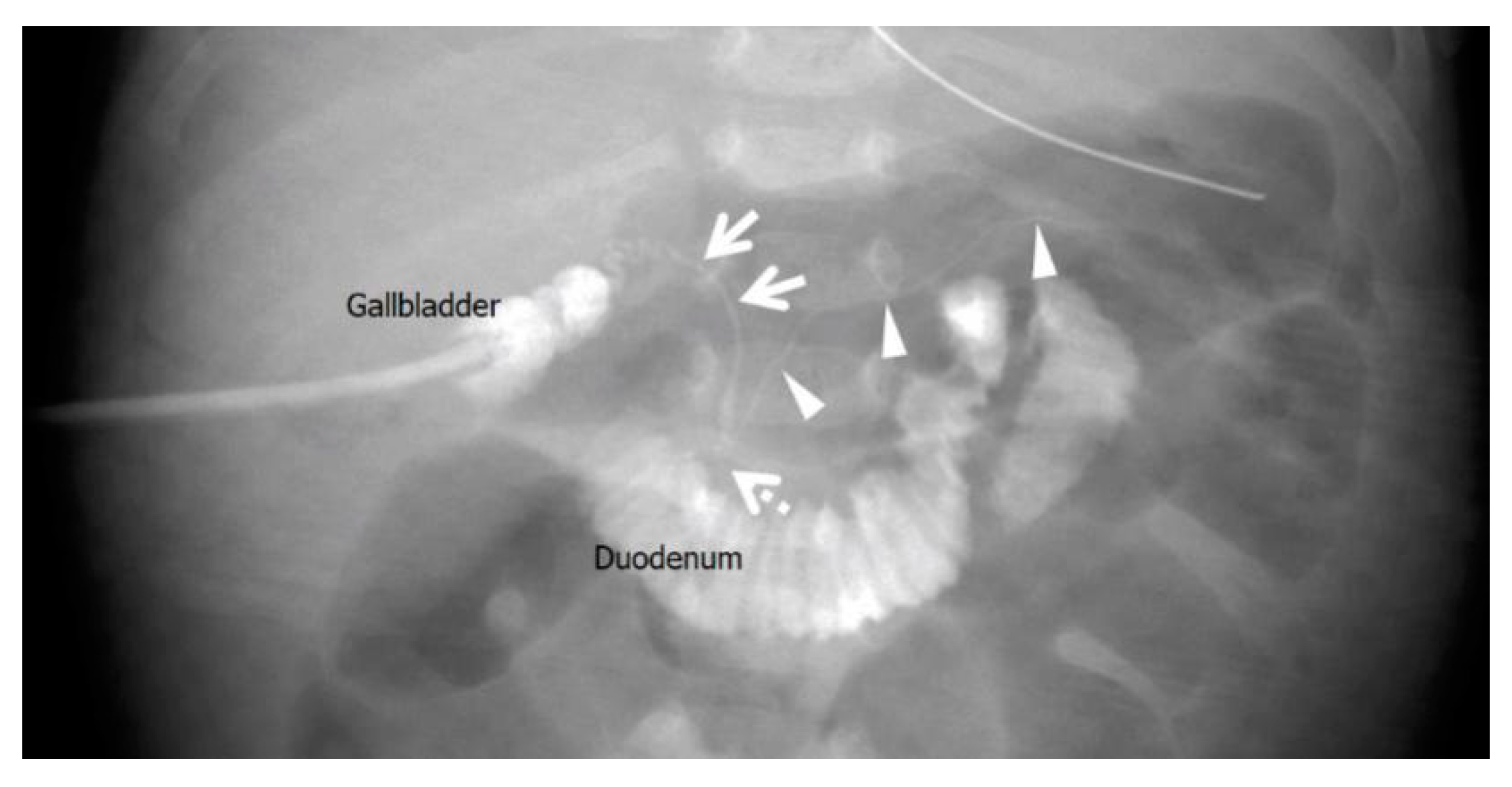
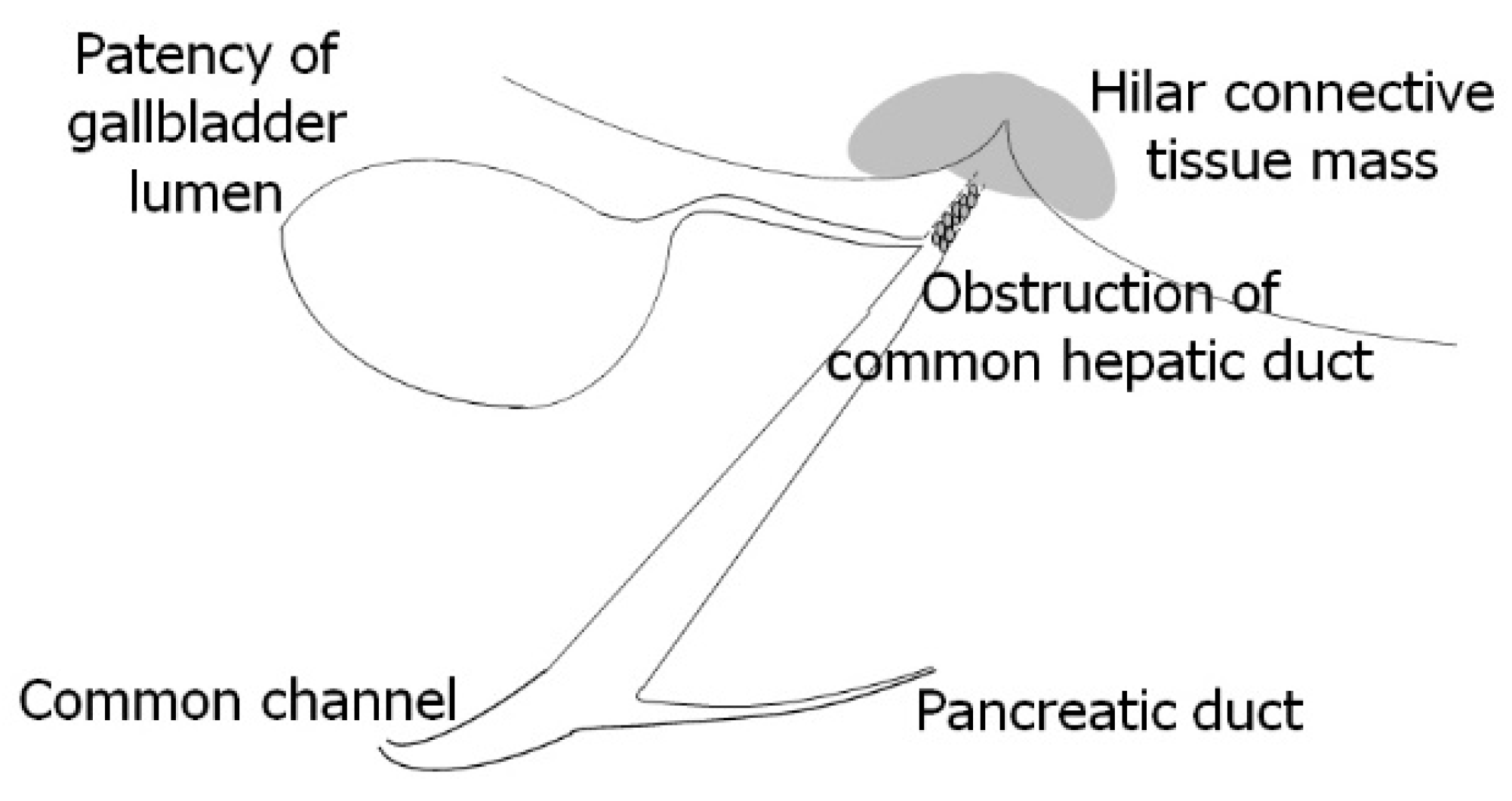
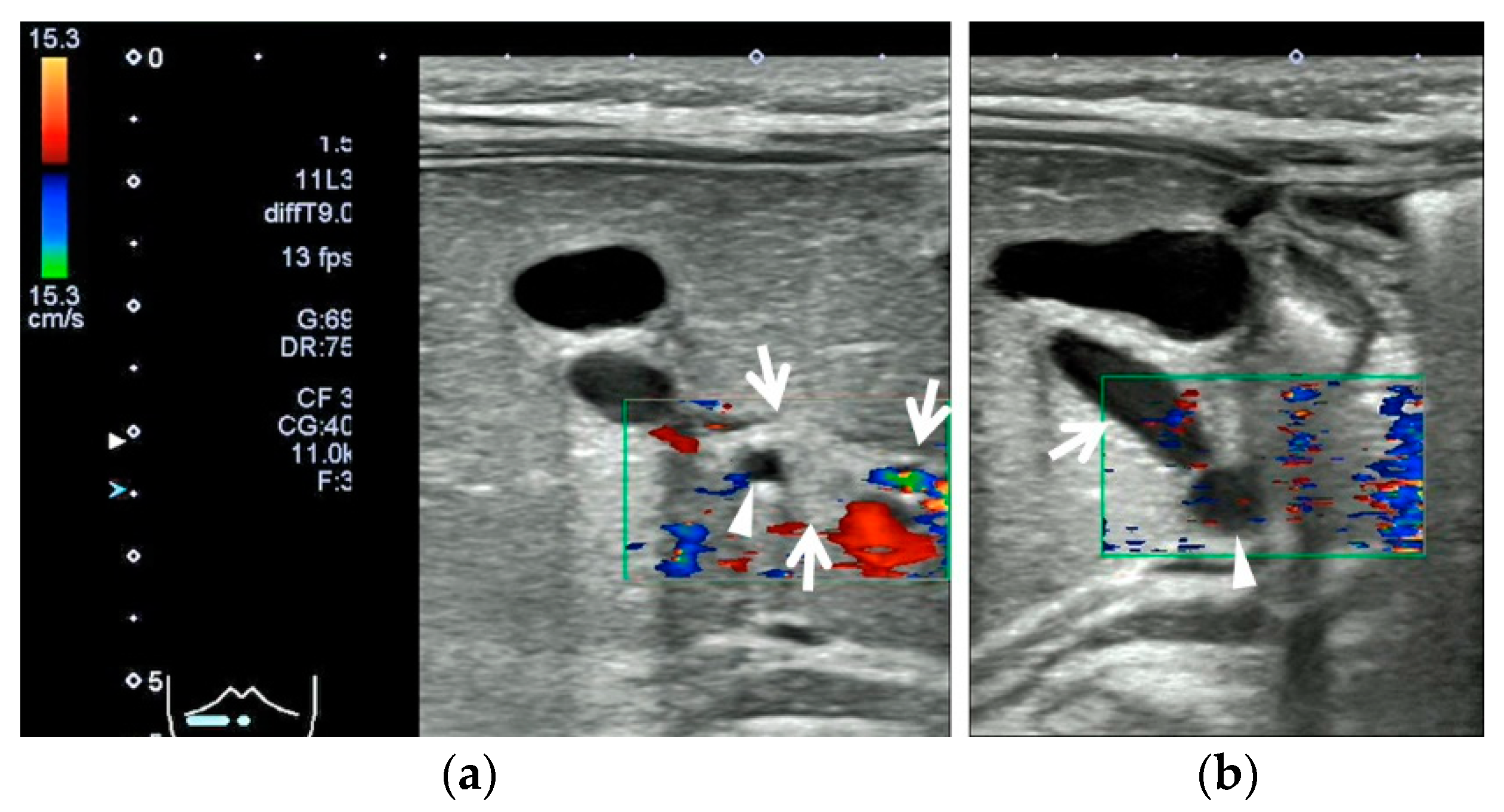
2.2. Case 2: 67-Day-Old Girl
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yoon, H.; Lim, H.J.; Kim, J.; Lee, M.-J. Diagnostic Imaging of Biliary Atresia. J. Korean Soc. Radiol. 2022, 83, 991–1002. [Google Scholar] [CrossRef] [PubMed]
- Napolitano, M.; Franchi-Abella, S.; Damasio, M.B.; Augdal, T.A.; Avni, F.E.; Bruno, C.; Darge, K.; Ključevšek, D.; Littooij, A.S.; Lobo, L.; et al. Practical approach to imaging diagnosis of biliary atresia, Part 1: Prenatal ultrasound and magnetic resonance imaging, and postnatal ultrasound. Pediatr. Radiol. 2021, 51, 314–331. [Google Scholar] [CrossRef] [PubMed]
- Zhou, W.; Zhou, L. Ultrasound for the Diagnosis of Biliary Atresia: From Conventional Ultrasound to Artificial Intelligence. Diagnostics 2021, 12, 51. [Google Scholar] [CrossRef] [PubMed]
- Endo, K.; Yokoi, A.; Mishima, Y.; Tamaki, A.; Morita, K.; Okata, Y.; Hisamatsu, C.; Fukuzawa, H.; Yoshida, M.; Akasaka, Y.; et al. A case of biliary atresia with pancreaticobiliary maljunction. Surg. Case Rep. 2017, 3, 100. [Google Scholar] [CrossRef] [PubMed]
- Superina, R.; Magee, J.C.; Brandt, M.L.; Healey, P.J.; Tiao, G.; Ryckman, F.; Karrer, F.M.; Iyer, K.; Fecteau, A.; West, F.; et al. The anatomic pattern of biliary atresia identified at time of Kasai hepatoportoenterostomy and early postoperative clearance of jaundice are significant preditors of transplant-free survival. Ann. Surg. 2011, 254, 577–585. [Google Scholar] [CrossRef] [PubMed]
- Brahee, D.D.; Lampl, B.S. Neonatal diagnosis of biliary atresia: A practical review and update. Pediatr. Radiol. 2022, 52, 685–692. [Google Scholar] [CrossRef] [PubMed]
- Deguchi, E.; Iwai, N.; Kimura, O.; Ono, S.; Shimadera, S.; Fumino, S. Significance of the Anomalous Arrangement of the Pancreaticobiliary Duct in the Etiology of Biliary Atresia. Eur. J. Pediatr. Surg. 2007, 17, 96–99. [Google Scholar] [CrossRef] [PubMed]
- Bezerra, J.A.; Wells, R.G.; Mack, C.L.; Karpen, S.J.; Hoofnagle, J.H.; Doo, E.; Sokol, R.J. Biliary Atresia: Clinical and Research Challenges for the Twenty-First Century. Hepatology 2018, 68, 1163–1173. [Google Scholar] [CrossRef] [PubMed]
- dos Santos, J.L.; Quelhas, P.; Cerski, C. Update on etiology and pathogenesis of biliary atresia. Curr. Pediatr. Rev. 2022, 19, 48–67. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kosuga, M.; Fujii, Y.; Doi, T.; Kaneko, K.; Breugelmans, R. Diagnostic Significance of Absence of Post-Feeding Contraction of the Gallbladder in Biliary Atresia: Two Case Reports. Pediatr. Rep. 2023, 15, 541-547. https://doi.org/10.3390/pediatric15030049
Kosuga M, Fujii Y, Doi T, Kaneko K, Breugelmans R. Diagnostic Significance of Absence of Post-Feeding Contraction of the Gallbladder in Biliary Atresia: Two Case Reports. Pediatric Reports. 2023; 15(3):541-547. https://doi.org/10.3390/pediatric15030049
Chicago/Turabian StyleKosuga, Masahiko, Yoshimitsu Fujii, Takashi Doi, Kazunari Kaneko, and Raoul Breugelmans. 2023. "Diagnostic Significance of Absence of Post-Feeding Contraction of the Gallbladder in Biliary Atresia: Two Case Reports" Pediatric Reports 15, no. 3: 541-547. https://doi.org/10.3390/pediatric15030049
APA StyleKosuga, M., Fujii, Y., Doi, T., Kaneko, K., & Breugelmans, R. (2023). Diagnostic Significance of Absence of Post-Feeding Contraction of the Gallbladder in Biliary Atresia: Two Case Reports. Pediatric Reports, 15(3), 541-547. https://doi.org/10.3390/pediatric15030049