
Myopericarditis in a Male Adolescent Following the Second Shot of COVID-19 Pfizer m-RNA Vaccine: Typical Example and Analysis of 110 Single Case Reports


Abstract
:1. Introduction
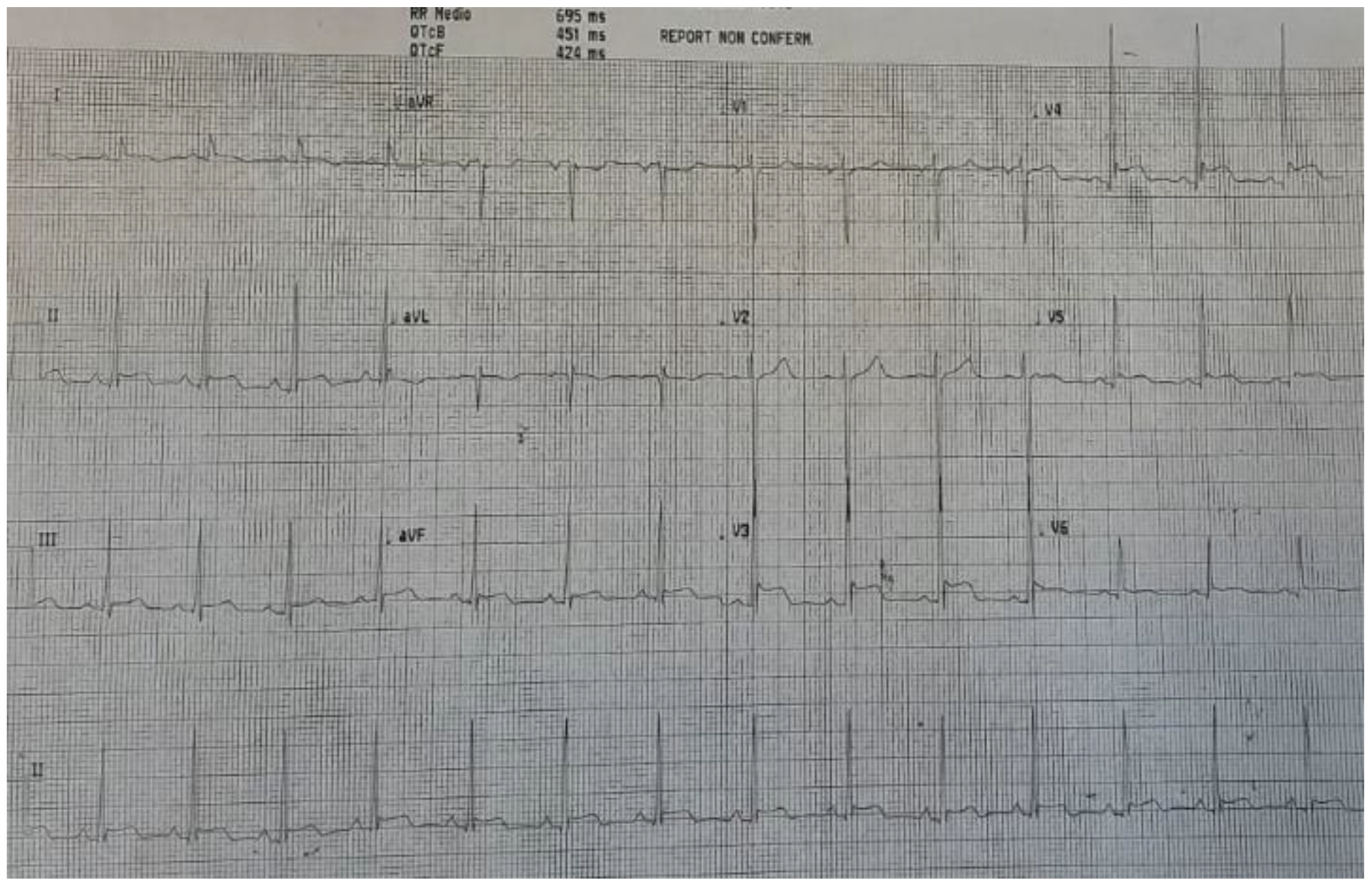
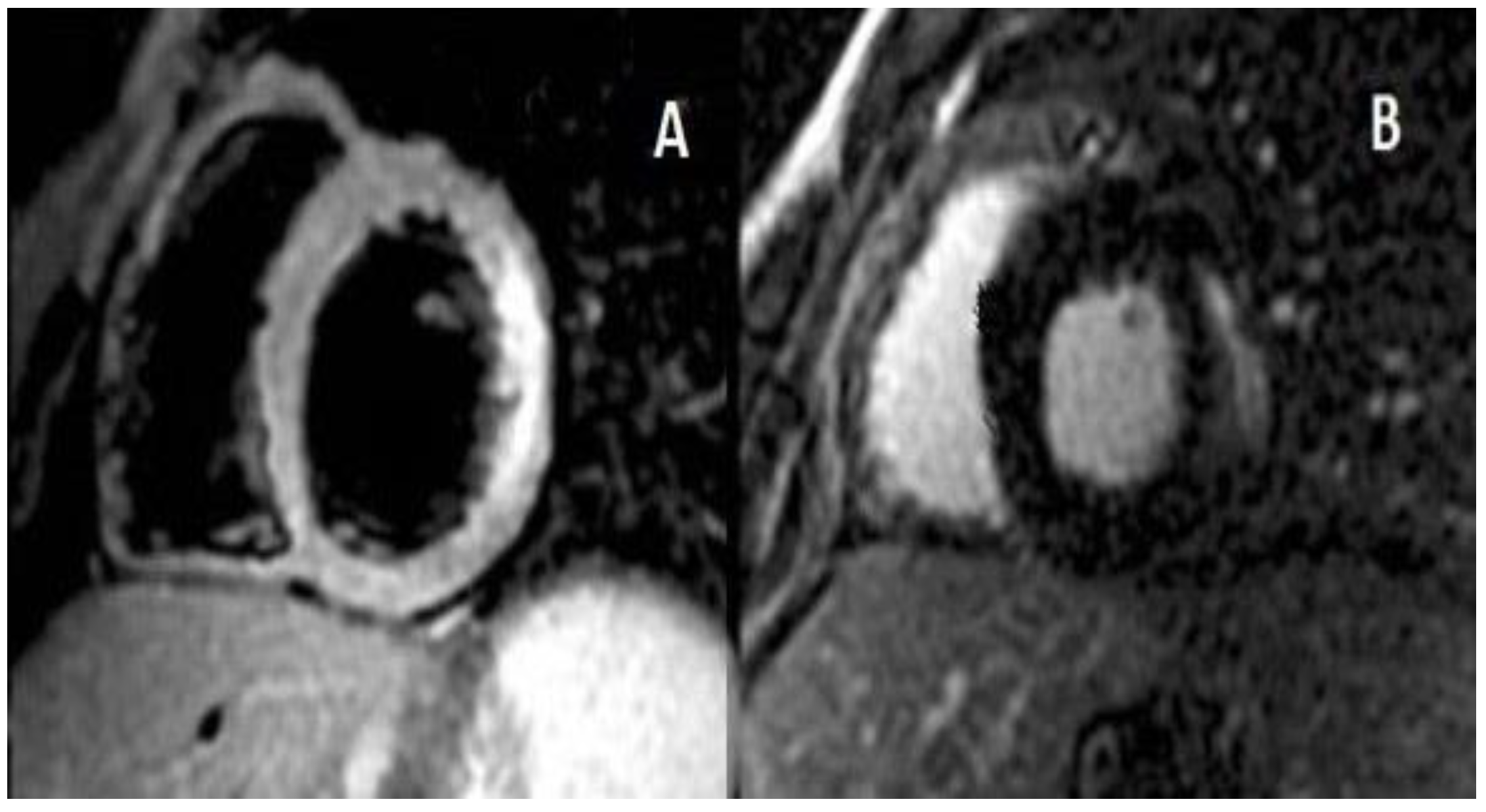
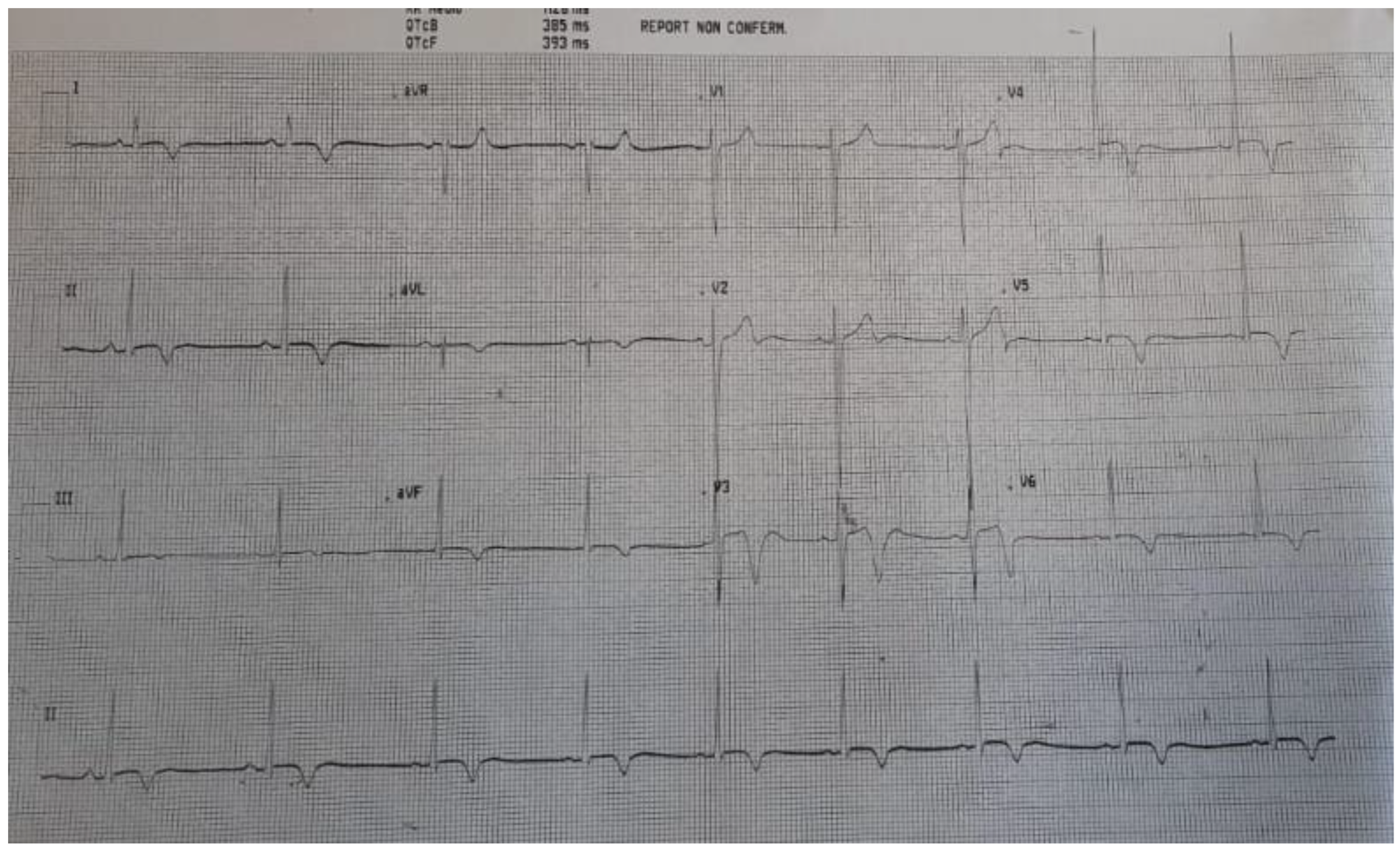
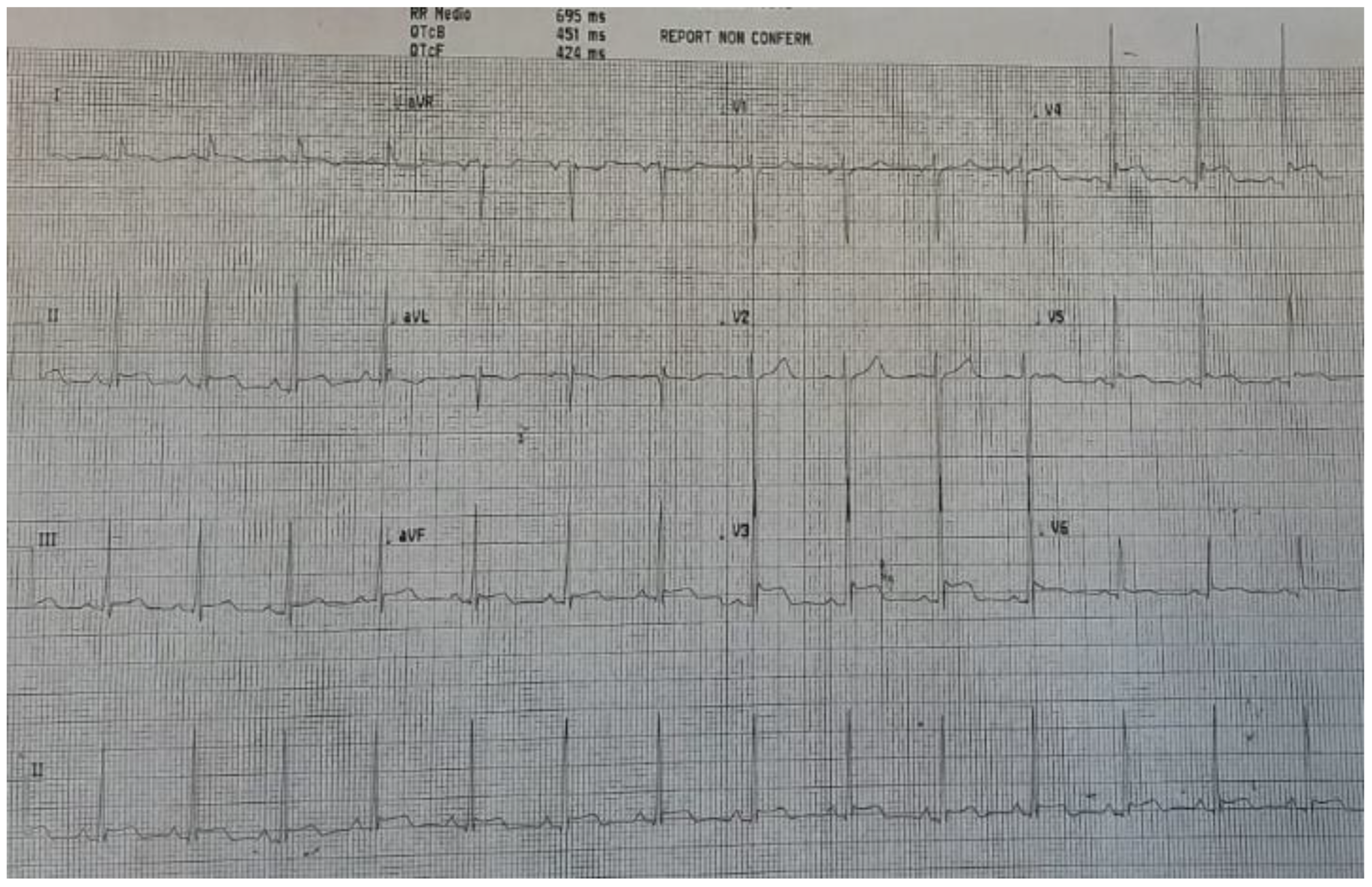
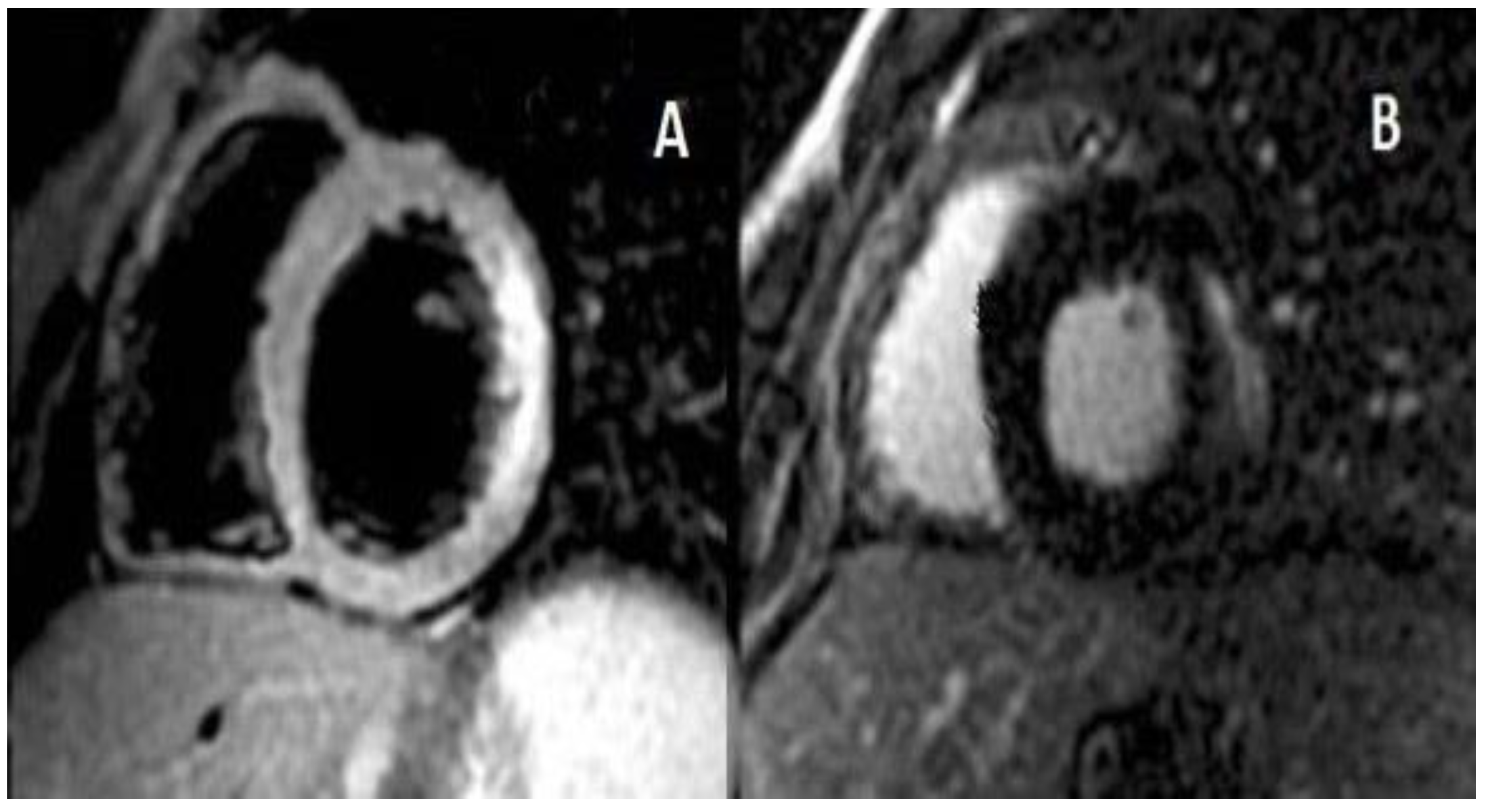
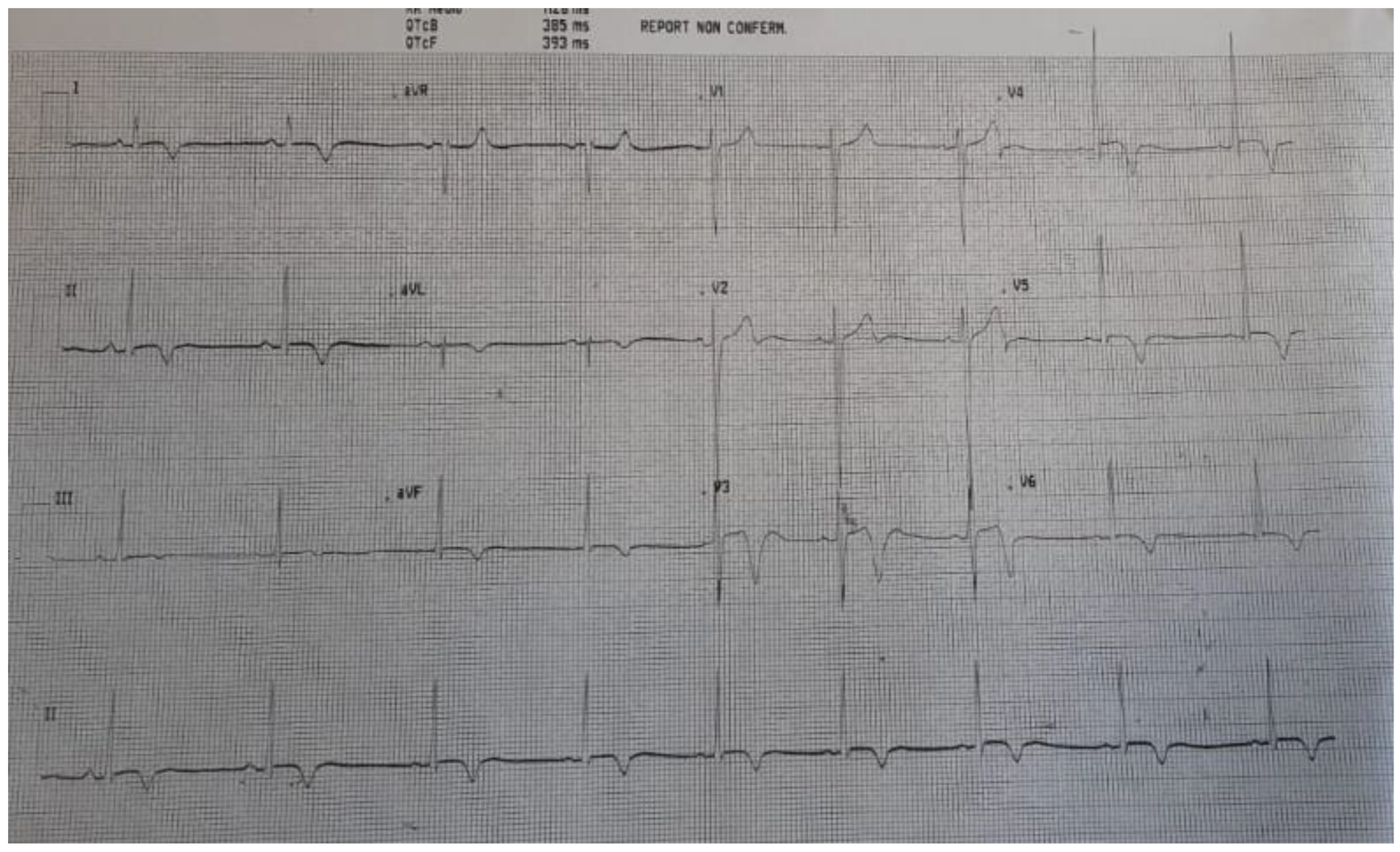
2. Case Report
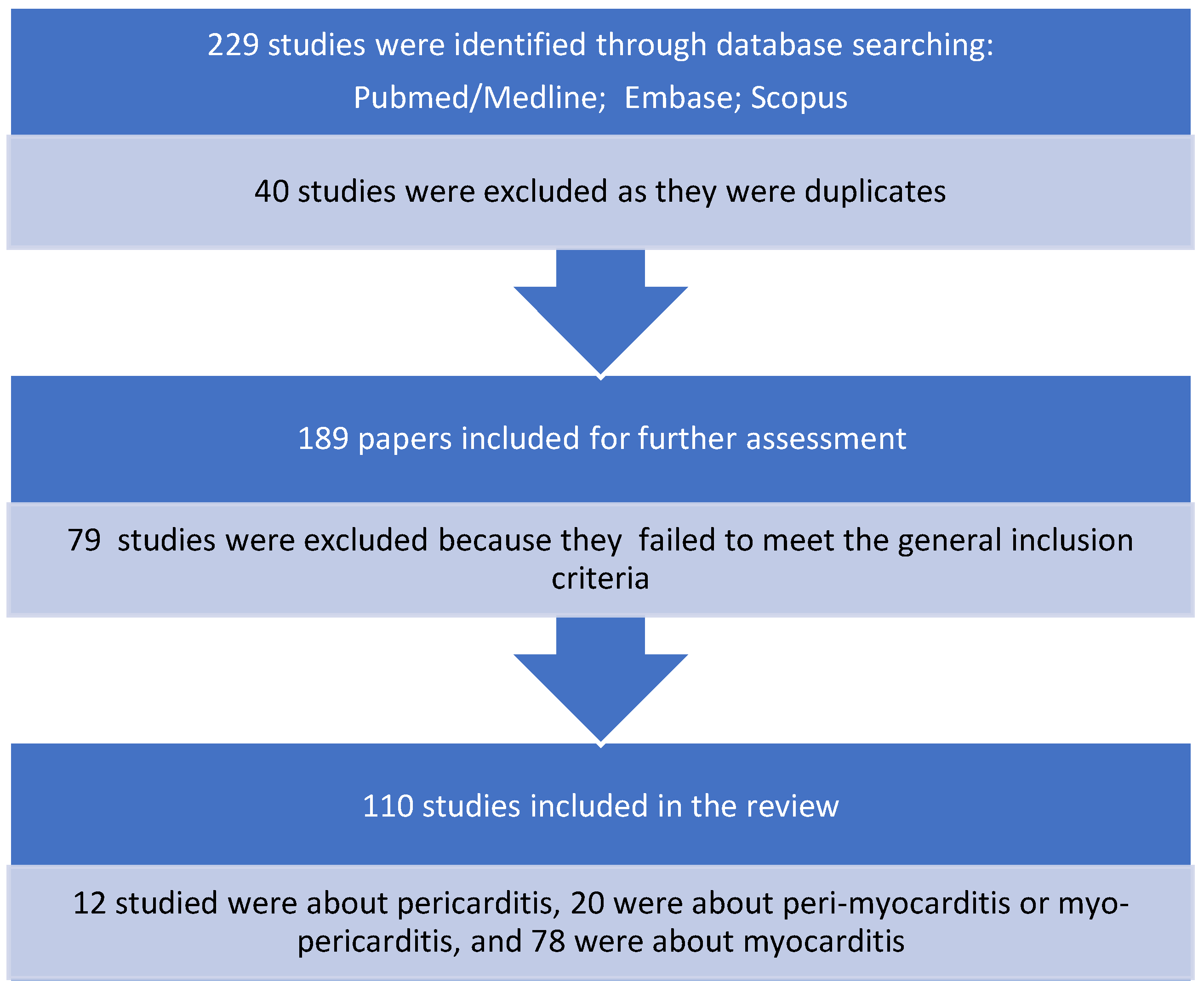
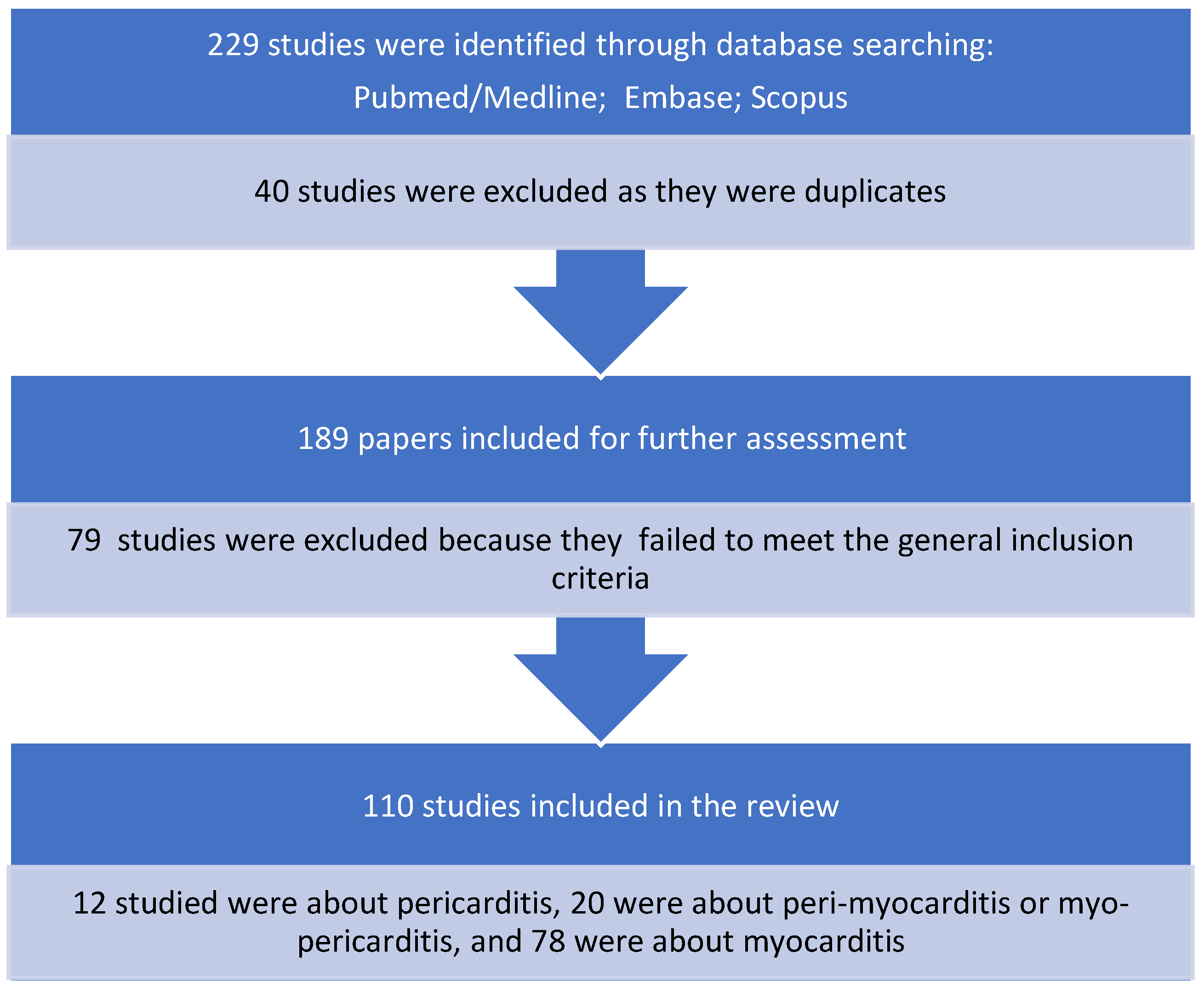
3. Search Strategy
3.1. Study Selection
3.2. Data Extraction
3.3. Data Presentation
4. Results
5. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Calcaterra, G.; Bassareo, P.P.; Barillà, F.; Sergi, D.; Chiocchi, M.; Romeo, F.; Mehta, J.L. The Deadly Quartet (COVID-19, Old Age, Lung Disease, and Heart Failure) Explains Why Coronavirus-Related Mortality in Northern Italy Was So High. Curr. Cardiol. Rev. 2021, 17, 74–77. [Google Scholar]
- Frenck, R.W., Jr.; Klein, N.P.; Kitchin, N.; Gurtman, A.; Absalon, J.; Lockhart, S.; Perez, J.L.; Walter, E.B.; Senders, S.; Bailey, R.; et al. Safety, Immunogenicity, and Efficacy of the BNT162b2 Covid-19 Vaccine in Adolescents. N. Engl. J. Med. 2021, 385, 239–250. [Google Scholar] [CrossRef] [PubMed]
- Calcaterra, G.; Mehta, J.L.; Fanos, V.; Bassareo, P.P. Insights on Kawasaki disease and multisystem inflammatory syndrome: Relationship with COVID-19 infection. Minerva Pediatr. 2021, 73, 203–208. [Google Scholar] [CrossRef] [PubMed]
- Calcaterra, G.; Mehta, J.L.; de Gregorio, C.; Butera, G.; Neroni, P.; Fanos, V.; Bassareo, P.P. COVID-19 Vaccine for Adolescents. Concern about Myocarditis and Pericarditis. Pediatr. Rep. 2021, 13, 530–533. [Google Scholar] [CrossRef]
- Dionne, A.; Sperotto, F.; Chamberlain, S.; Baker, A.L.; Powell, A.J.; Prakash, A.; Castellanos, D.A.; Saleeb, S.F.; de Ferranti, S.D.; Newburger, J.W.; et al. Association of Myocarditis with BNT162b2 Messenger RNA COVID-19 Vaccine in a Case Series of Children. JAMA Cardiol. 2021, 6, 1446. [Google Scholar] [CrossRef] [PubMed]
- Ling, R.R.; Ramanathan, K.; Tan, F.L.; Tai, B.C.; Somani, J.; Fisher, D.; MacLaren, G. Myopericarditis following COVID-19 vaccination and non-COVID-19 vaccination: A systematic review and meta-analysis. Lancet Respir. Med. 2022, 10, 679–688. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Clinical Considerations: Myocarditis and Pericarditis after Receipt of mRNA COVID-19 Vaccines among Adolescents and Young Adults. Published 2021. Available online: https://www.cdc.gov/vaccines/covid-19/clinical-considerations/myocarditis.html (accessed on 28 May 2021).
- Staff, T. Israel Said Probing Link between Pfizer Shot and Heart Problem in Men under 30. The Times of Israel. Available online: https://www.timesofisrael.com (accessed on 23 April 2021).
- Israel Examining Heart Inflammation Cases in People Who Received Pfizer COVID Shot Reuters. Published 25 April 2021. Available online: https://www.reuters.com/world/middle-east/israel-examining-heart-inflammation-cases-people-who-received-pfizer-covid-shot-2021-04-25/ (accessed on 16 May 2021).
- Wong, H.-L.; Hu, M.; Zhou, C.K.; Lloyd, P.C.; Amend, K.L.; Beachler, D.C.; Secora, A.; McMahill-Walraven, C.N.; Lu, Y.; Wu, Y.; et al. Risk of myocarditis and pericarditis after the COVID-19 mRNA vaccination in the USA: A cohort study in claims databases. Lancet 2022, 399, 2191–2199. [Google Scholar] [CrossRef]
- Mansanguan, S.; Charunwatthana, P.; Piyaphanee, W.; Dechkhajorn, W.; Poolcharoen, A.; Mansanguan, C. Cardiovascular Manifestation of the BNT162b2 mRNA COVID-19 Vaccine in Adolescents. Trop. Med. Infect. Dis. 2022, 7, 196. [Google Scholar] [CrossRef]
- Elliott, P.M.; Anastasakis, A.; Borger, M.A.; Borggrefe, M.; Cecchi, F.; Charron, P.; Hagege, A.A.; Lafont, A.; Limongelli, G.; Mahrholdt, H.; et al. 2014 ESC Guidelines on diagnosis and management of hypertrophic cardiomyopathy: The Task Force for the Diagnosis and Management of Hypertrophic Cardiomyopathy of the European Society of Cardiology (ESC). Eur. Heart J. 2014, 35, 2733–2779. [Google Scholar]
- Chou, O.H.I.; Mui, J.; Chung, C.T.; Radford, D.; Ranjithkumar, S.; Evbayekha, E.; Nam, R.; Pay, L.; Satti, D.I.; Garcia-Zamora, S.; et al. COVID-19 vaccination and carditis in children and adolescents: A systematic review and meta-analysis. Clin. Res. Cardiol. 2022. Epub ahead of print. [Google Scholar] [CrossRef]
- Kim, H.W.; Jenista, E.R.; Wendell, D.C.; Azevedo, C.F.; Campbell, M.J.; Darty, S.N.; Parker, M.A.; Kim, R.J. Patients with Acute Myocarditis Following mRNA COVID-19 Vaccination. JAMA Cardiol. 2021, 6, 1196–1201. [Google Scholar] [CrossRef] [PubMed]
- Montgomery, J.; Ryan, M.; Engler, R.; Hoffman, D.; McClenathan, B.; Collins, L.; Loran, D.; Hrncir, D.; Herring, K.; Platzer, M.; et al. Myocarditis Following Immunization with mRNA COVID-19 Vaccines in Members of the US Military. JAMA Cardiol. 2021, 6, 1202–1206. [Google Scholar] [CrossRef] [PubMed]
- Shay, D.K.; Shimabukuro, T.T.; DeStefano, F. Myocarditis Occurring after Immunization with mRNA-Based COVID-19 Vaccines. JAMA Cardiol. 2021, 6, 1115–1117. [Google Scholar] [CrossRef] [PubMed]
- Navar, A.M.; McNally, E.; Yancy, C.W.; O’Gara, P.T.; Bonow, R.O. Temporal Associations between Immunization with the COVID-19 mRNA Vaccines and Myocarditis: The Vaccine Safety Surveillance System Is Working. JAMA Cardiol. 2021, 6, 1117–1118. [Google Scholar] [CrossRef] [PubMed]
- Perez, Y.; Levy, E.R.; Joshi, A.Y.; Virk, A.; Rodriguez-Porcel, M.; Johnson, M.; Roellinger, D.; Vanichkachorn, G.; Huskins, W.C.; Swift, M.D. Myocarditis Following COVID-19 mRNA Vaccine: A Case Series and Incidence Rate Determination. Clin. Infect. Dis. 2021, 3, ciab926. [Google Scholar]
- Bozkurt, B.; Kamat, I.; Hotez, P.J. Myocarditis with COVID-19 mRNA Vaccines. Circulation 2021, 144, 471–484. [Google Scholar] [CrossRef]
- AbdelMassih, A.; El Shershaby, M.; Gaber, H.; Ismail, H.A.; El-Hussseiny, N.; Amin, A.; ElBoraie, A.; Ayad, A.; Menshawey, E.; Sefein, F.; et al. Can sarcopenia index serve as a predictor of myocarditis from mRNA based COVID-19 vaccine, insights from clustered cases and potential involvement of micro-RNAs in its pathogenesis (preprint). EuropePMC 2021. [Google Scholar] [CrossRef]
- Boursier, C.; Chevalier, E.; Filippetti, L.; Imbert, L.; Roch, V.; Huttin, O.; Claudin, M.; Marie, P.Y. 68Ga-DOTATOC digital-PET imaging of inflammatory cell infiltrates in myocarditis following COVID-19 vaccination. Eur. J. Nucl. Med. Mol. Imaging 2022, 49, 1433–1434. [Google Scholar] [CrossRef]
- Chouchana, L.; Blet, A.; Al-Khalaf, M.; Kafil, T.S.; Nair, G.; Robblee, J.; Drici, M.; Valnet-Rabier, M.; Micallef, J.; Salvo, F.; et al. Features of Inflammatory Heart Reactions Following mRNA COVID-19 Vaccination at a Global Level. Clin. Pharmacol. Ther. 2022, 111, 605–613. [Google Scholar] [CrossRef]
- D’Angelo, T.; Cattafi, A.; Carerj, M.L.; Booz, C.; Ascenti, G.; Cicero, G.; Blandino, A.; Mazziotti, S. Myocarditis after SARS-CoV-2 Vaccination: A Vaccine-Induced Reaction? Can. J. Cardiol. 2021, 37, 1665–1667. [Google Scholar] [CrossRef]
- Das, B.B.; Kohli, U.; Ramachandran, P.; Nguyen, H.H.; Greil, G.; Hussain, T.; Tandon, A.; Kane, C.; Avula, S.; Duru, C.; et al. Myopericarditis after messenger RNA Coronavirus Disease 2019 Vaccination in Adolescents 12 to 18 Years of Age. J. Pediatr. 2021, 238, 26–32.e1. [Google Scholar] [CrossRef] [PubMed]
- Ehrlich, P.; Klingel, K.; Ohlmann-Knafo, S.; Hüttinger, S.; Sood, N.; Pickuth, D.; Kindermann, M. Biopsy-proven lymphocytic myocarditis following first mRNA COVID-19 vaccination in a 40-year-old male: Case report. Clin. Res. Cardiol. 2021, 110, 1855–1859. [Google Scholar] [CrossRef] [PubMed]
- Elkazzaz, M.R.; Alshuwaier, G.; Ahmed, A.K. Crosstalk among Strenuous Exercise, IL-6 and S-Protein Based Vaccines for COVID-19 May Explain the Rare Adverse Effects of Myocarditis and Thrombosis in Recently Vaccinated Young People. A Prospective Observational Study. Protoc. Exch. 2022. [Google Scholar] [CrossRef]
- Hajra, A.; Gupta, M.; Ghosh, B.; Ashish, K.; Patel, N.; Manek, G.; Rai, D.; Sreenivasan, J.; Goel, A.; Lavie, C.J.; et al. Proposed Pathogenesis, Characteristics, and Management of COVID-19 mRNA Vaccine-Related Myopericarditis. Am. J. Cardiovasc. Drugs 2022, 22, 9–26. [Google Scholar] [CrossRef] [PubMed]
- Heymans, S.; Cooper, L.T. Myocarditis after COVID-19 mRNA vaccination: Clinical observations and potential mechanisms. Nat. Rev. Cardiol. 2022, 19, 75–77. [Google Scholar] [CrossRef]
- Kadkhoda, K. Post RNA-based COVID vaccines myocarditis: Proposed mechanisms. Vaccine 2022, 40, 406–407. [Google Scholar] [CrossRef]
- Kounis, N.G.; Koniari, I.; Mplani, V.; Velissaris, D.; Tsigkas, G. The pathogenesis of potential myocarditis induced by COVID-19 vaccine. Am. J. Emerg. Med. 2022, 56, 382–383. [Google Scholar] [CrossRef]
- Kounis, N.G.; Mplani, V.; Koniari, I.; Velissaris, D. Hypersensitivity myocarditis and COVID-19 vaccines. Kardiol. Pol. 2022, 80, 109–110. [Google Scholar] [CrossRef]
- Milano, G.; Gal, J.; Creisson, A.; Chamorey, E. Myocarditis and COVID-19 mRNA vaccines: A mechanistic hypothesis involving dsRNA. Future Virol. 2021, 17, 191–196. [Google Scholar] [CrossRef]
- Parra-Lucares, A.; Toro, L.; Weitz-Muñoz, S.; Ramos, C. Cardiomyopathy Associated with Anti-SARS-CoV-2 Vaccination: What Do We Know? Viruses 2021, 13, 2493. [Google Scholar] [CrossRef]
- Switzer, C.; Loeb, M. Evaluating the relationship between myocarditis and mRNA vaccination. Expert Rev. Vaccines 2022, 21, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Takeda, M.; Ishio, N.; Shoji, T.; Mori, N.; Matsumoto, M.; Shikama, N. Eosinophilic Myocarditis Following Coronavirus Disease 2019 (COVID-19) Vaccination. Circ. J. 2022, 86, 1020. [Google Scholar] [CrossRef] [PubMed]
- Truong, D.T.; Dionne, A.; Muniz, J.C.; McHugh, K.E.; Portman, M.A.; Lambert, L.M.; Thacker, D.; Elias, M.D.; Li, J.S.; Toro-Salazar, O.H.; et al. Clinically Suspected Myocarditis Temporally Related to COVID-19 Vaccination in Adolescents and Young Adults: Suspected Myocarditis after COVID-19 Vaccination. Circulation 2022, 145, 345–356. [Google Scholar] [CrossRef] [PubMed]
- Tsilingiris, D.; Vallianou, N.G.; Karampela, I.; Liu, J.; Dalamaga, M. Potential implications of lipid nanoparticles in the pathogenesis of myocarditis associated with the use of mRNA vaccines against SARS-CoV-2. Metabol. Open 2022, 13, 100159. [Google Scholar] [CrossRef]
- Verma, A.K.; Lavine, K.J.; Lin, C.Y. Myocarditis after Covid-19 mRNA Vaccination. N. Engl. J. Med. 2021, 385, 1332–1334. [Google Scholar] [CrossRef]
- Mungmunpuntipantip, R.; Wiwanitkit, V. Response to case report on myocarditis and pericarditis after COVID-19 vaccination. J. Am. Coll. Emerg. Physicians Open 2021, 2, e12559. [Google Scholar] [CrossRef]
- Sharff, K.A.; Dancoes, D.M.; Longueil, J.L.; Johnson, E.S.; Lewis, P.F. Risk of myopericarditis following COVID-19 mRNA vaccination in a large integrated health system: A comparison of completeness and timeliness of two methods. Pharmacoepidemiol. Drug Saf. 2022, 31, 921–925. [Google Scholar] [CrossRef]
- Zorzi, A.; Perazzolo Marra, M.; Rigato, I.; De Lazzari, M.; Susana, A.; Niero, A.; Pilichou, K.; Migliore, F.; Rizzo, S.; Giorgi, B.; et al. Nonischemic Left Ventricular Scar as a Substrate of Life-Threatening Ventricular Arrhythmias and Sudden Cardiac Death in Competitive Athletes. Circ. Arrhythm. Electrophysiol. 2016, 9, e004229. [Google Scholar] [CrossRef]
- Cadegiani, F.A. Catecholamines Are the Key Trigger of COVID-19 mRNA Vaccine-Induced Myocarditis: A Compelling Hypothesis Supported by Epidemiological, Anatomopathological, Molecular, and Physiological Findings. Cureus 2022, 14, e27883. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pfizer-BioNTech | Moderna | AstraZeneca | Other/and Janssen Not Specified |
|---|---|---|---|
| Number: 60/110 | 37/110 | 8/110 | 5/110 |
| Percentage: 54.5% | 33.7% | 7.3% | 4.5% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piras, A.; Melis, G.; Cugusi, L.; Bassareo, P.P. Myopericarditis in a Male Adolescent Following the Second Shot of COVID-19 Pfizer m-RNA Vaccine: Typical Example and Analysis of 110 Single Case Reports. Pediatr. Rep. 2022, 14, 401-409. https://doi.org/10.3390/pediatric14040048
Piras A, Melis G, Cugusi L, Bassareo PP. Myopericarditis in a Male Adolescent Following the Second Shot of COVID-19 Pfizer m-RNA Vaccine: Typical Example and Analysis of 110 Single Case Reports. Pediatric Reports. 2022; 14(4):401-409. https://doi.org/10.3390/pediatric14040048
Chicago/Turabian StylePiras, Alessandra, Giada Melis, Lucia Cugusi, and Pier Paolo Bassareo. 2022. "Myopericarditis in a Male Adolescent Following the Second Shot of COVID-19 Pfizer m-RNA Vaccine: Typical Example and Analysis of 110 Single Case Reports" Pediatric Reports 14, no. 4: 401-409. https://doi.org/10.3390/pediatric14040048
APA StylePiras, A., Melis, G., Cugusi, L., & Bassareo, P. P. (2022). Myopericarditis in a Male Adolescent Following the Second Shot of COVID-19 Pfizer m-RNA Vaccine: Typical Example and Analysis of 110 Single Case Reports. Pediatric Reports, 14(4), 401-409. https://doi.org/10.3390/pediatric14040048