Abstract
Chlamydia trachomatis infection is a public health problem. Serological tests can determine the disease burden and serve as a biomarker for identifying patients with infertility due to tubal obstruction. However, cross-reactions between chlamydial species have been reported, which causes problems with diagnosis. A real-time PCR commercial test for the detection of endocervical infection and two ELISAs with the recombinant major outer membrane protein (rMOMP) from C. trachomatis and C. abortus as antigens were used to diagnose both infections. The prevalence of endocervical infection by C. trachomatis was 7.77%, and that of IgG antibodies against C. trachomatis and C. abortus was 31.1% and 10.7%, respectively. The ELISA with C. trachomatis rMOMP showed a sensitivity of 75% and a specificity of 72.5%. The lowest sensitivity (25%) and high specificity (76.8%) were obtained with anti-C. abortus rMOMP ELISAs. A low cross-reactivity of 7% between ELISA tests was observed. Conclusion. The recombinant MOMP ELISA could help identify women who had contact with C. trachomatis or C. abortus and could be a tool to lower the costs of performing molecular testing on all patients attending an infertility clinic.
1. Introduction
According to the WHO, sexually transmitted infections (STIs) affect 374 million people worldwide annually [Sexually Transmitted Infections, WHO]. Chlamydia trachomatis (CT) is one of these microorganisms, affecting 129 million individuals [1]. However, this figure may be lower than the actual number, as the infection is usually asymptomatic in 50% of men and 80% of women [2]. CT infection is known to be more common in women than in men, and its prevalence varies according to age and country of residence [3,4]. Untreated CT infections cause severe complications in women, such as pelvic inflammatory disease (PID), ectopic pregnancy, and tubal factor infertility (TFI) [5]. Moreover, it can promote HIV transmission and contribute to the development of cervical cancer [4,6]. Despite the above, the detection and treatment of this pathogen’s infection remain unmet goals in various countries.
Currently, the diagnosis of CT infection is based on nucleic acid amplification techniques (NAATs). These methods necessitate substantial resources and labor [7], making it impossible to perform extensive screening, and even routine diagnosis is impractical in settings with limited resources. Furthermore, a negative NAAT endocervical sample result does not assure that there is no active infection with this pathogen in the upper genital tract [7,8], so the test cannot determine the impact it may have on the health of a population, while a serological study can determine the disease burden [9,10]. Likewise, serological studies are also valuable for understanding the natural history of the infection and supporting the development and evaluation of vaccines against CT [10,11].
Significant differences in sensitivity and specificity have been observed among the different antigens used to detect antibodies to CT [12]. For more straightforward anti-CT ELISA tests, the majority of immunodominant protein antigens, such as OmpA, Omp2, PorB, or Hsp60, are highly conserved across several Chlamydia species [13,14,15]. Therefore, these have been considered poorly suited for CT diagnosis through this test. However, few studies have been conducted on the cross-reactivity of the major outer membrane protein (MOMP) antigen from various Chlamydia species in the context of CT diagnoses.
In a mouse model, pooled sera from 9 to 50 mice immunized against a single Chlamydia species were tested for cross-reactivity using commercial kits for diagnosing CT and C. pneumoniae [15]. The Serion ELISA’s CT-specific OmpA fragment antigen showed no cross-reactivity. In contrast, the GenWay ELISA’s C. trachomatis EB (elementary bodies) antigen showed complete cross-reactivity with antisera against all other Chlamydia species. This cross-reactivity could be due to LPS or other surface proteins in EB. Compared with the Serion ELISAs, the antigen used is a recombinant MOMP purified via chromatography in urea [15].
Chlamydia abortus (CA) is known as the causative agent of ovine enzootic abortion (OEA) and goat abortion. Knowledge of the epidemiology of CA infections in humans is limited. In the absence of global data, the UK generally reports one or two cases each year in pregnant women, with diagnosis established through culture, PCR, or immunohistochemical analysis of placental tissue following abortion [16]. To date, no human serology studies have been conducted to determine whether it is common for humans to come into contact with this bacterium.
The ELISA test is a suitable technique for detecting anti-chlamydia antibodies. However, many other factors can affect the test result, such as the type of microplate, antigen, blocking substance, antibody dilution, conjugate, and substrate used [17]. Recently, our research group standardized an ELISA test with the recombinant MOMP as an antigen [18], which showed a good correlation with infertile women (RR = 1.8, CI95% 1.43–2.39; p < 0.001). This study aimed to identify the effect of cross-reactivity in the ELISA CT recombinant MOMP system by evaluating the antibody response against CA recombinant MOMP from negative and positive serum samples of patients with or without CT infection.
2. Materials and Methods
2.1. Ethics Approval and Consent to Participate
All participants received and signed written informed consent to participate in this study. The ethical principles of the Declaration of Helsinki and the Ethics Committee of the National Institute of Perinatology were followed. This study was registered with the number 2019-1-33.
2.2. Participants and Clinical Samples
This prospective study included 80 infertile and 23 pregnant women, aged 18–45 years, who attended a tertiary institution between 4 July 2022 and 16 February 2023. The patients studied resided in the following locations: 88.3% were from the Mexico City Metropolitan Area (State of Mexico, 53.4%, Mexico City, 29.1%, and State of Hidalgo, 5.8%), and 11.6% were from other states, such as Guerrero, Morelos, Puebla, Tlaxcala, and Veracruz. On the other hand, the socioeconomic level of the patients was level 1 in 90% and level 2 in 10%.
The inclusion criteria were as follows: (1) pregnant women with cervicitis; (2) women with infertility (women of childbearing age who did not become pregnant within one year despite living with a partner, maintaining a regular sex life, and lacking contraceptive measures); and (3) women not treated with antibiotics, antiviral medications, or vaginal medications within the three days before the examination. The exclusion criteria were as follows: (1) refusal to provide informed consent; (2) any acute or chronic condition that would limit the patient’s ability to participate in the study. Patients were classified as infertile or pregnant by physicians specializing in gynecology and obstetrics.
Experienced paramedics obtained blood samples. Serum was recovered after clotting and centrifuging each sample. Serum samples were stored at −80 °C until analysis.
2.3. Obtaining Recombinant MOMP (rMOMP)
The recombinant protein of CT serotype L2 (CTrMOMP) was obtained from the transformed Escherichia coli strain BL-21 with the CT ompA gene (1142 bp), as previously described by de Haro-Cruz et al. [19]. The quality and purity of the protein were determined via electrophoresis in 12% polyacrylamide gels, and the concentration was assessed using the Bradford technique.
Dr. Miguel A. De la Rosa-Ramos, a researcher at the Faculty of Veterinary Medicine, UNAM, Mexico, donated the Chlamydia abortus rMOMP (CArMOMP).
2.4. Recombinant ELISA
For the ELISA, Costar® high-affinity 96-well plates (Corning Inc., NY, USA) were used. Each plate was sensitized with 100 µL of either CTrMOMP or CArMOMP at a concentration of 200 pg/mL in carbonate–bicarbonate solution (0.1 M, pH 9.5). Analyzed sera were diluted 1:256 in PBS-Tween (0.05%), and the procedure was performed as previously described by de Haro-Cruz et al., 2019 (The ELISA assay description is provided in more detail in the Supplementary Material S1). The signal intensity value (S/Co) was obtained using the following formula described by de Haro-Cruz et al. [19].
Each sample was analyzed in duplicate.
AU = absorbance units
2.5. Molecular Detection of Chlamydia trachomatis Infection
The reference test used for CT detection in endocervical samples was a real-time PCR test from Abbott Real-time CT/NG (Abbott Molecular Inc., Des Plaines, IL, USA), performed on the Abbott m2000 robotic system. The Abbott system amplifies and detects two cryptic plasmid sites: a 102 bp fragment in the 377 bp deletion region (CD1) of the Swedish variant and a second 140 bp fragment located outside the CD1 region. The procedure involved placing the 103 endocervical sample tubes from each participating woman in the m2000 automated equipment, which performed the entire procedure.
2.6. Statistical Analysis
The cutoff point and the highest sensitivity and specificity were evaluated by analyzing receiver operating characteristic (ROC) curves. The positive and negative predictive values (PPV and NPV) were calculated, and using two-by-two tables, McNemar’s test was used to compare the differences in sensitivity and specificity between the tests. In addition, likelihood ratios for a positive test (LR+) and a negative test (LR) were determined. Student’s t-test was used to test parametric values. The magnitude of the associations between variables was expressed as the relative risk (RR) with a 95% confidence interval (CI). p values ≤ 0.05 were considered statistically significant. A Bland–Altman analysis was performed to compare the cross-reactivity of the recombinant MOMP antigen of CT with that of the recombinant MOMP of C. abortus in an ELISA system. All data were analyzed using IBM SPSS 21.0 (SPSS Inc., Chicago, IL, USA).
3. Results
3.1. Population Characteristics
One hundred and three serum samples were analyzed, consisting of twenty-three from pregnant women and eighty from women with infertility. The average age of the participants was 30.9 ± 5.2 and 33.8 ± 4.3 years, respectively. Most of the pregnant women were under 34 years (Chi2 = 4.312; p < 0.038).
The most common causes of infertility were endocrine–ovarian factors and male factors. The prevalence of endocrine–ovarian was statistically significant (Chi2 = 6.277; p < 0.012), although this significance was moderate. A sexual debut at 18 years of age or older and having two or more sexual partners were more common during the patient’s sexually active life (p < 0.05), although this association was weak.
Another interesting aspect was the frequent presence of tubal factor infertility in infertile women, but no association was observed concerning the Chlamydia infection diagnosis in the endocervix; the same situation occurred with ectopic pregnancy (Table 1). Only eight patients (7.77%) showed positivity to DNA PCR detection in their endocervical samples; two of them were pregnant, and six were infertile patients.

Table 1.
Demographic characteristics of participants contributing sera samples to this validation.
3.2. Sensitivity and Specificity of ELISA with Recombinant MOMP
To determine the diagnostic accuracy of the ELISA tests sensitized with the recombinant MOMPs of CT and CA (CTrMOMP and CArMOMP, respectively), the cutoff point, the highest sensitivity, and specificity were evaluated by analyzing receiver operating characteristic (ROC) curves based on the results of PCR for the detection of C. trachomatis DNA in endocervical samples. The results are shown in Figure 1.
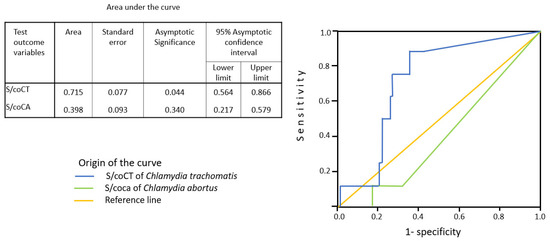
Figure 1.
Anti-Chlamydia trachomatis or anti-Chlamydia abortus antibodies in enzyme-linked immunosorbent assays (ELISAs) in receiver operating characteristic (ROC) analyses. The antibody consensus of eight C. trachomatis infection-positive and 95 C. trachomatis infection-negative sera was used as the categorical variable known a priori, and the signal intensity (S/Co) observed values of serum reactivities of an ELISA test were used as predictor variables of the anti-C. trachomatis antibody (blue line) or anti-C. abortus antibody (green line) status. IgG’s average sensitivity against the recombinant MOMP from C. trachomatis or C. abortus detection was 75% and 12.5%, respectively. The specificities were 72.6% and 82%, respectively. The area under the curve (AUC) was 0.715 (p < 0.05) and 0.398, respectively.
The CTrMOMP exhibited a sensitivity and specificity of 75% and 72.6%, respectively, when the cutoff point was set at 0.215 of the S/Co ratios. The total area under the curve was 0.715 (p < 0.05). In the case of the CArMOMP, it exhibited a sensitivity and specificity of 12.5% and 82.1%, respectively, when the cutoff point was set at 0.067 of the S/Co ratios. The total area under the curve was not statistically significant (Figure 1).
The PPV and NPV tests were 19% and 97% for recombinant C. trachomatis MOMP, while they were 6% and 92% for recombinant C. abortus MOMP (Table 2A,B).
Table 2.
Sensitivity, specificity, and cross-reactivity for the determination of anti-C. trachomatis or anti-C abortus antibody status using different ELISAs.
The ELISA test using recombinant C. trachomatis MOMP (CTrMOMP) as an antigen was suitable for identifying individuals exposed to C. trachomatis (Table 2A). In contrast, according to likelihood ratio analysis, the ELISA test using recombinant C. abortus MOMP (CArMOMP) as an antigen was found to be a poor test for identifying these individuals (Table 2B). The cross-reactivity percentage between the CTrMOMP and CArMOMP was 6.8% (Table 2C).
3.3. The Cross-Reactivity Analyses Between the Recombinant MOMPs
A Bland–Altman analysis was used to assess the concordance between the two ELISAs (Figure 2). The absorbance difference mean (0.1246) was statistically significant (p < 0.0001), indicating a positive bias. This suggests that, on average, the ELISA with C. trachomatis antigens tends to yield higher absorbance values (purple points) than the ELISA with C. abortus antigen (yellow points). The standard deviation of the observance differences (0.16129) and the standard error of the mean (0.01589) indicate the variability of the differences between the two ELISA systems.
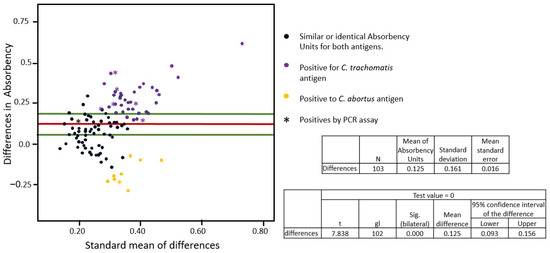
Figure 2.
Agreement analyses between recombinant MOMP of Chlamydia trachomatis and Chlamydia abortus ELISA systems using the Bland–Altman test. The X-axis represents the mean of the absorbance measurements from the two ELISA systems, and the Y-axis represents the difference between the absorbance measurements from the two ELISA systems for each serum sample—black points are sera with similar or identical absorbance for both antigens; purple points are positive for C. trachomatis; yellow points are positive for C. abortus; asterisks are PCR samples positive for C. trachomatis infection. The red line represents the mean of the differences (bias), which is 0.1246, and the green lines represent the limits of agreement (generally ±1.96 times the standard deviation of the differences).
In Figure 2, the red line represents the mean of the absorbance difference, while the green lines represent the limits of agreement (generally ± 1.96 times the standard deviation of the differences). The black points between the green lines indicate the concordance, where a negative result was obtained from both the between-antigens and the PCR assay for Chlamydia.
The black points adjacent to the yellow points, extending beyond the green line, represent serum samples that exhibited cross-reactivity with both recombinant MOMPs but with lower absorbance for the C. trachomatis protein. In contrast, the black points adjacent to the purple points indicate cross-reactivity with both recombinant MOMPs but with a lower absorbance value for the C. abortus protein.
3.4. Association Between Antibodies Against C. trachomatis and Gynecology or Obstetric Pathology
The overall prevalence of patients with antibodies against C. trachomatis was 31.1% (32/103). A statistically significant association was observed in patients with a negative molecular diagnosis for Chlamydia, in whom antibodies against C. trachomatis were present (RR = 1.2; 95% CI: 1.01–1.42; p < 0.011). Conversely, no significant association was observed between the presence of antibodies against C. trachomatis sera and infertile women, ectopic pregnancies, miscarriage, endocrine–ovarian factors, uterine factors, tubal factor infertility, or masculine factors (Table 3). Similarly, the association observed with the age of patients, sexual debut, and the number of sexual partners was not statistically significant.
Table 3.
Association between the presence of anti-Chlamydia trachomatis IgG antibodies and various clinical and demographic characteristics.
4. Discussion
Over the past 50 years, several seroassays have been developed to detect any immunoglobulin-type anti-C. trachomatis. Furthermore, the majority of immunodominant protein candidate antigens in ELISAs (e.g., OmpA, Omp2, PorB, or Hsp60) are highly conserved within Chlamydia species [13,14,15] and, therefore, have not been considered for CT infection diagnoses. Additionally, the use of these assays outside of epidemiologic CT studies is relatively limited, although some argue that seroassays may be helpful when evaluating patients with suspected PID or TFI [20,21].
Acknowledging these limitations, this study specifically analyzed the cross-reactivity between two recombinant MOMPs, CTrMOMP and CArMOMP, in the same ELISA conditions and the same sera of pregnant and infertile women. Our findings demonstrated that women with PCR-confirmed CT infection in endocervical samples showed IgG antibodies against CT in 75% of cases and not in 25% (two patients). Both showed negative results of IgG against CT, which is possible if the infection has recently occurred. Similar results were reported by Rahman et al. [12], who tested sera from 125 women with a molecular test-proven active C. trachomatis infection using four commercial ELISAs. The anti-C. trachomatis IgG was detected in 61% (GenWay), 58% (Serion), 53% (Savyon), and 42% (Medac) of these sera, and 32% of the sera were negative for anti-C. trachomatis IgG.
The prevalence of Chlamydia infection in this study was 7.77%, a significant percentage compared to that reported in 2018 in Mexico, which was 4.3% [22]. This suggests an increase in the incidence of CT infection, which is particularly concerning given that the Latin American population, in general, has the highest prevalence of CT infection globally, with 6.7%, compared with Africa (3.8%) and Southeast Asia (0.8%) [23]. This observed increase in prevalence could have significant implications for public health and underscores the need for effective diagnostic tools.
Given resource constraints in lower/middle-income countries, molecular Chlamydia screening is cost-prohibitive [24], and only symptomatic persons presenting to clinical settings are treated, based primarily on the World Health Organization’s (WHO) guidelines for managing STIs [25]. In this context, the seric antibodies against the CT test could be a cost-effective solution to identify the population exposed to Chlamydia infection. Following molecular confirmation in people with IgG antibodies against CT, they could receive treatment for Chlamydia infection and eliminate it, potentially reducing overall healthcare costs. Such cost reductions could have significant implications for healthcare systems in resource-constrained settings, making the ELISA a potentially valuable tool in the fight against Chlamydia.
In this study, the prevalence of IgG antibodies against CT was 33%, similar to that reported in infertile women in Mexico in 2011 [26]. However, several other studies have identified a prevalence of more than 50%. Ohman et al. found anti-C. trachomatis MOMP-specific IgG antibodies in 65.5% (269/411) of women with recurrent infection. Without recurrent disease, seroprevalence declined to 34.5% (142/411) 3–10 years after the initial infection [27]. This could suggest that positive patients with anti-CT antibodies in this study had the infection three or more years before detecting these antibodies, as in the study of Cortés-Rivas et al., where patients who were positive for molecular detection three years before had the highest levels of anti-Chlamydia antibodies [18].
On the other hand, 17.5% of women in this study showed IgG antibodies against the CArMOMP, 10.7% of them did not show anti-MOMP antibodies of CT, and 6.8% showed cross-reactivity with recombinant CTrMOMP antigen. These findings suggest a low cross-reactivity of 7%, which might be further diminished with a change in ELISA test conditions. The prevalence of antibodies against CA is not entirely known. A study by Hagemann et al. [28] demonstrated that the sera of women who had an abortion caused by CA infection revealed an antibody response to the bacterium’s surface antigens (MOMP, MIP, and Pmp13G). This suggests that this study’s positive sera are due to a response to CA infection or previous contact with this pathogen. The CArMOMP has been evaluated previously with goat sera from Mexico and showed more sensitivity than the ELISA ID Screen Chlamydophila abortus indirect multi-species (rue Luis Pasteur, Grabels, France) [manuscript in preparation]. In this study, the prevalence of IgG antibodies against C. abortus was 10.7%.
Eight of the 17 positive to CA sera identified in this study exhibited high absorbance in the ELISA with C. abortus antigen, with six samples originating from the State of Mexico, one from the State of Guerrero, and one from Mexico City. However, no statistically significant results were shown (X2 = 1.474; p = 0.225). The State of Mexico is one of the central sheep-producing states. A study conducted by Palomares et al. in 2020 on Mexican sheep demonstrated the presence of antibodies against CA in 25.4% of the flocks in the State of Mexico that presented the disease known as ovine enzootic abortion [29]. This suggests that these women may have had previous contact with these animals. However, we cannot confirm this phenomenon because the necessary information was not collected on whether the patient had contact with domestic or pet animals; therefore, it is advisable to collect this information for future studies, as it could help in understanding the transmission and potential spread of CA infections.
Furthermore, it is necessary to consider that C. pneumoniae or C. psittaci infection can also produce IgG antibodies with cross-reactivity against CTrMOMP. Hernández-Trejo et al. [30] have shown that 46% of Mexican pregnant women had antibodies against CT, C. psittaci, and C. pneumoniae via micro-immunofluorescence assay; hence, this could also be a reason for the hindrance of the diagnosis of CT infection. In addition, Baud et al. [31] identified that three tests of ELISA for CT diagnosis showed cross-reaction with C. psittaci (p < 0.001) and one with C. pneumoniae. Similarly, Jones et al. [32] showed poor specificity (5.6%; 95% CI, 0.68–18.7) in CT, wherein an ELISA test (Genzyme Virotech) was reactive with 34 of 36 positive sera to C. psittaci and C. pneumoniae.
Currently, C. psittaci infection in humans is more common than previously thought. A high number of avian species have been identified as susceptible to this bacterium (467 different species from 30 different orders of birds) [33]. The primary mode of transmission may be through aspiration or contact with feces from infected birds. A study by Hou et al. [34] in poultry farms and zoos in China showed that 3.13% (40/1278) of poultry fecal samples were positive in the qPCR assay, while 3.82% (6/157) were from throat samples. Similar results were obtained in a Chinese poultry market, finding positivity rates in wastewater (12.5%), poultry feces (7.43%), cage swabs (6.59%), pharyngeal/cloacal swabs from birds (3.33%), and air samples (2.29%); furthermore, human-to-human transmission has also been documented [35], which favors the development of asymptomatic carriers and the first step towards colonization of human tissue. Similarly, the detection of C. abortus as a cause of pneumonia or infection in different human tissues has been reported [16,36,37].
It is essential to point out that C. abortus is regarded as the most closely related to and is suggested to have evolved from C. psittaci [38]. The study’s low cross-reactivity against recombinant CArMOMP may indicate that the principal cross-reactivity may be directed to C. pneumoniae or other Chlamydia species. This finding underscores the need for further research to understand the cross-reactivity patterns among different Chlamydia species, which could significantly impact the accuracy of seroassays for Chlamydia diagnosis.
The ELISA test offers significant potential in adjusting the antigen concentration and the serum titer, enhancing the system’s sensitivity and specificity. Our previous study demonstrated that a serum dilution 1:256, when the ELISA microplate is sensitized at 200 pg/mL, can identify sera with IgG antibodies against CT [18]. Furthermore, this ELISA effectively identified infertile women with Chlamydia infection (RR = 1.85; CI 95% 1.43–2.39; p < 0.001) compared to pregnant women [18]. The ELISA test has significant potential in adjusting the antigen concentration and the serum titer, enhancing the system’s sensitivity and specificity. However, the ELISA conditions employed in this study showed no statistical significance in the infertile population; this could be because many of the pregnant women had a history of infertility. One possibility for the observed decrease in anti-chlamydia antibodies is the absence of reinfection. It is known that recurrent infections can enhance the humoral immune response. A study by Öhman found that approximately one-third of women who received a single notification of chlamydia infection remained seropositive 3 to 10 years after their initial infection. Moreover, the absence of recurrent infections led to a decline in seroprevalence from 65% to 34.5% over the same period. The above highlights the importance of monitoring IgG levels over different years, as it can provide valuable insights into the long-term effects of C. trachomatis infection or other species of Chlamydia infections [27].
The ELISA system’s sensitivity and specificity with the CT antigen in this study, when the cutoff was 0.217, were 75% and 72.6%, respectively. It also had a high NPV and had a likelihood ratio suggesting a fair test. Meanwhile, ELISA with CA antigen showed a low sensitivity and a high specificity of 25% and 85%, respectively, and a low NPV of 70%, and had a likelihood ratio suggesting a poor test. The Bland–Atman plot suggests moderate agreement between the two ELISA systems, with a positive bias to the CT antigen ELISA’s assay and significant variability in the differences. Thus, cross-reactivity between these two systems is low. Although the sample size of 103 may be considered inadequate for obtaining a precise estimate of the test’s operating characteristics, it provides a solid starting point for further analysis. This study can be regarded as a pilot or preliminary study.
Finally, it would be interesting to know the response of antibodies against another recombinant MOMP from C. pneumoniae and C. psittaci, as well as to identify whether the women with IgG antibodies against CA have endocervical infection by this pathogen.
5. Conclusions
The recombinant MOMP ELISA could help identify women who had contact with CT or CA and serve as a valuable tool to lower the costs of performing molecular testing on all patients attending infertility clinics.
Supplementary Materials
The following supporting information can be downloaded at https://www.mdpi.com/article/10.3390/microbiolres16070159/s1: Recombinant ELISA test.
Author Contributions
Conceptualization, B.A.-R., M.J.d.H.-C. and F.M.G.-I.; methodology, M.L.-H. and M.A.D.l.R.-R.; validation, B.A.-R., M.J.d.H.-C. and E.D.-A.; formal analysis, M.L.-H. and F.M.G.-I.; investigation, B.A.-R., M.J.d.H.-C., F.M.G.-I., M.L.-H., M.A.D.l.R.-R. and E.D.-A.; writing—original draft preparation, F.M.G.-I.; writing—review and editing, B.A.-R., M.J.d.H.-C., M.L.-H., M.A.D.l.R.-R. and E.D.-A. All authors have read and agreed to the published version of the manuscript.
Funding
The authors thank the National Institute of Perinatology, Isidro Espinosa de los Reyes, for supporting this research project, registered with ID numbers 2022-1-19 and 2019-1-33, and the DGAPA PAPIIT from the Universidad Nacional Autónoma de Mexico project, registered with ID Number IT202224.
Institutional Review Board Statement
The research, ethics, and biosafety committees of the National Institute of Perinatology Isidro Espinosa de los Reyes approved this study, registration number 2022-1-19. The authors declare that the procedures followed were in accordance with the regulations of the relevant clinical research ethics committee and with those of the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Informed Consent Statement
The authors obtained written informed consent from the patients or subjects mentioned in this article.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Conflicts of Interest
The authors declare that this study was conducted without any commercial or financial relationships that could potentially create conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| CT | Chlamydia trachomatis |
| CA | Chlamydia abortus |
| CTrMOMP | Chlamydia trachomatis recombinant MOMP |
| CArMOMP | Chlamydia abortus recombinant MOMP |
| MOMP | Major outer membrane protein |
References
- World Health Organization. Sexually Transmitted Infections (STIs). Available online: https://www.who.int/news-room/fact-sheets/detail/sexually-transmitted-infections-(stis) (accessed on 15 May 2025).
- Malhotra, M.; Sood, S.; Mukherjee, A.; Muralidhar, S.; Bala, M. Genital Chlamydia trachomatis: An update. Indian J. Med. Res. 2013, 138, 303–316. [Google Scholar] [PubMed]
- Dielissen, P.W.; Teunissen, D.A.M.; Lagro-Janssen, A.L.M. Chlamydia prevalence in the general population: Is there a sex difference? a systematic review. BMC Infect. Dis. 2013, 13, 534. [Google Scholar] [CrossRef]
- World Health Organization. Chlamydia. Available online: https://www.who.int/news-room/fact-sheets/detail/chlamydia (accessed on 15 May 2025).
- Alexiou, Z.W.; Hoenderboom, B.M.; Hoebe, C.J.; Dukers-Muijrers, N.H.; Götz, H.M.; van der Sande, M.A.; de Vries, H.J.; den Hartog, J.E.; Morré, S.A.; van Benthem, B.H. Reproductive tract complication risks following Chlamydia trachomatis infections: A long-term prospective cohort study from 2008 to 2022. Lancet Reg. Health Eur. 2024, 45, 101027. [Google Scholar] [CrossRef]
- Escarcega-Tame, M.A.; López-Hurtado, M.; Escobedo-Guerra, M.R.; Reyes-Maldonado, E.; Castro-Escarpulli, G.; Guerra-Infante, F.M. Co-infection between genotypes of the human papillomavirus and Chlamydia trachomatis in Mexican women. Int. J. STD AIDS 2020, 31, 1255–1262. [Google Scholar] [CrossRef]
- Herrmann, B.; Malm, K. Comparison between Abbott m2000 RealTime and Alinity m STI systems for detection of Chlamydia trachomatis, Neisseria gonorrhoeae, and Mycoplasma genitalium. Eur. J. Clin. Microbiol. Infect. Dis. 2021, 40, 2217–2220. [Google Scholar] [CrossRef]
- Villagrana, Z.J.R.; López, H.M.; Flores, S.V.R.; de Haro, C.M.J.; Escobedo, G.M.R.; Guerra, I.F.M. Persistence of Chlamydia trachomatis in the endometrium and peritoneal fluid of patients with infertility but negative cervical cultures. Ginecol. Obstet. Mex. 2013, 81, 23–28. [Google Scholar]
- Puolakkainen, M. Laboratory diagnosis of persistent human chlamydial infection. Front. Cell. Infect. Microbiol. 2013, 3, 99. [Google Scholar] [CrossRef]
- Hepler, R.W.; Nahas, D.D.; Lucas, B.; Kaufhold, R.; Flynn, J.A.; Galli, J.D.; Swoyer, R.; Wagner, J.M.; Espeseth, A.S.; Joyce, J.G.; et al. Spectroscopic analysis of chlamydial major outer membrane protein in support of structure elucidation. Protein Sci. 2018, 27, 1923–1941. [Google Scholar] [CrossRef] [PubMed]
- Horner, P. Can Chlamydia Serology Be Used to Help Inform a Potential Future Chlamydia Vaccination Strategy? Sex. Transm. Dis. 2017, 44, 722–724. [Google Scholar] [CrossRef]
- Rahman, K.S.; Darville, T.; Russell, A.N.; O’Connell, C.M.; Wiesenfeld, H.C.; Hillier, S.L.; Lee, D.A.E.; Kaltenboeck, B. Comprehensive molecular serology of human Chlamydia trachomatis infections using peptide enzyme-linked immunosorbent assays. mSphere 2018, 3, e00253-18. [Google Scholar] [CrossRef]
- Bas, S.; Muzzin, P.; Ninet, B.; Bornand, J.E.; Scieux, C.; Vischer, T.L. Chlamydial serology: Comparative diagnostic value of immunoblotting, microimmunofluorescence test, and immunoassays using different recombinant proteins as antigens. J. Clin. Microbiol. 2001, 39, 1368–1377. [Google Scholar] [CrossRef] [PubMed]
- Hammerschlag, M.R. Pneumonia due to Chlamydia pneumoniae in children: Epidemiology, diagnosis, and treatment. Pediatr. Pulmonol. 2003, 36, 384–390. [Google Scholar] [CrossRef]
- Rahman, K.S.; Kaltenboeck, B. Multipeptide Assays for Sensitive and Differential Detection of Anti-Chlamydia trachomatis Antibodies. J. Infect. Dis. 2021, 24, S86–S95. [Google Scholar] [CrossRef]
- Turin, L.; Surini, S.; Wheelhouse, N.; Rocchi, M.S. Recent advances and public health implications for environmental exposure to Chlamydia abortus: From enzootic to zoonotic disease. Vet. Res. 2022, 53, 37. [Google Scholar] [CrossRef]
- Alhajj, M.; Zubair, M.; Farhana, A. Interfering Factors. In Enzyme-Linked Immunosorbent Assay; StatPearls Publishing LLC: Treasure Island, FL, USA, 2023. Available online: https://www.ncbi.nlm.nih.gov/books/NBK555922/#article-21178.s5 (accessed on 17 May 2025).
- Cortés-Rivas, A.; López-Hurtado, M.; Guerra-Infante, F. Seroprevalence of Chlamydia trachomatis infection using an ELISA test sensitized with a recombinant protein. JBBR 2025, 9, 9–16. [Google Scholar] [CrossRef]
- de Haro-Cruz, M.J.; Guadarrama-Macedo, S.I.; López-Hurtado, M.; Escobedo-Guerra, M.R.; Guerra-Infante, F.M. Obtaining an ELISA test based on a recombinant protein of Chlamydia trachomatis. Int. Microbiol. 2019, 22, 471–478. [Google Scholar] [CrossRef]
- Broeze, K.A.; Opmeer, B.C.; Coppus, S.F.P.J.; Van Geloven, N.; Alves, M.F.C.; Ånestad, G.; Bhattacharya, S.; Allan, J.; Guerra-Infante, M.F.; Den Hartog, J.E.; et al. Chlamydia antibody testing and diagnosing tubal pathology in subfertile women: An individual patient data meta-analysis. Hum. Reprod. Update 2011, 17, 301–310. [Google Scholar] [CrossRef]
- Akabueze, J.C.; Agu, P.U.; Ugwu, E.O.; Obi, S.N.; Aniebue, U.U.; Eleje, G.U.; Ugwu, A.O.; Anigbo, C.S.; Ekwueme, P.C.; Eze, M.I.; et al. Association Between Anti-Chlamydial Antibodies and Tubal Factor Infertility in South Eastern Nigeria. West Afr. J. Med. 2024, 41, 1091–1096. [Google Scholar]
- López-Hurtado, M.; García-Romero, S.; Escobedo-Guerra, M.R.; Bustos-López, D.; Guerra-Infante, F.M. Prevalence of genital Chlamydia trachomatis infection in women attending in the National Institute of Perinatology from Mexico City. Rev. Chil. Infectol. 2018, 35, 371–376. [Google Scholar] [CrossRef] [PubMed]
- Huai, P.; Li, F.; Chu, T.; Liu, D.; Liu, J.; Zhang, F. Prevalence of genital Chlamydia trachomatis infection in the general population: A meta-analysis. BMC Infect. Dis. 2020, 20, 589. [Google Scholar] [CrossRef]
- Connolly, S.; Kilembe, W.; Inambao, M.; Visoiu, A.M.; Sharkey, T.; Parker, R.; Wall, K.M.; Tichacek, A.; Hunter, E.; Allen, S. A Population-Specific Optimized GeneXpert Pooling Algorithm for Chlamydia trachomatis and Neisseria gonorrhoeae to Reduce Cost of Molecular Sexually Transmitted Infection Screening in Resource-Limited Settings. J. Clin. Microbiol. 2020, 58, e00176-20. [Google Scholar] [CrossRef]
- World Health Organization. Guidelines for the Management of Symptomatic Sexually Transmitted Infections. Available online: https://www.who.int/publications/i/item/9789240024168 (accessed on 15 May 2025).
- Hubacher, D.; Lara-Ricalde, R.; Taylor, D.J.; Guerra-Infante, F.; Guzmán-Rodríguez, R. Use of copper intrauterine devices and the risk of tubal infertility among nulligravid women. N. Engl. J. Med. 2001, 345, 561–567. [Google Scholar] [CrossRef] [PubMed]
- Öhman, H.; Rantsi, T.; Joki-Korpela, P.; Tiitinen, A.; Surcel, H.-M. Prevalence and persistence of Chlamydia trachomatis-specific antibodies after occasional and recurrent infections. Sex. Transm. Infect. 2020, 96, 277–282. [Google Scholar] [CrossRef] [PubMed]
- Hagemann, J.B.; Simnacher, U.; Longbottom, D.; Livingstone, M.; Maile, J.; Soutschek, E.; Walder, G.; Boden, K.; Sachse, K.; Essig, A. Analysis of Humoral Immune Responses to Surface and Virulence-Associated Chlamydia abortus Proteins in Ovine and Human Abortions by Use of a Newly Developed Line Immunoassay. J. Clin. Microbiol. 2016, 54, 1883–1890. [Google Scholar] [CrossRef]
- Palomares Reséndiz, E.G.; Mejía Sánchez, P.; Aguilar Romero, F.; Cruz Colín, L.D.L.; Jiménez Severiano, H.; Leyva Corona, J.C.; Morales Pablos, M.I.; Díaz Aparicio, E. Frecuencia y factores de riesgo asociados a la presencia de Chlamydia abortus, en rebaños ovinos en México. Rev. Mex. Cienc. Pecu. 2020, 11, 783–794. [Google Scholar] [CrossRef]
- Hernández-Trejo, M.; Herrera-González, N.; Guerra-Infante, F.M. Serological evidence of infection by three Chlamydia species in pregnant women. Ginecol. Obstet. Mex. 2014, 82, 585–590. [Google Scholar]
- Baud, D.; Regan, L.; Greub, G. Comparison of five commercial serological tests for the detection of anti-Chlamydia trachomatis antibodies. Eur. J. Clin. Microbiol. Infect. Dis. 2010, 29, 669–675. [Google Scholar] [CrossRef]
- Jones, C.S.; Maple, P.A.; Andrews, N.J.; Paul, I.D.; Caul, E.O. Measurement of IgG antibodies to Chlamydia trachomatis by commercial enzyme immunoassays and immunofluorescence in sera from pregnant women and patients with infertility, pelvic inflammatory disease, ectopic pregnancy, and laboratory diagnosed Chlamydia psittaci/Chlamydia pneumoniae infection. J. Clin. Pathol. 2003, 56, 225–229. [Google Scholar]
- Chu, J.; Yarrarapu, S.N.S.; Vaqar, S.; Durrani, M.I. Psittacosis. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2023. Available online: https://www.ncbi.nlm.nih.gov/books/NBK538305/ (accessed on 1 July 2025).
- Hou, L.; Jia, J.; Qin, X.; Fang, M.; Liang, S.; Deng, J.; Pan, B.; Zhang, X.; Wang, B.; Mao, C.; et al. Prevalence and genotypes of Chlamydia psittaci in birds and related workers in three cities of China. PLoS ONE. 2024, 19, e0308532. [Google Scholar] [CrossRef]
- Zhang, Z.; Zhou, H.; Cao, H.; Ji, J.; Zhang, R.; Li, W.; Guo, H.; Chen, L.; Ma, C.; Cui, M.; et al. Human-to-human transmission of Chlamydia psittaci in China, 2020: An epidemiological and aetiological investigation. Lancet Microbe 2022, 3, e512–e520. [Google Scholar] [CrossRef]
- Ortega, N.; Caro, M.R.; Gallego, M.C.; Murcia-Belmonte, A.; Álvarez, D.; Del Río, L.; Cuello, F.; Buendía, A.J.; Salinas, J. Isolation of Chlamydia abortus from a laboratory worker diagnosed with atypical pneumonia. Ir. Vet. J. 2015, 69, 8. [Google Scholar] [CrossRef] [PubMed]
- Walder, G.; Meusburger, H.; Hotzel, H.; Oehme, A.; Neunteufel, W.; Dierich, M.P.; Würzner, R. Chlamydophila abortus pelvic inflammatory disease. Emerg. Infect. Dis. 2003, 9, 1642–1644. [Google Scholar] [CrossRef] [PubMed]
- Longbottom, D.; Livingstone, M.; Ribeca, P.; Beeckman, D.S.A.; van der Ende, A.; Pannekoek, Y.; Vanrompay, D. Whole genome de novo sequencing and comparative genomic analyses suggests that Chlamydia psittaci strain 84/2334 should be reclassified as Chlamydia abortus species. BMC Genom. 2021, 22, 159. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).