
SARS-CoV-2 Variants of Concern and Clinical Severity in the Mexican Pediatric Population

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Data Sources
2.2. Variants of Concern High Predominance Estimation
2.3. Pediatric Severity Indicators
2.4. Statistical Analysis
3. Results
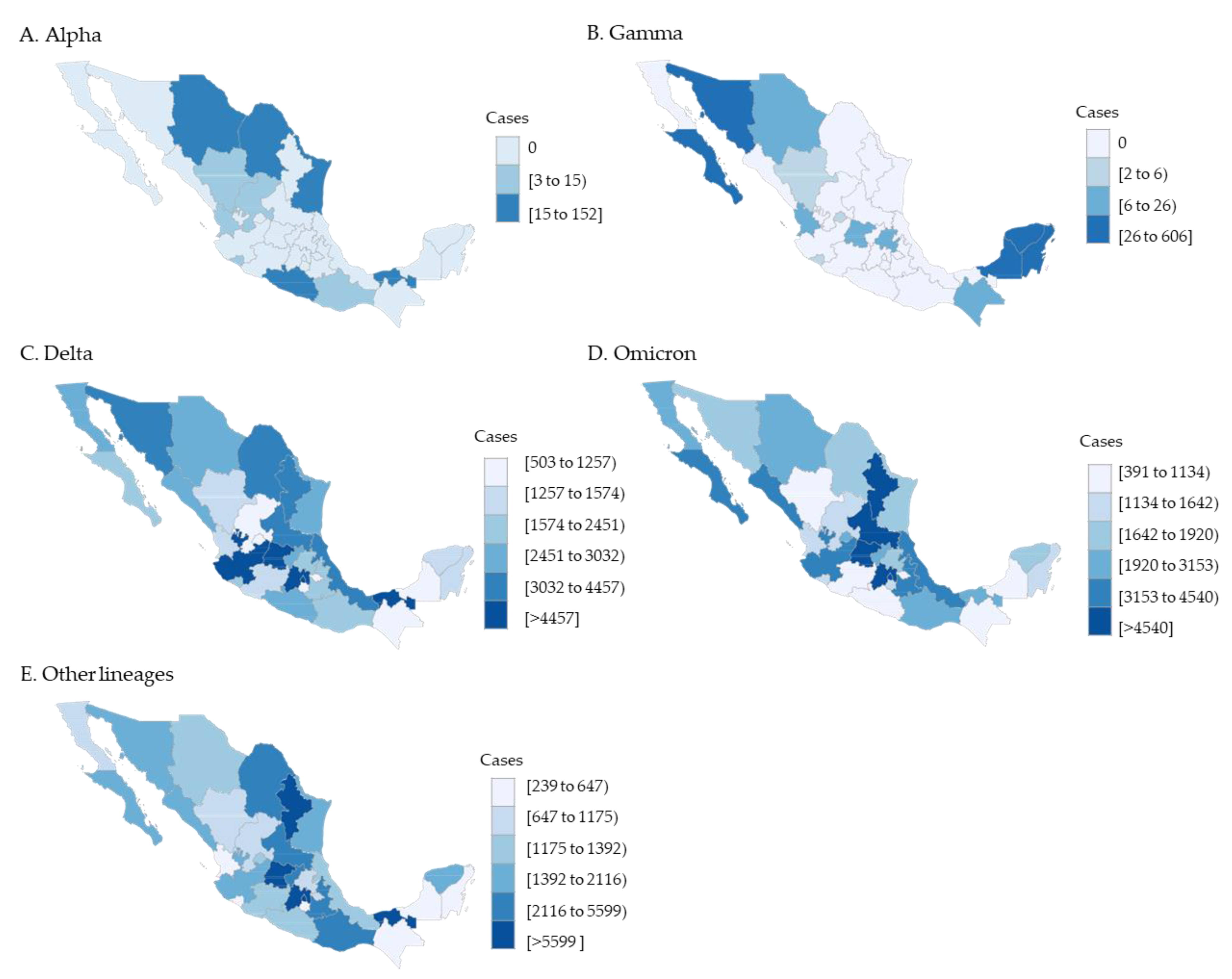
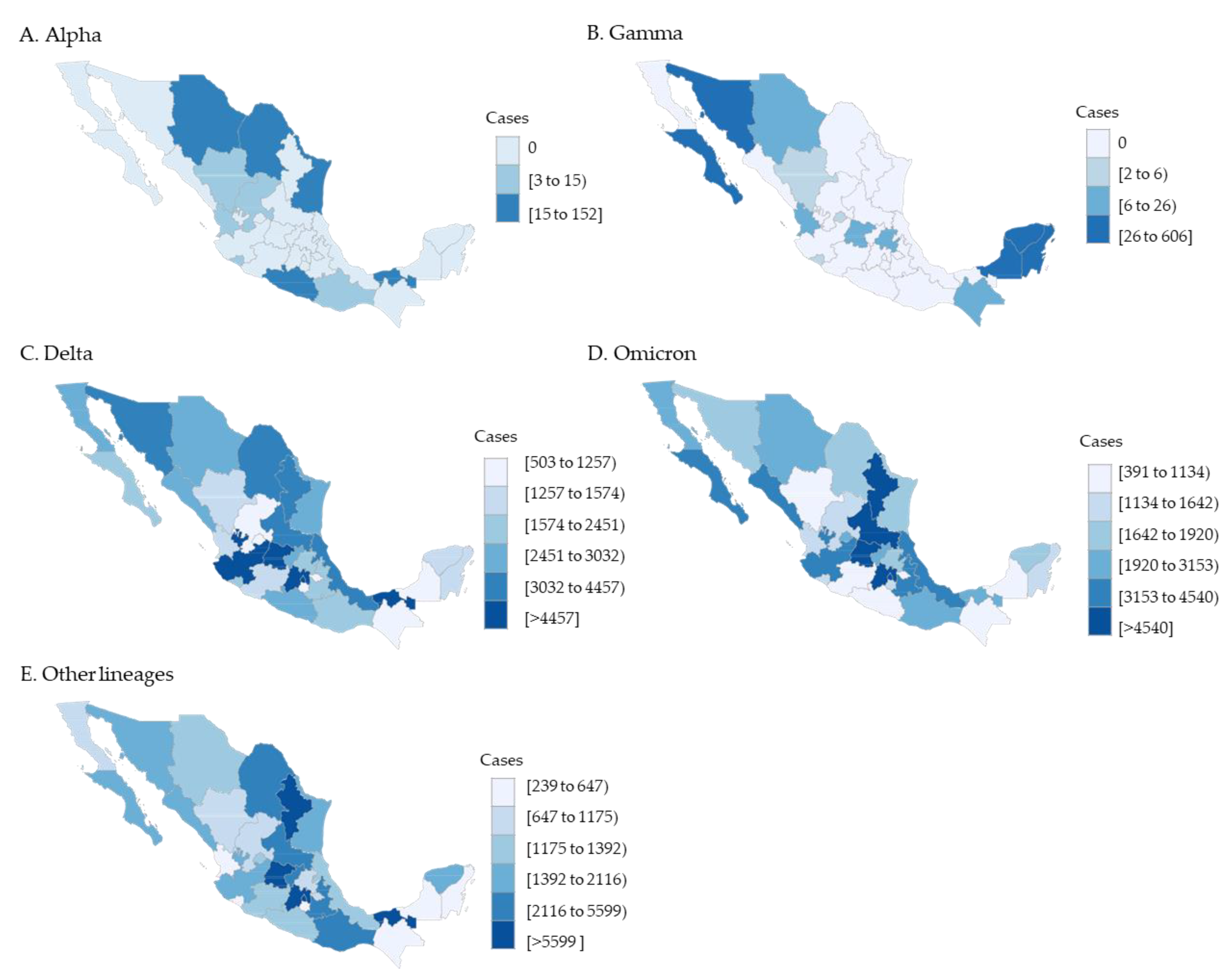
3.1. SARS-CoV-2 Sequence Results in the General Population
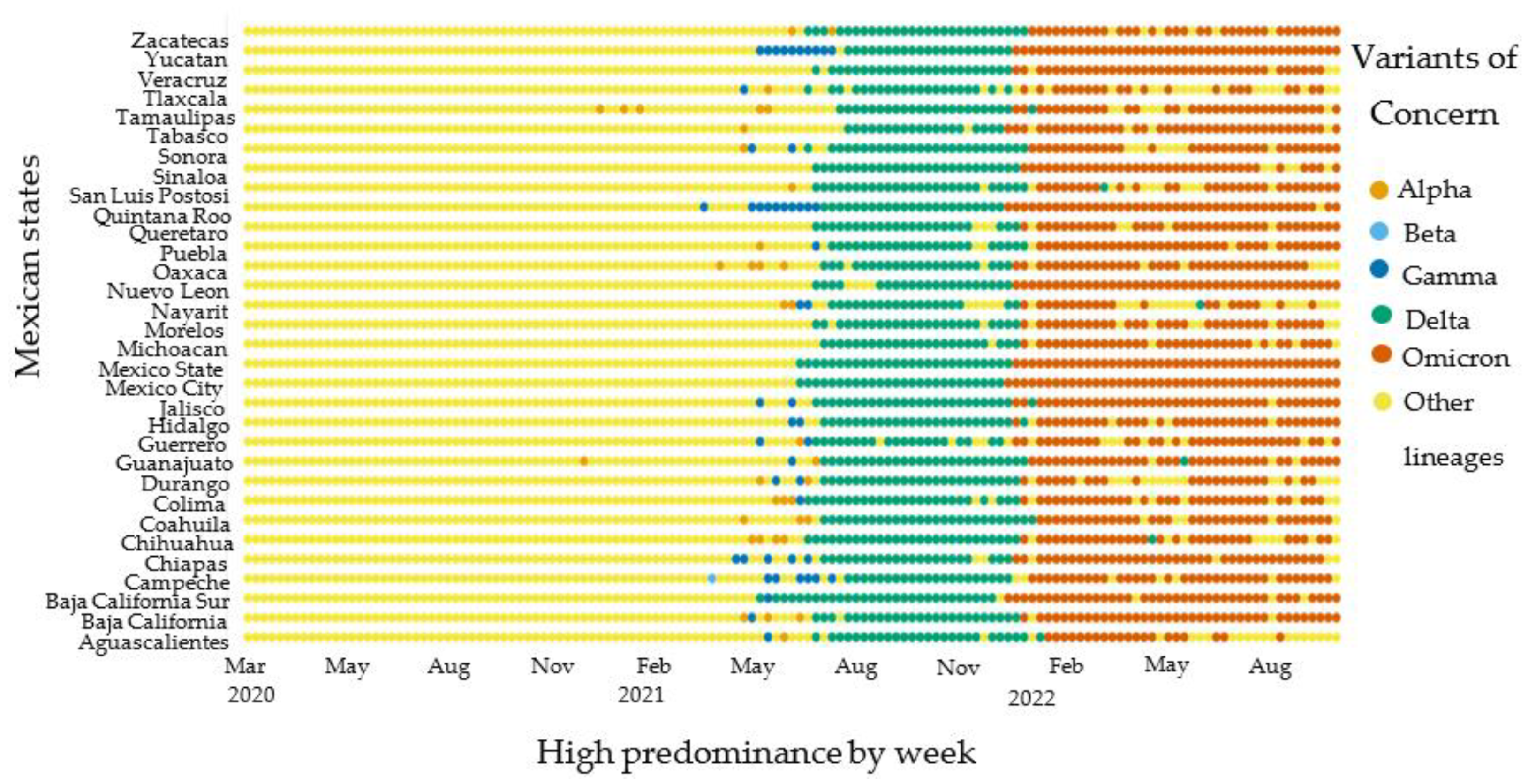
3.2. Variants of Concern High Predominance Circulation
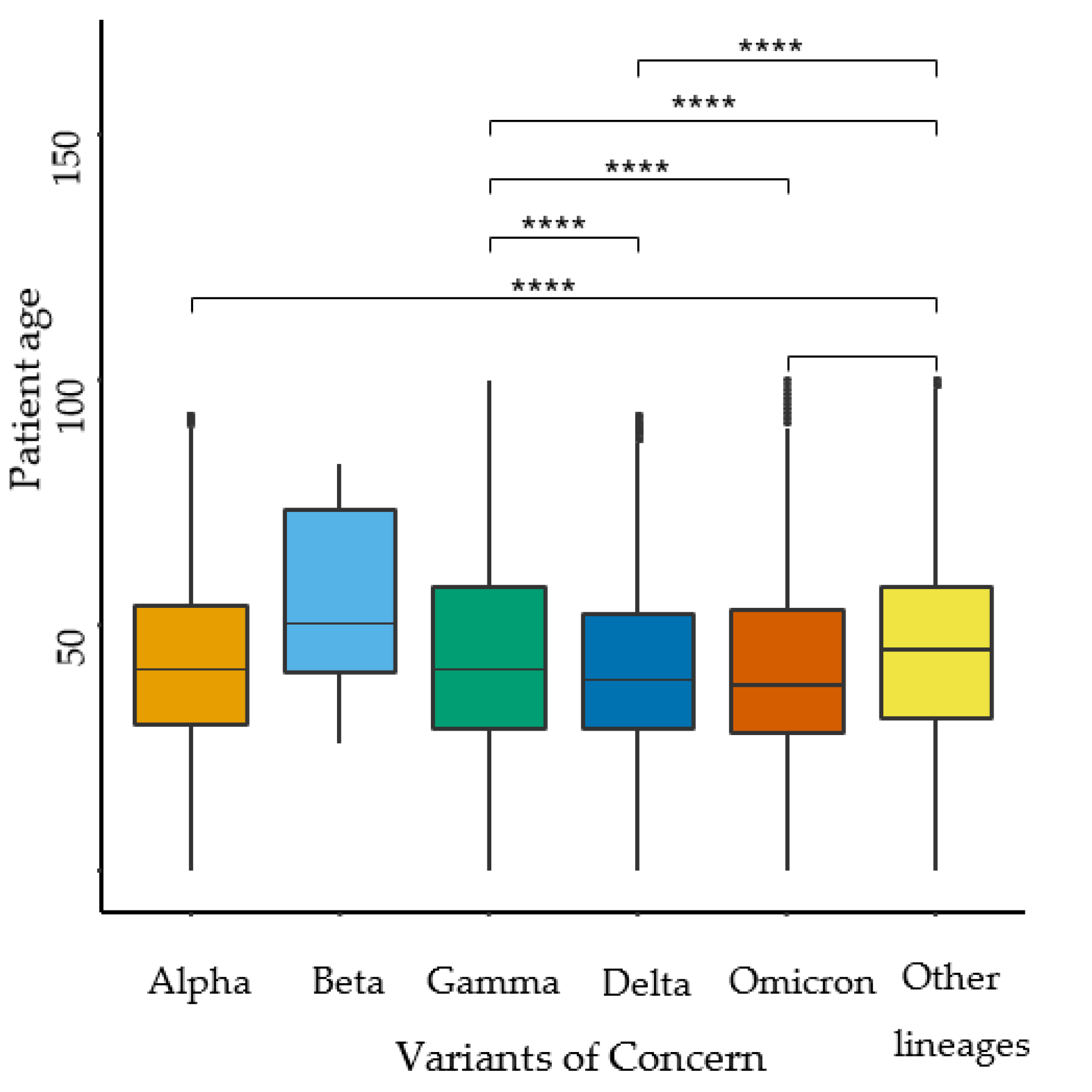
3.3. Pediatric Severity Outcomes
4. Discussion
Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Frenkel, L.D.; Gomez, F.; Bellanti, J.A. COVID-19 in children: Pathogenesis and current status. Allergy Asthma Proc. 2021, 42, 8–15. [Google Scholar] [CrossRef]
- Wu, F.; Zhao, S.; Yu, B.; Chen, Y.-M.; Wang, W.; Song, Z.-G.; Hu, Y.; Tao, Z.-W.; Tian, J.-H.; Pei, Y.-Y.; et al. A new coronavirus associated with human respiratory disease in China. Nature 2020, 579, 265–269. [Google Scholar] [CrossRef] [PubMed]
- van Dorp, L.; Acman, M.; Richard, D.; Shaw, L.P.; Ford, C.E.; Ormond, L.; Owen, C.J.; Pang, J.; Tan, C.C.S.; Boshier, F.A.T.; et al. Emergence of genomic diversity and recurrent mutations in SARS-CoV-2. Infect. Genet. Evol. 2020, 83, 104351. [Google Scholar] [CrossRef]
- Tosta, S.; Moreno, K.; Schuab, G.; Fonseca, V.; Segovia, F.M.C.; Kashima, S.; Elias, M.C.; Sampaio, S.C.; Ciccozzi, M.; Alcantara, L.C.J.; et al. Global SARS-CoV-2 genomic surveillance: What we have learned (so far). Infect. Genet. Evol. 2023, 108, 105405. [Google Scholar] [CrossRef]
- Hill, S.; Perkins, M.; von Eije, K.J.; Benschop, K.; Faria, N.R.; Golubchik, T.; Holmes, E.; Kafetzopoulou, L.; Lemey, P.; Minn Mak, T.; et al. Genomic Sequencing of SARS-CoV-2: A Guide to Implementation for Maximum Impact on Public Health; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- TAG-VE. Classification of Omicron (B.1.1.529): SARS-CoV-2 Variant of Concern; WHO: Geneva, Switzerland, 2021. [Google Scholar]
- Fontenele, R.S.; Kraberger, S.; Hadfield, J.; Driver, E.M.; Bowes, D.; Holland, L.A.; Faleye, T.O.C.; Adhikari, S.; Kumar, R.; Inchausti, R.; et al. High-throughput sequencing of SARS-CoV-2 in wastewater provides insights into circulating variants. Water Res. 2021, 205, 117710. [Google Scholar] [CrossRef]
- Sironi, M.; Hasnain, S.E.; Rosenthal, B.; Phan, T.; Luciani, F.; Shaw, M.-A.; Sallum, M.A.; Mirhashemi, M.E.; Morand, S.; González-Candelas, F. SARS-CoV-2 and COVID-19: A genetic, epidemiological, and evolutionary perspective. Infect. Genet. Evol. 2020, 84, 104384. [Google Scholar] [CrossRef]
- Shu, Y.; McCauley, J. GISAID: Global initiative on sharing all influenza data—From vision to reality. Euro Surveill. 2017, 22, 30494. [Google Scholar] [CrossRef]
- Marks, K.J.; Whitaker, M.; Anglin, O.; Milucky, J.; Patel, K.; Pham, H.; Chai, S.J.; Kirley, P.D.; Armistead, I.; McLafferty, S.; et al. Hospitalizations of Children and Adolescents with Laboratory-Confirmed COVID-19—COVID-NET, 14 States, July 2021–January 2022. MMWR Morb. Mortal Wkly. Rep. 2022, 71, 271–278. [Google Scholar] [CrossRef] [PubMed]
- Abuyadek, R.; Amirtharaj, F.; Al Marzooqi, S.; Mahmoud, S.; Al Hosani, F. Combined epidemiology and genetic sequencing surveillance in the era of COVID-19 pandemic; Abu Dhabi experience, United Arab Emirates. Infect. Genet. Evol. 2023, 109, 105–411. [Google Scholar] [CrossRef] [PubMed]
- Torres, C.; Nabaes Jodar, M.; Acuña, D.; Montaño, R.M.Z.; Culasso, A.C.A.; Amadio, A.F.; Aulicino, P.; Ceballos, S.; Cacciabue, M.; Debat, H.; et al. Omicron Waves in Argentina: Dynamics of SARS-CoV-2 Lineages BA.1, BA.2 and the Emerging BA.2.12.1 and BA.4/BA.5. Viruses 2023, 15, 312. [Google Scholar] [CrossRef]
- Liu, J.Q.; Xu, J.W.; Sun, C.Y.; Wang, J.N.; Wang, X.T.; Chen, X.; Gao, S.L. Age-stratified analysis of SARS-CoV-2 infection and case fatality rate in China, Italy, and South Korea. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 12575–12578. [Google Scholar] [CrossRef]
- Jiménez, D.; Torres Arias, M. Immunouniverse of SARS-CoV-2. Immunol. Med. 2022, 45, 186–224. [Google Scholar] [CrossRef]
- Williams, N.; Radia, T.; Harman, K.; Agrawal, P.; Cook, J.; Gupta, A. COVID-19 Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection in children and adolescents: A systematic review of critically unwell children and the association with underlying comorbidities. Eur. J. Pediatr. 2021, 180, 689–697. [Google Scholar] [CrossRef]
- Maldonado-Cabrera, A.; Angulo-Molina, A.; Haque, U.; Velazquez, C.; Álvarez-Villaseñor, A.S.; Santacruz-Gómez, K.J.; Gallego-Hernández, A.L. Acute Inflammatory Mediators in Young Adult Patients with COVID-19 in Mexico. Pathogens 2021, 10, 1056. [Google Scholar] [CrossRef]
- Secretaria de Salud. Vacuna COVID-19. Available online: https://vacunacovid.gob.mx/ (accessed on 16 October 2022).
- Castañeda, X. Migration and health between Mexico and the United States. Salud Publica Mex. 2013, 55, S447–S448. [Google Scholar]
- Chakraborty, I.; Maity, P. COVID-19 outbreak: Migration, effects on society, global environment and prevention. Sci. Total Environ. 2020, 728, 138–882. [Google Scholar] [CrossRef]
- Taboada, B.; Zárate, S.; Iša, P.; Boukadida, C.; Vazquez-Perez, J.A.; Muñoz-Medina, J.E.; Ramírez-González, J.E.; Comas-García, A.; Grajales-Muñiz, C.; Rincón-Rubio, A.; et al. Genetic Analysis of SARS-CoV-2 Variants in Mexico during the First Year of the COVID-19 Pandemic. Viruses 2021, 13, 2161. [Google Scholar] [CrossRef]
- Hernández-Huerta, M.T.; Pérez-Campos Mayoral, L.; Romero Díaz, C.; Martínez Cruz, M.; Mayoral-Andrade, G.; Sánchez Navarro, L.M.; Pina-Canseco, M.D.S.; Cruz Parada, E.; Martínez Cruz, R.; Pérez-Campos Mayoral, E.; et al. Analysis of SARS-CoV-2 mutations in Mexico, Belize, and isolated regions of Guatemala and its implication in the diagnosis. J. Med. Virol. 2021, 93, 2099–2114. [Google Scholar] [CrossRef] [PubMed]
- GISAID. Latin-America Phylodynamics GISAID. Available online: https://www.gisaid.org/phylodynamics/latin-america/ (accessed on 16 October 2022).
- Gozashti, L.; Corbett-Detig, R. Shortcomings of SARS-CoV-2 genomic metadata. BMC Res. Notes 2021, 14, 189. [Google Scholar] [CrossRef]
- Pilailuk, O. Reference Sequence Employed by GISAID (EPI_ISL_402124). Available online: https://gisaid.org/wiv04/ (accessed on 3 February 2022).
- WHO. Tracking SARS-CoV-2 Variants; WHO: Geneva, Switzerland, 2021. [Google Scholar]
- CDC. COVID Data Tracker Pediatric Data; CDC: Atlanta, GA, USA, 2023. [Google Scholar]
- Hazra, A.; Gogtay, N. Biostatistics Series Module 3: Comparing Groups: Numerical Variables. Indian J. Dermatol. 2016, 61, 251–260. [Google Scholar] [CrossRef]
- Tian, D.; Sun, Y.; Zhou, J.; Ye, Q. The Global Epidemic of the SARS-CoV-2 Delta Variant, Key Spike Mutations and Immune Escape. Front. Immunol. 2021, 12, 751778. [Google Scholar] [CrossRef]
- Winger, A.; Caspari, T. The Spike of Concern-The Novel Variants of SARS-CoV-2. Viruses 2021, 13, 1002. [Google Scholar] [CrossRef]
- Delahoy, M.J.; Ujamaa, D.; Whitaker, M.; O’Halloran, A.; Anglin, O.; Burns, E.; Cummings, C.; Holstein, R.; Kambhampati, A.K.; Milucky, J.; et al. Hospitalizations Associated with COVID-19 among Children and Adolescents—COVID-NET, 14 States, March 1, 2020–August 14, 2021. MMWR Morb. Mortal Wkly. Rep. 2021, 70, 1255–1260. [Google Scholar] [CrossRef]
- Siegel, D.A.; Reses, H.E.; Cool, A.J.; Shapiro, C.N.; Hsu, J.; Boehmer, T.K.; Cornwell, C.R.; Gray, E.B.; Henley, S.J.; Lochner, K.; et al. Trends in COVID-19 Cases, Emergency Department Visits, and Hospital Admissions among Children and Adolescents Aged 0–17 Years—United States, August 2020–August 2021. MMWR Morb. Mortal Wkly. Rep. 2021, 70, 1249–1254. [Google Scholar] [CrossRef]
- Bálint, G.; Vörös-Horváth, B.; Széchenyi, A. Omicron: Increased transmissibility and decreased pathogenicity. Signal Transduct. Target. Ther. 2022, 7, 151. [Google Scholar] [CrossRef] [PubMed]
- Cedro-Tanda, A.; Gómez-Romero, L.; Alcaraz, N.; de Anda-Jauregui, G.; Peñaloza, F.; Moreno, B.; Escobar-Arrazola, M.A.; Ramirez-Vega, O.A.; Munguia-Garza, P.; Garcia-Cardenas, F.; et al. The Evolutionary Landscape of SARS-CoV-2 Variant B.1.1.519 and Its Clinical Impact in Mexico City. Viruses 2021, 13, 2182. [Google Scholar] [CrossRef]
- Chintala, S.; Dutta, R.; Tadmor, D. COVID-19 spatiotemporal research with workflow-based data analysis. Infect. Genet. Evol. 2021, 88, 104–701. [Google Scholar] [CrossRef]
- Marks, K.J.; Whitaker, M.; Agathis, N.T.; Anglin, O.; Milucky, J.; Patel, K.; Pham, H.; Kirley, P.D.; Kawasaki, B.; Meek, J.; et al. Hospitalization of Infants and Children Aged 0–4 Years with Laboratory-Confirmed COVID-19—COVID-NET, 14 States, March 2020–February 2022. MMWR Morb. Mortal Wkly. Rep. 2022, 71, 429–436. [Google Scholar] [CrossRef]
- Grint, D.J.; Wing, K.; Houlihan, C.; Gibbs, H.P.; Evans, S.J.W.; Williamson, E.; McDonald, H.I.; Bhaskaran, K.; Evans, D.; Walker, A.J.; et al. Severity of Severe Acute Respiratory System Coronavirus 2 (SARS-CoV-2) Alpha Variant (B.1.1.7) in England. Clin. Infect. Dis. 2022, 75, e1120–e1127. [Google Scholar] [CrossRef]
- Pascall, D.J.; Vink, E.; Blacow, R.; Bulteel, N.; Campbell, A.; Campbell, R.; Clifford, S.; Davis, C.; da Silva Filipe, A.; Sakka, N.E.; et al. The SARS-CoV-2 Alpha variant is associated with increased clinical severity of COVID-19 in Scotland: A genomics-based retrospective cohort analysis. medRxiv 2022. [Google Scholar] [CrossRef]
- Bahl, A.; Mielke, N.; Johnson, S.; Desai, A.; Qu, L. Severe COVID-19 outcomes in pediatrics: An observational cohort analysis comparing Alpha, Delta, and Omicron variants. Lancet Reg. Health—Am. 2023, 18, 100–405. [Google Scholar] [CrossRef] [PubMed]
- Weinberger, D.M.; Cohen, T.; Crawford, F.W.; Mostashari, F.; Olson, D.; Pitzer, V.E.; Reich, N.G.; Russi, M.; Simonsen, L.; Watkins, A.; et al. Estimating the early death toll of COVID-19 in the United States. medRxiv 2020. [Google Scholar] [CrossRef]
- Woodruff, R.C.; Campbell, A.P.; Taylor, C.A.; Chai, S.J.; Kawasaki, B.; Meek, J.; Anderson, E.J.; Weigel, A.; Monroe, M.L.; Reeg, L.; et al. Risk Factors for Severe COVID-19 in Children. Pediatrics 2021, 149, e2021053418. [Google Scholar] [CrossRef]
- Xia, B.; Wang, Y.; Pan, X.; Cheng, X.; Ji, H.; Zuo, X.; Jiang, H.; Li, J.; Gao, Z. Why Is the SARS-CoV-2 Omicron variant milder? Innovation 2022, 3, 100251. [Google Scholar] [CrossRef] [PubMed]
- de Silva, T.I.; Liu, G.; Lindsey, B.B.; Dong, D.; Moore, S.C.; Hsu, N.S.; Shah, D.; Wellington, D.; Mentzer, A.J.; Angyal, A.; et al. The Impact of Viral Mutations on Recognition by SARS-CoV-2 Specific T Cells. iScience 2021, 24, 103353. [Google Scholar] [CrossRef] [PubMed]
- Koyama, T.; Parida, L. Identification of a Low Pathogenicity Clade of SARS-CoV-2. Preprints 2020. [Google Scholar] [CrossRef]
- Oulas, A.; Zanti, M.; Tomazou, M.; Zachariou, M.; Minadakis, G.; Bourdakou, M.M.; Pavlidis, P.; Spyrou, G.M. Generalized Linear Models Provide a Measure of Virulence for Specific Mutations in SARS-CoV-2 Strains. PLoS ONE 2020, 16, e0238665. [Google Scholar] [CrossRef]
- Hendy, M.; Kaufman, S.; Ponga, M. Molecular Strategies for Antibody Binding and Escape of SARS-CoV-2 and Its Mutations. Sci. Rep. 2021, 11, 21735. [Google Scholar] [CrossRef]
- Kumar, S.; Thambiraja, T.S.; Karuppanan, K.; Subramaniam, G. Omicron and Delta Variant of SARS-CoV-2: A Comparative Computational Study of Spike Protein. J. Med. Virol. 2022, 94, 1641–1649. [Google Scholar] [CrossRef]
- Kannan, S.R.; Spratt, A.N.; Sharma, K.; Chand, H.S.; Byrareddy, S.N.; Singh, K. Omicron SARS-CoV-2 Variant: Unique Features and Their Impact on Pre-Existing Antibodies. J. Autoimmun. 2022, 126, 102779. [Google Scholar] [CrossRef]
- Zhang, L.; Li, Q.; Wu, J.; Yu, Y.; Zhang, Y.; Nie, J.; Liang, Z.; Cui, Z.; Liu, S.; Wang, H.; et al. Analysis of SARS-CoV-2 Variants B.1.617: Host Tropism, Proteolytic Activation, Cell–Cell Fusion, and Neutralization Sensitivity. Emerg. Microbes Infect. 2022, 11, 1024–1036. [Google Scholar] [CrossRef]
- Wang, R.; Chen, J.; Hozumi, Y.; Yin, C.; Wei, G.-W. Emerging Vaccine-Breakthrough SARS-CoV-2 Variants. ACS Infect. Dis. 2022, 8, 546–556. [Google Scholar] [CrossRef] [PubMed]
- Joshi, M.; Kumar, M.; Srivastava, V.; Kumar, D.; Rathore, D.; Pandit, R.; Joshi, C.G. First Detection of SARS-CoV-2 Delta Variant (B.1.617.2) in the Wastewater of (Ahmedabad), India. MedRxiv 2021. MedRxiv: 2021.07.07.21260142. [Google Scholar]
- Chauhan, D.; Chakravarty, N.; Jeyachandran, A.V.; Jayakarunakaran, A.; Sinha, S.; Mishra, R.; Arumugaswami, V.; Ramaiah, A. In Silico Genome Analysis Reveals the Evolution and Potential Impact of SARS-CoV-2 Omicron Structural Changes on Host Immune Evasion and Antiviral Therapeutics. Viruses 2022, 14, 2461. [Google Scholar] [CrossRef] [PubMed]
- Mohammad, A.; Abubaker, J.; Al-Mulla, F. Structural Modelling of SARS-CoV-2 Alpha Variant (B.1.1.7) Suggests Enhanced Furin Binding and Infectivity. Virus Res. 2021, 303, 198522. [Google Scholar] [CrossRef]
- Voss, C.; Esmail, S.; Liu, X.; Knauer, M.J.; Ackloo, S.; Kaneko, T.; Lowes, L.; Stogios, P.; Seitova, A.; Hutchinson, A.; et al. Epitope-Specific Antibody Responses Differentiate COVID-19 Outcomes and Variants of Concern. JCI Insight 2021, 6, e148855. [Google Scholar] [CrossRef]
- Liu, Y.; Liu, J.; Johnson, B.A.; Xia, H.; Ku, Z.; Schindewolf, C.; Widen, S.G.; An, Z.; Weaver, S.C.; Menachery, V.D.; et al. Delta Spike P681R Mutation Enhances SARS-CoV-2 Fitness over Alpha Variant. bioRxiv 2021. bioRxiv: 2021.08.12.456173. [Google Scholar] [CrossRef]
- Chakravarty, N.; Senthilnathan, T.; Paiola, S.; Gyani, P.; Castillo Cario, S.; Urena, E.; Jeysankar, A.; Jeysankar, P.; Ignatius Irudayam, J.; Natesan Subramanian, S.; et al. Neurological Pathophysiology of SARS-CoV-2 and Pandemic Potential RNA Viruses: A Comparative Analysis. FEBS Lett. 2021, 595, 2854–2871. [Google Scholar] [CrossRef]
- Pastorio, C.; Zech, F.; Noettger, S.; Jung, C.; Jacob, T.; Sparrer, K.M.J.; Kirchhoff, F. Determinants of Spike Infectivity, Processing and Neutralization in SARS-CoV-2 Omicron Subvariants BA.1 and BA.2. Cell Host Microbe 2022, 30, 1255–1268.e5. [Google Scholar] [CrossRef]
- Maaroufi, H. The N764K and N856K Mutations in SARS-CoV-2 Omicron BA.1 S Protein Generate Potential Cleavage Sites for SKI-1/S1P Protease. bioRxiv 2022. bioRxiv:2022.01.21.477298. [Google Scholar]
- Alkhatib, M.; Salpini, R.; Carioti, L.; Ambrosio, F.A.; D’Anna, S.; Duca, L.; Costa, G.; Bellocchi, M.C.; Piermatteo, L.; Artese, A.; et al. Update on SARS-CoV-2 Omicron Variant of Concern and Its Peculiar Mutational Profile. Microbiol. Spectr. 2022, 10, e02732-21. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Gen/Mutation | Associated VOCs a | Pediatrics | Adults | p-Value b | ||
|---|---|---|---|---|---|---|
| n = 4965 | (%) | n = 71,873 | (%) | |||
| Envelope | ||||||
| T9I | ο | 2333 | (46.8) | 27,146 | (37.7) | <0.001 *** |
| Membrane | ||||||
| A63T | ο | 2342 | (47) | 27,195 | (37.8) | <0.001 *** |
| Q19E | ο | 2251 | (45.2) | 26,235 | (36.5) | <0.001 *** |
| Nucleocapsid | ||||||
| G204R | α ɣ ο | 2718 | (54.6) | 39,554 | (55) | 0.702 |
| R203K | α ɣ ο | 2716 | (54.5) | 39,650 | (55.1) | 0.534 |
| P13L | ο | 2346 | (47.1) | 27,374 | (38) | <0.001 *** |
| E31del | ο | 2293 | (46) | 26,228 | (36.4) | <0.001 *** |
| R32del | ο | 2293 | (46) | 26,235 | (36.5) | <0.001 *** |
| S33del | ο | 2266 | (45.5) | 25,892 | (36) | <0.001 *** |
| Spike | ||||||
| D614G | α β ɣ δ ο | 4911 | (98.7) | 71,072 | (98.8) | 0.916 |
| T478K | δ ο | 3795 | (76.2) | 51,975 | (72.3) | <0.001 *** |
| P681H | α ο | 2774 | (55.7) | 38,490 | (53.5) | <0.001 *** |
| G142D | ο | 2558 | (51.4) | 33,179 | (46.1) | <0.001*** |
| H655Y | ɣ ο | 2468 | (49.6) | 30,106 | (41.8) | <0.001 *** |
| L452R | δ ο | 2427 | (48.7) | 31,479 | (43.7) | <0.001 *** |
| N679K | ο | 2354 | (47.3) | 27,299 | (37.9) | <0.001 *** |
| N969K | ο | 2348 | (47.1) | 27,212 | (37.8) | <0.001 *** |
| Q954H | ο | 2346 | (47.1) | 27,212 | (37.8) | <0.001 *** |
| D796Y | ο | 2318 | (46.5) | 26,947 | (37.4) | <0.001 *** |
| N764K | ο | 2256 | (45.3) | 26,103 | (36.3) | <0.001 *** |
| G339D | ο | 2249 | (45.2) | 25,919 | (36) | <0.001 *** |
| T95I | ο | 2162 | (43.4) | 27,023 | (37.5) | <0.001 *** |
| S375F | ο | 2104 | (42.2) | 24,058 | (33.4) | <0.001 *** |
| S373P | ο | 2068 | (41.5) | 23,687 | (32.9) | <0.001 *** |
| N501Y | α β ɣ ο | 2013 | (40.4) | 26,458 | (36.8) | <0.001 *** |
| Alpha | Gamma | Delta | Omicron | Other Lineages | p-Value | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| n Mean | % (SD) | n Mean | % (SD) | n Mean | % (SD) | n Mean | % (SD) | n Mean | % (SD) | ||
| Age | <0.001 a | ||||||||||
| Mean (SD) | 11.83 (±5.07) | 11.61 (±4.95) | 11.19 (±4.88) | 10.33 (±4.88) | 11.45 (±5.0) | ||||||
| Sex | <0.001 b | ||||||||||
| Female | 213 | 53% | 551 | 47% | 60,396 | 50% | 77,291 | 49% | 45,455 | 49% | |
| Male | 191 | 47% | 622 | 53% | 60,403 | 50% | 81,418 | 51% | 46,399 | 51% | |
| Social | |||||||||||
| Ethnicity | 9 | 2% | 47 | 4% | 1662 | 1% | 1275 | 1% | 1004 | 1% | |
| Adolescent pregnancy | 2 | 0% | 5 | 0% | 578 | 0% | 531 | 0% | 355 | 0% | |
| Clinical outcomes | <0.001 b | ||||||||||
| Ambulatory | 344 | 91% | 1134 | 95% | 116,139 | 96% | 117,971 | 96% | 89,517 | 94% | |
| Hospitalized | 31 | 8% | 52 | 4% | 3978 | 3% | 4532 | 4% | 5,341 | 6% | |
| Death | 3 | 1% | 2 | 0% | 321 | 0% | 224 | 0% | 654 | 1% | |
| ICU/AMV | 4 | 1% | 4 | 0% | 368 | 0% | 343 | 0% | 1050 | 1% | <0.01 b |
| Infants | 0 | 0% | 2 | 50% | 162 | 44% | 176 | 51% | 618 | 59% | <0.001 b |
| Preschoolers | 0 | 0% | 0 | 0% | 24 | 7% | 48 | 14% | 66 | 6% | |
| Children | 0 | 0% | 1 | 25% | 51 | 14% | 46 | 13% | 144 | 14% | |
| Adolescents | 4 | 100% | 1 | 25% | 131 | 36% | 73 | 21% | 222 | 21% | |
| 7-Day Hospitalization Rate | 0.11 | (±0.14) | 0.29 | (±0.44) | 12.6 | (±41) | 16.4 | (±44) | 3.16 | (±13) | <0.001 a |
| Case Fatality Rate | 3 | 0.495 | 2 | 0.170 | 330 | 0.273 | 240 | 0.151 | 650 | 0.707 | <0.001 b |
| Early mortality rate (<28 days) | 3 | 100% | 2 | 100% | 283 | 88% | 205 | 92% | 605 | 93% | <0.001 b |
| Model | Hospitalization | ICU/AMV | Deaths | ||||||
|---|---|---|---|---|---|---|---|---|---|
| IRR a | 95% CI | p-Value | IRR a | 95% CI | p-Value | IRR a | 95% CI | p-Value | |
| VOCs | |||||||||
| Other lineages | — | — | — | — | — | — | |||
| Alpha | 1.69 | 1.54, 1.86 | <0.001 | 1.67 | 1.52, 1.84 | <0.001 | 1.68 | 1.52, 1.85 | <0.001 |
| Delta | 0.97 | 0.96, 0.98 | <0.001 | 0.99 | 0.98, 1.00 | 0.004 | 0.99 | 0.98, 1.00 | 0.049 |
| Gamma | 2.67 | 2.52, 2.82 | <0.001 | 2.69 | 2.54, 2.85 | <0.001 | 2.7 | 2.54, 2.85 | <0.001 |
| Omicron | 0.95 | 0.94, 0.96 | <0.001 | 0.97 | 0.96, 0.97 | <0.001 | 0.97 | 0.96, 0.98 | <0.001 |
| Age category | |||||||||
| Adolescent | — | — | — | — | — | — | |||
| Infant | 1.27 | 1.25, 1.28 | <0.001 | 1.12 | 1.10, 1.13 | <0.001 | 1.10 | 1.09, 1.11 | <0.001 |
| Preschool | 1.10 | 1.09, 1.11 | <0.001 | 1.06 | 1.04, 1.07 | <0.001 | 1.06 | 1.04, 1.07 | <0.001 |
| Child | 1.03 | 1.02, 1.04 | <0.001 | 1.02 | 1.02, 1.03 | <0.001 | 1.02 | 1.02, 1.03 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maldonado-Cabrera, A.; Colin-Vilchis, J.A.; Haque, U.; Velazquez, C.; Alvarez Villaseñor, A.S.; Magdaleno-Márquez, L.E.; Calleros-Muñoz, C.I.; Figueroa-Enríquez, K.F.; Angulo-Molina, A.; Gallego-Hernández, A.L. SARS-CoV-2 Variants of Concern and Clinical Severity in the Mexican Pediatric Population. Infect. Dis. Rep. 2023, 15, 535-548. https://doi.org/10.3390/idr15050053
Maldonado-Cabrera A, Colin-Vilchis JA, Haque U, Velazquez C, Alvarez Villaseñor AS, Magdaleno-Márquez LE, Calleros-Muñoz CI, Figueroa-Enríquez KF, Angulo-Molina A, Gallego-Hernández AL. SARS-CoV-2 Variants of Concern and Clinical Severity in the Mexican Pediatric Population. Infectious Disease Reports. 2023; 15(5):535-548. https://doi.org/10.3390/idr15050053
Chicago/Turabian StyleMaldonado-Cabrera, Anahí, Jesus Alejandro Colin-Vilchis, Ubydul Haque, Carlos Velazquez, Andrea Socorro Alvarez Villaseñor, Luis Eduardo Magdaleno-Márquez, Carlos Iván Calleros-Muñoz, Karen Fernanda Figueroa-Enríquez, Aracely Angulo-Molina, and Ana Lucía Gallego-Hernández. 2023. "SARS-CoV-2 Variants of Concern and Clinical Severity in the Mexican Pediatric Population" Infectious Disease Reports 15, no. 5: 535-548. https://doi.org/10.3390/idr15050053
APA StyleMaldonado-Cabrera, A., Colin-Vilchis, J. A., Haque, U., Velazquez, C., Alvarez Villaseñor, A. S., Magdaleno-Márquez, L. E., Calleros-Muñoz, C. I., Figueroa-Enríquez, K. F., Angulo-Molina, A., & Gallego-Hernández, A. L. (2023). SARS-CoV-2 Variants of Concern and Clinical Severity in the Mexican Pediatric Population. Infectious Disease Reports, 15(5), 535-548. https://doi.org/10.3390/idr15050053