
Vaccine Hesitancy towards COVID-19 Vaccination: Investigating the Role of Information Sources through a Mediation Analysis




Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Data Collection
2.2. Questionnaire
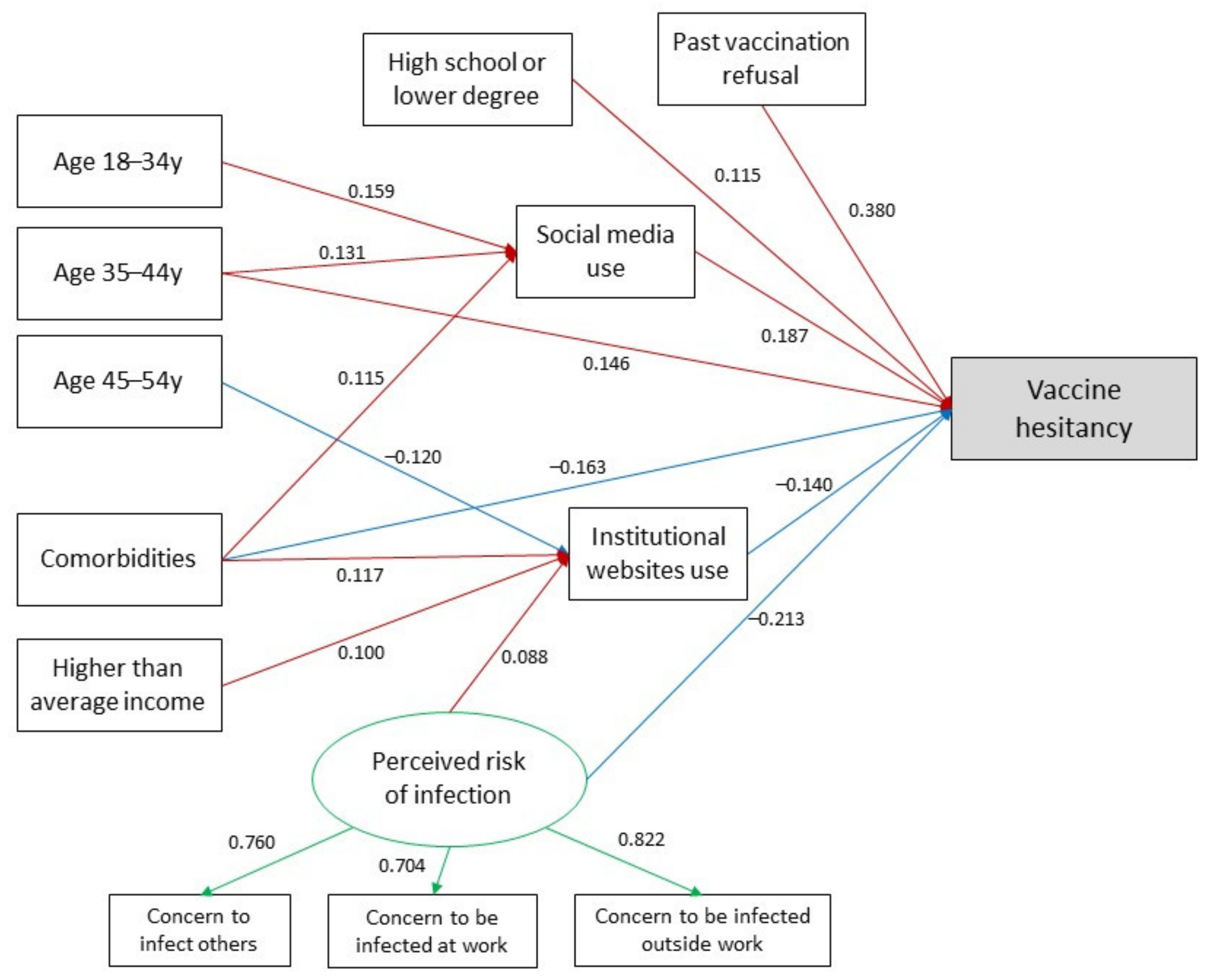
2.3. Theoretical Model
2.4. Statistical Analysis
3. Results
3.1. Sample Characteristics and Association between Information Source Use and Vaccine Hesitancy
3.2. Mediation Analysis
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Haas, E.J.; Angulo, F.J.; McLaughlin, J.M.; Anis, E.; Singer, S.R.; Khan, F.; Brooks, N.; Smaja, M.; Mircus, G.; Pan, K.; et al. Impact and Effectiveness of MRNA BNT162b2 Vaccine against SARS-CoV-2 Infections and COVID-19 Cases, Hospitalisations, and Deaths Following a Nationwide Vaccination Campaign in Israel: An Observational Study Using National Surveillance Data. Lancet 2021, 397, 1819–1829. [Google Scholar] [CrossRef]
- Bernal, J.L.; Andrews, N.; Gower, C.; Robertson, C.; Stowe, J.; Tessier, E.; Simmons, R.; Cottrell, S.; Roberts, R.; O’Doherty, M.; et al. Effectiveness of the Pfizer-BioNTech and Oxford-AstraZeneca Vaccines on COVID-19 Related Symptoms, Hospital Admissions, and Mortality in Older Adults in England: Test Negative Case-Control Study. BMJ 2021, 373, n1088. [Google Scholar] [CrossRef]
- CDCMMWR. COVID-19 Vaccine Breakthrough Infections Reported to CDC—United States, 1 January–30 April 2021. Morb. Mortal. Wkly. Rep. 2021, 70, 792–793. [Google Scholar] [CrossRef] [PubMed]
- Aschwanden, C. Five Reasons Why COVID Herd Immunity Is Probably Impossible. Nature 2021, 591, 520–522. [Google Scholar] [CrossRef] [PubMed]
- Nelson, M.C.; Rogers, J. The Right to Die? Anti-Vaccination Activity and the 1874 Smallpox Epidemic in Stockholm. Soc. Hist. Med. 1992, 5, 369–388. [Google Scholar] [CrossRef] [PubMed]
- Cooper, S.; Betsch, C.; Sambala, E.Z.; Mchiza, N.; Wiysonge, C.S. Vaccine Hesitancy—A Potential Threat to the Achievements of Vaccination Programmes in Africa. Hum. Vaccines Immunother. 2018, 14, 2355–2357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Measles. Available online: https://www.nhs.uk/conditions/measles/ (accessed on 24 June 2021).
- CDC. Measles Cases and Outbreaks. Available online: https://www.cdc.gov/measles/cases-outbreaks.html (accessed on 24 June 2021).
- Ten Health Issues WHO Will Tackle This Year—World Health Organization. Available online: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019 (accessed on 24 June 2021).
- MacDonald, N.E. Vaccine Hesitancy: Definition, Scope and Determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- Razai, M.S.; Oakeshott, P.; Esmail, A.; Wiysonge, C.S.; Viswanath, K.; Mills, M.C. COVID-19 Vaccine Hesitancy: The Five Cs to Tackle Behavioural and Sociodemographic Factors. J. R. Soc. Med. 2021, 114, 295–298. [Google Scholar] [CrossRef]
- Del Riccio, M.; Boccalini, S.; Rigon, L.; Biamonte, M.A.; Albora, G.; Giorgetti, D.; Bonanni, P.; Bechini, A. Factors Influencing SARS-CoV-2 Vaccine Acceptance and Hesitancy in a Population-Based Sample in Italy. Vaccines 2021, 9, 633. [Google Scholar] [CrossRef] [PubMed]
- Sallam, M.; Dababseh, D.; Eid, H.; Al-Mahzoum, K.; Al-Haidar, A.; Taim, D.; Yaseen, A.; Ababneh, N.A.; Bakri, F.G.; Mahafzah, A. High Rates of COVID-19 Vaccine Hesitancy and Its Association with Conspiracy Beliefs: A Study in Jordan and Kuwait among Other Arab Countries. Vaccines 2021, 9, 42. [Google Scholar] [CrossRef]
- Al-Mohaithef, M.; Padhi, B.K. Determinants of COVID-19 Vaccine Acceptance in Saudi Arabia: A Web-Based National Survey. J. Multidiscip. Healthc. 2020, 13, 1657–1663. [Google Scholar] [CrossRef]
- Larson, H.; Paterson, P.B.; Erondu, N. The Globalization of Risk and Risk Perception. SpringerLink. Available online: https://link.springer.com/article/10.1007/BF03261991 (accessed on 24 June 2021).
- Larson, H.J.; Jarrett, C.; Eckersberger, E.; Smith, D.M.D.; Paterson, P. Understanding Vaccine Hesitancy around Vaccines and Vaccination from a Global Perspective: A Systematic Review of Published Literature, 2007–2012. Vaccine 2014, 32, 2150–2159. [Google Scholar] [CrossRef]
- Reno, C.; Maietti, E.; Fantini, M.P.; Savoia, E.; Manzoli, L.; Montalti, M.; Gori, D. Enhancing COVID-19 Vaccines Acceptance: Results from a Survey on Vaccine Hesitancy in Northern Italy. Vaccines 2021, 9, 378. [Google Scholar] [CrossRef]
- COVID-19 Vaccine Hesitancy in a Representative Working-Age Population in France: A Survey Experiment Based on Vaccine Characteristics—The Lancet Public Health. Available online: https://www.thelancet.com/journals/lanpub/article/PIIS2468-2667(21)00012-8/fulltext (accessed on 24 June 2021).
- Razai, M.S.; Chaudhry, U.A.R.; Doerholt, K.; Bauld, L.; Majeed, A. COVID-19 Vaccination Hesitancy. BMJ 2021, 373, n1138. [Google Scholar] [CrossRef]
- Puri, N.; Coomes, E.; Haghbayan, H.; Gunaratne, K. Social media and vaccine hesitancy: New updates for the era of COVID-19 and globalized infectious diseases. Hum. Vaccines Immunother. 2020, 16, 2586–2593. [Google Scholar] [CrossRef] [PubMed]
- Vraga, E.K.; Bode, L. Using Expert Sources to Correct Health Misinformation in Social Media. Sci. Commun. 2017, 39, 621–645. [Google Scholar] [CrossRef]
- Mcbrien, J.; Murphy, J.; Gill, D.; Cronin, M.; O’donovan, C.; Cafferkey, M.T. Measles Outbreak in Dublin, 2000. Pediatr. Infect. Dis. J. 2003, 22, 580–584. [Google Scholar] [CrossRef] [PubMed]
- Dobson, R. Media misled the public over the MMR vaccine. BMJ 2003, 326, 1107. [Google Scholar] [CrossRef] [Green Version]
- Speers, T.; Lewis, J. Journalists and Jabs: Media Coverage of the MMR Vaccine. Commun. Med. 2004, 1, 171–181. [Google Scholar] [CrossRef] [PubMed]
- Simione, L.; Vagni, M.; Gnagnarella, C.; Bersani, G.; Pajardi, D. Mistrust and Beliefs in Conspiracy Theories Differently Mediate the Effects of Psychological Factors on Propensity for COVID-19 Vaccine. Front. Psychol. 2021, 12, 683684. [Google Scholar] [CrossRef]
- Shearer, E.; Mitchell, A. News Use across Social Media Platforms in 2020; Pew Research Center: Washington, DC, USA, 2021. [Google Scholar]
- Tang, L.; Bie, B.; Park, S.-E.; Zhi, D. Social Media and Outbreaks of Emerging Infectious Diseases: A Systematic Review of Literature. Am. J. Infect. Control 2018, 46, 962–972. [Google Scholar] [CrossRef]
- Marcelin, J.R.; Cortés-Penfield, N.; Del Rio, C.; Desai, A.; Echenique, I.; Granwehr, B.; Lawal, F.; Kuriakose, K.; Lee, D.H.; Malinis, M.; et al. How the Field of Infectious Diseases Can Leverage Digital Strategy and Social Media Use During a Pandemic. Open Forum Infect. Dis. 2021, 8, ofab027. [Google Scholar] [CrossRef] [PubMed]
- Sooknanan, J.; Comissiong, D.M.G. Trending on Social Media: Integrating Social Media into Infectious Disease Dynamics. Bull Math. Biol. 2020, 82, 86. [Google Scholar] [CrossRef]
- Al-Surimi, K.; Khalifa, M.; Bahkali, S.; El-Metwally, A.; Househ, M. The Potential of Social Media and Internet-Based Data in Preventing and Fighting Infectious Diseases: From Internet to Twitter. Adv. Exp. Med. Biol. 2017, 972, 131–139. [Google Scholar] [CrossRef]
- Marzouki, Y.; Aldossari, F.S.; Veltri, G.A. Understanding the Buffering Effect of Social Media Use on Anxiety during the COVID-19 Pandemic Lockdown. Humanit. Soc. Sci. Commun. 2021, 8, 47. [Google Scholar] [CrossRef]
- Pollett, S.; Rivers, C. Social Media and the New World of Scientific Communication During the COVID-19 Pandemic. Clin. Infect. Dis. 2020, 71, 2184–2186. [Google Scholar] [CrossRef]
- Larson, H.J.; Cooper, L.Z.; Eskola, J.; Katz, S.L.; Ratzan, S. Addressing the vaccine confidence gap. Lancet 2011, 378, 526–535. [Google Scholar] [CrossRef]
- Basch, C.H.; Zybert, P.; Reeves, R.; Basch, C.E. What Do Popular YouTubeTM Videos Say about Vaccines? Child Care Health Dev. 2017, 43, 499–503. [Google Scholar] [CrossRef] [PubMed]
- Blankenship, E.B.; Goff, M.E.; Yin, J.; Tse, Z.T.H.; Fu, K.-W.; Liang, H.; Saroha, N.; Fung, I.C.-H. Sentiment, Contents, and Retweets: A Study of Two Vaccine-Related Twitter Datasets. Perm. J. 2018, 22, 17–138. [Google Scholar] [CrossRef] [PubMed]
- Betsch, C.; Renkewitz, F.; Betsch, T.; Ulshöfer, C. The influence of vaccine-critical websites on perceiving vaccination risks. J. Health Psychol. 2010, 15, 446–455. [Google Scholar] [CrossRef]
- Nan, X.; Madden, K. HPV vaccine information in the blogosphere: How positive and negative blogs influence vaccine-related risk perceptions, attitudes, and behavioral intentions. Health Commun. 2012, 27, 829–836. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, N.; Quinn, S.C.; Hancock, G.R.; Freimuth, V.S.; Jamison, A. Social media use and influenza vaccine uptake among White and African American adults. Vaccine 2018, 36, 7556–7561. [Google Scholar] [CrossRef] [PubMed]
- Wilson, S.L.; Wiysonge, C. Social Media and Vaccine Hesitancy. BMJ Global Health 2020, 5, e004206. [Google Scholar] [CrossRef] [PubMed]
- Piltch-Loeb, R.; Savoia, E.; Goldberg, B.; Hughes, B.; Verhey, T.; Kayyem, J.; Miller-Idriss, C.; Testa, M. Examining the effect of information channel on COVID-19 vaccine acceptance. PLoS ONE 2021, 16, e0251095. [Google Scholar] [CrossRef]
- Rosseel, Y. lavaan: An R Package for Structural Equation Modeling. J. Stat. Softw. 2012, 48, 1–36. [Google Scholar] [CrossRef] [Green Version]
- McDonald, R.P.; Ho, M.H. Principles and practice in reporting structural equation analyses. Psychol. Methods 2002, 7, 64–82. [Google Scholar] [CrossRef] [PubMed]
- Kline, R. Principles and Practice of Structural Equation Modeling, 4th ed.; The Guilford Press: New York, NY, USA, 2015; pp. 273–278. [Google Scholar]
- Jordan, R.E.; Adab, P.; Cheng, K.K. COVID-19: Risk Factors for Severe Disease and Death. BMJ 2020, 368, m1198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGurnaghan, S.J.; Weir, A.; Bishop, J.; Kennedy, S.; Blackbourn, L.A.K.; McAllister, D.A.; Hutchinson, S.; Caparrotta, T.M.; Mellor, J.; Jeyam, A.; et al. Risks of and Risk Factors for COVID-19 Disease in People with Diabetes: A Cohort Study of the Total Population of Scotland. Lancet Diabetes Endocrinol. 2021, 9, 82–93. [Google Scholar] [CrossRef]
- Gerayeli, F.V.; Milne, S.; Cheung, C.; Li, X.; Yang, C.W.T.; Tam, A.; Choi, L.H.; Bae, A.; Sin, D.D. COPD and the Risk of Poor Outcomes in COVID-19: A Systematic Review and Meta-Analysis. EClinicalMedicine 2021, 33, 100789. [Google Scholar] [CrossRef]
- Guaraldi, F.; Montalti, M.; Di Valerio, Z.; Mannucci, E.; Nreu, B.; Monami, M.; Gori, D. Rate and Predictors of Hesitancy toward SARS-CoV-2 Vaccine among Type 2 Diabetic Patients: Results from an Italian Survey. Vaccines 2021, 9, 460. [Google Scholar] [CrossRef]
- Freeman, D.; Loe, B.S.; Chadwick, A.; Vaccari, C.; Waite, F.; Rosebrock, L.; Jenner, L.; Petit, A.; Lewandowsky, S.; Vanderslott, S.; et al. COVID-19 Vaccine Hesitancy in the UK: The Oxford Coronavirus Explanations, Attitudes, and Narratives Survey (Oceans) II. Psychol. Med. 2020, 1–15. [Google Scholar] [CrossRef]
- Descamps, A.; Launay, O.; Bonnet, C.; Blondel, B. Seasonal Influenza Vaccine Uptake and Vaccine Refusal among Pregnant Women in France: Results from a National Survey. Hum. Vaccines Immunother. 2020, 16, 1093–1100. [Google Scholar] [CrossRef]
- Montalti, M.; Rallo, F.; Guaraldi, F.; Bartoli, L.; Po, G.; Stillo, M.; Perrone, P.; Squillace, L.; Dallolio, L.; Pandolfi, P.; et al. Would Parents Get Their Children Vaccinated Against SARS-CoV-2? Rate and Predictors of Vaccine Hesitancy According to a Survey over 5000 Families from Bologna, Italy. Vaccines 2021, 9, 366. [Google Scholar] [CrossRef]
- Bertoncello, C.; Ferro, A.; Fonzo, M.; Zanovello, S.; Napoletano, G.; Russo, F.; Baldo, V.; Cocchio, S. Socioeconomic Determinants in Vaccine Hesitancy and Vaccine Refusal in Italy. Vaccines 2020, 8, 276. [Google Scholar] [CrossRef] [PubMed]
- Costantino, C.; Gori, D.; Alba, D.; Cimino, L.; Conforto, A.; Tomasello, F.; Rallo, F.; Mauro, G.L.; Vitale, F.; Mazzucco, W. Willingness to receive covid-19 vaccination in costumers accessing community pharmacies in the province of Palermo, Italy. EuroMediterr. Biomed. J. 2021, 16, 80–84. [Google Scholar] [CrossRef]
- Steinborn, M.B.; Langner, R.; Flehmig, H.C.; Huestegge, L. Methodology of Performance Scoring in the D2 Sustained-Attention Test: Cumulative-Reliability Functions and Practical Guidelines. Psychol. Assess. 2018, 30, 339–357. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control. Utilising Social Media to Support HIV/STI Prevention: Evidence to Inform a Handbook for Public Health Programme Managers; ECDC: Stockholm, Sweden, 2017.
- Updates to Our Work on COVID-19 Vaccine Misinformation. Available online: https://blog.twitter.com/en_us/topics/company/2021/updates-to-our-work-on-covid-19-vaccine-misinformation (accessed on 27 June 2021).
- Helping People Stay Safe and Informed about COVID-19 Vaccines|Instagram Blog. Available online: https://about.instagram.com/blog/announcements/continuing-to-keep-people-safe-and-informed-about-covid-19 (accessed on 27 June 2021).

{kind=link}
| Characteristics | N (%) |
|---|---|
| Gender | |
| Male | 453(44.8) |
| Female | 558 (55.2) |
| Age (years) | |
| 18–34 | 154 (15.2) |
| 35–44 | 271 (26.8) |
| 45–54 | 314 (31.1) |
| ≥55 | 272 (26.9) |
| Education | |
| High school or lower degree | 642 (63.5) |
| Bachelor’s or higher degree | 369 (36.5) |
| Family income | |
| Higher than average | 104 (10.3) |
| On average | 591 (58.5) |
| Lower than average | 316 (31.3) |
| Comorbidities | |
| No | 724 (71.6) |
| One or more | 287 (28.4) |
| Past vaccination refusal | |
| No | 853 (84.4) |
| Yes | 158 (15.6) |
| Concern about contracting COVID-19 at work | |
| Not at all | 182 (18.0) |
| A little | 308 (30.5) |
| Somewhat | 346 (34.2) |
| Very concerned | 175 (17.3) |
| Concern about contracting COVID-19 outside of work | |
| Not at all | 88 (8.7) |
| A little | 298 (29.5) |
| Somewhat | 434 (42.9) |
| Very concerned | 191 (18.9) |
| Concern about infecting family or friends with COVID-19 | |
| Not at all | 56 (5.5) |
| A little | 151 (14.9) |
| Somewhat | 376 (37.2) |
| Very concerned | 428 (42.3) |
| COVID-19 vaccine hesitancy | |
| No | 697 (68.9) |
| Yes | 314 (31.1) |
| Source | Users N (%) | Hesitant Users N (%) | p-Value |
|---|---|---|---|
| TV | 727 (71.9%) | 211 (29.0%) | 0.245 |
| Newspapers | 438 (43.3%) | 123 (28.1%) | 0.197 |
| Radio | 90 (8.9%) | 27 (30.0%) | 0.910 |
| Institutional websites | 396 (39.2%) | 96 (24.2%) | 0.003 |
| Social media | 191 (18.9%) | 78 (40.8%) | 0.005 |
| Word of mouth | 182 (18.0%) | 53 (29.1%) | 0.631 |
| Direct Effect | Indirect Effect via Institutional Websites | Indirect Effect via Social Media | Total Effect | |||||
|---|---|---|---|---|---|---|---|---|
| Estimate | p-Value | Estimate | p-Value | Estimate | p-Value | Estimate | p-Value | |
| Individual determinants | ||||||||
| Female gender | 0.047 | 0.230 | −0.003 | 0.611 | 0.010 | 0.243 | 0.054 | 0.161 |
| Age (reference category ≥55 y) | ||||||||
| 18–34 y | −0.025 | 0.607 | 0.001 | 0.881 | 0.026 | 0.032 | 0.003 | 0.954 |
| 35–44 y | 0.138 | 0.005 | 0.007 | 0.332 | 0.021 | 0.080 | 0.166 | 0.001 |
| 45–54 y | 0.062 | 0.195 | 0.016 | 0.066 | 0.012 | 0.285 | 0.090 | 0.060 |
| High school or lower degree | 0.100 | 0.010 | 0.002 | 0.730 | 0.013 | 0.161 | 0.115 | 0.003 |
| Higher than average family income | −0.054 | 0.207 | −0.012 | 0.077 | −0.006 | 0.522 | −0.072 | 0.088 |
| Presence of comorbidities | −0.164 | <0.001 | −0.015 | 0.047 | 0.020 | 0.042 | −0.159 | <0.001 |
| Past vaccination refusal | 0.373 | <0.001 | 0.005 | 0.350 | 0.003 | 0.716 | 0.381 | <0.001 |
| Perceived risk of infection | −0.214 | <0.001 | −0.012 | 0.088 | −0.005 | 0.595 | −0.230 | <0.001 |
| Mediators | ||||||||
| Social media use | 0.179 | <0.001 | 0.179 | <0.001 | ||||
| Institutional websites use | −0.131 | 0.006 | −0.131 | 0.006 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Reno, C.; Maietti, E.; Di Valerio, Z.; Montalti, M.; Fantini, M.P.; Gori, D. Vaccine Hesitancy towards COVID-19 Vaccination: Investigating the Role of Information Sources through a Mediation Analysis. Infect. Dis. Rep. 2021, 13, 712-723. https://doi.org/10.3390/idr13030066
Reno C, Maietti E, Di Valerio Z, Montalti M, Fantini MP, Gori D. Vaccine Hesitancy towards COVID-19 Vaccination: Investigating the Role of Information Sources through a Mediation Analysis. Infectious Disease Reports. 2021; 13(3):712-723. https://doi.org/10.3390/idr13030066
Chicago/Turabian StyleReno, Chiara, Elisa Maietti, Zeno Di Valerio, Marco Montalti, Maria Pia Fantini, and Davide Gori. 2021. "Vaccine Hesitancy towards COVID-19 Vaccination: Investigating the Role of Information Sources through a Mediation Analysis" Infectious Disease Reports 13, no. 3: 712-723. https://doi.org/10.3390/idr13030066
APA StyleReno, C., Maietti, E., Di Valerio, Z., Montalti, M., Fantini, M. P., & Gori, D. (2021). Vaccine Hesitancy towards COVID-19 Vaccination: Investigating the Role of Information Sources through a Mediation Analysis. Infectious Disease Reports, 13(3), 712-723. https://doi.org/10.3390/idr13030066