

Lysosomal Acid Lipase Deficiency in the Etiological Investigation of Cryptogenic Liver Disease in Adults: A Multicenter Brazilian Study
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
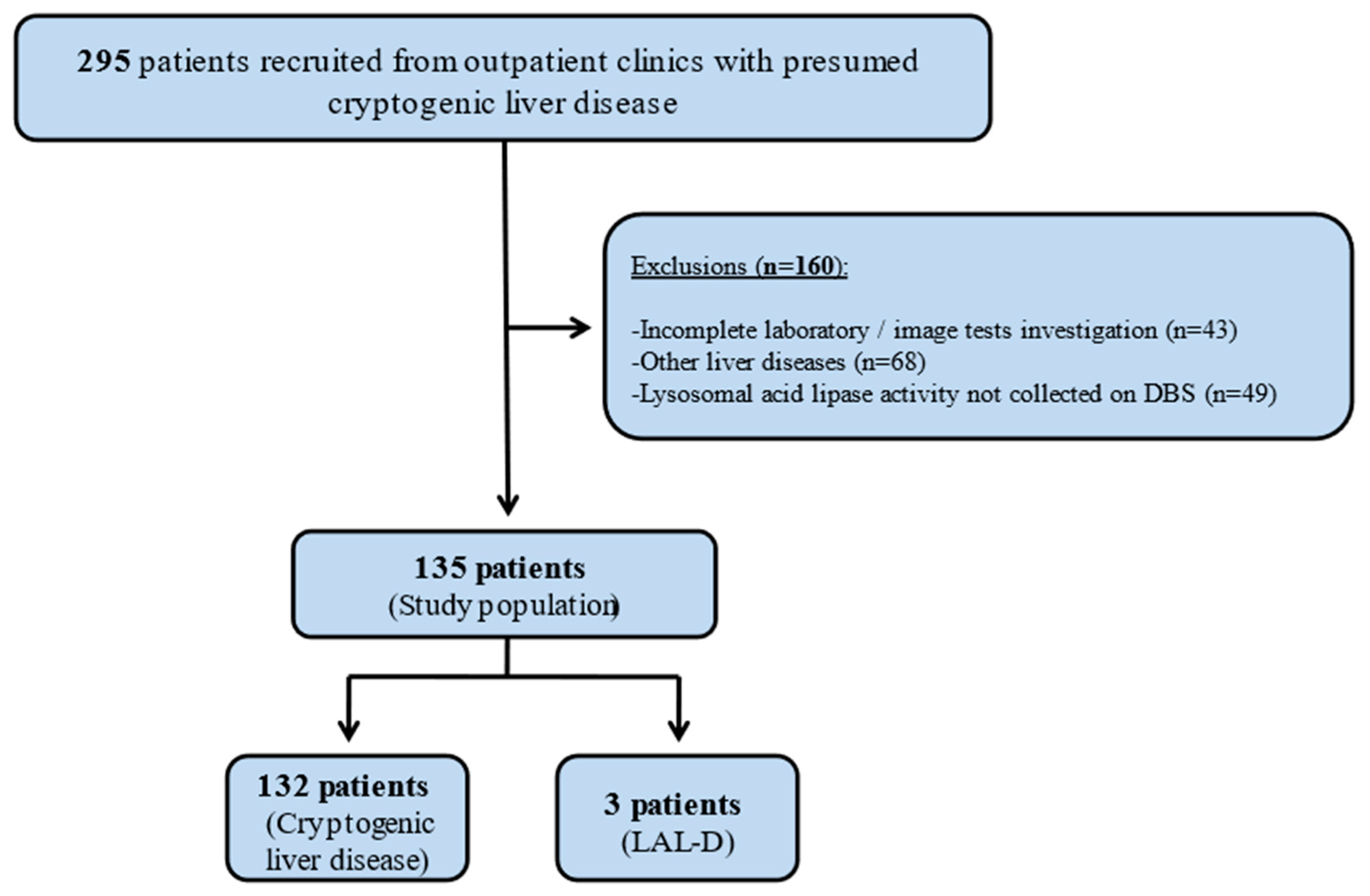
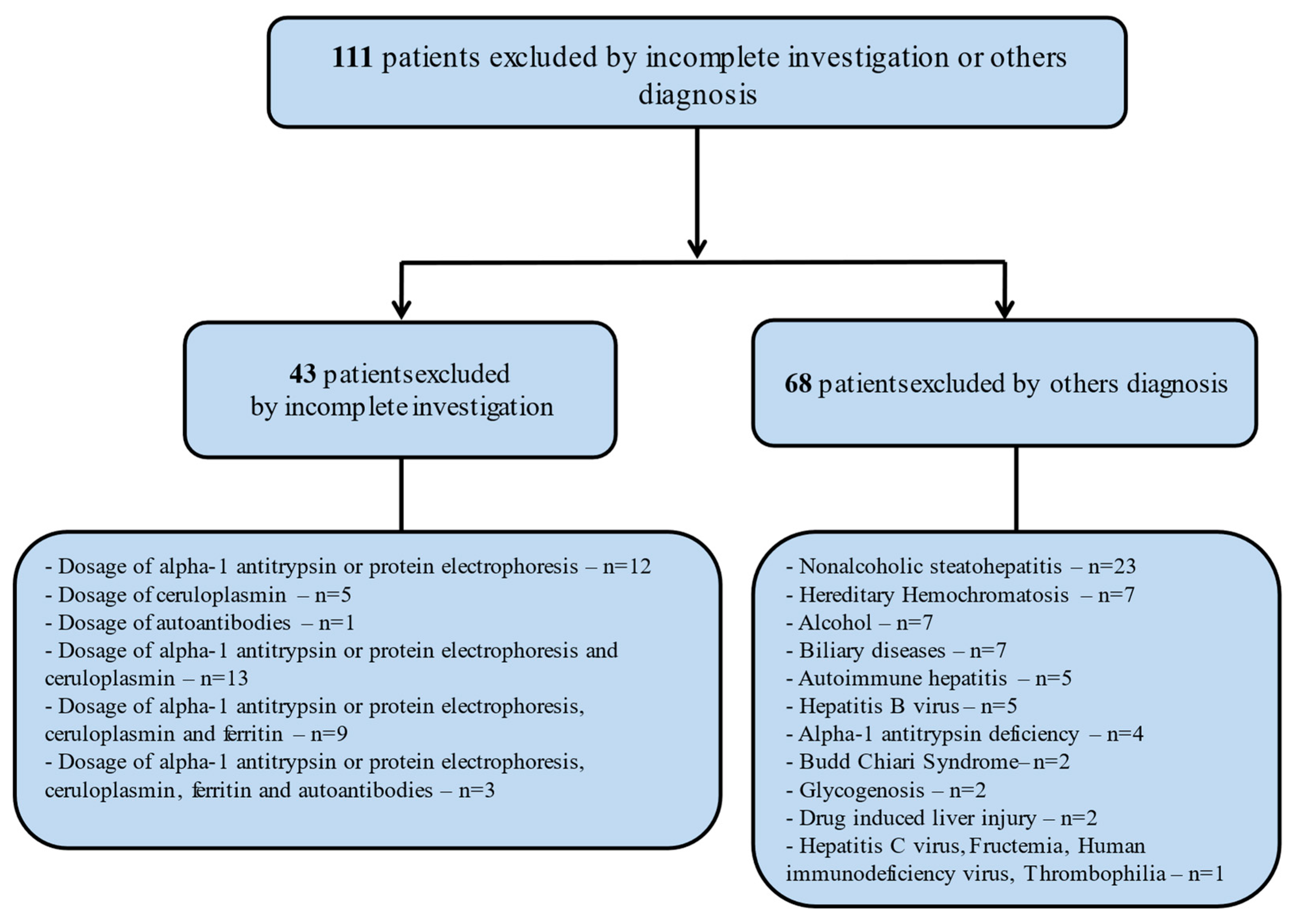
2.1. Clinical Design and Patients Selection
2.2. Study Variables
2.3. Lysosomal Acid Lipase Enzyme Activity
2.4. Statistical Analysis
3. Results
Comparison between Patients with MASLD and Non-MASLD Chronic Cryptogenic Hepatitis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Czaja, A.J. Cryptogenic chronic hepatitis and its changing guise in adults. Dig. Dis. Sci. 2011, 56, 3421–3438. [Google Scholar] [CrossRef] [PubMed]
- Czaja, A.J.; Carpenter, H.A.; Santrach, P.J.; Moore, S.B.; Homburger, H.A. The nature and prognosis of severe cryptogenic chronic active hepatitis. Gastroenterology 1993, 104, 1755–1761. [Google Scholar] [CrossRef] [PubMed]
- Saunders, J.B.; Walters, J.R.; Davies, A.P.; Paton, A. A 20-year prospective study of cirrhosis. Br. Med. J. (Clin. Res. Ed.) 1981, 282, 263–266. [Google Scholar] [CrossRef]
- Caldwell, S.H.; Oelsner, D.H.; Iezzoni, J.C.; Hespenheide, E.E.; Battle, E.H.; Driscoll, C.J. Cryptogenic cirrhosis: Clinical characterization and risk factors for underlying disease. Hepatology 1999, 29, 664–669. [Google Scholar] [CrossRef] [PubMed]
- Caldwell, S.H.; Crespo, D.M. The spectrum expanded: Cryptogenic cirrhosis and the natural history of non-alcoholic fatty liver disease. J. Hepatol. 2004, 40, 578–584. [Google Scholar] [CrossRef]
- Younossi, Z.; Stepanova, M.; Sanyal, A.J.; Harrison, S.A.; Ratziu, V.; Abdelmalek, M.F.; Diehl, A.M.; Caldwell, S.; Shiffman, M.L.; Schall, R.A.; et al. The conundrum of cryptogenic cirrhosis: Adverse outcomes without treatment options. J. Hepatol. 2018, 69, 1365–1370. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, D.L.; Hülkova, H.; Bialer, M.G.; Desnick, R.J. Cholesteryl ester storage disease: Review of the findings in 135 reported patients with an underdiagnosed disease. J. Hepatol. 2013, 58, 1230–1243. [Google Scholar] [CrossRef] [PubMed]
- Elleder, M.; Ledvinová, J.; Cieslar, P.; Kuhn, R. Subclinical course of cholesterol ester storage disease (CESD) diagnosed in adulthood—Report on two cases with remarks on the nature of the liver storage process. Virchows Arch. A Pathol. Anat. Histopathol. 1990, 416, 357–365. [Google Scholar] [CrossRef]
- Burke, J.A.; Schubert, W.K. Deficient activity of hepatic acid lipase in cholesterol ester storage disease. Science 1972, 176, 309–310. [Google Scholar] [CrossRef]
- Aslanidis, C.; Ries, S.; Fehringer, P.; Büchler, C.; Klima, H.; Schmitz, G. Genetic and biochemical evidence that CESD and Wolman disease are distinguished by residual lysosomal acid lipase activity. Genomics 1996, 33, 85–93. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, J.L.; Dana, S.E.; Faust, J.R.; Beaudet, A.L. Role of lysosomal acid lipase in the metabolism of plasma low density lipoprotein. Observations in cultured fibroblasts from a patient with cholesteryl ester storage disease. J. Biol. Chem. 1975, 250, 8487–8496. [Google Scholar] [CrossRef] [PubMed]
- Balwani, M.; Breen, C.; Enns, G.M.; Deegan, P.B.; Honzík, T.; Jones, S.; Kane, J.P.; Malinova, V.; Sharma, R.; Stock, E.O.; et al. Clinical effect and safety profile of recombinant human lysosomal acid lipase in patients with cholesteryl ester storage disease. Hepatology 2013, 58, 950–957. [Google Scholar] [CrossRef]
- Frampton, J.E. Sebelipase Alfa: A Review in lysosomal acid lipase deficiency. Am. J. Cardiovasc. Drugs 2016, 16, 461–468. [Google Scholar] [CrossRef] [PubMed]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef]
- Eslam, M.; Newsome, P.N.; Sarin, S.K.; Anstee, Q.M.; Targher, G.; Romero-Gomez, M.; Zelber-Sagi, S.; Wong, V.W.-S.; Dufour, J.-F.; Schattenberg, J.M.; et al. A new definition for metabolic dysfunction-associated fatty liver disease: An international expert consensus statement. J. Hepatol. 2020, 73, 202–209. [Google Scholar] [CrossRef] [PubMed]
- Nascimbeni, F.; Vici, C.D.; Gentilucci, U.V.; Angelico, F.; Nobili, V.; Petta, S.; Valenti, L.; AISF Rare Diseases Committee. AISF update on the diagnosis and management of adult-onset lysosomal storage diseases with hepatic involvement. Dig. Liver Dis. 2020, 52, 359–367. [Google Scholar] [CrossRef]
- Cunha-Silva, M.; Mazo, D.F.C.; Corrêa, B.R.; Lopes, T.M.; Arrelaro, R.C.; Ferreira, G.L.; Rabello, M.I.; Sevá-Pereira, T.; Escanhoela, C.A.F.; Almeida, J.R.S. Lysosomal acid lipase deficiency leading to liver cirrhosis: A case report of a rare variant mutation. Ann. Hepatol. 2019, 18, 230–235. [Google Scholar] [CrossRef]
- Hamilton, J.; Jones, I.; Srivastava, R.; Galloway, P. A new method for the measurement of lysosomal acid lipase in dried blood spots using the inhibitor Lalistat 2. Clin. Chim. Acta 2012, 413, 1207–1210. [Google Scholar] [CrossRef] [PubMed]
- Reiner, Ž.; Guardamagna, O.; Nair, D.; Soran, H.; Hovingh, K.; Bertolini, S.; Jones, S.; Ćorić, M.; Calandra, S.; Hamilton, J.; et al. Lysosomal acid lipase deficiency—An under-recognized cause of dyslipidaemia and liver dysfunction. Atherosclerosis 2014, 235, 21–30. [Google Scholar] [CrossRef] [PubMed]
- Carter, A.; Brackley, S.M.; Gao, J.; Mann, J.P. The global prevalence and genetic spectrum of lysosomal acid lipase deficiency: A rare condition that mimics NAFLD. J. Hepatol. 2019, 70, 142–150. [Google Scholar] [CrossRef]
- Valayannopoulos, V.; Mengel, E.; Brassier, A.; Grabowski, G. Lysosomal acid lipase deficiency: Expanding differential diagnosis. Mol. Genet. Metab. 2016, 120, 62–66. [Google Scholar] [CrossRef] [PubMed]
- Strebinger, G.; Müller, E.; Feldman, A.; Aigner, E. Lysosomal acid lipase deficiency—Early diagnosis is the key. Hepat. Med. 2019, 11, 79–88. [Google Scholar] [CrossRef] [PubMed]
- Valayannopoulos, V.; Malinova, V.; Honzík, T.; Balwani, M.; Breen, C.; Deegan, P.B.; Enns, G.M.; Jones, S.A.; Kane, J.P.; Stock, E.O.; et al. Sebelipase alfa over 52 weeks reduces serum transaminases, liver volume and improves serum lipids in patients with lysosomal acid lipase deficiency. J. Hepatol. 2014, 61, 1135–1142. [Google Scholar] [CrossRef]
- Burton, B.K.; Balwani, M.; Feillet, F.; Barić, I.; Burrow, T.A.; Grande, C.C.; Coker, M.; Consuelo-Sánchez, A.; Deegan, P.; Di Rocco, M.; et al. A Phase 3 Trial of Sebelipase Alfa in lysosomal acid lipase deficiency. N. Engl. J. Med. 2015, 373, 1010–1020. [Google Scholar] [CrossRef] [PubMed]
- Burton, B.K.; Marulkar, S.; Friedman, M.; Tripuraneni, R.; Furuya, K.N. [Poster] Long-term benefit of sebelipase alfa over 76 weeks in children and adults with lysosomal acid lipase deficiency (ARISE). Mol. Genet Metab. 2016, 120, S33. [Google Scholar] [CrossRef]
- Caldwell, S. Cryptogenic cirrhosis: What are we missing? Curr. Gastroenterol. Rep. 2010, 12, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Fink, S.; Schilsky, M.L. Inherited metabolic disease of the liver. Curr. Opin. Gastroenterol. 2007, 23, 237–243. [Google Scholar] [CrossRef]
- Park, R.H.R.; Mccabe, P.; Fell, G.S.; Russell, R.I. Wilson’s disease in Scotland. Gut 1991, 32, 1541–1545. [Google Scholar] [CrossRef] [PubMed]
- Hamesch, K.; Mandorfer, M.; Pereira, V.M.; Moeller, L.S.; Pons, M.; Dolman, G.E.; Reichert, M.C.; Schneider, C.V.; Woditsch, V.; Voss, J.; et al. Liver fibrosis and metabolic alterations in adults with alpha-1-antitrypsin deficiency caused by the Pi*ZZ Mutation. Gastroenterology 2019, 157, 705–719.e18. [Google Scholar] [CrossRef] [PubMed]
- De Lédinghen, V.; Combes, M.; Trouette, H.; Winnock, M.; Amouretti, M.; De Mascarel, A.; Couzigou, P. Should a liver biopsy be done in patients with subclinical chronically elevated transaminases? Eur. J. Gastroenterol. Hepatol. 2004, 16, 879–883. [Google Scholar] [CrossRef]
- Thuluvath, P.J.; Kantsevoy, S.; Thuluvath, A.J.; Savva, Y. Is cryptogenic cirrhosis different from NASH cirrhosis? J. Hepatol. 2018, 68, 519–525. [Google Scholar] [CrossRef] [PubMed]
- Caldwell, S.; Marchesini, G. Cryptogenic vs NASH-cirrhosis: The rose exists well before its name. J. Hepatol. 2018, 68, 391–392. [Google Scholar] [CrossRef] [PubMed]
- Thuluvath, P.J.; Kantsevoy, S.; Thuluvath, A.J.; Savva, Y. Reply to: “NASH-related and cryptogenic cirrhosis similarities extend beyond cirrhosis”: Cryptogenic cirrhosis should not be equated with NASH cirrhosis based on UNOS data mining and Bayesian ‘doctrine of chances’. J. Hepatol. 2018, 69, 973–975. [Google Scholar] [CrossRef] [PubMed]
- Powell, E.E.; Cooksley, W.G.; Hanson, R.; Searle, J.; Halliday, J.W.; Powell, L.W. The natural history of nonalcoholic steatohepatitis: A follow-up study of forty-two patients for up to 21 years. Hepatology 1990, 11, 74–80. [Google Scholar] [CrossRef] [PubMed]
- Golabi, P.; Paik, J.; Reddy, R.; Bugianesi, E.; Trimble, G.; Younossi, Z.M. Prevalence and long-term outcomes of non-alcoholic fatty liver disease among elderly individuals from the United States. BMC Gastroenterol. 2019, 19, 56. [Google Scholar] [CrossRef]
- Skelly, M.M.; James, P.D.; Ryder, S.D. Findings on liver biopsy to investigate abnormal liver function tests in the absence of diagnostic serology. J. Hepatol. 2001, 35, 195–199. [Google Scholar] [CrossRef]
- Poonawala, A.; Nair, S.P.; Thuluvath, P.J. Prevalence of obesity and diabetes in patients with cryptogenic cirrhosis: A case-control study. Hepatology 2000, 32, 689–692. [Google Scholar] [CrossRef]
- Czaja, A.J.; Carpenter, H.A. Optimizing diagnosis from the medical liver biopsy. Clin. Gastroenterol. Hepatol. 2007, 5, 898–907. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Variable | Case 1 | Case 2 | Case 3 |
|---|---|---|---|
| Age at diagnosis (years) | 45.5 | 53.1 | 33.1 |
| Age of onset of symptoms | 10 years | 52 years | 5 years |
| Gender (male/female) | Female | Male | Female |
| BMI (kg/m2) | 24.8 | 23.8 | 20.7 |
| Fasting glucose (mg/dL) | 86 | 81 | 82 |
| Total cholesterol (mg/dL) | 146 | 211 | 140 |
| HDL (mg/dL) | 24 | 18 | 23 |
| LDL (mg/dL) | 83 | 153 | 79 |
| ALT (U/L) | 22 | 49 | 16 |
| AST (U/L) | 24 | 76 | 15 |
| Total bilirubin (mg/dL) | 0.2 | 1.1 | 0.3 |
| INR | 1.0 | 1.6 | 1.04 |
| Albumin (g/dL) | 2.6 | 3.6 | 3.7 |
| Triglycerides (mg/dL) | 194 | 236 | 190 |
| Anti-HBc (positive/negative) | Negative | Negative | Negative |
| High blood pressure (yes/no) | No | No | No |
| Use of lipid-lowering (yes/no) | No | Yes | No |
| LAL activity | Zero * | Zero * | 1.58 ** |
| DNA mutations | Intron 2 homozygous variation c.1-64C>A; Exon 2 heterozygous variation c.46A>C (ACC>CCC), p.T16P; Intron 6 heterozygous mutation c.538-4C>T; Intron 7 heterozygous variation found at base location c.675+62A>C; Exon 8 heterozygous variations c.867 T>G p. Ser289Ser. | c.386A>G p.H129R/p.H129R | Normal |
| Initial symptoms | Anemia and hepatosplenomegaly | Asymptomatic splenomegaly and thrombocytopenia—findings observed in routine exams | Increased abdominal volume, fever, anemia |
| Initial diagnosis | Niemann–Pick disease | Cryptogenic cirrhosis | Niemann–Pick disease |
| Current symptoms | Ascites, hepatic hydrothorax, protein-losing enteropathy | Asymptomatic | Asymptomatic |
| Liver fibrosis staging | Not cirrhotic | Cirrhotic | Not cirrhotic |
| Liver biopsy | Preserved liver architecture, with the widening of the portal spaces due to fibrosis and a large number of xanthomatous macrophages | Cirrhosis and intense and diffuse microvesicular steatosis, associated with macrophages containing focal deposits of cholesterol crystals | Not performed |
| Upper digestive endoscopy | Multiple sessile pedicled polyps, yellowish in color. Histology compatible with navy blue histiocytosis | Small-caliber esophageal varices multiple polypoid lesions in the duodenum. Histology with xanthomatous macrophages | Multiple elevated polypoid lesions in the duodenum, confluent and pedicled, bluish in color. Histology compatible with navy blue histiocytosis |
| Abdominal imaging exam | Computed tomography with enlarged liver, and multiple sparse calcifications across hepatic and splenic parenchyma, splenomegaly, and a small amount of peritoneal fluid | Computed tomography showing signs of fatty infiltration in the liver, diffuse intrahepatic calcifications, splenomegaly, and right adrenal hemangioma | Ultrasound with mild steatosis |
| Cardiovascular disease | Absent | Absent | Absent |
| Positive family history for LAL-D | Nephew | Absent | Brother and nephew |
| Family history of cardiovascular disease | Absent | Brother who died at 55 years of age from acute myocardial infarction, and father who died of an ischemic stroke | Absent |
| Variable | n | % or Mean | SD |
|---|---|---|---|
| Age (years) | 132 | 51.5 | 14.6 |
| Gender (male/female) | 53/79 | 40.2/59.8 | |
| BMI (kg/m2) | 126 | 27.6 | 5.9 |
| Fasting glucose (mg/dL) | 129 | 110 | 354.7 |
| Total cholesterol (mg/dL) | 128 | 165.3 | 45.9 |
| HDL (mg/dL) | 127 | 48.1 | 17 |
| LDL (mg/dL) | 127 | 92.6 | 38.4 |
| Triglycerides (mg/dL) | 128 | 114 | 376.7 |
| Hypertension (yes/no) | 49/83 | 37.1/62.9 | |
| Liver biopsy (yes/no) | 56/75 | 42.7/57.3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Candolo, A.C.R.; Cançado, G.G.L.; Zitelli, P.M.; Mazo, D.F.d.C.; Oliveira, C.P.M.; Cunha-Silva, M.; Greca, R.D.; Araújo, R.C.; Alustau, A.S.P.T.; Couto, C.A.; et al. Lysosomal Acid Lipase Deficiency in the Etiological Investigation of Cryptogenic Liver Disease in Adults: A Multicenter Brazilian Study. Gastroenterol. Insights 2023, 14, 564-574. https://doi.org/10.3390/gastroent14040040
Candolo ACR, Cançado GGL, Zitelli PM, Mazo DFdC, Oliveira CPM, Cunha-Silva M, Greca RD, Araújo RC, Alustau ASPT, Couto CA, et al. Lysosomal Acid Lipase Deficiency in the Etiological Investigation of Cryptogenic Liver Disease in Adults: A Multicenter Brazilian Study. Gastroenterology Insights. 2023; 14(4):564-574. https://doi.org/10.3390/gastroent14040040
Chicago/Turabian StyleCandolo, Aline Coelho Rocha, Guilherme Grossi Lopes Cançado, Patricia Momoyo Zitelli, Daniel Ferraz de Campos Mazo, Claudia Pinto Marques Oliveira, Marlone Cunha-Silva, Raquel Dias Greca, Roberta Chaves Araújo, Amanda Sacha Paulino Tolentino Alustau, Claudia Alves Couto, and et al. 2023. "Lysosomal Acid Lipase Deficiency in the Etiological Investigation of Cryptogenic Liver Disease in Adults: A Multicenter Brazilian Study" Gastroenterology Insights 14, no. 4: 564-574. https://doi.org/10.3390/gastroent14040040
APA StyleCandolo, A. C. R., Cançado, G. G. L., Zitelli, P. M., Mazo, D. F. d. C., Oliveira, C. P. M., Cunha-Silva, M., Greca, R. D., Araújo, R. C., Alustau, A. S. P. T., Couto, C. A., Nardelli, M. J., de Lima, R. G. R., Farias, A. Q., Carrilho, F. J., & Pessôa, M. G. (2023). Lysosomal Acid Lipase Deficiency in the Etiological Investigation of Cryptogenic Liver Disease in Adults: A Multicenter Brazilian Study. Gastroenterology Insights, 14(4), 564-574. https://doi.org/10.3390/gastroent14040040