
The Combination of Nucleotide Analog Therapy and Steroid Pulse Therapy for Acute HBV Infection Effectively Promotes HBV Clearance

Abstract
:1. Introduction
2. Materials and Methods
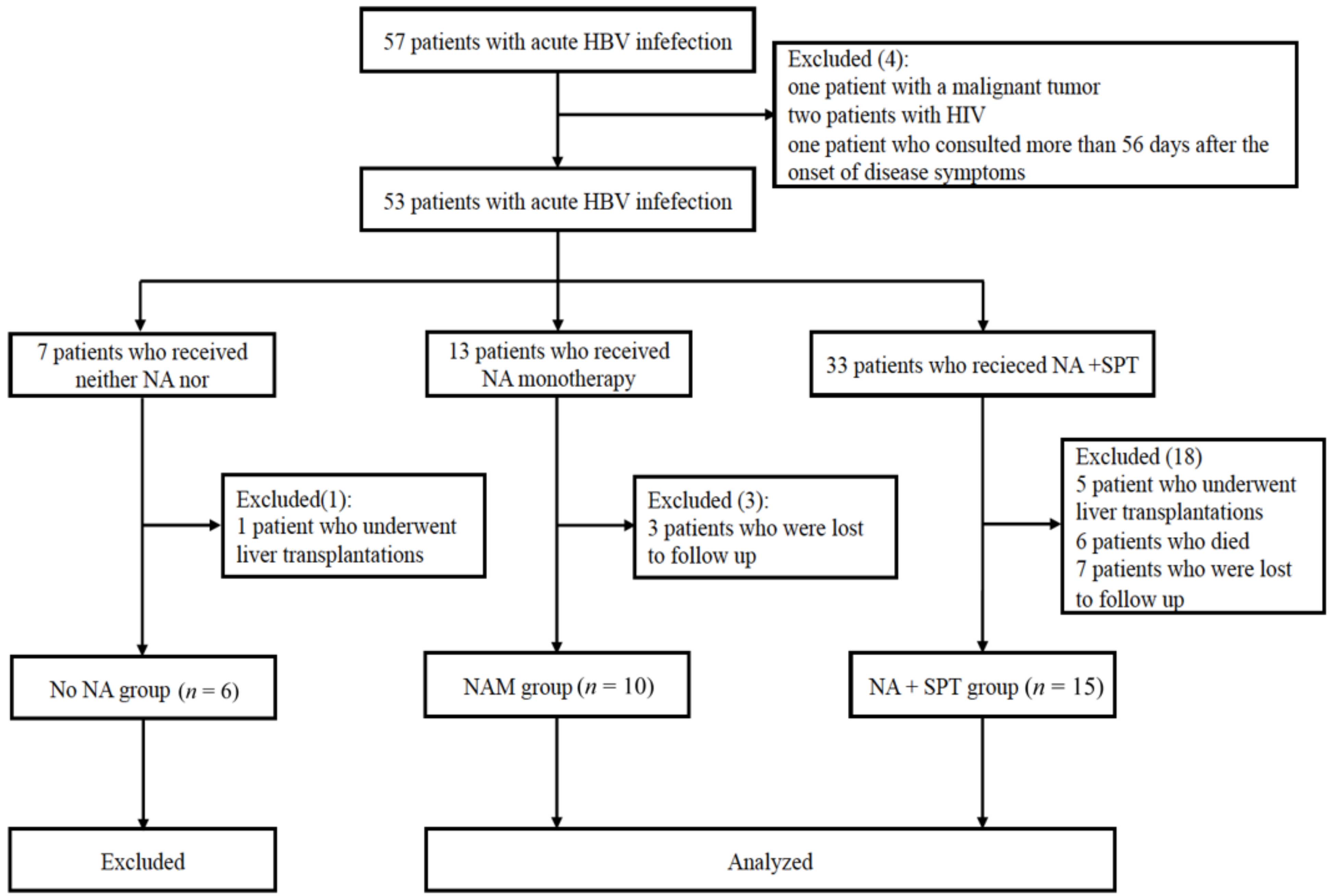
2.1. Patients
2.2. Therapy
2.3. Statistical Analysis
3. Result
3.1. Subject Characteristics
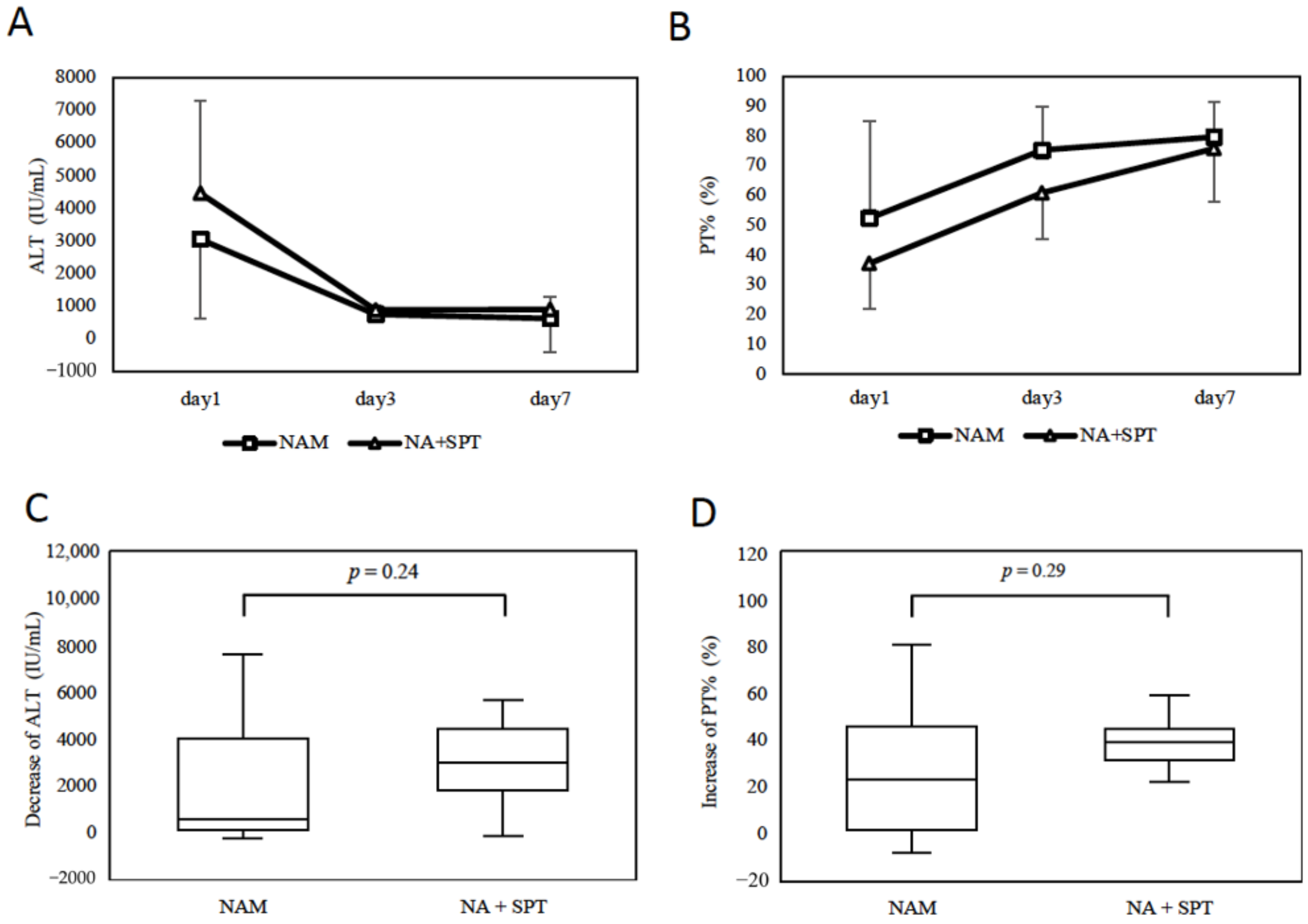
3.2. The Short-Term Effect of NA + SPT
3.3. NA + SPT Efficiently Accelerates HBV Elimination
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Hepatitis, B. 2021. Available online: http://www.who.int/news-room/fact-sheets/detail/hepatitis-b (accessed on 9 December 2021).
- Sato, M.; Tateishi, R.; Yasunaga, H.; Horiguchi, H.; Yoshida, H.; Matsuda, S.; Fushimi, K.; Koike, K. Acute liver disease in Japan: A nationwide analysis of the Japanese Diagnosis Procedure Combination database. J. Gastroenterol. 2014, 49, 547–554. [Google Scholar] [CrossRef] [PubMed]
- Tillmann, H.L.; Hadem, J.; Leifeld, L.; Zachou, K.; Canbay, A.; Eisenbach, C.; Graziadei, I.; Encke, J.; Schmidt, H.; Vogel, W.; et al. Safety and efficacy of lamivudine in patients with severe acute or fulminant hepatitis B, a multicenter experience. J. Viral Hepat. 2006, 13, 256–263. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.-W.; Sun, L.-J.; Zhao, Y.-H.; Kang, P.; Li, S.-C. The Study of Efficacy of Lamivudine in Patients with Severe Acute Hepatitis, B. Dig. Dis. Sci. 2010, 55, 775–783. [Google Scholar] [CrossRef] [PubMed]
- Ito, K.; Yotsuyanagi, H.; Yatsuhashi, H.; Karino, Y.; Takikawa, Y.; Saito, T.; Arase, Y.; Imazeki, F.; Kurosaki, M.; Umemura, T.; et al. Risk factors for long-term persistence of serum hepatitis B surface antigen following acute hepatitis B virus infection in Japanese adults. Hepatology 2014, 59, 89–97. [Google Scholar] [CrossRef] [PubMed]
- Coutinho, A.E.; Chapman, K.E. The anti-inflammatory and immunosuppressive effects of glucocorticoids, recent developments and mechanistic insights. Mol. Cell. Endocrinol. 2011, 335, 2–13. [Google Scholar] [CrossRef] [PubMed]
- Gregory, P.B.; Knauer, C.M.; Kempson, R.L.; Miller, R. Steroid therapy in severe viral hepatitis. A double-blind, randomized trial of methyl-prednisolone versus placebo. N. Engl. J. Med. 1976, 294, 681–687. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver. Randomized trial of steroid therapy in acute liver failure: A report from the European Association for the Study of the Liver. Gut 1979, 20, 620–623. [Google Scholar] [CrossRef] [PubMed]
- Zhao, B.; Zhang, H.-Y.; Xie, G.-J.; Liu, H.-M.; Chen, Q.; Li, R.-F.; You, J.-P.; Yang, S.; Mao, Q.; Zhang, X.-Q. Evaluation of the efficacy of steroid therapy on acute liver failure. Exp. Ther. Med. 2016, 12, 3121–3129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujiwara, K.; Yasui, S.; Yonemitsu, Y.; Mikata, R.; Arai, M.; Kanda, T.; Imazeki, F.; Oda, S.; Yokosuka, O. Efficacy of high-dose corticosteroid in the early stage of viral acute liver failure. Hepatol. Res. 2014, 44, 491–501. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, K.; Yasui, S.; Haga, Y.; Haga, Y.; Nakamura, M.; Yonemitsu, Y.; Arai, M.; Kanda, T.; Oda, S.; Yokosuka, O.; et al. Early combination therapy with corticosteroid and nucleoside analog induces rapid resolution of inflammation in acute liver failure due to transient hepatitis B virus Infection. Intern. Med. 2018, 57, 1543–1552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mochida, S.; Takikawa, Y.; Nakayama, N.; Oketani, M.; Naiki, T.; Yamagishi, Y.; Ichida, T.; Tsubouchi, H. Diagnostic criteria of acute liver failure: A report by the intractable hepato-biliary diseases study group of Japan. Hepatol. Res. 2011, 41, 805–812. [Google Scholar] [CrossRef] [PubMed]
- Rueff, B.; Benhamou, J.P. Acute hepatic necrosis and fulminant hepatic failure. Gut 1973, 14, 805–815. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robert, A.; Chazouilleres, O. Prothrombin time in liver failure: Time, ratio, activity percentage, or international normalized ratio. Hepatology 1996, 24, 1392–1394. [Google Scholar] [CrossRef] [PubMed]
- Tur-Kaspa, R.; Burk, R.D.; Shaul, Y.; Shafritz, D.A. Hepatitis B virus DNA contains a glucocorticoid-responsive element. Proc. Natl. Acad. Sci. USA 1986, 83, 1627–1631. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chou, C.-K.; Wang, L.-H.; Lin, H.-M.; Chi, C.-W. Glucocorticoid stimulates hepatitis B viral gene expression in cultured human hepatoma cells. Hepatology 1992, 16, 13–18. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, M.; Arase, Y.; Ikeda, K.; Tsubota, A.; Suzuki, Y.; Saitoh, S.; Kobayashi, M.; Suzuki, F.; Akuta, N.; Someya, T.; et al. Viral genotypes and response to interferon in patients with acute prolonged hepatitis B virus infection of adulthood in Japan. J. Med. Virol. 2002, 68, 522–528. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Factor | NAM Group (n = 10) | NA + SPT Group (n = 15) | p Value |
|---|---|---|---|
| Age (y.o.) | 44.5 (32–58.5) | 43 (36–54) | 0.57 |
| Gender (M/F) | 7/3 | 7/8 | 0.41 |
| WBC (/mL) | 6035 (5397.5–9507.5) | 5200 (4260–9170) | 0.17 |
| Hb (g/dL) | 14.95 (13.2–15.5) | 14.8 (12.3–15.8) | 0.62 |
| Plt (/μL) | 16.7 (11–19.4) | 11.3 (9.4–17.2) | 0.24 |
| Alb (g/dL) | 3.6 (3.0–4.0) | 3.7 (3.3–4.0) | 0.71 |
| T-Bil (mg/dL) | 6.0 (1.3–10.9) | 5.6 (3.6–7.8) | 1 |
| AST (IU/L) | 1188 (547–4438) | 3261 (1802–5080) | 0.07 |
| ALT (IU/L) | 1562 (1014–7700) | 3868 (2981–5421) | 0.07 |
| LDH (IU/L) | 560 (407–1753) | 1512 (825–3180) | 0.049 |
| γ-GTP (IU/L) | 181 (119–279.5) | 146 (82–273) | 0.7 |
| ALP (IU/L) | 609 (371–685)) | 466 (393–790) | 0.88 |
| BUN (mg/dL) | 8 (7–17) | 9 (5–14) | 0.63 |
| Cre (mg/dL) | 0.71 (0.58–0.86) | 0.63 (0.46–0.77) | 0.45 |
| CRP (mg/dL) | 0.74 (0.4–2.2) | 2.1 (0.5–6.6) | 0.13 |
| PT% | 45 (31.8–90.2) | 40 (25–49) | 0.28 |
| APTT | 38.8 (34.4–47.1) | 41.3 (37.2–43.4) | 0.85 |
| ATⅢ | 66 (43–101) | 67 (45–74) | 0.95 |
| NH3 | 51 (35–60) | 69 (35–166) | 0.17 |
| Ferrtin | 2388 (1028–6371) | 8813 (384–13545) | 0.33 |
| AFP | 5 (3.0–14.3) | 2.8 (1.7–3.6) | 0.078 |
| MELD score | 20 (11–24) | 19 (16–26) | 0.37 |
| Type of disease | |||
| ALI | 5 | 1 | |
| ALF without coma | 5 | 11 | |
| ALF with coma | 0 | 3 | |
| Proportion of ALF | 50% | 93% | 0.023 |
| Therapy | |||
| Plasma exchange (Y/N) | 6/4 (60%) | 13/2 (87%) | 0.17 |
| CHDF (Y/N) | 1/9 (10%) | 2/13 (13%) | 1 |
| Anticoagulant (Y/N) | 5/5 (50%) | 12/3 (80%) | 0.19 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Goya, T.; Kurashige, T.; Kurokawa, M.; Tanaka, M.; Aoyagi, T.; Takahashi, M.; Imoto, K.; Tashiro, S.; Suzuki, H.; Kato, M.; et al. The Combination of Nucleotide Analog Therapy and Steroid Pulse Therapy for Acute HBV Infection Effectively Promotes HBV Clearance. Gastroenterol. Insights 2022, 13, 1-8. https://doi.org/10.3390/gastroent13010001
Goya T, Kurashige T, Kurokawa M, Tanaka M, Aoyagi T, Takahashi M, Imoto K, Tashiro S, Suzuki H, Kato M, et al. The Combination of Nucleotide Analog Therapy and Steroid Pulse Therapy for Acute HBV Infection Effectively Promotes HBV Clearance. Gastroenterology Insights. 2022; 13(1):1-8. https://doi.org/10.3390/gastroent13010001
Chicago/Turabian StyleGoya, Takeshi, Tomoyuki Kurashige, Miho Kurokawa, Masatake Tanaka, Tomomi Aoyagi, Motoi Takahashi, Koji Imoto, Shigeki Tashiro, Hideo Suzuki, Masaki Kato, and et al. 2022. "The Combination of Nucleotide Analog Therapy and Steroid Pulse Therapy for Acute HBV Infection Effectively Promotes HBV Clearance" Gastroenterology Insights 13, no. 1: 1-8. https://doi.org/10.3390/gastroent13010001
APA StyleGoya, T., Kurashige, T., Kurokawa, M., Tanaka, M., Aoyagi, T., Takahashi, M., Imoto, K., Tashiro, S., Suzuki, H., Kato, M., Kohjima, M., & Ogawa, Y. (2022). The Combination of Nucleotide Analog Therapy and Steroid Pulse Therapy for Acute HBV Infection Effectively Promotes HBV Clearance. Gastroenterology Insights, 13(1), 1-8. https://doi.org/10.3390/gastroent13010001