
Enteropathogenic Escherichia coli—A Summary of the Literature


 ,
,  ,
,
Abstract
1. Introduction
2. EPEC Definition and Classification
3. Virulence Factors
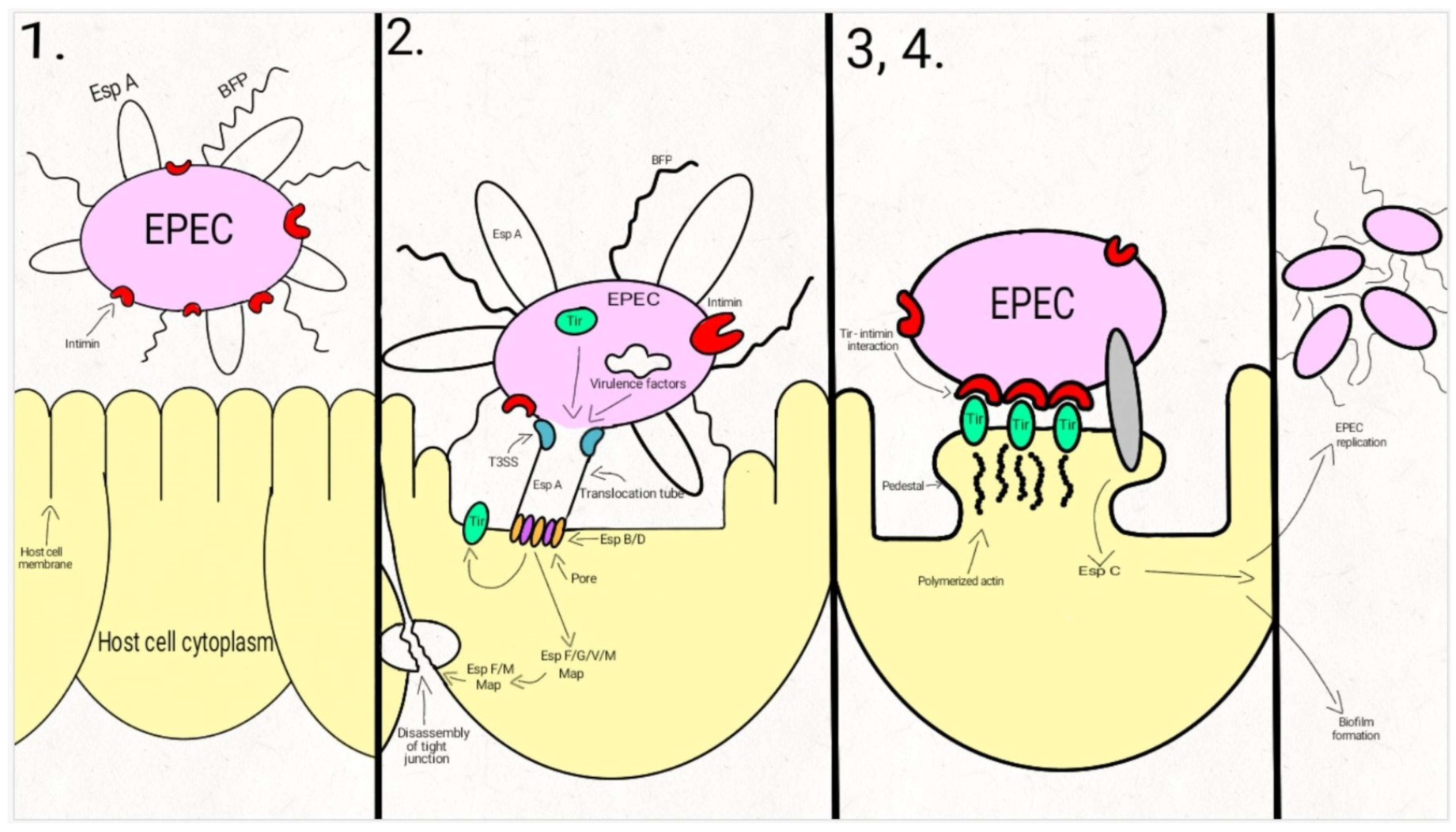
4. Pathogenesis
5. Clinical Aspects
6. Epidemiology
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Troeger, C.; Blacker, B.F.; Khalil, I.A.; Rao, P.C.; Cao, S.; Zimsen, S.R.; Albertson, S.B.; Stanaway, J.D.; Deshpande, A.; Abebe, Z.; et al. Estimates of the Global, Regional, and National Morbidity, Mortality, and Aetiologies of Diarrhoea in 195 Countries: A Systematic Analysis for the Global Burden of Disease Study 2016. Lancet Infect. Dis. 2018, 18, 1211–1228. [Google Scholar] [CrossRef]
- Yu, J.; Jing, H.; Lai, S.; Xu, W.; Li, M.; Wu, J.; Liu, W.; Yuan, Z.; Chen, Y.; Zhao, S.; et al. Etiology of Diarrhea among Children under the Age Five in China: Results from a Five-Year Surveillance. J. Infect. 2015, 71, 19–27. [Google Scholar] [CrossRef] [PubMed]
- Hazen, T.H.; Donnenberg, M.S.; Panchalingam, S.; Antonio, M.; Hossain, A.; Mandomando, I.; Ochieng, J.B.; Ramamurthy, T.; Tamboura, B.; Qureshi, S.; et al. Genomic Diversity of EPEC Associated with Clinical Presentations of Differing Severity. Nat. Microbiol. 2016, 1, 15014. [Google Scholar] [CrossRef] [PubMed]
- Radlović, N.; Leković, Z.; Vuletić, B.; Radlović, V.; Simić, D. Acute Diarrhea in Children. Srp. Arh. Celok. Lek. 2015, 143, 755–762. [Google Scholar] [CrossRef]
- Bellido-Blasco, J.B.; Arnedo-Pena, A. Epidemiology of Infectious Diarrhea. Encycl. Environ. Health 2011, 659–671. [Google Scholar] [CrossRef]
- Allocati, N.; Masulli, M.; Alexeyev, M.F.; Di Ilio, C. Escherichia coli in Europe: An Overview. Int. J. Environ. Res. Public Health 2013, 10, 6235–6254. [Google Scholar] [CrossRef]
- Kotloff, K.L. The Burden and Etiology of Diarrheal Illness in Developing Countries. Pediatric Clin. N. Am. 2017, 64, 799–814. [Google Scholar] [CrossRef]
- Robins-Browne, R.M.; Hartland, E.L. Escherichia coli as a Cause of Diarrhea. J. Gastroenterol. Hepatol. 2002, 17, 467–475. [Google Scholar] [CrossRef]
- Escherich, T. The Intestinal Bacteria of the Neonate and Breast-Fed Infant. 1884. Rev. Infect. Dis. 1988, 10, 1220–1225. [Google Scholar] [CrossRef]
- Chaudhuri, R.R.; Henderson, I.R. The Evolution of the Escherichia coli Phylogeny. Infect. Genet. Evol. 2012, 12, 214–226. [Google Scholar] [CrossRef]
- Gomes, T.A.T.; Elias, W.P.; Scaletsky, I.C.A.; Guth, B.E.C.; Rodrigues, J.F.; Piazza, R.M.F.; Ferreira, L.C.S.; Martinez, M.B. Diarrheagenic Escherichia coli. Braz. J. Microbiol. 2016, 47, 3–30. [Google Scholar] [CrossRef] [PubMed]
- Fratamico, P.M.; DebRoy, C.; Liu, Y.; Needleman, D.S.; Baranzoni, G.M.; Feng, P. Advances in Molecular Serotyping and Subtyping of Escherichia coli. Front. Microbiol. 2016, 7. [Google Scholar] [CrossRef] [PubMed]
- DebRoy, C.; Fratamico, P.M.; Roberts, E. Molecular Serogrouping of Escherichia coli. Anim. Health Res. Rev. 2018, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Campos, L.C.; Franzolin, M.R.; Trabulsi, L.R. Diarrheagenic Escherichia coli Categories among the Traditional Enteropathogenic E. coli O Serogroups: A Review. Memórias Do Inst. Oswaldo Cruz 2004, 99, 545–552. [Google Scholar] [CrossRef] [PubMed]
- Díaz-Jiménez, D.; García-Meniño, I.; Herrera, A.; García, V.; López-Beceiro, A.M.; Alonso, M.P.; Blanco, J.; Mora, A. Genomic Characterization of Escherichia coli Isolates Belonging to a New Hybrid AEPEC/ExPEC Pathotype O153:H10-A-ST10 Eae-Beta1 Occurred in Meat, Poultry, Wildlife and Human Diarrheagenic Samples. Antibiotics 2020, 9, 192. [Google Scholar] [CrossRef]
- Abdalhamid, B.; Mccutchen, E.L.; Bouska, A.C.; Weiwei, Z.; Loeck, B.; Hinrichs, S.H.; Iwen, P.C. Whole Genome Sequencing to Characterize Shiga Toxin-Producing Escherichia coli O26 in a Public Health Setting. J. Infect. Public Health 2019, 12, 884–889. [Google Scholar] [CrossRef] [PubMed]
- Robins-Browne, R.M.; Holt, K.E.; Ingle, D.J.; Hocking, D.M.; Yang, J.; Tauschek, M. Are Escherichia coli Pathotypes Still Relevant in the Era of Whole-Genome Sequencing? Front. Cell Infect. Microbiol. 2016, 6. [Google Scholar] [CrossRef]
- Koutsoumanis, K.; Allende, A.; Alvarez-Ordóñez, A.; Bolton, D.; Bover-Cid, S.; Chemaly, M.; Davies, R.; Cesare, A.D.; Hilbert, F.; Lindqvist, R.; et al. Whole Genome Sequencing and Metagenomics for Outbreak Investigation, Source Attribution and Risk Assessment of Food-Borne Microorganisms. EFSA J. 2019, 17, e05898. [Google Scholar] [PubMed]
- Arimizu, Y.; Kirino, Y.; Sato, M.P.; Uno, K.; Sato, T.; Gotoh, Y.; Auvray, F.; Brugere, H.; Oswald, E.; Mainil, J.G.; et al. Large-Scale Genome Analysis of Bovine Commensal Escherichia coli Reveals That Bovine-Adapted E. coli Lineages Are Serving as Evolutionary Sources of the Emergence of Human Intestinal Pathogenic Strains. Genome Res. 2019, 29, 1495–1505. [Google Scholar] [CrossRef]
- Iguchi, A.; Thomson, N.R.; Ogura, Y.; Saunders, D.; Ooka, T.; Henderson, I.R.; Harris, D.; Asadulghani, M.; Kurokawa, K.; Dean, P.; et al. Complete Genome Sequence and Comparative Genome Analysis of Enteropathogenic Escherichia coli O127:H6 Strain E2348/69. J. Bacteriol. 2009, 191, 347–354. [Google Scholar] [CrossRef]
- Kaper, J.B. Pathogenic Escherichia coli. Int. J. Med. Microbiol. 2005, 295, 355–356. [Google Scholar] [CrossRef] [PubMed]
- Chervy, M.; Barnich, N.; Denizot, J. Adherent-Invasive E. coli: Update on the Lifestyle of a Troublemaker in Crohn’s Disease. Int. J. Mol. Sci. 2020, 21, 3734. [Google Scholar] [CrossRef] [PubMed]
- Meza-Segura, M.; Estrada-Garcia, T. Diffusely Adherent Escherichia coli. In Escherichia coli in the Americas; Torres, A.G., Ed.; Springer International Publishing: Cham, Switzerland, 2016; pp. 125–147. ISBN 978-3-319-45092-6. [Google Scholar]
- Croxen, M.A.; Law, R.J.; Scholz, R.; Keeney, K.M.; Wlodarska, M.; Finlay, B.B. Recent Advances in Understanding Enteric Pathogenic Escherichia coli. Clin. Microbiol. Rev. 2013, 26, 822–880. [Google Scholar] [CrossRef] [PubMed]
- Nataro, J.P.; Kaper, J.B. Diarrheagenic Escherichia coli. Clin. Microbiol. Rev. 1998, 11, 142–201. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.; Torres, A.G. Enteropathogenic Escherichia coli: Foe or Innocent Bystander? Clin Microbiol. Infect. 2015, 21, 729–734. [Google Scholar] [CrossRef] [PubMed]
- Trabulsi, L.R.; Keller, R.; Gomes, T.A.T. Typical and Atypical Enteropathogenic Escherichia coli. Emerg. Infect. Dis. J. Cdc 2002, 8. [Google Scholar] [CrossRef]
- Sánchez, S.; Llorente, M.T.; Echeita, M.A.; Herrera-León, S. Development of Three Multiplex PCR Assays Targeting the 21 Most Clinically Relevant Serogroups Associated with Shiga Toxin-Producing E. coli Infection in Humans. PLoS ONE 2015, 10. [Google Scholar] [CrossRef]
- Joensen, K.G.; Tetzschner, A.M.M.; Iguchi, A.; Aarestrup, F.M.; Scheutz, F. Rapid and Easy In Silico Serotyping of Escherichia coli Isolates by Use of Whole-Genome Sequencing Data. J. Clin. Microbiol. 2015, 53, 2410–2426. [Google Scholar] [CrossRef]
- Scaletsky, I.C.; Silva, M.L.; Toledo, M.R.; Davis, B.R.; Blake, P.A.; Trabulsi, L.R. Correlation between Adherence to HeLa Cells and Serogroups, Serotypes, and Bioserotypes of Escherichia coli. Infect. Immun. 1985, 49, 528–532. [Google Scholar] [CrossRef]
- Ochoa, T.J.; Contreras, C.A. Enteropathogenic E. coli (EPEC) Infection in Children. Curr. Opin. Infect. Dis. 2011, 24, 478. [Google Scholar] [CrossRef]
- Singh, A.P.; Aijaz, S. Enteropathogenic E. coli: Breaking the Intestinal Tight Junction Barrier. F1000Res 2016, 4, 231. [Google Scholar] [CrossRef]
- Cepeda-Molero, M.; Berger, C.N.; Walsham, A.D.S.; Ellis, S.J.; Wemyss-Holden, S.; Schüller, S.; Frankel, G.; Fernández, L.Á. Attaching and Effacing (A/E) Lesion Formation by Enteropathogenic E. coli on Human Intestinal Mucosa Is Dependent on Non-LEE Effectors. PLoS Pathog. 2017, 13, e1006706. [Google Scholar] [CrossRef] [PubMed]
- De Jong, M.F.; Alto, N.M. Cooperative Immune Suppression by Escherichia coli and Shigella Effector Proteins. Infect. Immun. 2018, 86. [Google Scholar] [CrossRef] [PubMed]
- Montso, P.K.; Mlambo, V.; Ateba, C.N. The First Isolation and Molecular Characterization of Shiga Toxin-Producing Virulent Multi-Drug Resistant Atypical Enteropathogenic Escherichia coli O177 Serogroup From South African Cattle. Front. Cell. Infect. Microbiol. 2019, 9. [Google Scholar] [CrossRef]
- Dean, P.; Kenny, B. The Effector Repertoire of Enteropathogenic E. coli: Ganging up on the Host Cell. Curr. Opin. Microbiol. 2009, 12, 101–109. [Google Scholar] [CrossRef]
- Litvak, Y.; Sharon, S.; Hyams, M.; Zhang, L.; Kobi, S.; Katsowich, N.; Dishon, S.; Nussbaum, G.; Dong, N.; Shao, F.; et al. Epithelial Cells Detect Functional Type III Secretion System of Enteropathogenic Escherichia coli through a Novel NF-ΚB Signaling Pathway. PLoS Pathog. 2017, 13, e1006472. [Google Scholar] [CrossRef] [PubMed]
- Pinaud, L.; Sansonetti, P.J.; Phalipon, A. Host Cell Targeting by Enteropathogenic Bacteria T3SS Effectors. Trends Microbiol. 2018, 26, 266–283. [Google Scholar] [CrossRef]
- Leh, H.; Khodr, A.; Bouger, M.-C.; Sclavi, B.; Rimsky, S.; Bury-Moné, S. Bacterial-Chromatin Structural Proteins Regulate the Bimodal Expression of the Locus of Enterocyte Effacement (LEE) Pathogenicity Island in Enteropathogenic Escherichia coli. mBio 2017, 8. [Google Scholar] [CrossRef]
- Pal, R.R.; Baidya, A.K.; Mamou, G.; Bhattacharya, S.; Socol, Y.; Kobi, S.; Katsowich, N.; Ben-Yehuda, S.; Rosenshine, I. Pathogenic E. coli Extracts Nutrients from Infected Host Cells Utilizing Injectisome Components. Cell 2019, 177, 683–696.e18. [Google Scholar] [CrossRef]
- Navarro-Garcia, F.; Serapio-Palacios, A.; Ugalde-Silva, P.; Tapia-Pastrana, G.; Chavez-Dueñas, L. Actin Cytoskeleton Manipulation by Effector Proteins Secreted by Diarrheagenic Escherichia coli Pathotypes. Available online: https://www.hindawi.com/journals/bmri/2013/374395/ (accessed on 27 December 2020).
- Guignot, J.; Segura, A.; Tran Van Nhieu, G. The Serine Protease EspC from Enteropathogenic Escherichia coli Regulates Pore Formation and Cytotoxicity Mediated by the Type III Secretion System. PLoS Pathog. 2015, 11, e1005013. [Google Scholar] [CrossRef]
- Clarke, S.C.; Haigh, R.D.; Freestone, P.P.E.; Williams, P.H. Virulence of Enteropathogenic Escherichia coli, a Global Pathogen. Clin. Microbiol. Rev. 2003, 16, 365–378. [Google Scholar] [CrossRef] [PubMed]
- Vallance, B.A.; Finlay, B.B. Exploitation of Host Cells by Enteropathogenic Escherichia coli. Proc. Natl. Acad. Sci. USA 2000, 97, 8799–8806. [Google Scholar] [CrossRef] [PubMed]
- Franzin, F.M.; Sircili, M.P. Locus of Enterocyte Effacement: A Pathogenicity Island Involved in the Virulence of Enteropathogenic and Enterohemorragic Escherichia coli Subjected to a Complex Network of Gene Regulation. Biomed. Res. Int. 2015, 2015. [Google Scholar] [CrossRef] [PubMed]
- Donnenberg, M.S.; Kaper, J.B. Enteropathogenic Escherichia coli. Infect. Immun. 1992, 60, 3953–3961. [Google Scholar] [CrossRef] [PubMed]
- Scholz, R.; Imami, K.; Scott, N.E.; Trimble, W.S.; Foster, L.J.; Finlay, B.B. Novel Host Proteins and Signaling Pathways in Enteropathogenic E. coli Pathogenesis Identified by Global Phosphoproteome Analysis. Mol. Cell. Proteom. 2015, 14, 1927–1945. [Google Scholar] [CrossRef] [PubMed]
- Hartland, E.L.; Leong, J. Enteropathogenic and Enterohemorrhagic E. coli: Ecology, Pathogenesis, and Evolution. Front. Cell. Infect. Microbiol. 2013, 3. [Google Scholar] [CrossRef] [PubMed]
- Shenoy, A.R.; Furniss, R.C.D.; Goddard, P.J.; Clements, A. Modulation of Host Cell Processes by T3SS Effectors. Curr. Top. Microbiol. Immunol. 2018, 416, 73–115. [Google Scholar] [CrossRef]
- Song, T.; Li, K.; Zhou, W.; Zhou, J.; Jin, Y.; Dai, H.; Xu, T.; Hu, M.; Ren, H.; Yue, J.; et al. A Type III Effector NleF from EHEC Inhibits Epithelial Inflammatory Cell Death by Targeting Caspase-4. Biomed. Res. Int. 2017, 2017. [Google Scholar] [CrossRef] [PubMed]
- Pearson, J.S.; Giogha, C.; Ong, S.Y.; Kennedy, C.L.; Kelly, M.; Robinson, K.S.; Wong, T.; Mansell, A.; Riedmaier, P.; Oates, C.V.; et al. A Type III Effector Antagonises Death Receptor Signalling during Bacterial Gut Infection. Nature 2013, 501, 247–251. [Google Scholar] [CrossRef]
- Wong, A.R.C.; Pearson, J.S.; Bright, M.D.; Munera, D.; Robinson, K.S.; Lee, S.F.; Frankel, G.; Hartland, E.L. Enteropathogenic and Enterohaemorrhagic Escherichia coli: Even More Subversive Elements. Mol. Microbiol. 2011, 80, 1420–1438. [Google Scholar] [CrossRef]
- Ugalde-Silva, P.; Gonzalez-Lugo, O.; Navarro-Garcia, F. Tight Junction Disruption Induced by Type 3 Secretion System Effectors Injected by Enteropathogenic and Enterohemorrhagic Escherichia coli. Front. Cell Infect. Microbiol. 2016, 6. [Google Scholar] [CrossRef] [PubMed]
- Creuzburg, K.; Giogha, C.; Wong Fok Lung, T.; Scott, N.E.; Mühlen, S.; Hartland, E.L.; Pearson, J.S. The Type III Effector NleD from Enteropathogenic Escherichia coli Differentiates between Host Substrates P38 and JNK. Infect. Immun. 2017, 85. [Google Scholar] [CrossRef] [PubMed]
- Deborah Chen, H.; Frankel, G. Enteropathogenic Escherichia coli: Unravelling Pathogenesis. FEMS Microbiol. Rev. 2005, 29, 83–98. [Google Scholar] [CrossRef] [PubMed]
- Serapio-Palacios, A.; Navarro-Garcia, F. EspC, an Autotransporter Protein Secreted by Enteropathogenic Escherichia coli, Causes Apoptosis and Necrosis through Caspase and Calpain Activation, Including Direct Procaspase-3 Cleavage. mBio 2016, 7. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Villamil, J.I.; Navarro-Garcia, F.; Castillo-Romero, A.; Gutierrez-Gutierrez, F.; Tapia, D.; Tapia-Pastrana, G. Curcumin Blocks Cytotoxicity of Enteroaggregative and Enteropathogenic Escherichia coli by Blocking Pet and EspC Proteolytic Release From Bacterial Outer Membrane. Front. Cell Infect. Microbiol. 2019, 9. [Google Scholar] [CrossRef]
- Habouria, H.; Pokharel, P.; Maris, S.; Garénaux, A.; Bessaiah, H.; Houle, S.; Veyrier, F.J.; Guyomard-Rabenirina, S.; Talarmin, A.; Dozois, C.M. Three New Serine-Protease Autotransporters of Enterobacteriaceae (SPATEs) from Extra-Intestinal Pathogenic Escherichia coli and Combined Role of SPATEs for Cytotoxicity and Colonization of the Mouse Kidney. Virulence 2019, 10, 568–587. [Google Scholar] [CrossRef]
- Navarro-Garcia, F.; Serapio-Palacios, A.; Vidal, J.E.; Salazar, M.I.; Tapia-Pastrana, G. EspC Promotes Epithelial Cell Detachment by Enteropathogenic Escherichia coli via Sequential Cleavages of a Cytoskeletal Protein and Then Focal Adhesion Proteins. Infect. Immun. 2014, 82, 2255–2265. [Google Scholar] [CrossRef]
- Govindarajan, D.K.; Viswalingam, N.; Meganathan, Y.; Kandaswamy, K. Adherence Patterns of Escherichia coli in the Intestine and Its Role in Pathogenesis. Med. Microecol. 2020, 5, 100025. [Google Scholar] [CrossRef]
- Xicohtencatl-Cortes, J.; Saldaña, Z.; Deng, W.; Castañeda, E.; Freer, E.; Tarr, P.I.; Finlay, B.B.; Puente, J.L.; Girón, J.A. Bacterial Macroscopic Rope-like Fibers with Cytopathic and Adhesive Properties. J. Biol. Chem. 2010, 285, 32336–32342. [Google Scholar] [CrossRef]
- Kaper, J.B.; Nataro, J.P.; Mobley, H.L.T. Pathogenic Escherichia coli. Nat. Rev. Microbiol. 2004, 2, 123–140. [Google Scholar] [CrossRef]
- Lapointe, T.K.; O’Connor, P.M.; Buret, A.G. The Role of Epithelial Malfunction in the Pathogenesis of Enteropathogenic E. coli -Induced Diarrhea. Lab. Investig. 2009, 89, 964–970. [Google Scholar] [CrossRef] [PubMed]
- Gujral, T.; Kumar, A.; Priyamvada, S.; Saksena, S.; Gill, R.K.; Hodges, K.; Alrefai, W.A.; Hecht, G.A.; Dudeja, P.K. Mechanisms of DRA Recycling in Intestinal Epithelial Cells: Effect of Enteropathogenic E. coli. Am. J. Physiol. Cell Physiol. 2015, 309, C835–C846. [Google Scholar] [CrossRef] [PubMed]
- Cao, L.; Yuan, Z.; Liu, M.; Stock, C. (Patho-)Physiology of Na+/H+ Exchangers (NHEs) in the Digestive System. Front. Physiol. 2020, 10. [Google Scholar] [CrossRef] [PubMed]
- Gurney, M.A.; Laubitz, D.; Ghishan, F.K.; Kiela, P.R. Pathophysiology of Intestinal Na+/H+ Exchange. Cell Mol. Gastroenterol. Hepatol. 2016, 3, 27–40. [Google Scholar] [CrossRef]
- Das, S.; Jayaratne, R.; Barrett, K.E. The Role of Ion Transporters in the Pathophysiology of Infectious Diarrhea. Cell Mol. Gastroenterol. Hepatol. 2018, 6, 33–45. [Google Scholar] [CrossRef]
- Anand, S.; Mandal, S.; Patil, P.; Tomar, S.K. Pathogen-Induced Secretory Diarrhea and Its Prevention. Eur. J. Clin. Microbiol. Infect. Dis. 2016, 35, 1721–1739. [Google Scholar] [CrossRef]
- Broz, P.; Dixit, V.M. Inflammasomes: Mechanism of Assembly, Regulation and Signalling. Nat. Rev. Immunol. 2016, 16, 407–420. [Google Scholar] [CrossRef]
- Nguyen, R.N.; Taylor, L.S.; Tauschek, M.; Robins-Browne, R.M. Atypical Enteropathogenic Escherichia coli Infection and Prolonged Diarrhea in Children. Emerg. Infect. Dis. 2006, 12, 597–603. [Google Scholar] [CrossRef]
- Ronin, I.; Katsowich, N.; Rosenshine, I.; Balaban, N.Q. A Long-Term Epigenetic Memory Switch Controls Bacterial Virulence Bimodality. eLife 2017, 6, e19599. [Google Scholar] [CrossRef]
- Nair, G.B.; Ramamurthy, T.; Bhattacharya, M.K.; Krishnan, T.; Ganguly, S.; Saha, D.R.; Rajendran, K.; Manna, B.; Ghosh, M.; Okamoto, K.; et al. Emerging Trends in the Etiology of Enteric Pathogens as Evidenced from an Active Surveillance of Hospitalized Diarrhoeal Patients in Kolkata, India. Gut Pathog. 2010, 2, 4. [Google Scholar] [CrossRef]
- Okeke, I.N. Diarrheagenic Escherichia coli in Sub-Saharan Africa: Status, Uncertainties and Necessities. J. Infect. Dev. Ctries. 2009, 3, 817–842. [Google Scholar] [CrossRef] [PubMed]
- Spina, A.; Kerr, K.G.; Cormican, M.; Barbut, F.; Eigentler, A.; Zerva, L.; Tassios, P.; Popescu, G.A.; Rafila, A.; Eerola, E.; et al. Spectrum of Enteropathogens Detected by the FilmArray GI Panel in a Multicentre Study of Community-Acquired Gastroenteritis. Clin. Microbiol. Infect. 2015, 21, 719–728. [Google Scholar] [CrossRef] [PubMed]
- Enserink, R.; Scholts, R.; Bruijning-Verhagen, P.; Duizer, E.; Vennema, H.; de Boer, R.; Kortbeek, T.; Roelfsema, J.; Smit, H.; Kooistra-Smid, M.; et al. High Detection Rates of Enteropathogens in Asymptomatic Children Attending Day Care. PLoS ONE 2014, 9, e89496. [Google Scholar] [CrossRef] [PubMed]
- Estrada-Garcia, T.; Lopez-Saucedo, C.; Thompson-Bonilla, R.; Abonce, M.; Lopez-Hernandez, D.; Santos, J.I.; Rosado, J.L.; DuPont, H.L.; Long, K.Z. Association of Diarrheagenic Escherichia coli Pathotypes with Infection and Diarrhea among Mexican Children and Association of Atypical Enteropathogenic E. coli with Acute Diarrhea. J. Clin. Microbiol. 2009, 47, 93–98. [Google Scholar] [CrossRef]
- Hernandes, R.T.; Elias, W.P.; Vieira, M.A.M.; Gomes, T.A.T. An Overview of Atypical Enteropathogenic Escherichia coli. Fems Microbiol. Lett. 2009, 297, 137–149. [Google Scholar] [CrossRef]
- Girón, J.A.; Qadri, F.; Azim, T.; Jarvis, K.J.; Kaper, J.B.; Albert, M.J. Monoclonal Antibodies Specific for the Bundle-Forming Pilus of Enteropathogenic Escherichia coli. Infect. Immun. 1995, 63, 4949–4952. [Google Scholar] [CrossRef]
- Gismero-Ordoñez, J.; Dall’Agnol, M.; Trabulsi, L.R.; Girón, J.A. Expression of the Bundle-Forming Pilus by Enteropathogenic Escherichia coli Strains of Heterologous Serotypes. J. Clin. Microbiol. 2002, 40, 2291–2296. [Google Scholar] [CrossRef]
- Nakasone, N.; Toma, C.; Lu, Y.; Iwanaga, M. Development of a Rapid Immunochromatographic Test to Identify Enteropathogenic and Enterohemorrhagic Escherichia coli by Detecting EspB. Diagn. Microbiol. Infect. Dis. 2007, 57, 21–25. [Google Scholar] [CrossRef]
- Lu, Y.; Toma, C.; Honma, Y.; Iwanaga, M. Detection of EspB Using Reversed Passive Latex Agglutination: Application to Determination of Enteropathogenic Escherichia coli. Diagn. Microbiol. Infect. Dis. 2002, 43, 7–12. [Google Scholar] [CrossRef]
- Rocha, L.B.; Santos, A.R.R.; Munhoz, D.D.; Cardoso, L.T.A.; Luz, D.E.; Andrade, F.B.; Horton, D.S.P.Q.; Elias, W.P.; Piazza, R.M.F. Development of a Rapid Agglutination Latex Test for Diagnosis of Enteropathogenic and Enterohemorrhagic Escherichia coli Infection in Developing World: Defining the Biomarker, Antibody and Method. PLoS Negl. Trop. Dis. 2014, 8, e3150. [Google Scholar] [CrossRef]
- Ashworth, M.; White, P.; Jongsma, H.; Schofield, P.; Armstrong, D. Antibiotic Prescribing and Patient Satisfaction in Primary Care in England: Cross-Sectional Analysis of National Patient Survey Data and Prescribing Data. Br. J. Gen. Pr. 2016, 66, e40–e46. [Google Scholar] [CrossRef] [PubMed]
- Bruzzese, E.; Giannattasio, A.; Guarino, A. Antibiotic Treatment of Acute Gastroenteritis in Children. F1000Research 2018, 7. [Google Scholar] [CrossRef] [PubMed]
- Zollner-Schwetz, I.; Krause, R. Therapy of Acute Gastroenteritis: Role of Antibiotics. Clin. Microbiol. Infect. 2015, 21, 744–749. [Google Scholar] [CrossRef] [PubMed]
- Salam, M.; Lindberg, G.; Dite, P.; Khalif, I.; Salazar-Lindo, E.; Ramakrishna, B.S.; Goh, K.; Thomson, A.; Khan, A.G.; Krabshuis, D.J.; et al. Acute Diarrhea in Adults and Children: A Global Perspective. J. Clin. Gastroenterol. 2013, 47, 12–20. [Google Scholar]
- Lee, T.-H.; Wong, J.G.; Lye, D.C.; Chen, M.I.; Loh, V.W.; Leo, Y.-S.; Lee, L.K.; Chow, A.L. Medical and Psychosocial Factors Associated with Antibiotic Prescribing in Primary Care: Survey Questionnaire and Factor Analysis. Br. J. Gen. Pr. 2017, 67, e168–e177. [Google Scholar] [CrossRef]
- Subramanian, K.; Selvakkumar, C.; Vinaykumar, K.S.; Goswami, N.; Meenakshisundaram, S.; Balakrishnan, A.; Lakshmi, B.S. Tackling Multiple Antibiotic Resistance in Enteropathogenic Escherichia coli (EPEC) Clinical Isolates: A Diarylheptanoid from Alpinia Officinarum Shows Promising Antibacterial and Immunomodulatory Activity against EPEC and Its Lipopolysaccharide-Induced Inflammation. Int. J. Antimicrob. Agents 2009, 33, 244–250. [Google Scholar] [CrossRef]
- Taghadosi, R.; Shakibaie, M.R.; Hosseini -Nave, H. Antibiotic Resistance, ESBL Genes, Integrons, Phylogenetic Groups and MLVA Profiles of Escherichia coli Pathotypes Isolated from Patients with Diarrhea and Farm Animals in South-East of Iran. Comp. Immunol. Microbiol. Infect. Dis. 2019, 63, 117–126. [Google Scholar] [CrossRef]
- Scaletsky, I.C.; Souza, T.B.; Aranda, K.R.; Okeke, I.N. Genetic Elements Associated with Antimicrobial Resistance in Enteropathogenic Escherichia coli (EPEC) from Brazil. BMC Microbiol. 2010, 10, 25. [Google Scholar] [CrossRef]
- Khairy, R.M.M.; Fathy, Z.A.; Mahrous, D.M.; Mohamed, E.S.; Abdelrahim, S.S. Prevalence, Phylogeny, and Antimicrobial Resistance of Escherichia coli Pathotypes Isolated from Children Less than 5 Years Old with Community Acquired- Diarrhea in Upper Egypt. BMC Infect Dis. 2020, 20, 908. [Google Scholar] [CrossRef]
- Chen, Y.; Chen, X.; Zheng, S.; Yu, F.; Kong, H.; Yang, Q.; Cui, D.; Chen, N.; Lou, B.; Li, X.; et al. Serotypes, Genotypes and Antimicrobial Resistance Patterns of Human Diarrhoeagenic Escherichia coli Isolates Circulating in Southeastern China. Clin. Microbiol. Infect. 2014, 20, 52–58. [Google Scholar] [CrossRef]
- Zhang, S.-X.; Zhou, Y.-M.; Tian, L.-G.; Chen, J.-X.; Tinoco-Torres, R.; Serrano, E.; Li, S.-Z.; Chen, S.-H.; Ai, L.; Chen, J.-H.; et al. Antibiotic Resistance and Molecular Characterization of Diarrheagenic Escherichia coli and Non-Typhoidal Salmonella Strains Isolated from Infections in Southwest China. Infect. Dis. Poverty 2018, 7. [Google Scholar] [CrossRef] [PubMed]
- Alikhani, M.Y.; Hashemi, S.H.; Aslani, M.M.; Farajnia, S. Prevalence and Antibiotic Resistance Patterns of Diarrheagenic Escherichia coli Isolated from Adolescents and Adults in Hamedan, Western Iran. Iran J. Microbiol. 2013, 5, 42–47. [Google Scholar]
- Sirous, M.; Hashemzadeh, M.; Keshtvarz, M.; Amin, M.; Shams, N.; Dastoorpoor, M.; Shahin, M.; Koraei, D. Molecular Characterization and Antimicrobial Resistance of Enteropathogenic Escherichia coli in Children from Ahvaz, Iran. Available online: https://sites.kowsarpub.com/jjm/articles/100877.html#abstract (accessed on 15 January 2021).
- Thakur, N.; Jain, S.; Changotra, H.; Shrivastava, R.; Kumar, Y.; Grover, N.; Vashistt, J. Molecular Characterization of Diarrheagenic Escherichia coli Pathotypes: Association of Virulent Genes, Serogroups, and Antibiotic Resistance among Moderate-to-severe Diarrhea Patients. J. Clin. Lab. Anal. 2018, 32. [Google Scholar] [CrossRef]
- Eltai, N.O.; Al Thani, A.A.; Al Hadidi, S.H.; Al Ansari, K.; Yassine, H.M. Antibiotic Resistance and Virulence Patterns of Pathogenic Escherichia coli Strains Associated with Acute Gastroenteritis among Children in Qatar. BMC Microbiol. 2020, 20, 54. [Google Scholar] [CrossRef] [PubMed]
- Seidman, J.C.; Johnson, L.B.; Levens, J.; Mkocha, H.; Muñoz, B.; Silbergeld, E.K.; West, S.K.; Coles, C.L. Longitudinal Comparison of Antibiotic Resistance in Diarrheagenic and Non-Pathogenic Escherichia coli from Young Tanzanian Children. Front. Microbiol. 2016, 7. [Google Scholar] [CrossRef]
- Canizalez-Roman, A.; Flores-Villaseñor, H.M.; Gonzalez-Nuñez, E.; Velazquez-Roman, J.; Vidal, J.E.; Muro-Amador, S.; Alapizco-Castro, G.; Díaz-Quiñonez, J.A.; León-Sicairos, N. Surveillance of Diarrheagenic Escherichia coli Strains Isolated from Diarrhea Cases from Children, Adults and Elderly at Northwest of Mexico. Front. Microbiol. 2016, 7. [Google Scholar] [CrossRef]
- Mare, A.; Man, A.; Toma, F.; Ciurea, C.N.; Coșeriu, R.L.; Vintilă, C.; Maier, A.C. Hemolysin-Producing Strains among Diarrheagenic Escherichia coli Isolated from Children under 2 Years Old with Diarrheal Disease. Pathogens 2020, 9, 1022. [Google Scholar] [CrossRef]
- Zhou, Y.; Zhu, X.; Hou, H.; Lu, Y.; Yu, J.; Mao, L.; Mao, L.; Sun, Z. Characteristics of Diarrheagenic Escherichia coli among Children under 5 Years of Age with Acute Diarrhea: A Hospital Based Study. BMC Infect. Dis. 2018, 18. [Google Scholar] [CrossRef]
- Xu, Y.; Sun, H.; Bai, X.; Fu, S.; Fan, R.; Xiong, Y. Occurrence of Multidrug-Resistant and ESBL-Producing Atypical Enteropathogenic Escherichia coli in China. Gut Pathog. 2018, 10, 8. [Google Scholar] [CrossRef]
- Jafari, E.; Mostaan, S.; Bouzari, S. Characterization of Antimicrobial Susceptibility, Extended-Spectrum β-Lactamase Genes and Phylogenetic Groups of Enteropathogenic Escherichia coli Isolated from Patients with Diarrhea. Osong Public Health Res. Perspect. 2020, 11, 327–333. [Google Scholar] [CrossRef]
- Yang, K.; Pagaling, E.; Yan, T. Estimating the Prevalence of Potential Enteropathogenic Escherichia coli and Intimin Gene Diversity in a Human Community by Monitoring Sanitary Sewage. Appl. Environ. Microbiol. 2014, 80, 119–127. [Google Scholar] [CrossRef] [PubMed]
- Platenkamp, A.; Mellies, J.L. Environment Controls LEE Regulation in Enteropathogenic Escherichia coli. Front. Microbiol. 2018, 9. [Google Scholar] [CrossRef] [PubMed]
- Franzolin, M.R.; Alves, R.C.B.; Keller, R.; Gomes, T.A.T.; Beutin, L.; Barreto, M.L.; Milroy, C.; Strina, A.; Ribeiro, H.; Trabulsi, L.R. Prevalence of Diarrheagenic Escherichia coli in Children with Diarrhea in Salvador, Bahia, Brazil. Memórias Do Inst. Oswaldo Cruz 2005, 100, 359–363. [Google Scholar] [CrossRef] [PubMed]
- Rajendran, P.; Ajjampur, S.S.R.; Chidambaram, D.; Chandrabose, G.; Thangaraj, B.; Sarkar, R.; Samuel, P.; Rajan, D.P.; Kang, G. Pathotypes of Diarrheagenic Escherichia coli in Children Attending a Tertiary Care Hospital in South India. Diagn. Microbiol. Infect. Dis. 2010, 68, 117–122. [Google Scholar] [CrossRef]
- Kotloff, K.L.; Nataro, J.P.; Blackwelder, W.C.; Nasrin, D.; Farag, T.H.; Panchalingam, S.; Wu, Y.; Sow, S.O.; Sur, D.; Breiman, R.F.; et al. Burden and Aetiology of Diarrhoeal Disease in Infants and Young Children in Developing Countries (the Global Enteric Multicenter Study, GEMS): A Prospective, Case-Control Study. Lancet 2013, 382, 209–222. [Google Scholar] [CrossRef]
- Santona, S.; Diaz, N.; Fiori, P.L.; Francisco, M.; Sidat, M.; Cappuccinelli, P.; Rappelli, P. Genotypic and Phenotypic Features of Enteropathogenic Escherichia coli Isolated in Industrialized and Developing Countries. J. Infect. Dev. Ctries. 2013, 7, 214–219. [Google Scholar] [CrossRef][Green Version]
- Langendorf, C.; Hello, S.L.; Moumouni, A.; Gouali, M.; Mamaty, A.-A.; Grais, R.F.; Weill, F.-X.; Page, A.-L. Enteric Bacterial Pathogens in Children with Diarrhea in Niger: Diversity and Antimicrobial Resistance. PLoS ONE 2015, 10, e0120275. [Google Scholar] [CrossRef]
- Odetoyin, B.W.; Hofmann, J.; Aboderin, A.O.; Okeke, I.N. Diarrhoeagenic Escherichia coli in Mother-Child Pairs in Ile-Ife, South Western Nigeria. BMC Infect. Dis. 2016, 16, 28. [Google Scholar] [CrossRef]
- Ben Salem-Ben Nejma, I.; Hassine Zaafrane, M.; Hassine, F.; Sdiri-Loulizi, K.; Ben Said, M.; Aouni, M.; Mzoughi, R. Etiology of Acute Diarrhea in Tunisian Children with Emphasis on Diarrheagenic Escherichia coli: Prevalence and Identification of E. coli Virulence Markers. Iran J. Public Health 2014, 43, 947–960. [Google Scholar]
- Swennes, A.G.; Buckley, E.M.; Parry, N.M.A.; Madden, C.M.; García, A.; Morgan, P.B.; Astrofsky, K.M.; Fox, J.G. Enzootic Enteropathogenic Escherichia coli Infection in Laboratory Rabbits. J. Clin. Microbiol. 2012, 50, 2353–2358. [Google Scholar] [CrossRef]
- Sekse, C.; Sunde, M.; Lindstedt, B.-A.; Hopp, P.; Bruheim, T.; Cudjoe, K.S.; Kvitle, B.; Urdahl, A.M. Potentially Human-Pathogenic Escherichia coli O26 in Norwegian Sheep Flocks. Appl. Environ. Microbiol. 2011, 77, 4949–4958. [Google Scholar] [CrossRef] [PubMed]
- Moura, R.A.; Sircili, M.P.; Leomil, L.; Matté, M.H.; Trabulsi, L.R.; Elias, W.P.; Irino, K.; Pestana de Castro, A.F. Clonal Relationship among Atypical Enteropathogenic Escherichia coli Strains Isolated from Different Animal Species and Humans. Appl. Environ. Microbiol 2009, 75, 7399–7408. [Google Scholar] [CrossRef] [PubMed]
- Rojas-Lopez, M.; Monterio, R.; Pizza, M.; Desvaux, M.; Rosini, R. Intestinal Pathogenic Escherichia coli: Insights for Vaccine Development. Front. Microbiol. 2018, 9. [Google Scholar] [CrossRef] [PubMed]
- Caetano, B.A.; Rocha, L.B.; Carvalho, E.; Piazza, R.M.F.; Luz, D. Immunogenic Domains and Secondary Structure of Escherichia coli Recombinant Secreted Protein Escherichia coli-Secreted Protein B. Front. Immunol. 2017, 8. [Google Scholar] [CrossRef]


{kind=link}
| Pathotype of Diarrheagenic E. coli | Acronym | Virulence Factors | Diagnostic Targets for PCR | Disease | Clinical Symptoms | Ref |
|---|---|---|---|---|---|---|
| Enteropathogenic E. coli | EPEC | Locus of enterocyte effacement (LEE), intimin, bundle-forming pilus | bae, bfpA | Acute/persistent diarrhea in children | Watery diarrhea, vomiting | [6,17,21] |
| Enterohaemorrhagic E. coli (Shiga toxin-producing) | EHEC/STEC | Shiga toxin 1 and/or 2 LEE, adhesins (EHEC) | stx1, stx2, eae, ehxA, bfp | Hemolytic-uremic syndrome, hemorrhagic colitis | Bloody diarrhea | [6,11,17] |
| Enteroinvasive E. coli | EIEC | Shiga toxin, hemolysin, cellular invasion, Ipa | ipaH, other ipa genes | Shigellosis-like syndrome | Watery, bloody diarrhea | [6,11] |
| Adherent Invasive E. coli | AIEC | Type 1 fimbriae, cellular invasion | none | Associated with Crohn disease | Persistent intestinal inflammation | [12,17,22] |
| Enterotoxigenic E. coli | ETEC | Heat-labile and heat-stable toxins, CFAs (colonization factors) | elt, est | Traveler’s diarrhea | Watery diarrhea, vomiting | [6,11,17] |
| Diffusely Adherent E. coli | DAEC | Adhesins | Afa/Dr adhesins | Diarrhea in children | Watery diarrhea | [6,17,23] |
| Enteroaggregative E. coli (hybrid pathotype) | EAEC | Adhesins, toxins and secreted proteins | pAA, AggR, AAFs | Diarrhea in children | Vomiting diarrhea (with mucus) | [6,11] |
| EPEC Strain | eae | bfp | stx |
|---|---|---|---|
| Typical EPEC | + | + | − |
| Atypical EPEC | + | − | − |
| EPEC Strain | EPEC | Atypical EPEC | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Reference | Southeastern China, 2014 [92] | Southwest China, 2018 [93] | Western Iran, 2013 [94] | Iran, 2020 [95] | India, 2018 [96] | Qatar, 2020 [97] | Tanzania, 2016 [98] | Northwest Mexico, 2016 [99] | Romania, 2020 [100] | Central China, 2018 [101] | China, 2018 [102] | Iran, 2020 [103] |
| Antibiotic | Antibiotic Resistance | |||||||||||
| Ampicillin | 86.5% | 75.41% | 84.2% | 100% | 82.2% | 51.7% | 79.0% | 83% | 36.1% | 81.0% | 55.6% | 70.8% |
| Amoxicillin-clavulanic acid | 32.7 | 42.62% | - | - | - | 7.1% | 15% | - | 2.4% | - | 9.3% | - |
| Cefuroxime | 40.4% | - | - | - | - | 23.2% | - | - | 11.1% | 61.9% | 25.8% | - |
| Cefotaxime | 36.5% | 19.67% | 73.6% | 64.7% | - | - | - | 32.1% | 11.2% | 66.7% | 25.8% | 35.4% |
| Cefepime | 9.6% | - | - | - | - | 3.6% | - | - | 14.3% | 38.1% | 9.3% | - |
| Imipenem | 0% | - | - | 0% | - | - | - | - | 0% | 14.3% | 0% | 0% |
| Meropenem | 0% | - | - | 0% | - | - | - | - | 0% | 14.3% | 0% | - |
| Gentamycin | 36.5% | 21.31% | 10.5% | 11.76% | - | 5.5% | - | 13.2% | 1% | 47.6% | 37.7% | - |
| Ciprofloxacin | 25.0% | 4.92% | 0% | 35.29% | - | 7.1% | 0% | 45.3% | 5% | 42.9% | 5.3% | 7.7% |
| Trimethoprim–sulphamethoxazole | 63.5% | 57.38% | 73.7% | 76.47% | - | 42.9% | 79.0% | 83% | 25.9% | 66.7% | 47.7% | 56.9% |
| Tetracycline | 69.2% | 78.69% | 63.2% | 35.29% | - | 46.4% | - | 94.3% | 28.6% | - | 58.9% | 46.2% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mare, A.D.; Ciurea, C.N.; Man, A.; Tudor, B.; Moldovan, V.; Decean, L.; Toma, F. Enteropathogenic Escherichia coli—A Summary of the Literature. Gastroenterol. Insights 2021, 12, 28-40. https://doi.org/10.3390/gastroent12010004
Mare AD, Ciurea CN, Man A, Tudor B, Moldovan V, Decean L, Toma F. Enteropathogenic Escherichia coli—A Summary of the Literature. Gastroenterology Insights. 2021; 12(1):28-40. https://doi.org/10.3390/gastroent12010004
Chicago/Turabian StyleMare, Anca Delia, Cristina Nicoleta Ciurea, Adrian Man, Bianca Tudor, Valeriu Moldovan, Luminița Decean, and Felicia Toma. 2021. "Enteropathogenic Escherichia coli—A Summary of the Literature" Gastroenterology Insights 12, no. 1: 28-40. https://doi.org/10.3390/gastroent12010004
APA StyleMare, A. D., Ciurea, C. N., Man, A., Tudor, B., Moldovan, V., Decean, L., & Toma, F. (2021). Enteropathogenic Escherichia coli—A Summary of the Literature. Gastroenterology Insights, 12(1), 28-40. https://doi.org/10.3390/gastroent12010004