
Sudden Unexpected Death in Epilepsy

 ,
,  and
and 
Abstract
:1. Introduction
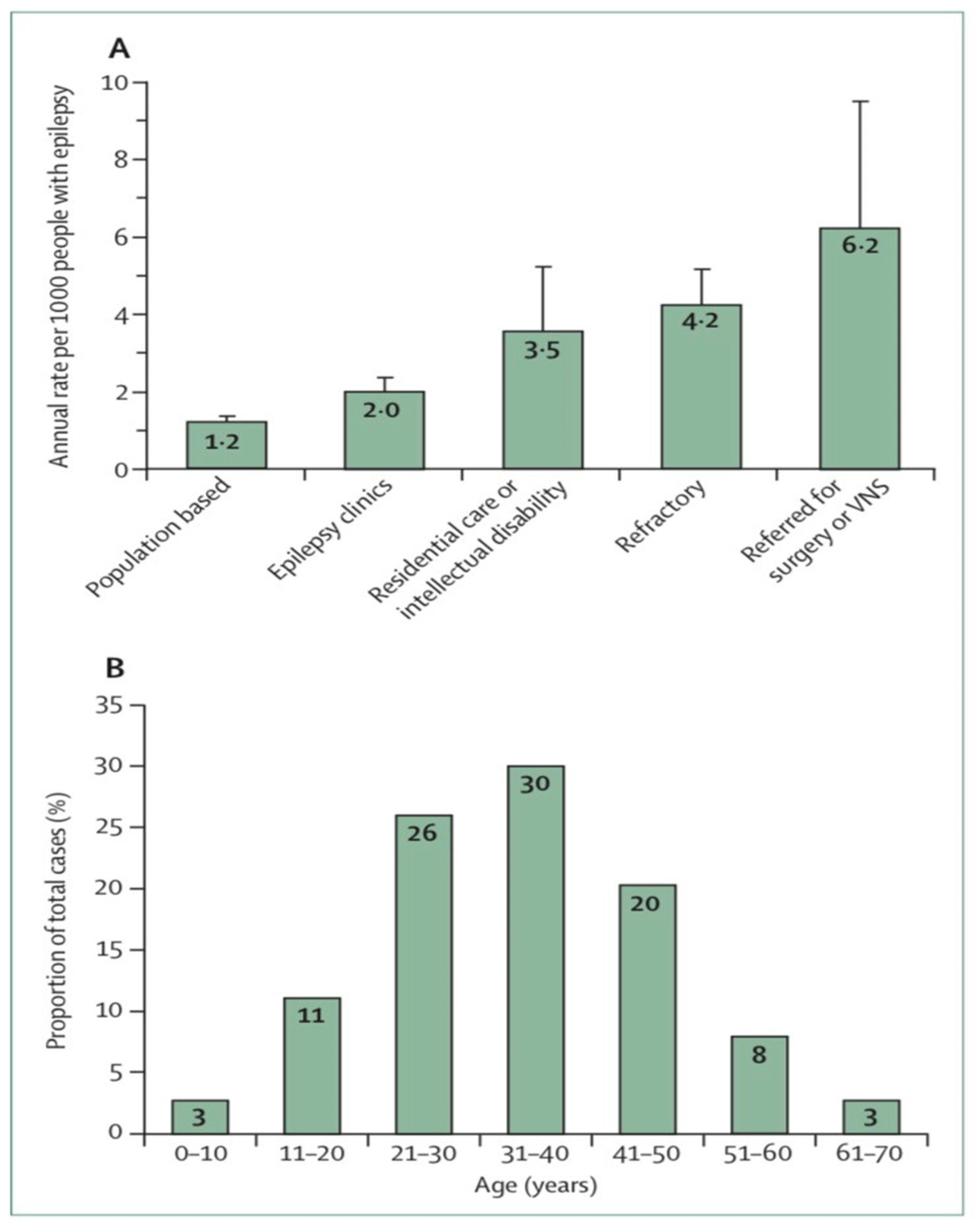
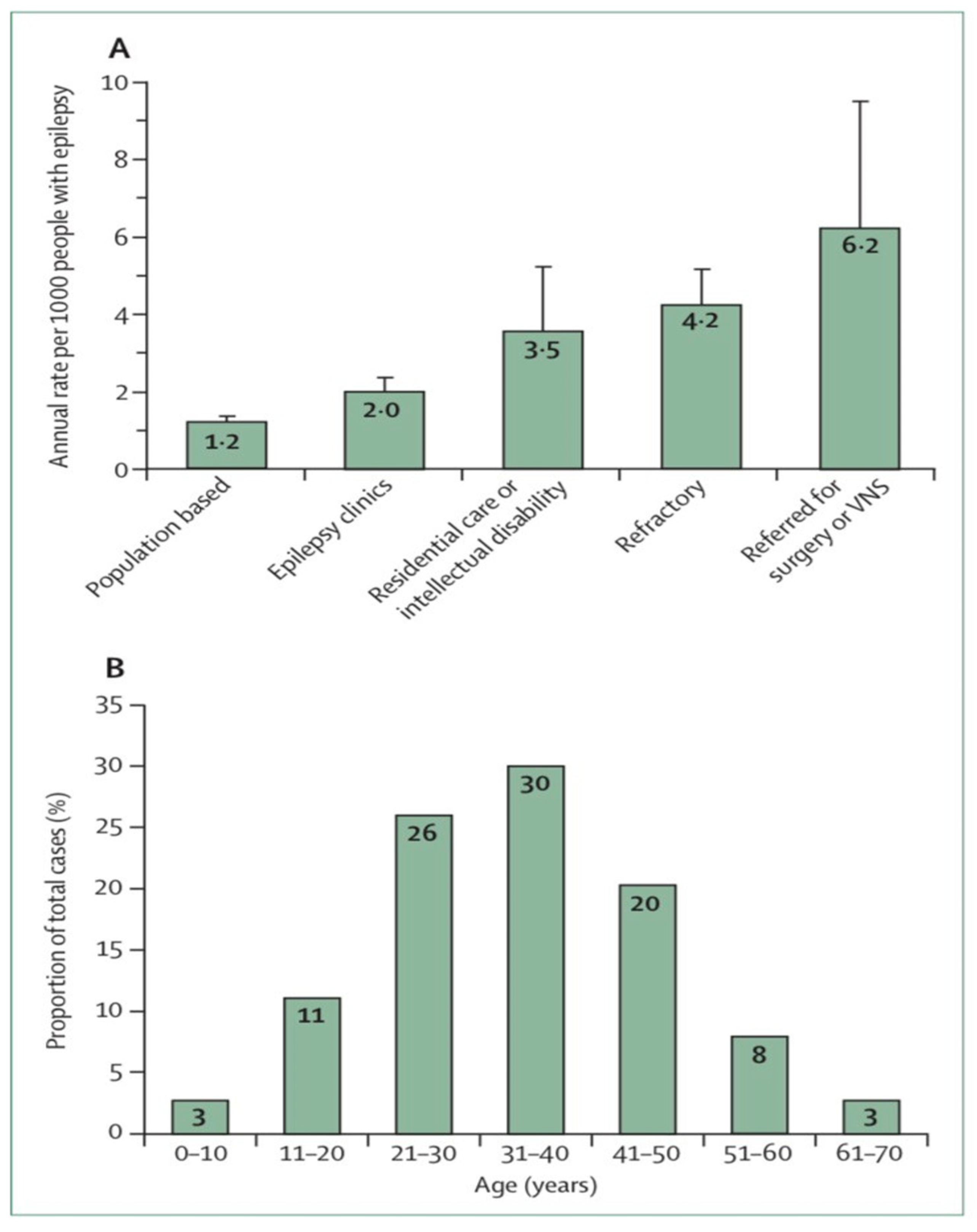
2. Epidemiology
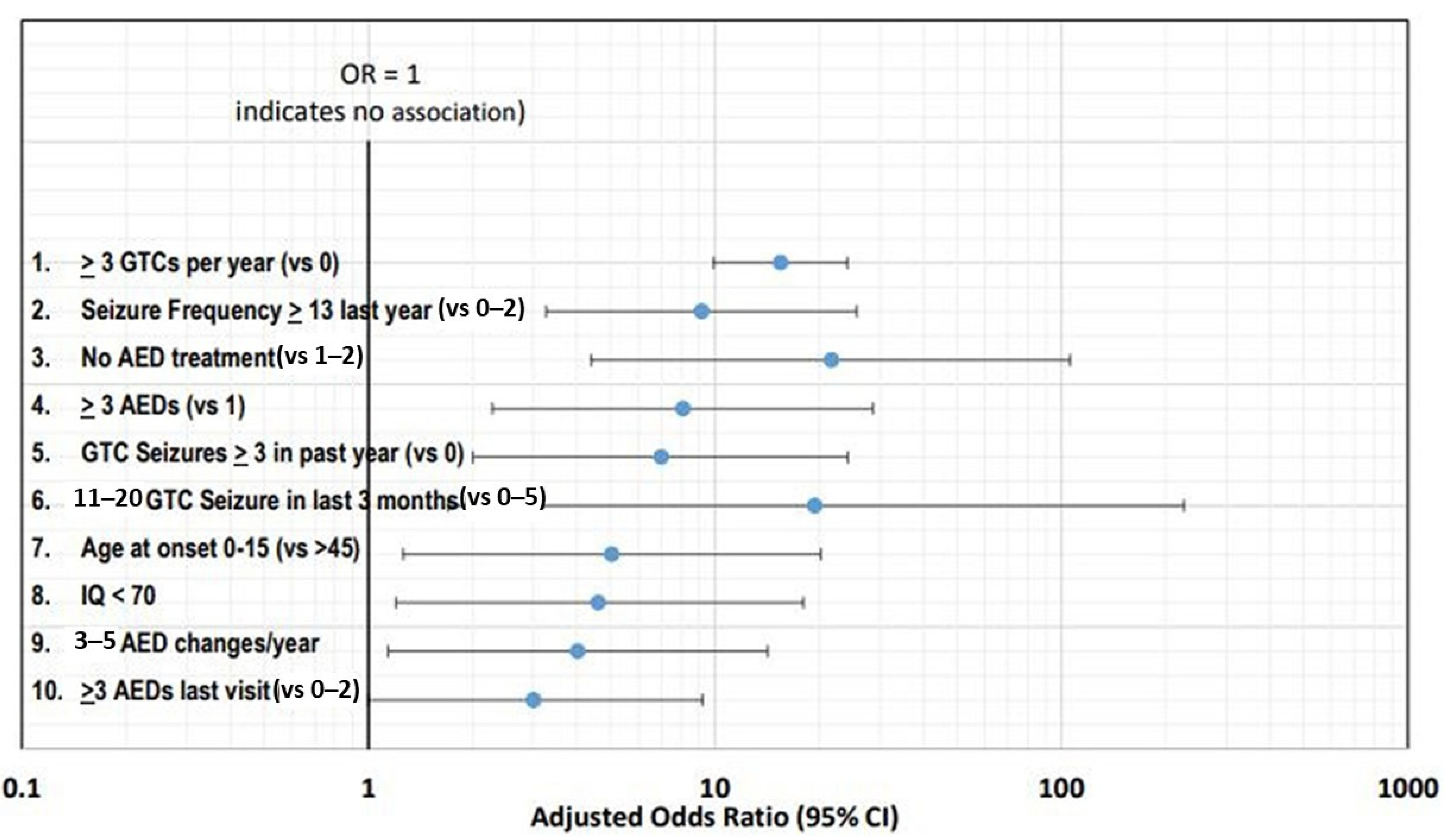
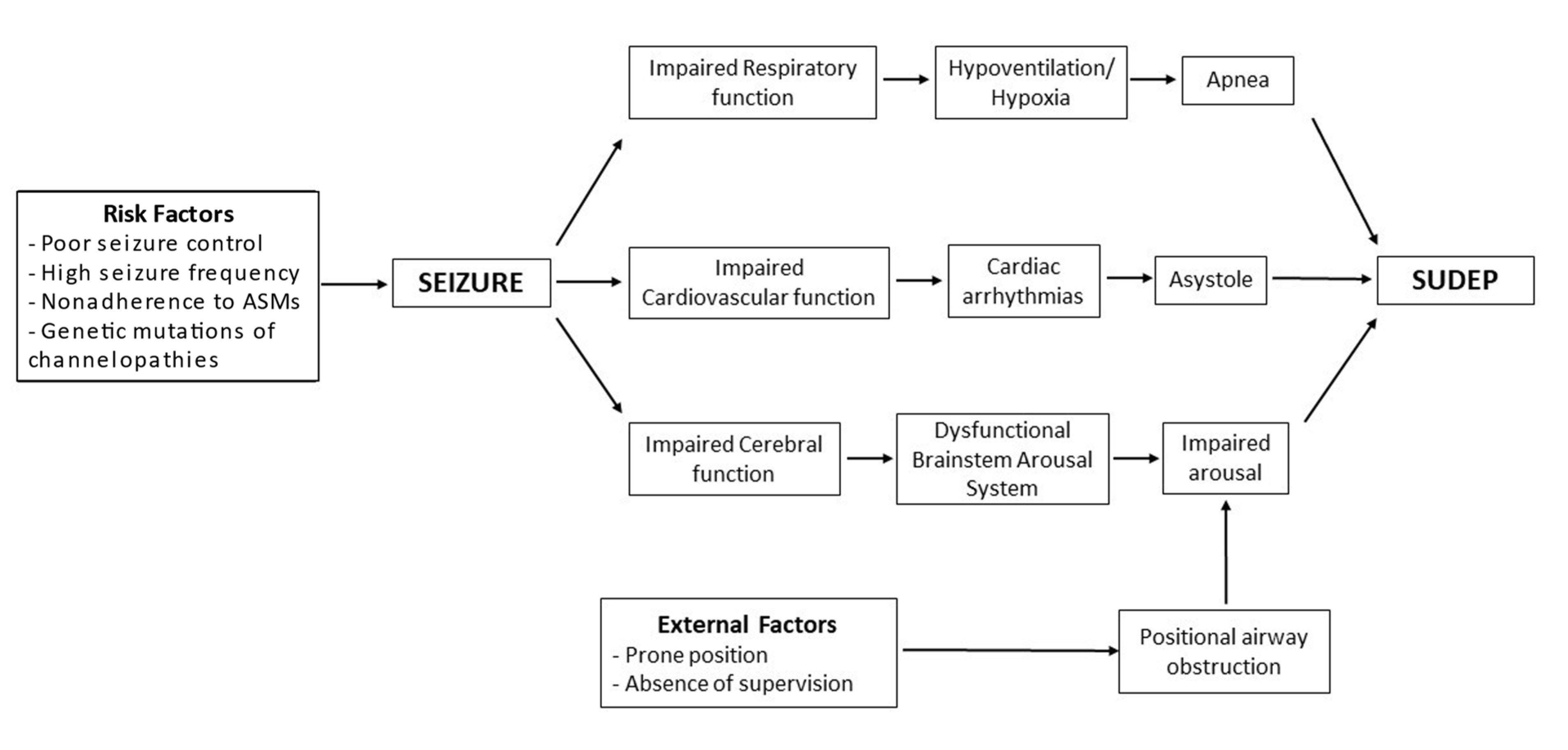
2.1. Risk Factors
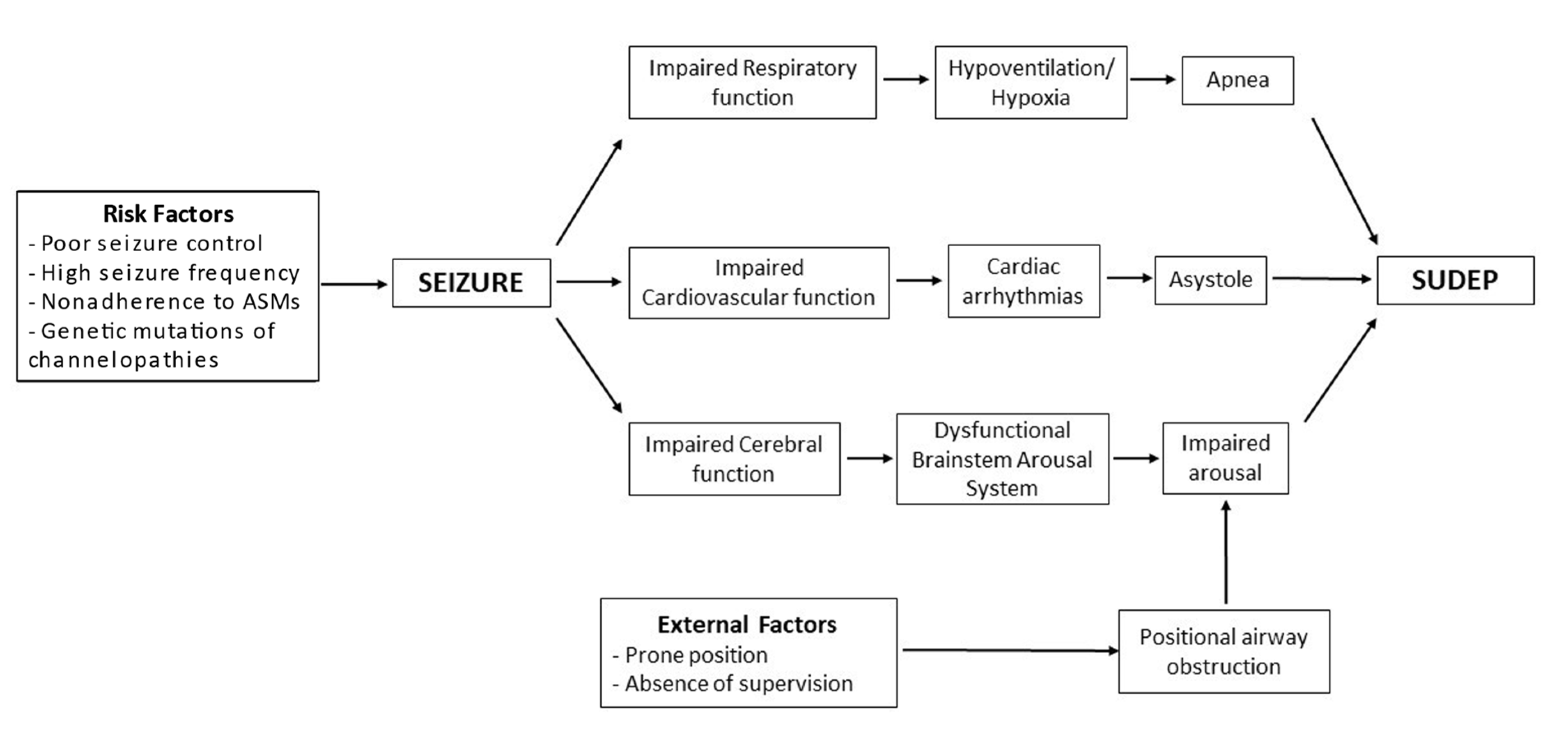
2.2. Pathophysiology
2.2.1. Cardiac Hypothesis
2.2.2. Autonomic Dysfunction
2.2.3. Respiratory and Cerebral Dysfunctions
2.3. Treatment for the Prevention of Sudden Unexpected Death in Epilepsy
2.3.1. Counseling and Education
2.3.2. Optimize Treatment of Drug-Resistant Epilepsy
2.3.3. Seizure-Monitoring Devices
2.3.4. Preventing Airway Obstruction
2.3.5. Reducing Brain and Brainstem Depression from Endogenous Opioids and Adenosine
2.3.6. Cardiac and Diaphragmatic Pacing
2.3.7. Clinical Practice Recommendations
3. Recent Clinical Findings
4. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fisher, R.S.; Acevedo, C.; Arzimanoglou, A.; Bogacz, A.; Cross, J.H.; Elger, C.E., Jr.; Forsgren, L.; French, J.A.; Glynn, M.; Hesdorffer, D.C.; et al. ILAE official report: A practical clinical definition of epilepsy. Epilepsia 2014, 55, 475–482. [Google Scholar] [CrossRef] [Green Version]
- Watila, M.M.; Balarabe, S.A.; Ojo, O.; Keezer, M.R.; Sander, J.W. Overall and cause-specific premature mortality in epilepsy: A systematic review. Epilepsy Behav. EB 2018, 87, 213–225. [Google Scholar] [CrossRef]
- Güngör, M.; Arslan, E.A.; Filik, F.İ.T.; Saygi, S. SUDEP: The First Case Series in Turkey. Noro Psikiyatr. Ars. 2016, 53, 67–71. [Google Scholar] [CrossRef] [Green Version]
- Collazo, I.V.M.; Tatum, W.O. Sudden Unexpected Death in Epilepsy (SUDEP): Are All Your Patients Informed? Neurologist 2016, 21, 66–71. [Google Scholar] [CrossRef]
- Ryvlin, P.; Nashef, L.; Lhatoo, S.D.; Bateman, L.M.; Bird, J.; Bleasel, A.; Boon, P.; Crespel, A.; Dworetzky, B.A.; Høgenhaven, H.; et al. Incidence and mechanisms of cardiorespiratory arrests in epilepsy monitoring units (MORTEMUS): A retrospective study. Lancet Neurol. 2013, 12, 966–977. [Google Scholar] [CrossRef]
- Pathak, S.J.; Yousaf, M.I.K.; Shah, V.B. Sudden Unexpected Death in Epilepsy. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. Available online: http://www.ncbi.nlm.nih.gov/books/NBK559104/ (accessed on 31 March 2022).
- Thurman, D.J.; Hesdorffer, D.C.; French, J.A. Sudden unexpected death in epilepsy: Assessing the public health burden. Epilepsia 2014, 55, 1479–1485. [Google Scholar] [CrossRef]
- Ryvlin, P.; Cucherat, M.; Rheims, S. Risk of sudden unexpected death in epilepsy in patients given adjunctive antiepileptic treatment for refractory seizures: A meta-analysis of placebo-controlled randomised trials. Lancet Neurol. 2011, 10, 961–968. [Google Scholar] [CrossRef]
- Graber, K.D.; Buchhalter, J.; So, E.; Surges, R.; Boison, D.; Kalume, F.; Wright, C.; Gehlbach, B.; Noebels, J.; Whittemore, V.; et al. Summary of the 2016 Partners Against Mortality in Epilepsy (PAME) Conference. Epilepsy Curr. 2016, 16, 1–17. [Google Scholar] [CrossRef]
- Devinsky, O.; Hesdorffer, D.C.; Thurman, D.J.; Lhatoo, S.; Richerson, G. Sudden unexpected death in epilepsy: Epidemiology, mechanisms, and prevention. Lancet Neurol. 2016, 5, 1075–1088. [Google Scholar] [CrossRef]
- Sillanpää, M.; Shinnar, S. Long-term mortality in childhood-onset epilepsy. N. Engl. J. Med. 2010, 363, 2522–2529. [Google Scholar] [CrossRef]
- Mohanraj, R.; Norrie, J.; Stephen, L.J.; Kelly, K.; Hitiris, N.; Brodie, M.J. Mortality in adults with newly diagnosed and chronic epilepsy: A retrospective comparative study. Lancet Neurol. 2006, 5, 481–487. [Google Scholar] [CrossRef]
- May, T.W.; Israel, C.W. Sudden unexpected death in epilepsy (SUDEP): Epidemiology, cardiac and other risk factors. Herzschrittmacherther. Elektrophysiol. 2019, 30, 274–286. [Google Scholar] [CrossRef]
- Tomson, T.; Nashef, L.; Ryvlin, M. Sudden unexpected death in epilepsy: Current knowledge and future directions. Lancet Neurol. 2008, 7, 1021–1031. [Google Scholar] [CrossRef]
- DeGiorgio, C.M.; Markovic, D.; Mazumder, R.; Moseley, B.D. Ranking the Leading Risk Factors for Sudden Unexpected Death in Epilepsy. Front. Neurol. 2017, 8, 473. [Google Scholar] [CrossRef]
- Sathyaprabha, T.N.; Satishchandra, P.; Netravathi, K.; Sinha, S.; Thennarasu, K.; Raju, T.R. Cardiac autonomic dysfunctions in chronic refractory epilepsy. Epilepsy Res. 2006, 72, 49–56. [Google Scholar] [CrossRef]
- Hesdorffer, D.C.; Tomson, T.; Benn, E.; Sander, J.W.; Nilsson, L.; Langan, Y.; Walczak, T.S.; Beghi, E.; Brodie, M.J.; Hauser, A.; et al. Combined analysis of risk factors for SUDEP. Epilepsia 2011, 52, 1150–1159. [Google Scholar] [CrossRef]
- Nilsson, L.; Farahmand, B.Y.; Persson, P.G.; Thiblin, I.; Tomson, T. Risk factors for sudden unexpected death in epilepsy: A case-control study. Lancet Lond. Engl. 1999, 353, 888–893. [Google Scholar] [CrossRef]
- Langan, Y.; Nashef, L.; Sander, J.W. Case-control study of SUDEP. Neurology 2005, 64, 1131–1133. [Google Scholar] [CrossRef]
- Hesdorffer, D.C.; Tomson, T.; Benn, E.; Sander, J.W.; Nilsson, L.; Langan, Y.; Walczak, T.S.; Beghi, E.; Brodie, M.J.; Hauser, W.A. Do antiepileptic drugs or generalized tonic-clonic seizure frequency increase SUDEP risk? A combined analysis. Epilepsia 2012, 53, 249–252. [Google Scholar] [CrossRef]
- Surges, R.; Adjei, P.; Kallis, C.; Erhuero, J.; Scott, C.A.; Bell, G.S.; Sander, J.W.; Walker, M.C. Pathologic cardiac repolarization in pharmacoresistant epilepsy and its potential role in sudden unexpected death in epilepsy: A case-control study. Epilepsia 2010, 51, 233–242. [Google Scholar] [CrossRef]
- Brotherstone, R.; Blackhall, B.; McLellan, A. Lengthening of corrected QT during epileptic seizures. Epilepsia 2010, 51, 221–232. [Google Scholar] [CrossRef]
- Moseley, B.D.; Wirrell, E.C.; Nickels, K.; Johnson, J.N.; Ackerman, M.J.; Britton, J. Electrocardiographic and oximetric changes during partial complex and generalized seizures. Epilepsy Res. 2011, 95, 237–245. [Google Scholar] [CrossRef]
- Surges, R.; Scott, C.A.; Walker, M.C. Enhanced QT shortening and persistent tachycardia after generalized seizures. Neurology 2010, 74, 421–426. [Google Scholar] [CrossRef] [Green Version]
- Surges, R.; Taggart, P.; Sander, J.W.; Walker, M.C. Too long or too short? New insights into abnormal cardiac repolarization in people with chronic epilepsy and its potential role in sudden unexpected death. Epilepsia 2010, 51, 738–744. [Google Scholar] [CrossRef]
- Rejdak, K.; Rubaj, A.; Głowniak, A.; Furmanek, K.; Kutarski, A.; Wysokiński, A.; Stelmasiak, Z. Analysis of ventricular late potentials in signal-averaged ECG of people with epilepsy. Epilepsia 2011, 52, 2118–2124. [Google Scholar] [CrossRef]
- Le Gal, F.; Korff, C.M.; Monso-Hinard, C.; Mund, M.T.; Morris, M.; Malafosse, A.; Schmitt-Mechelke, T. A case of SUDEP in a patient with Dravet syndrome with SCN1A mutation. Epilepsia 2010, 51, 1915–1918. [Google Scholar] [CrossRef]
- Aurlien, D.; Leren, T.P.; Taubøll, E.; Gjerstad, L. New SCN5A mutation in a SUDEP victim with idiopathic epilepsy. Seizure 2009, 18, 158–160. [Google Scholar] [CrossRef] [Green Version]
- Tu, E.; Bagnall, R.D.; Duflou, J.; Semsarian, C. Post-mortem review and genetic analysis of sudden unexpected death in epilepsy (SUDEP) cases. Brain Pathol. Zur. Switz. 2011, 21, 201–208. [Google Scholar] [CrossRef]
- Johnson, J.N.; Tester, D.J.; Bass, N.E.; Ackerman, M.J. Cardiac channel molecular autopsy for sudden unexpected death in epilepsy. J. Child Neurol. 2010, 25, 916–921. [Google Scholar] [CrossRef]
- Tu, E.; Waterhouse, L.; Duflou, J.; Bagnall, R.D.; Semsarian, C. Genetic analysis of hyperpolarization-activated cyclic nucleotide-gated cation channels in sudden unexpected death in epilepsy cases. Brain Pathol. Zur. Switz. 2011, 21, 692–698. [Google Scholar] [CrossRef]
- Glasscock, E. Genomic biomarkers of SUDEP in brain and heart. Epilepsy Behav. EB 2014, 38, 172–179. [Google Scholar] [CrossRef] [Green Version]
- Lehnart, S.E.; Mongillo, M.; Bellinger, A.; Lindegger, N.; Chen, B.; Hsueh, W.; Reiken, S.; Wronska, A.; Drew, L.J.; Ward, C.W.; et al. Leaky Ca2+ release channel/ryanodine receptor 2 causes seizures and sudden cardiac death in mice. J. Clin. Investig. 2008, 118, 2230–2245. [Google Scholar] [CrossRef] [Green Version]
- Goldman, A.M.; Glasscock, E.; Yoo, J.; Chen, T.T.; Klassen, T.L.; Noebels, J.L. Arrhythmia in heart and brain: KCNQ1 mutations link epilepsy and sudden unexplained death. Sci. Transl. Med. 2009, 1, 2ra6. [Google Scholar] [CrossRef] [Green Version]
- Nagrani, T.; Siyamwala, M.; Vahid, G.; Bekheit, S. Ryanodine calcium channel: A novel channelopathy for seizures. Neurologist 2011, 17, 91–94. [Google Scholar] [CrossRef]
- Rugg-Gunn, F.J.; Simister, R.J.; Squirrell, M.; Holdright, D.R.; Duncan, J.S. Cardiac arrhythmias in focal epilepsy: A prospective long-term study. Lancet Lond. Engl. 2004, 364, 2212–2219. [Google Scholar] [CrossRef]
- Britton, J.W.; Ghearing, G.R.; Benarroch, E.E.; Cascino, G.D. The ictal bradycardia syndrome: Localization and lateralization. Epilepsia 2006, 47, 737–744. [Google Scholar] [CrossRef]
- Lanz, M.; Oehl, B.; Brandt, A.; Schulze-Bonhage, A. Seizure induced cardiac asystole in epilepsy patients undergoing long term video-EEG monitoring. Seizure 2011, 20, 167–172. [Google Scholar] [CrossRef] [Green Version]
- Kerling, F.; Dütsch, M.; Linke, R.; Kuwert, T.; Stefan, H.; Hilz, M.J. Relation between ictal asystole and cardiac sympathetic dysfunction shown by MIBG-SPECT. Acta Neurol. Scand. 2009, 120, 123–129. [Google Scholar] [CrossRef]
- Strzelczyk, A.; Cenusa, M.; Bauer, S.; Hamer, H.M.; Mothersill, I.W.; Grunwald, T.; Hillenbrand, B.; Ebner, A.; Steinhoff, B.J.; Krämer, G.; et al. Management and long-term outcome in patients presenting with ictal asystole or bradycardia. Epilepsia 2011, 52, 1160–1167. [Google Scholar] [CrossRef]
- Moseley, B.D.; Ghearing, G.R.; Munger, T.M.; Britton, J.W. The treatment of ictal asystole with cardiac pacing. Epilepsia 2011, 52, e16–e19. [Google Scholar] [CrossRef]
- Stöllberger, C.; Wegner, C.; Finsterer, J. Seizure-associated Takotsubo cardiomyopathy. Epilepsia 2011, 52, e160–e167. [Google Scholar] [CrossRef]
- Dupuis, M.; van Rijckevorsel, K.; Evrard, F.; Dubuisson, N.; Dupuis, F.; van Robays, P. Takotsubo syndrome (TKS): A possible mechanism of sudden unexplained death in epilepsy (SUDEP). Seizure 2012, 21, 51–54. [Google Scholar] [CrossRef] [Green Version]
- Zijlmans, M.; Flanagan, D.; Gotman, J. Heart rate changes and ECG abnormalities during epileptic seizures: Prevalence and definition of an objective clinical sign. Epilepsia 2002, 43, 847–854. [Google Scholar] [CrossRef] [Green Version]
- Mukherjee, S.; Tripathi, M.; Chandra, P.S.; Yadav, R.; Choudhary, N.; Sagar, R.; Bhore, R.; Pandey, R.M.; Deepak, K.K. Cardiovascular autonomic functions in well-controlled and intractable partial epilepsies. Epilepsy Res. 2009, 85, 261–269. [Google Scholar] [CrossRef]
- Lotufo, P.A.; Valiengo, L.; Benseñor, I.M.; Brunoni, A.R. A systematic review and meta-analysis of heart rate variability in epilepsy and antiepileptic drugs. Epilepsia 2012, 53, 272–282. [Google Scholar] [CrossRef]
- Lossius, M.I.; Erikssen, J.E.; Mowinckel, P.; Gulbrandsen, P.; Gjerstad, L. Changes in autonomic cardiac control in patients with epilepsy after discontinuation of antiepileptic drugs: A randomized controlled withdrawal study. Eur. J. Neurol. 2007, 14, 1022–1028. [Google Scholar] [CrossRef]
- Suorsa, E.; Korpelainen, J.T.; Ansakorpi, H.; Huikuri, H.V.; Suorsa, V.; Myllylä, V.V.; Isojärvi, J.I.T. Heart rate dynamics in temporal lobe epilepsy-A long-term follow-up study. Epilepsy Res. 2011, 93, 80–83. [Google Scholar] [CrossRef]
- Yildiz, G.U.; Apaydın, E.; Umuttan, D.; Tokgoz, D.O.S.; Ozdemir, K.; Genca, B.O.; İlhana, N. Analysis of 24-hour heart rate variations in patients with epilepsy receiving antiepileptic drugs. Epilepsy Behav. EB 2011, 20, 349–354. [Google Scholar] [CrossRef]
- Rauscher, G.; DeGiorgio, A.C.; Miller, P.R.; De Giorgio, C.M. Sudden unexpected death in epilepsy associated with progressive deterioration in heart rate variability. Epilepsy Behav. EB 2011, 21, 103–105. [Google Scholar] [CrossRef]
- So, E.L.; Sam, M.C.; Lagerlund, T.L. Postictal central apnea as a cause of SUDEP: Evidence from near-SUDEP incident. Epilepsia 2000, 41, 1494–1497. [Google Scholar] [CrossRef]
- Pezzella, M.; Striano, P.; Ciampa, C.; Errichiello, L.; Penza, P.; Striano, S. Severe pulmonary congestion in a near miss at the first seizure: Further evidence for respiratory dysfunction in sudden unexpected death in epilepsy. Epilepsy Behav. EB 2009, 14, 701–702. [Google Scholar] [CrossRef]
- Tao, J.X.; Qian, S.; Baldwin, M.; Chen, X.J.; Rose, S.; Ebersole, S.H.; Ebersole, J.S. SUDEP, suspected positional airway obstruction, and hypoventilation in postictal coma. Epilepsia 2010, 51, 2344–2347. [Google Scholar] [CrossRef]
- Tavee, J.; Morris, H. Severe postictal laryngospasm as a potential mechanism for sudden unexpected death in epilepsy: A near-miss in an EMU. Epilepsia 2008, 49, 2113–2117. [Google Scholar] [CrossRef]
- Bateman, L.M.; Li, C.-S.; Seyal, M. Ictal hypoxemia in localization-related epilepsy: Analysis of incidence, severity and risk factors. Brain J. Neurol. 2008, 131, 3239–3245. [Google Scholar] [CrossRef]
- Seyal, M.; Bateman, L.M. Ictal apnea linked to contralateral spread of temporal lobe seizures: Intracranial EEG recordings in refractory temporal lobe epilepsy. Epilepsia 2009, 50, 2557–2562. [Google Scholar] [CrossRef]
- Lhatoo, S.D.; Faulkner, H.J.; Dembny, K.; Trippick, K.; Johnson, C.; Bird, J.M. An electroclinical case-control study of sudden unexpected death in epilepsy. Ann. Neurol. 2010, 68, 787–796. [Google Scholar] [CrossRef]
- Surges, R.; Strzelczyk, A.; Scott, C.A.; Walker, M.C.; Sander, J.W. Postictal generalized electroencephalographic suppression is associated with generalized seizures. Epilepsy Behav. EB 2011, 21, 271–274. [Google Scholar] [CrossRef]
- Maguire, M.J.; Jackson, C.F.; Marson, A.G.; Nevitt, S.J. Treatments for the prevention of Sudden Unexpected Death in Epilepsy (SUDEP). Cochrane Database Syst. Rev. 2020, 4, CD011792. [Google Scholar] [CrossRef]
- Bhasin, H.; Sharma, S.; Ramachandrannair, R. Can We Prevent Sudden Unexpected Death in Epilepsy (SUDEP)? Can. J. Neurol. Sci. J. Can. Sci. Neurol. 2021, 48, 464–468. [Google Scholar] [CrossRef]
- Pensel, M.C.; Nass, R.D.; Taubøll, E.; Aurlien, D.; Surges, R. Prevention of sudden unexpected death in epilepsy: Current status and future perspectives. Expert Rev. Neurother. 2020, 20, 497–508. [Google Scholar] [CrossRef]
- Sveinsson, O.; Andersson, T.; Mattsson, P.; Carlsson, S.; Tomson, T. Clinical risk factors in SUDEP: A nationwide population-based case-control study. Neurology 2020, 94, e419–e429. [Google Scholar] [CrossRef] [Green Version]
- Cross, J.H.; Galer, B.S.; Gil-Nagel, A.; Devinsky, O.; Ceulemans, B.; Lagae, L.; Schoonjans, A.; Donner, E.; Wirrell, E.; Kothare, S.; et al. Impact of fenfluramine on the expected SUDEP mortality rates in patients with Dravet syndrome. Seizure 2021, 93, 154–159. [Google Scholar] [CrossRef] [PubMed]
- Salanova, V.; Sperling, M.R.; Gross, R.E.; Irwin, C.P.; Vollhaber, J.A.; Giftakis, J.E.; Fisher, R.S.; SANTÉ Study Group. The SANTÉ study at 10 years of follow-up: Effectiveness, safety, and sudden unexpected death in epilepsy. Epilepsia 2021, 62, 1306–1317. [Google Scholar] [CrossRef] [PubMed]
- Vilella, L.; Lacuey, N.; Hampson, J.P.; Rani, M.R.S.; Sainju, R.K.; Friedman, D.; Nei, M.; Strohl, K.; Scott, C.; Gehlbach, B.K.; et al. Postconvulsive central apnea as a biomarker for sudden unexpected death in epilepsy (SUDEP). Neurology 2019, 92, e171–e182. [Google Scholar] [CrossRef] [Green Version]
- Myers, K.A.; Bello-Espinosa, L.E.; Symonds, J.D.; Zuberi, S.M.; Clegg, R.; Sadleir, L.G.; Buchhalter, J.; Scheffer, I.E. Heart rate variability in epilepsy: A potential biomarker of sudden unexpected death in epilepsy risk. Epilepsia 2018, 59, 1372–1380. [Google Scholar] [CrossRef] [Green Version]
- Sivathamboo, S.; Friedman, D.; Laze, J.; Nightscales, R.; Chen, Z.; Kuhlmann, L.; Devore, S.; Macefield, V.; Kwan, P.; D’Souza, W.; et al. Association of Short-term Heart Rate Variability and Sudden Unexpected Death in Epilepsy. Neurology 2021, 97, e2357–e2367. [Google Scholar] [CrossRef]
- Cihan, E.; Hesdorffer, D.C.; Brandsoy, M.; Li, L.; Fowler, D.R.; Graham, J.K.; Karlovich, M.; Donner, E.J.; Devinsky, O.; Friedman, D. Socioeconomic disparities in SUDEP in the US. Neurology 2020, 94, e2555. [Google Scholar] [CrossRef] [PubMed]
- Rasekhi, R.T.; Devlin, K.N.; Mass, J.A.; Donmez, M.; Asma, B.; Sperling, M.R.; Nei, M. Improving prediction of sudden unexpected death in epilepsy: From SUDEP-7 to SUDEP-3. Epilepsia 2021, 62, 1536–1545. [Google Scholar] [CrossRef]
- Bagnall, R.D.; Crompton, D.E.; Petrovski, S.; Lam, L.; Cutmore, C.; Garry, S.I.; Sadleir, L.G.; Dibbens, L.M.; Cairns, A.; Kivity, S.; et al. Exome-based analysis of cardiac arrhythmia, respiratory control, and epilepsy genes in sudden unexpected death in epilepsy. Ann. Neurol. 2016, 79, 522–534. [Google Scholar] [CrossRef]
- Chahal, C.A.A.; Salloum, M.N.; Alahdab, F.; Gottwald, J.A.; Tester, D.J.; Anwer, L.A.; So, E.L.; Murad, M.H.; Louis, E.K.S.; Ackerman, M.J.; et al. Systematic Review of the Genetics of Sudden Unexpected Death in Epilepsy: Potential Overlap with Sudden Cardiac Death and Arrhythmia-Related Genes. J. Am. Heart Assoc. 2020, 9, e012264. [Google Scholar] [CrossRef]
- Günbey, C. ICNApedia—Cardiac Autonomic Dysfunction in SUDEP. ICNApedia. Available online: https://icnapedia.org/education/journal-watch/cardiac-autonomic-dysfunction-in-sudep (accessed on 24 February 2022).
- Surges, R.; Rd, T.; Hl, T.; Jw, S. Sudden unexpected death in epilepsy: Risk factors and potential pathomechanisms. Nat. Rev. Neurol. 2009, 5, 492–504. [Google Scholar] [CrossRef]
- Devinsky, O.; Friedman, D.; Duckrow, R.B.; Fountain, N.B.; Gwinn, R.P.; Leiphart, J.W.; Murro, A.M.; van Ness, P.C. Sudden unexpected death in epilepsy in patients treated with brain-responsive neurostimulation. Epilepsia 2018, 59, 555–561. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
{kind=link}
| Gene | Clinical Condition | Function | SUDEP Hypothesis |
|---|---|---|---|
| SCN1A | Dravet syndrome, generalizedepilepsy with febrile seizures | Sodium channel | Increases epilepsyseverity by postictal parasympathetichyperactivity |
| SCN2A | Epileptic encephalopathy | Sodium channel | Increases severity of epilepsy |
| SCN8A | Epileptic encephalopathy | Sodium channel | Increases severity of epilepsy |
| PRRT2 | Benign familial infantile seizures | Proline-rich transmembrane protein 2 | Potential interaction withSNAP-25 and presynapticneurotransmitter release |
| DEPDC5 | Focal epilepsy | G-protein signaling pathway, inhibits the mTORC1 pathway | Potential increase in severity of epilepsy |
| CSTB | Unverricht-Lundborg disease | Inhibits intracellular thiol protease, prevents protease leakage from Lysosomes | Increases severity of epilepsy and neurological impairment due toprogressive myoclonic epilepsy |
| TSC1, TSC2 | Tuberous sclerosis complex | Downregulates mTORC1 pathway | Potential increase in severity of epilepsy |
| HCN2 | Generalized epilepsy | Contributes to spontaneous rhythmic activity in SA node and brain | Potential impairment inbrainstem or cardiac pacemaker cells |
| KCNQ1 | Long QT syndrome | Potassium channel; ventricular repolarization | Potentialarrhythmogenic effect |
| KCNH2 | Long QT syndrome | Potassium channel;repolarization of cardiac action potential | Uncertain |
| SCN5A | Long QT syndrome | Sodium channel; rapid depolarizing sodium current underlying cardiac action potential upstroke | Potential combination of epilepsy and arrhythmia |
| NOS1AP | Long QT syndrome | Cytosolic protein that binds to neuronal nitric oxide synthase | Potential combination of epilepsy and arrhythmia |
| RYR2 | Sudden cardiac death | Cardiac ryanodine receptor 2; intracellular calcium release channel, coupling excitation–contraction | Potential combination of epilepsy and arrhythmia |
| HCN4 | Bradycardia, sick sinus syndrome | Potassiumchannel; slow kinetics of activation and inactivation, cardiacpacemaker role | Variant identified in SUDEP |
| Grade B | Effective epilepsy treatment to decrease the burden of GTCS protects against SUDEP. Providers should use appropriate anti-seizure medications and combine ASM where necessary to achieve seizure control, while actively involving patients in their care and weighing the safety profile of the medications. |
| Grade C | Based on risk profile and psychosocial circumstances, clinicians should selectively counsel patients with frequent uncontrolled nocturnal seizures on nocturnal supervision, as this is protective against SUDEP. |
| Grade C | Prompt referral for surgical evaluation of drug-resistant epilepsy/lesional epilepsy is of paramount importance in reducing the risk of SUDEP. |
| Author (Year) | Intervention | Results and Findings | Conclusion |
|---|---|---|---|
| J. Helen Cross et al. (2021) [63] | Fenfluramine (FFA) added to anti-seizure medication for Dravet syndrome patients to assess its effect on the SUDEP mortality rate. | All-cause and SUDEP mortality rates were significantly lower than expected compared to estimates from literature studies. | FFA might have a role in reducing SUDEP in patients with Dravet syndrome. More studies will be required to ascertain if this effect is sustainable and applicable to other causes of SUDEP. |
| V. Salanova et al. (2021) [64] | Adults with severe epilepsy underwent deep brain stimulation surgery with leads implanted in the anterior thalamus (ANT DBS). They were followed up over 7–10 years. | The observed SUDEP rate was lower for patients with drug-resistant epilepsy, including patients being treated with adjunctive ASMs or considered for epilepsy surgery. | ANT DBS is associated with sustained improvement in seizure reduction over time. This reduction is possibly responsible for the reduction in SUDEP risk. |
| Vilella et al. (2019) [65] | Patients with intractable epilepsy (n = 87) underwent monitoring of autonomic and breathing biomarkers in epilepsy monitoring units. | Post-convulsive central apnea (PCCA) was associated with near-SUDEP phenomena and SUDEP. | The authors suggest PCCA is a possible SUDEP biomarker. |
| Author (Year) | Groups Studied | Results and Findings | Conclusion |
|---|---|---|---|
| Myers et al. (2018) [66] | HRV data were compared between a group of patients with SCN mutation drug-resistant epilepsy and a control group of non-SCN drug-resistant epilepsy. | SUDEP patients had more severe autonomic dysregulation. This dysregulation was worse in the SCN mutation group. | The authors suggest autonomic dysfunction is associated with SUDEP risk in patients with epilepsy due to SCN mutations. |
| Sivathamboo et al. (2021) [67] | A retrospective nested case–control study evaluated interictal ECG recordings among patients admitted for video EEG recording | Normalized LFP was lower in SUDEP cases than in matched controls. Every 1% reduction in normalized LFP conferred a 2.7% increase in latency to SUDEP. | The authors conclude reduced short-term LFP is associated with SUDEP. They suggest that increased LFP may be associated with longer survival. |
| Cihan et al. (2020) [68] | Over 2 years and in 3 diverse geographic regions, SUDEP rates plus certain demographic, biometric, and clinical variables were compared with community SES. | 159 SUDEP cases in the lowest quartile zip codes and 49 cases in the highest quartile zip codes. No reported difference in age, sex, BMI, epilepsy etiology, circumstances of death, nonadherence to medication, and comorbid conditions between highest and lowest quartile SES zip codes. | The authors concluded SUDEP rates were >2 times higher among people with epilepsy living in lowest income communities compared to the highest income communities. |
| Rasekhi et al. (2021) [69] | A retrospective case–control study evaluated 48 patients with epilepsy who underwent EEG monitoring and subsequently died of definite or probable SUDEP. Two matched controls with epilepsy were identified for each individual who died of SUDEP. | SUDEP-7 scores were significantly higher in the SUDEP group than in matched controls, both at the time of admission and last follow-up. | The authors conclude that results support the ability of SUDEP-7 inventory to predict SUDEP. However, it does not enhance the prediction of SUDEP over-generalized tonic-clonic seizure or seizure frequency alone. They propose a new tool—SUDEP-3 inventory, which improves predictive performance. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
O’Neal, T.B.; Shrestha, S.; Singh, H.; Osagie, I.; Ben-Okafor, K.; Cornett, E.M.; Kaye, A.D. Sudden Unexpected Death in Epilepsy. Neurol. Int. 2022, 14, 600-613. https://doi.org/10.3390/neurolint14030048
O’Neal TB, Shrestha S, Singh H, Osagie I, Ben-Okafor K, Cornett EM, Kaye AD. Sudden Unexpected Death in Epilepsy. Neurology International. 2022; 14(3):600-613. https://doi.org/10.3390/neurolint14030048
Chicago/Turabian StyleO’Neal, Teri B., Sanjay Shrestha, Harsimar Singh, Ihianle Osagie, Kenechukwu Ben-Okafor, Elyse M. Cornett, and Alan D. Kaye. 2022. "Sudden Unexpected Death in Epilepsy" Neurology International 14, no. 3: 600-613. https://doi.org/10.3390/neurolint14030048
APA StyleO’Neal, T. B., Shrestha, S., Singh, H., Osagie, I., Ben-Okafor, K., Cornett, E. M., & Kaye, A. D. (2022). Sudden Unexpected Death in Epilepsy. Neurology International, 14(3), 600-613. https://doi.org/10.3390/neurolint14030048