Extending Thrombolysis in Acute Ischemic Stroke to Primary Care: Early Experiences with a Network-Based Teleneurology Approach

 ,
, 
Abstract
:1. Introduction
2. Methods
2.1. Data
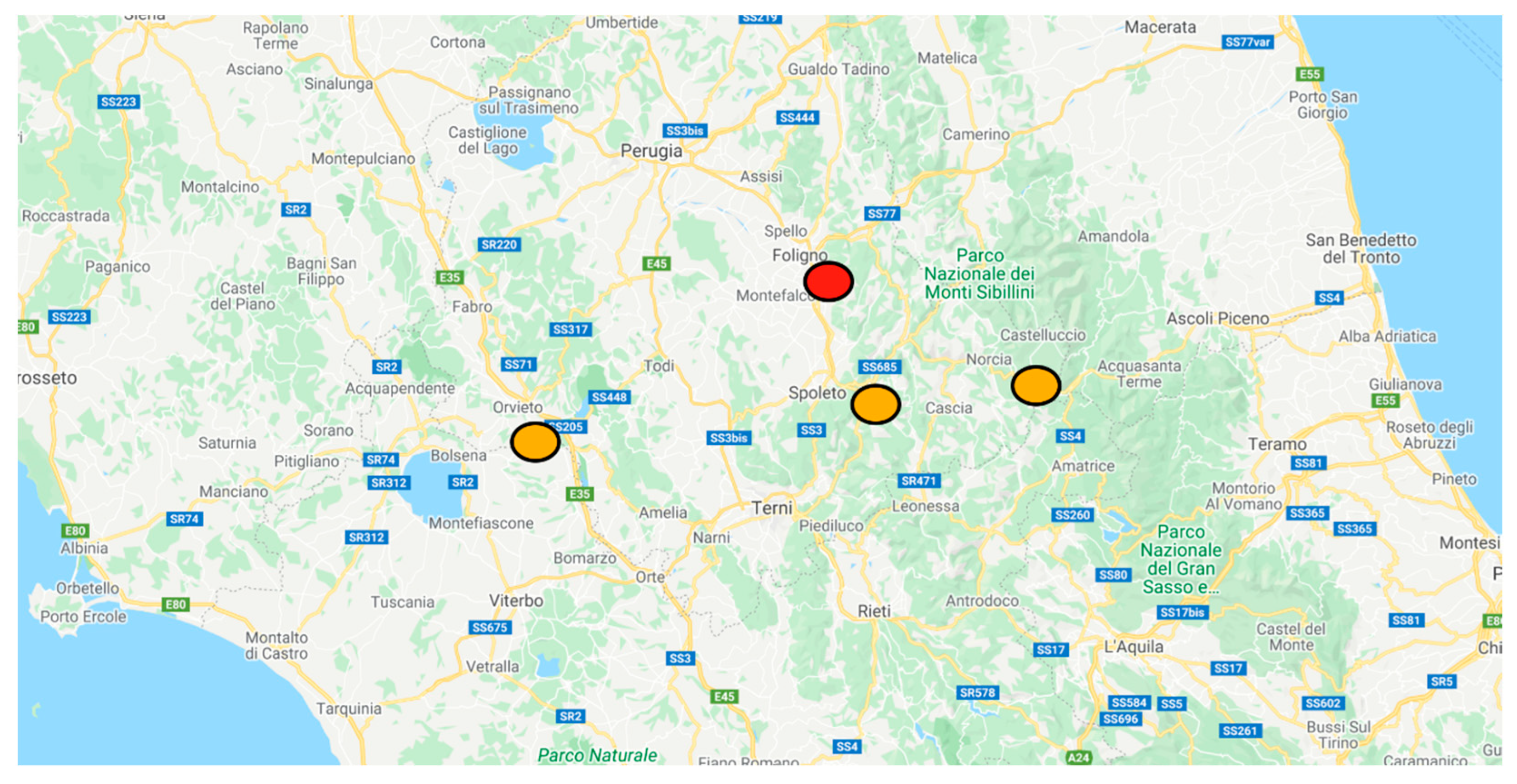
2.2. Teleneurology System
- -
- Access to Orvieto CT images via RIS/PACS system.
- -
- Patient televisit in the presence of medical and/or nursing staff in Orvieto Emergency Department.
2.3. Statistics and Data Management
3. Results
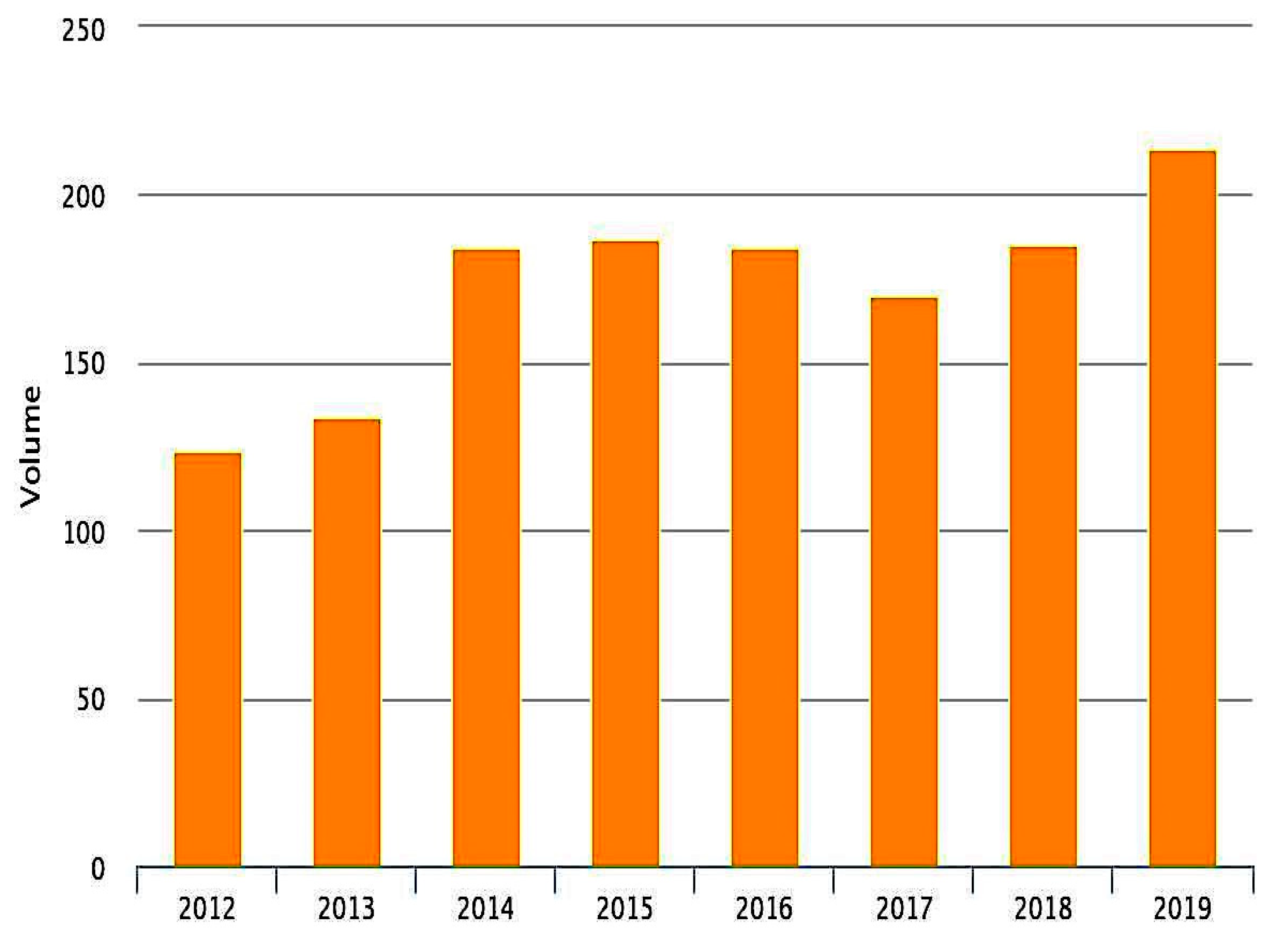
3.1. Volume of Admissions
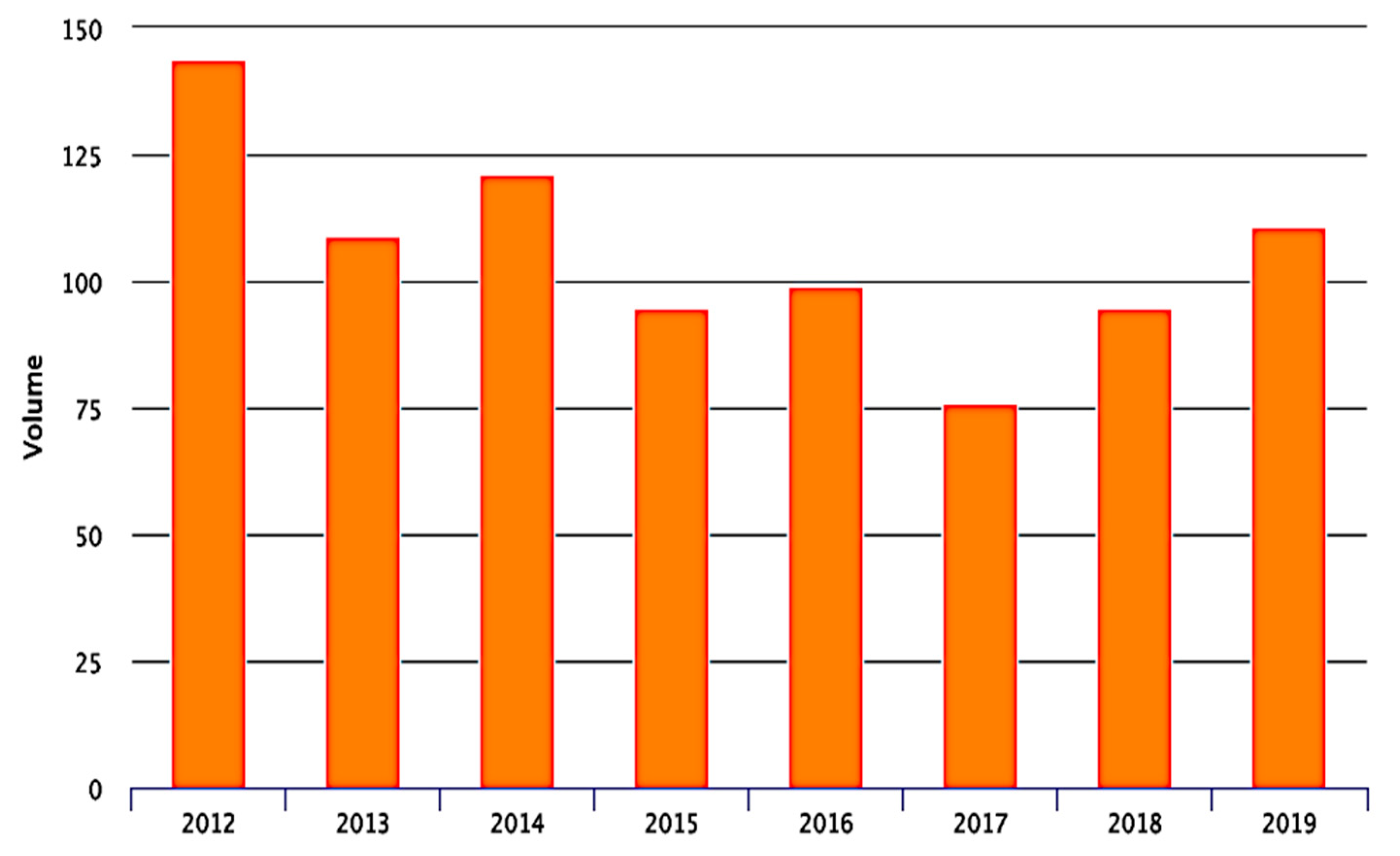
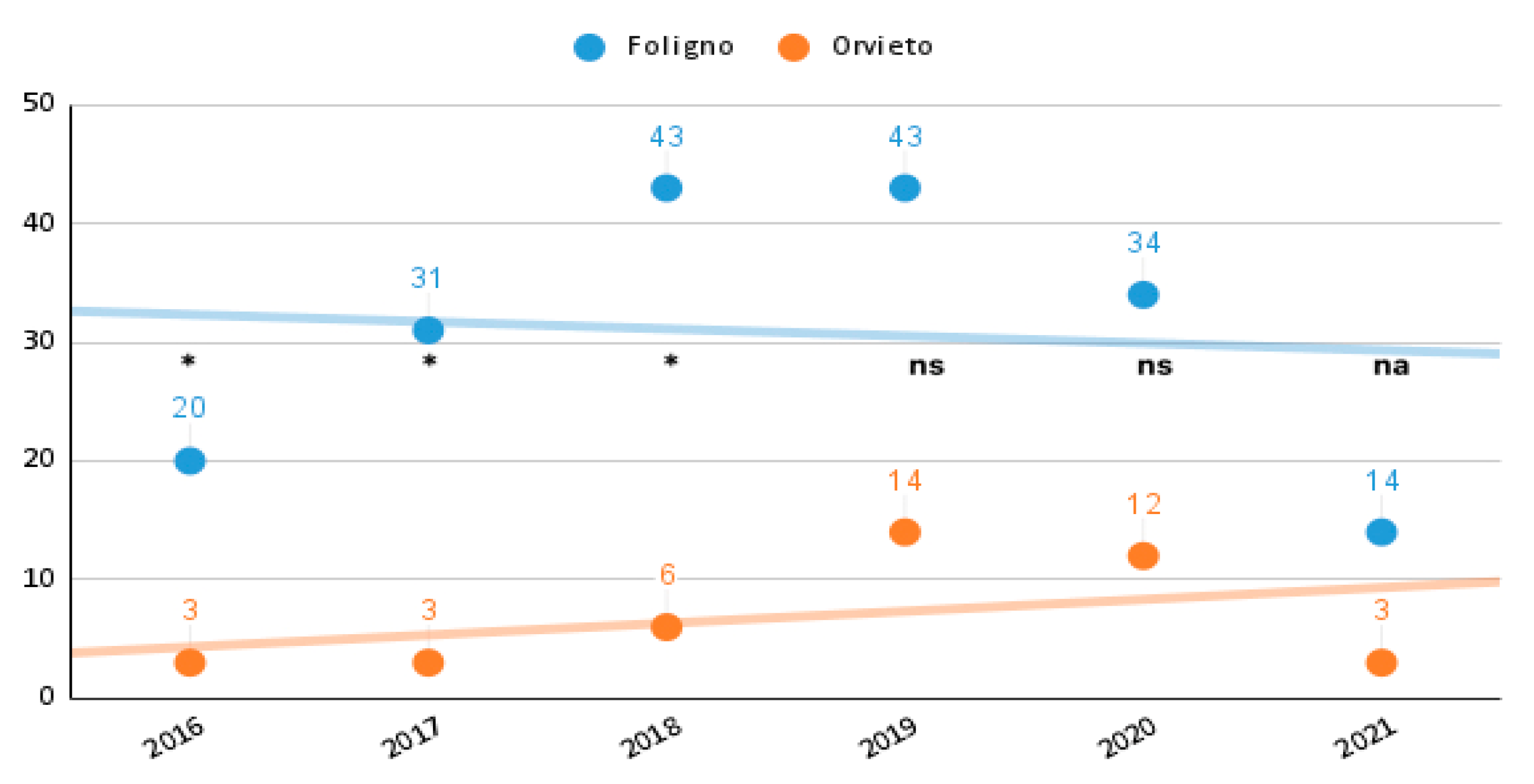
3.2. Thrombolytic Procedures
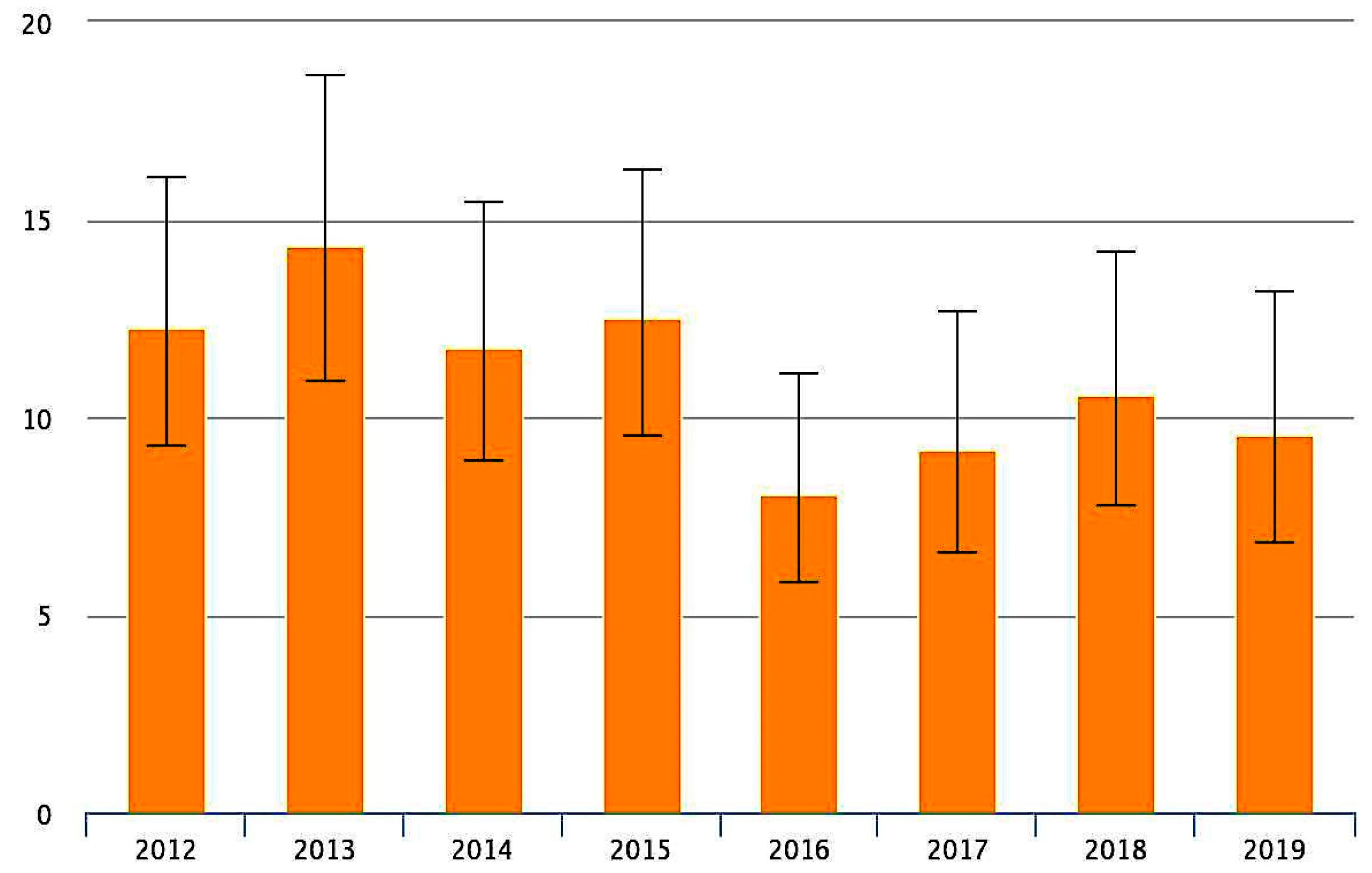
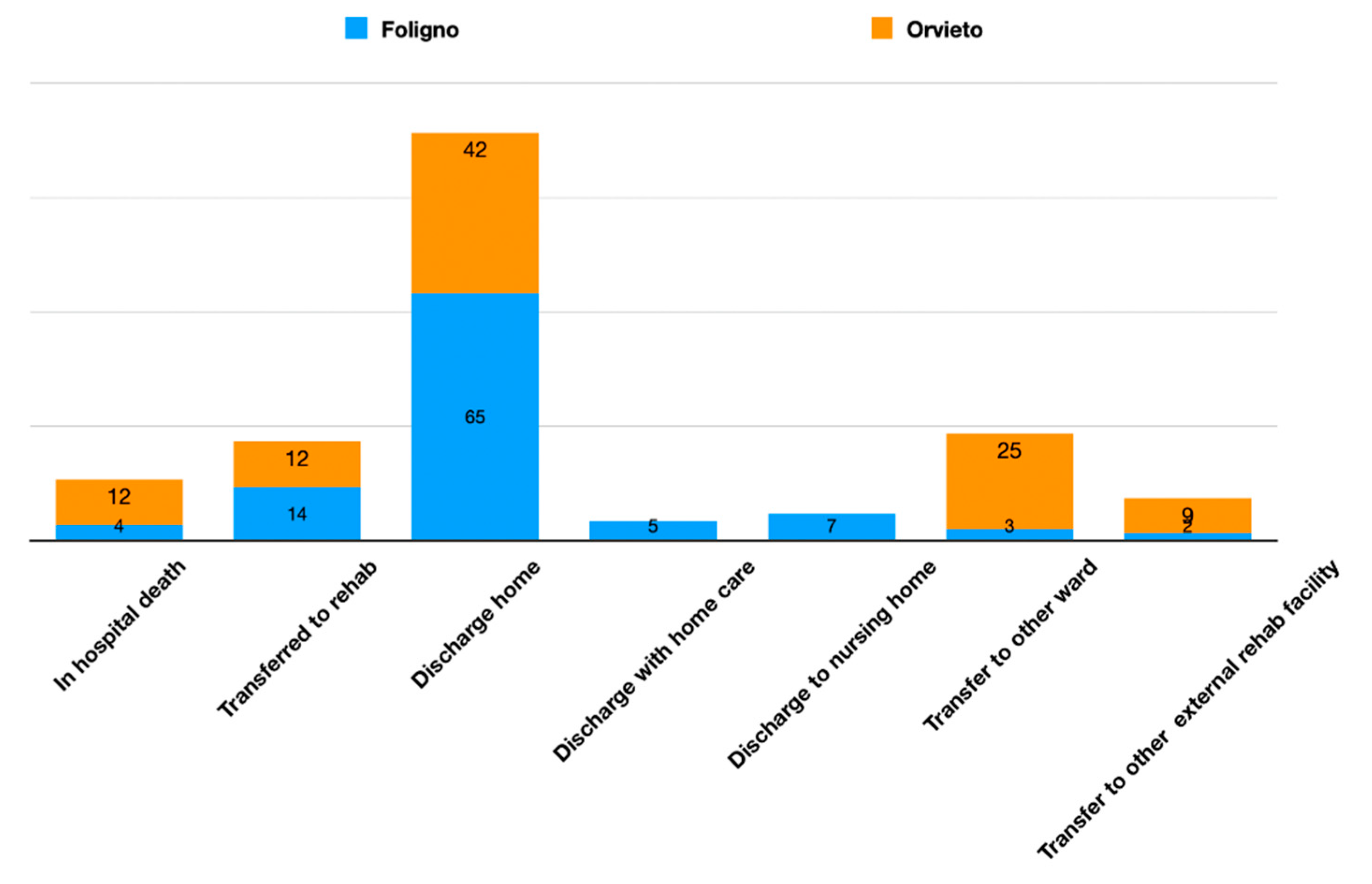
3.3. Distribution of Hospital Discharge
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wein, T.H.; Hickenbottom, S.L.; Alexandrov, A.V. Thrombolysis, stroke units and other strategies for reducing acute stroke costs. Pharm.-Econ. 1998, 14, 603–611. [Google Scholar] [CrossRef]
- Sinclair, S.E.; Frighetto, L.; Loewen, P.S.; Sunderji, R.; Teal, P.; Fagan, S.C.; Marra, C.A. Cost-utility analysis of tissue plasminogen activator therapy for acute ischaemic stroke: A Canadian healthcare perspective. Pharm.-Econ. 2001, 19, 927–936. [Google Scholar] [CrossRef]
- Audebert, H.J.; Kukla, C.; von Claranau, S.C.; Kühn, J.; Vatankhah, B.; Schenkel, J.; Ickenstein, G.W.; Haberl, R.L.; Horn, M. Telemedicine for Safe and Extended Use of Thrombolysis in Stroke. Stroke 2005, 36, 287–291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hubert, G.J.; Santo, G.; Vanhooren, G.; Zvan, B.; Campos, S.T.; Alasheev, A.; Abilleira, S.; Corea, F. Recommendations on telestroke in Europe. Eur. Stroke J. 2018, 4, 101–109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agostoni, E.C.; Carolei, A.; Micieli, G.; Provinciali, L.; Toni, D.; Vidale, S. The organisation of the acute ischemic stroke management: Key notes of the Italian Neurological Society and of the Italian Stroke Organization. Neurol. Sci. 2017, 39, 415–422. [Google Scholar] [CrossRef] [PubMed]
- di Poggio, M.B.; Toni, D.; Gandolfo, C.; Paolicelli, D.; Zini, A.; Agostoni, E.; Bandini, F.; Ragno, M.; Altavista, M.C.; Bertolotto, A.; et al. Coverage of the requirements of first and second level stroke unit in Italy. Neurol. Sci. 2020, 42, 1073–1079. [Google Scholar] [CrossRef] [PubMed]
- Corea, F. A Tele Stroke network in internal areas of Umbria. ITJM 2018, 7, 1–8. [Google Scholar] [CrossRef]
- Bernetti, L.; Nuzzaco, G.; Muscia, F.; Gamboni, A.; Zedde, M.; Eusebi, P.; Zampolini, M.; Corea, F. Stroke Networks and Telemedicine: An Italian National Survey. Neurol. Int. 2018, 10, 41–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Official Site of the Governmental Agency for Qualitative Data Analysis for Heath Care Providers. Available online: https://pne.agenas.it (accessed on 10 August 2021).
- Sairanen, T.; Soinila, S.; Nikkanen, M.; Rantanen, K.; Mustanoja, S.; Färkkilä, M.; Pieninkeroinen, I.; Numminen, H.; Baumann, P.; Valpas, J.; et al. Finnish Telestroke Task Force. Two years of Finnish Telestroke: Thrombolysis at spokes equal to that at the hub. Neurology 2011, 76, 1145–1152. [Google Scholar] [CrossRef] [PubMed]
- Schwab, S.; Vatankhah, B.; Kukla, C.; Hauchwitz, M.; Bogdahn, U.; Fürst, A.; TEMPiS Group. Long-term outcome after thrombolysis in tele- medical stroke care. Neurology 2007, 69, 898–903. [Google Scholar] [CrossRef]
- Tumma, A.; Berzou, S.; Jaques, K.; Shah, D.; Smith, A.C.; Thomas, E.E. Considerations for the Implementation of a Telestroke Network: A Systematic Review. J. Stroke Cerebrovasc. Dis. 2022, 31, 106171. [Google Scholar] [CrossRef] [PubMed]
- Nuzzaco, G.; Muscia, F.; Verrengia, E.P.; Raimondi, E.; Chiveri, L.R. Telestroke/Telemedicine in Lombardia. In Proceedings of the 2019 ESOC Conference, Leiden, The Netherlands, 12–14 May 2019; Available online: https://www.morressier.com/article/title-telestroketelemedicine-lombardia-italy-asst-ovest-milanese-experience/5cb58cfdc668520010b56d68 (accessed on 5 December 2021).
- Corea, F.; Gamboni, A.; Manzi, P.; Carducci, D.; Micheli, S.; Guidubaldi, A.; Rossi, V.; Brustenghi, P.; Calabrò, G.; Caso, V.; et al. A Stroke Network in Internal Areas of Central Italy. In Proceedings of the 2017 ESOC Conference, Basel, Switzerland, 18 April 2017; Available online: https://www.morressier.com/article/stroke-network-internal-areas-central-italy/58e389b2d462b80292385232? (accessed on 5 December 2021).
- Falcou, A.; Risitano, A.; Ruggeri, E.; Baracco, E.; Ferri, E.; Donati, U.; Toni, D. Telestroke in Latium. In Proceedings of the 2019 ESOC Conference, Leiden, The Netherlands, 12–14 May 2019; Available online: https://doi.org/10.26226/morressier.5cb58cf4c668520010b564b3 (accessed on 5 December 2021).
- Bravata, D.M.; Kim, N.; Concato, J.; Krumholz, H.M.; Brass, L.M. Thrombolysis for Acute Stroke in Routine Clinical Practice. Arch. Intern. Med. 2002, 162, 1994–2001. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fagan, S.C.; Morgenstern, L.B.; Petitta, A.; Ward, R.E.; Tilley, B.C.; Marler, J.R.; Levine, S.R.; Broderick, J.P.; Kwiatkowski, T.G.; Frankel, M.; et al. Cost-effectiveness of tissue plasminogen activator for acute ischemic stroke. Neurology 1998, 50, 883–890. [Google Scholar] [CrossRef]
- Silbergleit, R.; Scott, P.A.; Lowell, M.J.; Silbergleit, R. Cost-effectiveness of helicopter transport of stroke patients for thrombolysis. Acad. Emerg. Med. 2003, 10, 966–972. [Google Scholar] [PubMed] [Green Version]
- Silliman, S.L.; Quinn, B.; Huggett, V.; Merino, J.G. Use of a Field-to-Stroke Center Helicopter Transport Program to Extend Thrombolytic Therapy to Rural Residents. Stroke 2003, 34, 729–733. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Busti, C.; Gamboni, A.; Calabrò, G.; Zampolini, M.; Zedde, M.; Caso, V.; Corea, F. Telestroke: Barriers to the Transition. Front. Neurol. 2021, 12, 689191. [Google Scholar] [CrossRef] [PubMed]
- Zedde, M.; Pezzella, F.R.; Paciaroni, M.; Corea, F.; Reale, N.; Toni, D.; Caso, V. Stroke care in Italy: An overview of strategies to manage acute stroke in COVID-19 time. Eur. Stroke J. 2020, 5, 222–229. [Google Scholar] [CrossRef] [PubMed]
- The National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. Tissue plasminogen activator for acute ischemic stroke. N. Engl. J. Med. 1995, 333, 1581–1587. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n | N | % | |
|---|---|---|---|
| Age (median; IQR [years]) | 67 (54–79) | ||
| Female sex | 121 | 225 | 54% |
| Risk factors | |||
| arterial hypertension | 130 | 225 | 58% |
| diabetes mellitus | 45 | 225 | 20% |
| hypercholesterinemia | 78 | 225 | 35% |
| (ex-)smoker | 31 | 225 | 14% |
| atrial fibrilation | 33 | 225 | 14% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Corea, F.; Acciarresi, M.; Bernetti, L.; Brustenghi, P.; Guidubaldi, A.; Maiotti, M.; Micheli, S.; Pierini, V.; Gamboni, A.; Calabrò, G.; et al. Extending Thrombolysis in Acute Ischemic Stroke to Primary Care: Early Experiences with a Network-Based Teleneurology Approach. Neurol. Int. 2022, 14, 164-173. https://doi.org/10.3390/neurolint14010012
Corea F, Acciarresi M, Bernetti L, Brustenghi P, Guidubaldi A, Maiotti M, Micheli S, Pierini V, Gamboni A, Calabrò G, et al. Extending Thrombolysis in Acute Ischemic Stroke to Primary Care: Early Experiences with a Network-Based Teleneurology Approach. Neurology International. 2022; 14(1):164-173. https://doi.org/10.3390/neurolint14010012
Chicago/Turabian StyleCorea, Francesco, Monica Acciarresi, Laura Bernetti, Pierluigi Brustenghi, Arianna Guidubaldi, Mariangela Maiotti, Sara Micheli, Vilma Pierini, Alessio Gamboni, Giuseppe Calabrò, and et al. 2022. "Extending Thrombolysis in Acute Ischemic Stroke to Primary Care: Early Experiences with a Network-Based Teleneurology Approach" Neurology International 14, no. 1: 164-173. https://doi.org/10.3390/neurolint14010012
APA StyleCorea, F., Acciarresi, M., Bernetti, L., Brustenghi, P., Guidubaldi, A., Maiotti, M., Micheli, S., Pierini, V., Gamboni, A., Calabrò, G., Busti, C., Magistrato, C., Proietti-Silvestri, G., Bracaccia, M., Caso, V., & Zampolini, M. (2022). Extending Thrombolysis in Acute Ischemic Stroke to Primary Care: Early Experiences with a Network-Based Teleneurology Approach. Neurology International, 14(1), 164-173. https://doi.org/10.3390/neurolint14010012