Co-Designing a New Yoga-Based Mindfulness Intervention for Survivors of Stroke: A Formative Evaluation

 ,
,  , , , , , , , , and
, , , , , , , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Part A: Literature Review and Establishment of Advisory Committee
2.2.1. Literature Review
2.2.2. Advisory Committee
2.3. Part B Yoga Program Intervention Development
2.4. Formative Evaluation
2.4.1. Data Collection and Documentation
2.4.2. Data Synthesis and Interpretation
3. Results
3.1. Phase 1: Establishment of Advisory Committee to Co-Design the Program and Establish the Template for the Manual
3.1.1. Theme 1: Length and Content of Program
3.1.2. Theme 2: Assistant Teachers
3.1.3. Theme 3: Template Design and Sub-Themes
Sub-Theme 1: Background Information on Stroke for Teachers
Sub-Theme 2: Mindfulness Development
Sub-Theme 3: Clear Illustration of Poses
Sub-Theme 4: Active Therapy Feature
3.2. Phase 2: Development of the Yoga Teacher Training Manual to Detail the Intervention Components and Features in a Standardized Format by the Working Group
3.2.1. Theme 1: Yoga Intervention Working Group
3.2.2. Theme 2: Program Format and Content
3.2.3. Theme 3: Photo Shoot
3.3. Phase 3: Internal Review of the Program by Members of the Advisory Committee and Other Consumers and Allied Health Professionals
3.3.1. Theme 1: Refining Manual Format and Content
Advisor 1: “Empower participants to participate at a level that they are comfortable and may include sitting on a chair in some or all exercises. Safety within a class and a home must be carefully thought about (e.g., type of chairs, used, floor surfaces, tripping and other hazards)”.
Advisor 2: “Are participant able to do this pose with assistance from a caregiver. If so, this needs to be stated and the role of caregiver within the intervention defined”.
Advisor 3: “Avoiding injuring, safety is the priority. Imagine both limbs doing it, and encourage participant to use imagery technique”.
3.3.2. Theme 2: Transitioning to Home Practice
3.3.3. Theme 3: Clear Instructions on Transitions
3.3.4. Theme 4: Story of the Three Models
3.4. Phase 4: External Review of the Training Manual by Independent Yoga Teachers, and Finalization of Content
3.4.1. Theme 1: Use of Consistent Terminologies
3.4.2. Theme 2: Alterative Seating Options
3.4.3. Theme 3: Further Refinement to Other Manual Content
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stroke Foundation National Stroke Audit—Acute Services Report 2019; Melbourne, Australia, 2019.
- Lawrence, M.; Celestino Junior, F.T.; Matozinho, H.H.S.; Govan, L.; Booth, J.; Beecher, J. Yoga for stroke rehabilitation. Cochrane Database Syst. Rev. 2017, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmid, A.A.; Puymbroeck, M.V.; Altenburger, P.A.; Schalk, N.L.; Diercks, T.A.; Miller, K.K.; Williams, L.S. Poststroke Balance Improves With Yoga: A Pilot Study. Stroke 2012, 43, 2402–2407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Teijlingen, E.; Hundley, V. The importance of pilot studies. Nurs. Stand. 2002, 16, 33–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Craig, P.; Dieppe, P.; Macintyre, S.; Michie, S.; Nazareth, I.; Petticrew, M. Developing and evaluating complex interventions: The new Medical Research Council guidance. BMJ 2008, 337, a1655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Immink, M.A.; Hillier, S.; Petkov, J. Randomised Controlled Trial of Yoga for Chronic Poststroke Hemiparesis: Motor Function, Mental Health, and Quality of Life Outcomes. Top. Stroke Rehabil. 2014, 21, 256–271. [Google Scholar] [CrossRef] [PubMed]
- Garrett, R.; Immink, M.A.; Hillier, S. Becoming connected: The lived experience of yoga participation after stroke. Disabil. Rehabil. 2011, 33, 2404–2415. [Google Scholar] [CrossRef] [PubMed]
- Campbell, M.; Fitzpatrick, R.; Haines, A.; Kinmonth, A.; Sandercock, P.; Spiegelhalter, D.; Tyrer, P. Framework for design and evaluation of complex interventions to improve health. BMJ 2000, 321, 694–696. [Google Scholar] [CrossRef] [Green Version]
- Thayabaranathan, T.; Immink, M.A.; Stevens, P.; Hillier, S.; Thrift, A.G.; Brodtmann, A.; Carey, L.; Kilkenny, M.F.; Cadilhac, D.A. Understanding the potential for yoga and tai chi interventions to moderate risk factors for stroke—A scoping review. Future Neurol. 2018, 13, 239–252. [Google Scholar] [CrossRef]
- Thayabaranathan, T.; Andrew, N.E.; Immink, M.A.; Hillier, S.; Stevens, P.; Stolwyk, R.; Kilkenny, M.; Cadilhac, D.A. Determining the potential benefits of yoga in chronic stroke care: A systematic review and meta-analysis. Top. Stroke Rehabil. 2017, 24, 279–287. [Google Scholar] [CrossRef] [PubMed]
- Chan, W.; Immink, M.A.; Hillier, S. Yoga and Exercise for Symptoms of Depression and Anxiety in People With Poststroke Disability: A Randomised, Controlled Pilot Trial. Altern. Ther. 2012, 18, 34–43. [Google Scholar]
- Johnson-Frey, S.H. Stimulation through simulation? Motor imagery and functional reorganization in hemiplegic stroke patients. Brain Cogn. 2004, 55, 328–331. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, M.; Booth, J.; Mercer, S.; Crawford, E. A systematic review of the benefits of mindfulness-based interventions following transient ischemic attack and stroke. Int. J. Stroke 2013, 8, 465–474. [Google Scholar] [CrossRef] [PubMed]
- O’Cathain, A.; Croot, L.; Duncan, E.; Rousseau, N.; Sworn, K.; Turner, K.; Hoddinott, P. Guidance on how to develop complex interventions to improve health and healthcare. BMJ Open 2019, 9, e029954. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sturt, J.; Whitlock, S.; Hearnshaw, H. Complex intervention development for diabetes self-management. J. Adv. Nurs. 2006, 54, 293–303. [Google Scholar] [CrossRef] [PubMed]
- Stetler, C.B.; Legro, M.W.; Wallace, C.M.; Bowman, C.; Guihan, M.; Hagedorn, H.; Kimmel, B.; Sharp, N.D.; Smith, J.L. The role of formative evaluation in implementation research and the QUERI experience. J. Gen. Intern. Med. 2006, 21 (Suppl. S2), S1–S8. [Google Scholar] [CrossRef] [PubMed]
- Hedberg, J.G. Education design research—Edited by J van den Akker. Br. J. Educ. Technol. 2008, 39, 559–560. [Google Scholar] [CrossRef]
- Andersson, N. Community-led trials: Intervention co-design in a cluster randomised controlled trial. BMC Public Health 2017, 17, 397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walker, M.; Hoffmann, T.; Brady, M.; Dean, C.; Eng, J.J.; Farrin, A.J.; Felix, C.; Forster, A.; Langhorne, P.; Lynch, E.A.; et al. Improving the development, monitoring and reporting of stroke rehabilitation research: Consensus-based core recommendations from the Stroke Recovery and Rehabilitation Roundtable. Int. J. Stroke 2017, 12, 472–479. [Google Scholar] [CrossRef] [PubMed]
- Filipe, A.; Renedo, A.; Marston, C. The co-production of what? Knowledge, values, and social relations in health care. PLoS Biol. 2017, 15, e2001403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cadilhac, D.A.; Fisher, R.; Bernhardt, J. How to do health services research in stroke: A focus on performance measurement and quality improvement. Int. J. Stroke 2018, 13, 166–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
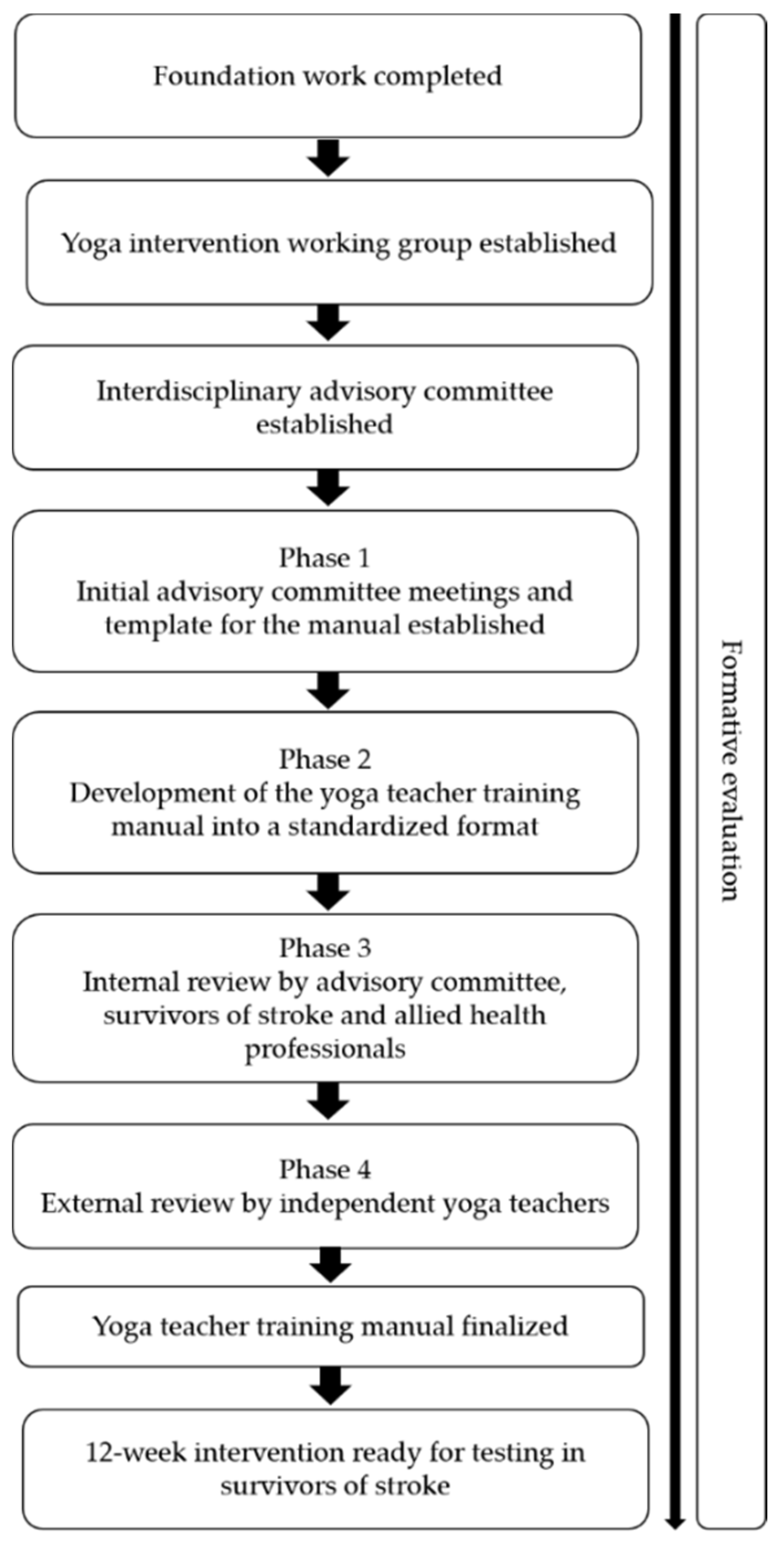
| Phases | Description |
|---|---|
| Phase 1 | Initial advisory committee meetings to achieve consensus on the broad principles of the intervention scope and establish the template for the manual |
| Phase 2 | Development of the yoga teacher training manual to detail the intervention components and features in a standardized format |
| Phase 3 | Internal review of the program by members of the advisory committee and other stakeholders (i.e., survivors of stroke) and allied health professionals |
| Phase 4 | External review of the training manual by independent yoga teachers, and finalization of content |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thayabaranathan, T.; Immink, M.A.; Hillier, S.; Stolwyk, R.; Andrew, N.E.; Stevens, P.; Kilkenny, M.F.; Gee, E.; Carey, L.; Brodtmann, A.; et al. Co-Designing a New Yoga-Based Mindfulness Intervention for Survivors of Stroke: A Formative Evaluation. Neurol. Int. 2022, 14, 1-10. https://doi.org/10.3390/neurolint14010001
Thayabaranathan T, Immink MA, Hillier S, Stolwyk R, Andrew NE, Stevens P, Kilkenny MF, Gee E, Carey L, Brodtmann A, et al. Co-Designing a New Yoga-Based Mindfulness Intervention for Survivors of Stroke: A Formative Evaluation. Neurology International. 2022; 14(1):1-10. https://doi.org/10.3390/neurolint14010001
Chicago/Turabian StyleThayabaranathan, Tharshanah, Maarten A. Immink, Susan Hillier, Rene Stolwyk, Nadine E. Andrew, Philip Stevens, Monique F. Kilkenny, Emma Gee, Leeanne Carey, Amy Brodtmann, and et al. 2022. "Co-Designing a New Yoga-Based Mindfulness Intervention for Survivors of Stroke: A Formative Evaluation" Neurology International 14, no. 1: 1-10. https://doi.org/10.3390/neurolint14010001
APA StyleThayabaranathan, T., Immink, M. A., Hillier, S., Stolwyk, R., Andrew, N. E., Stevens, P., Kilkenny, M. F., Gee, E., Carey, L., Brodtmann, A., Bernhardt, J., Thrift, A. G., & Cadilhac, D. A. (2022). Co-Designing a New Yoga-Based Mindfulness Intervention for Survivors of Stroke: A Formative Evaluation. Neurology International, 14(1), 1-10. https://doi.org/10.3390/neurolint14010001