Velocity Determinants in Spastic Patients after Stroke—A Gait Analysis Study

Abstract
1. Introduction
2. Methods
3. Results
4. Discussion
4.1. Spatiotemporal Parameters
4.2. Kinematic Parameters
4.3. Dynamometric Parameters
4.4. Integration of Concepts
- Cadence and non-paretic stride length. The latter probably relates to the compensations accomplished by the healthy side of the body, possibly reflecting the muscle strength and motor control of the areas non affected by the stroke, or even the cardiorespiratory fitness of the subject (the capacity to compensate for the motor deficits is usually accompanied by an increased energy expenditure). The clinical implication of this finding is that the strength and motor control of the non-paretic limb may be a target for rehabilitation programs in order to better compensate for the deficits of the paretic limb and, consequently, allow for higher gait velocity.
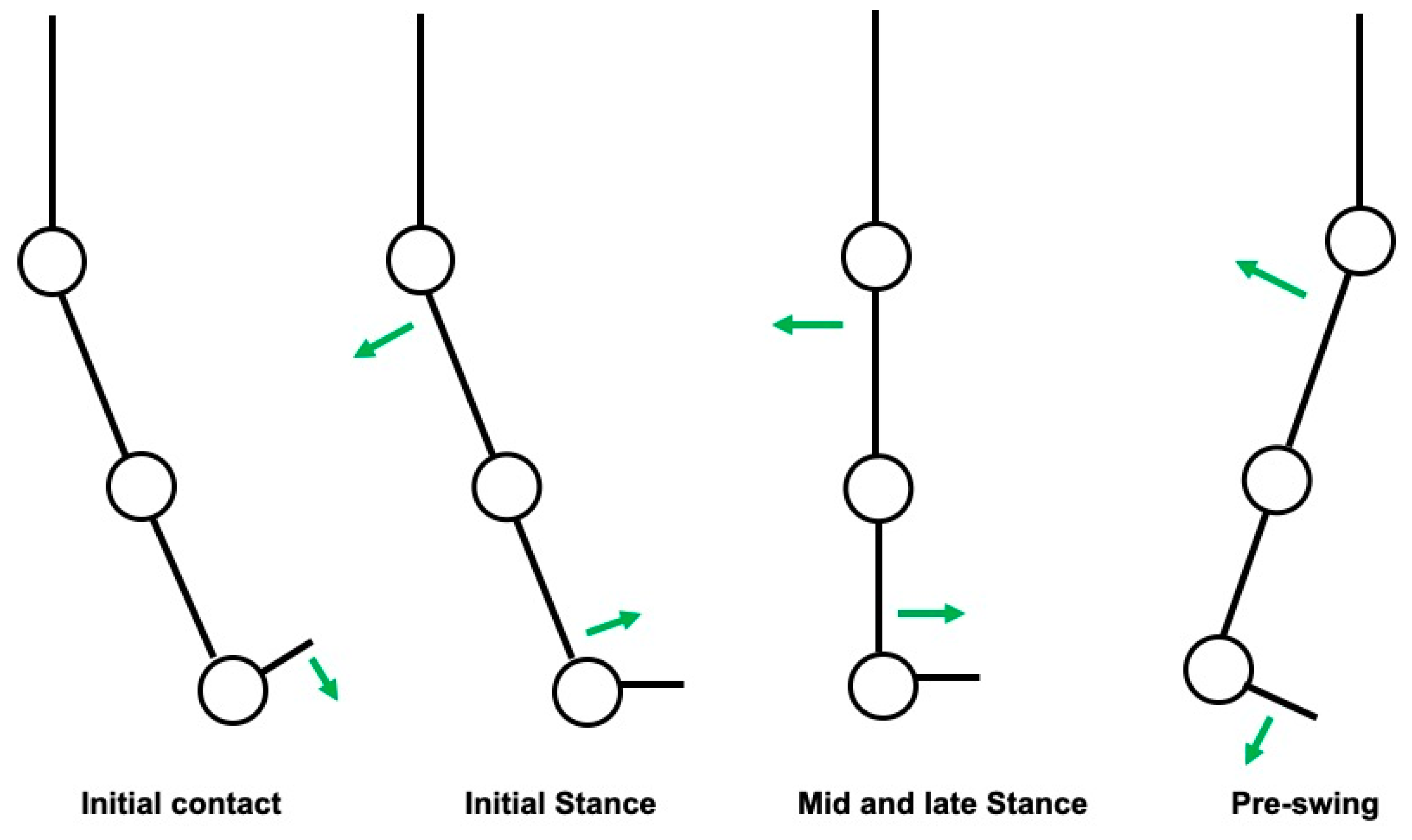
- Maximum hip extension during the stance phase of the paretic limb: the hip is the main driving force responsible for the anterior projection of the body during early stance phase (the knee is in slight flexion in the early stance phase and the ankle in slight plantarflexion, followed by passive dorsiflexion, that compensates for hip extension). Considering this, the correlation found is actually plausible. However, slower gait patterns are usually associated with a shorter step length and, consequently, with a limited hip extension (there is not enough time for the hip to extend fully). Hence, a limited hip extension may be at the same time a cause and a consequence of slower gait. The clinical implication of this finding is that a spastic Iliopsoas muscle (sometimes overlooked in the clinical examination) should be carefully tracked.
- Knee flexion of the paretic limb during swing phase: the knee is the lower limb joint that shows a larger sagittal range of motion during swing phase; consequently, an impairment at this level would have a greater impact on aerial limb progression. The clinical implication of this finding is that spasticity of the Quadriceps muscle (which can contribute to a stiff-knee pattern in extreme situations) should be carefully tracked.
- Ankle plantar flexion of the paretic limb during pre-swing (which enables the push-off): The ankle is the main driving force responsible for the anterior projection of the body during the late stance phase, after the hip stops extending. The clinical implication of this finding is that the maintenance of Gastrocnemius and Soleus normal activation (timely) and muscle strength is relevant to gait velocity.
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Schmid, A.; Duncan, P.W.; Studenski, S.; Lai, S.M.; Richards, L.; Perera, S.; Wu, S.S. Improvements in Speed-Based Gait Classifications Are Meaningful. Stroke 2007, 38, 2096–2100. [Google Scholar] [CrossRef] [PubMed]
- Bohannon, R.W.; Andrews, A.W. Normal walking speed: A descriptive meta-analysis. Physiotherapy 2011, 97, 182–189. [Google Scholar] [CrossRef] [PubMed]
- Middleton, A.; Fritz, S.L.; Lusardi, M. Walking speed: The functional vital sign. J. Aging Phys. Act. 2015, 23, 314–322. [Google Scholar] [CrossRef] [PubMed]
- Benjamin, E.J.; Blaha, M.J.; Chiuve, S.E.; Cushman, M.; Das, S.R.; Deo, R.; de Ferranti, S.D.; Floyd, J.; Fornage, M.; Gillespie, C.; et al. Heart Disease and Stroke Statistics’2017 Update: A Report from the American Heart Association. Circulation 2017, 135, 146–603. [Google Scholar] [CrossRef] [PubMed]
- Duncan, P.W.; Zorowitz, R.; Bates, B.; Choi, J.Y.; Glasberg, J.J.; Graham, G.D.; Katz, R.C.; Lamberty, K.; Reker, D. Management of Adult Stroke Rehabilitation Care. Stroke 2005, 36, e100–e143. [Google Scholar] [CrossRef]
- Kischka, U.; Wade, D.T. Rehabilitation after stroke. Handb. Cerebrovasc. Dis. Second Ed. Revis. Expand. 2004, 01, 231–241. [Google Scholar]
- Wonsetler, E.C.; Bowden, M.G. A systematic review of mechanisms of gait speed change post-stroke. Part 1: Spatiotemporal parameters and asymmetry ratios. Top. Stroke Rehabil. 2017, 24, 435–446. [Google Scholar] [CrossRef]
- Taylor-Piliae, R.E.; Latt, L.D.; Hepworth, J.T.; Coull, B.M. Predictors of gait velocity among community-dwelling stroke survivors. Gait Posture 2011, 35, 395–399. [Google Scholar] [CrossRef] [PubMed]
- Olney, S.J.; Griffin, M.P.; McBride, I.D. Temporal, Kinematic, and Kinetic Variables Related to Gait Speed in Subjects With Hemiplegia: A Regression Approach. Phys. Ther. 1994, 74, 872–885. [Google Scholar] [CrossRef]


{kind=link}
| Number of Participants | 34 |
| Age | 49.7 (±13.4) years |
| Sex | 32% (19) women/68% (15) men |
| Paretic Limb | 62% (23) right/38% (11) left |
| Speed | 0.5 (±0.2) m/s |
| Spatiotemporal Parameters |
|---|
| Cadence |
| Double support time |
| Percentage of the gait cycle at which Foot off occurs |
| Limp index |
| Percentage of the gait cycle at which the opposite foot contacts the ground |
| Percentage of the gait cycle at which the opposite foot leaves the ground |
| Single support time |
| Step length |
| Step width |
| Step time |
| Stride length |
| Stride time |
| Walking speed |
| Initial contact type |
| Static kinematic parameters |
| Pelvic tilt |
| Hip angle (P and NP) |
| Knee angle (P and NP) |
| Ankle angle (P and NP) |
| Dynamic kinematic parameters related to paretic limb |
| Pelvic transverse plane excursion (rotation) |
| Pelvic maximum obliquity during swing phase |
| Hip—maximum flexion during swing phase |
| Hip—angle in initial foot contact |
| Hip—maximum extension during stance phase |
| Hip—maximum extension during unipodal stance phase |
| Hip—angle at foot-off |
| Hip—excursion during unipodal stance phase |
| Knee—maximum flexion during swing phase |
| Knee—initial contact angle |
| Knee—maximum extension during stance phase |
| Knee—angle at foot-off |
| Ankle—maximum dorsiflexion during swing phase |
| Ankle—initial contact angle |
| Ankle—maximum dorsiflexion during unipodal stance phase |
| Ankle—maximum plantar flexion during unipodal stance phase |
| Ankle—angle at foot-off |
| Ankle—excursion during unipodal stance phase |
| Force (vertical)—percentage of gait cycle of the first peak |
| Maximum potency of the ankle during stance phase |
| Outcome | Pearson | Sig. |
|---|---|---|
| Age | 0.155 | 0.382 |
| Cadence | 0.685 ** | 0.000 |
| Double support time NP | −0.326 | 0.060 |
| Foot-off NP | −0.445 ** | 0.008 |
| Limp Index NP | 0.148 | 0.405 |
| Opposite Foot contact NP | −0.163 | 0.356 |
| Opposite Foot off NP | −0.156 | 0.377 |
| Single Support NP | −0.011 | 0.950 |
| Step Length NP | 0.166 | 0.349 |
| Step Time NP | −0.543 ** | 0.001 |
| Step width NP | −0.177 | 0.315 |
| Stride Length NP | 0.753 ** | 0.000 |
| Stride Time NP | −0.651 ** | 0.000 |
| Double support time | −0.414 * | 0.015 |
| Foot off P | 0.056 | 0.754 |
| Limp Index P | −0.177 | 0.317 |
| Opposite Foot Contact P | −0.016 | 0.926 |
| Opposite Foot Off P | −0.584 | 0.000 |
| Single Support P | 0.174 | 0.326 |
| Step Length P | 0.127 | 0.474 |
| Step Time P | −0.550 ** | 0.001 |
| Step width P | −0.021 | 0.905 |
| Stride Length P | −0.125 | 0.481 |
| Stride Time P | −0.665 ** | 0.000 |
| Static kinematic—Pelvic Tilt | −0.191 | 0.278 |
| Static kinematic—Hip angle NP | −0.122 | 0.491 |
| Static kinematic—Hip angle P | −0.116 | 0.513 |
| Static kinematic—Knee angle NP | −0.058 | 0.746 |
| Static kinematic—Knee angle P | 0.119 | 0.504 |
| Static kinematic—Ankle NP | −0.028 | 0.874 |
| Static kinematic—Ankle P | 0.032 | 0.859 |
| Pelvic amplitude of rotation | −0.200 | 0.256 |
| Pelvic maximum obliquity during swing phase | 0.099 | 0.585 |
| Hip—maximum flexion during swing phase | 0.100 | 0.572 |
| Hip—angle at initial foot contact | 0.221 | 0.210 |
| Hip—maximum extension during stance phase | −0.447 ** | 0.008 |
| Hip—maximum extension during unipodal stance phase | −0.431 ** | 0.011 |
| Hip—Foot off angle | −0.626 ** | 0.000 |
| Hip—excursion during unipodal stance phase | 0.533 ** | 0.001 |
| Knee—maximum flexion during swing phase | 0.403 * | 0.018 |
| Knee—angle at initial contact | 0.124 | 0.484 |
| Knee—maximum extension during stance phase | 0.154 | 0.384 |
| Knee—angle at Foot-off | 0.158 | 0.372 |
| Ankle—maximum dorsiflexion during swing phase | 0.112 | 0.528 |
| Angle—angle at initial contact | 0.009 | 0.958 |
| Ankle—maximum plantarflexion during stance phase | 0.359 * | 0.037 |
| Ankle—maximum dorsiflexion during unipodal stance phase | −0.152 | 0.392 |
| Ankle—maximum plantarflexion during unipodal stance phase | 0.371 * | 0.031 |
| Ankle—angle at foot-off | −0.299 | 0.085 |
| Ankle—excursion during unipodal stance phase | 0.641 ** | 0.000 |
| Force (vertical)—percentage of gait cycle of the first peak | −0.620 ** | 0.000 |
| Maximum potency of the ankle during stance phase | 0.643 ** | 0.000 |
| Initial Contact Type | t | df | Sig. |
|---|---|---|---|
| Velocity | −1.449 | 32 | 0.157 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Silva, M.R.e.; Jacinto, J. Velocity Determinants in Spastic Patients after Stroke—A Gait Analysis Study. Neurol. Int. 2020, 12, 48-54. https://doi.org/10.3390/neurolint12030011
Silva MRe, Jacinto J. Velocity Determinants in Spastic Patients after Stroke—A Gait Analysis Study. Neurology International. 2020; 12(3):48-54. https://doi.org/10.3390/neurolint12030011
Chicago/Turabian StyleSilva, Miguel Reis e, and Jorge Jacinto. 2020. "Velocity Determinants in Spastic Patients after Stroke—A Gait Analysis Study" Neurology International 12, no. 3: 48-54. https://doi.org/10.3390/neurolint12030011
APA StyleSilva, M. R. e., & Jacinto, J. (2020). Velocity Determinants in Spastic Patients after Stroke—A Gait Analysis Study. Neurology International, 12(3), 48-54. https://doi.org/10.3390/neurolint12030011