Abstract
Sarcoidosis is a multifaceted and multisystemic inflammatory disorder, the etiology of which remains unknown. However, it has been suggested that an intricate interplay between genetic, environmental, and inflammatory factors may contribute to the development and progression of sarcoidosis. Although 30–50% of patients demonstrate extra-pulmonary manifestations, cardiac involvement is rare, affecting only 2–5% of cases. Diagnosis is often challenging, relying on the careful application of clinical judgment, histopathological evidence, and imaging biomarkers. In this literature review, we aim to provide a comprehensive overview of the current understanding of the genetic basis of sarcoidosis, the contribution to the pathogenesis of the disorder, and discuss the potential link between certain genetic variants and the development of cardiac sarcoidosis.
1. Introduction
Sarcoidosis is a complex and obscure disorder with many implicated triggers, which include environmental, inflammatory, and genetic factors. It is characterized by the formation and accumulation of non-necrotizing epithelioid-cell granulomas typically in the lungs but may be multisystemic, impacting the cardiac, hepatic, ocular, skeletal, lymphatic, and nervous systems [1,2]. The signs and symptoms of sarcoidosis are non-specific, often taking months to years for diagnosis. Although it has been described since the 19th century, with extensive research being conducted to understand the mechanisms of this disorder, its exact etiology remains unknown. It is a clinically heterogeneous disorder, ranging from asymptomatic forms to aggressive disease, that impacts almost 20% of cases [1,3]. Although 30–50% of patients may have spontaneous remission or have a benign clinical course, it is chronic, life-changing, and at times fatal [4,5]. The prevalence is highly variable, ranging from 10 to 60 cases per 100,000 and an incidence of 1 to 36 cases per 100,000 owing to geographic, socioeconomic, and environmental factors [6,7,8]. Cardiac sarcoidosis (CS) is even more atypical and problematic to diagnose, accounting for only 2–5% of cases [9,10]. The clinical manifestations of CS may present as sudden cardiac death (SCD), conduction abnormalities, arrhythmias, or heart failure [10]. More importantly, it may be isolated (iCS) or nonisolated (niCS). Diagnosis typically involves high clinical suspicion, in combination with advanced cardiovascular imaging, with or without an endomyocardial biopsy [11,12]. Genetic testing has been pivotal in the management and risk stratification of inherited cardiac disorders, but its role is unclear in inflammatory cardiomyopathies [13]. Therefore, it is essential to understand whether genetics has a role and, thus, management in cardiac sarcoidosis. Given the nature and phenotypic variability of the disorder, it is crucial to have specialized sarcoid or inflammatory disease clinics equipped with advanced imaging, electrophysiological, and heart failure services to aid in diagnosis and management. The availability of expert guidance at these centers is of paramount importance in effectively managing this disorder.
2. Materials and Methods
We performed a review of the literature focusing on genetics and sarcoidosis (Supplementary Figure S1). Our search included meta-analyses, case series, reviews, prospective and retrospective studies. Conference abstracts or articles where there was no association between sarcoidosis and genetics were excluded. Key search terms included “sarcoidosis”, “cardiac sarcoidosis”, “infiltrative cardiomyopathy”, and “inflammatory cardiomyopathy”, in combination with “genetics”.
3. Results
From the literature review, a total of 137 studies were screened and evaluated. After careful consideration, 66 studies were identified as relevant and incorporated into the review.
3.1. Diagnosis of Sarcoidosis
Sarcoidosis is regarded as a consequence of an exaggerated immune response in a genetically predisposed individual after exposure to an unidentified antigen. The condition is manifested through a range of signs that may include respiratory symptoms, lymphadenopathy, fatigue, and erythema nodosum [5]. Notably, abnormal chest radiographs are observed in over 90% of patients with pulmonary sarcoidosis [14,15,16]. Furthermore, 50–85% of patients exhibit bilateral hilar lymphadenopathy, while parenchymal opacities are observed in 20–65% of cases [14,16]. In the case of cardiac sarcoidosis, the common presentations include atrioventricular (AV), bundle branch block, multi-focal premature ventricular contractions (PVCs), ventricular arrhythmias (VAs), pericarditis, heart failure, and or sudden cardiac death [16]. More significantly, both AV block and a history of VAs increase the risk of SCD.
High clinical suspicion is necessary since diagnostic testing is often invasive. Endobronchial ultrasound coupled with transbronchial fine aspiration of mediastinal and hilar lymphadenopathy is highly effective in diagnosing pulmonary sarcoid. If inconclusive, endobronchial and transbronchial lung biopsy may be necessary. Bronchoalveolar lavage (BAL) can serve as a complementary tool, revealing moderate lymphocytosis with a T lymphocyte CD4:CD8 ratio higher than 3.5 [8]. On the other hand, angiotensin-converting enzyme (ACE) is not a reliable marker for diagnosis, and interleukin-2, neopterin, or chitotriosidase may be better options to corroborate the diagnosis of sarcoid [17,18,19]. The assessment of extra-pulmonary manifestations is facilitated by the evaluation of inflammatory activity, for which 18F-fluorodeoxyglucose (18F-FDG) positron emission tomography (PET) can be a valuable tool [20]. Therefore, diagnosis is based on clinical and radiological presentation, corroborated by evidence of noncaseating granulomas without the suggestion of an alternative disease. It should be worth noting that while non-necrotizing granulomas are an essential feature of sarcoidosis, it may also be present in other infectious and inflammatory diseases.
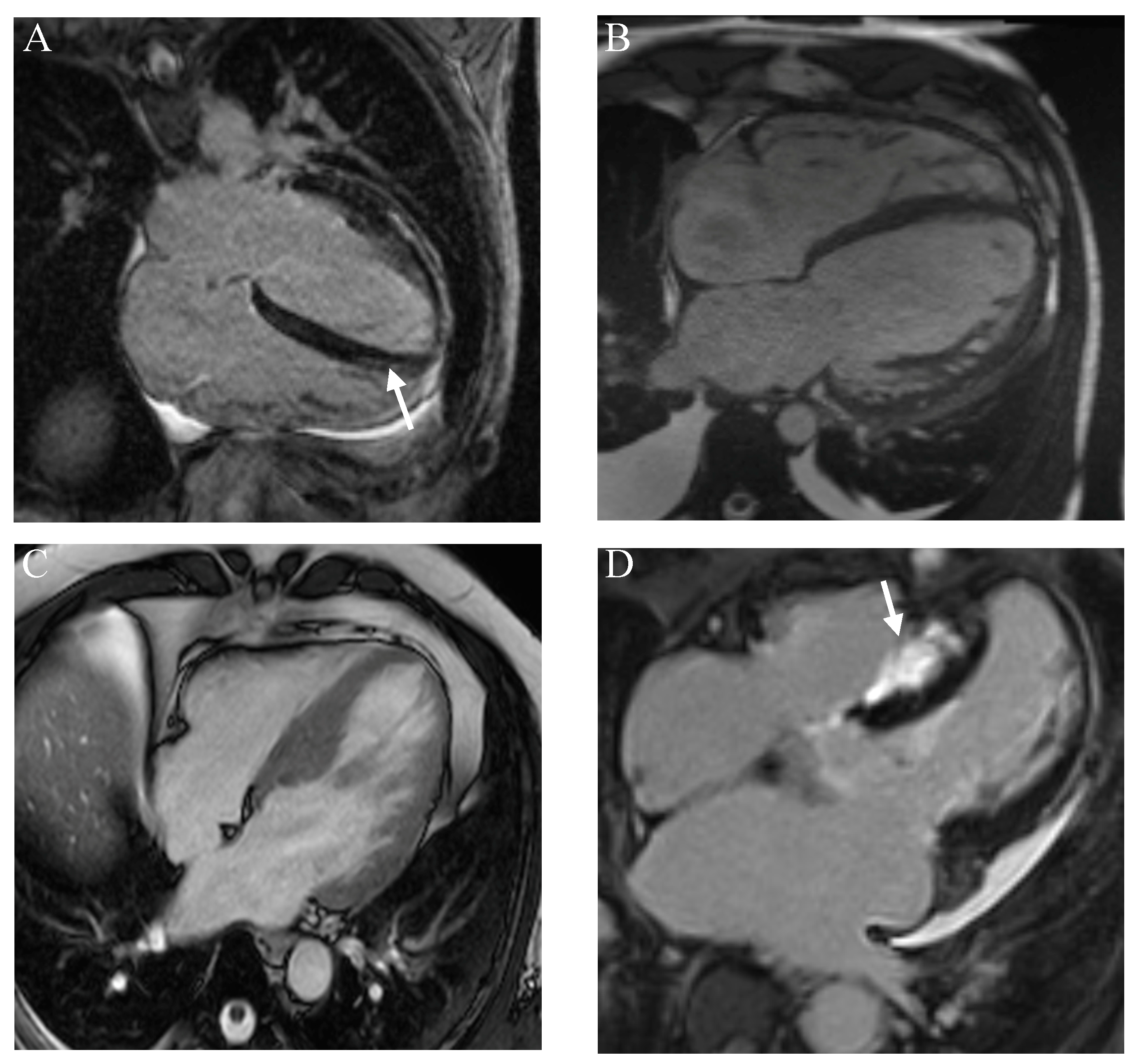
The diagnosis of cardiac sarcoidosis is particularly challenging as endomyocardial biopsy (EMB) is hard to obtain, with a reported yield of only approximately 25% [13]. More importantly, granulomas in CS are uncommon. With technological advancement, however, voltage-guided biopsy may increase the success rate to 50% [13,21]. Nonetheless, diagnosis predominantly relies on cardiac imaging, which includes trans-thoracic echocardiography (TTE), gallium scintigraphy, cardiac magnetic resonance imaging (MRI), PET and, more recently, combined MRI/PET, which may assist in guiding risk stratification and management of the disorder [22,23,24,25,26]. CS may be characterized by basal thinning of the ventricular septum, abnormal ventricular wall anatomy, and/or the presence of late gadolinium enhancement (LGE) [13]. Typically, the scar pattern is non-ischemic, which preferentially affects the sub- and mid-myocardium (Figure 1). T2 mapping is helpful in identifying areas of edema and inflammation [27]. In addition, 18F–FDG may identify granulomas, while the combination of PET perfusion with 82Rubidium or 13N- Ammonia or single-photon emission computed tomography (SPECT) with Technetium-99m Sestamibi or Thallium may identify areas of hypoperfusion secondary to micro-vascular compression from inflammatory cells [13]. TTE is useful in identifying regional wall motion abnormalities (RWMAs), valvulopathies, pericardial effusion, and aneurysms while speckle-tracking echocardiography can demonstrate strain abnormalities [28].
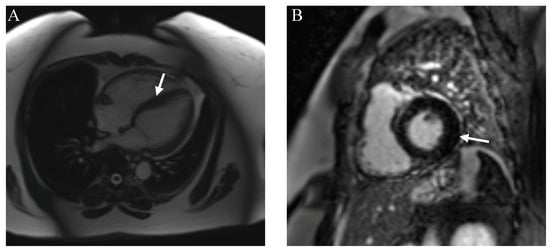
Figure 1.
Cardiac magnetic resonance imaging (MRI) demonstrating mild left ventricular hypertrophy (A) secondary to edema with sub-endocardial late gadolinium enhancement (B). The arrows depict myocardial hypertrophy and edema.
Additionally, right heart catheterization may be helpful in accurately assessing pulmonary pressures and guiding treatment options for pulmonary hypertension. Lastly, hybrid PET/MRI may be superior to MRI and PET in isolation due to its greater capability for resolution and sensitivity in detecting silent disease prior to overt functional and structural abnormalities [13,29]. The Heart Rhythm Society (HRS), the Japanese Ministry of Health and Welfare (JMHW), and the World Association of Sarcoidosis and Other Granulomatous Diseases (WASOG) have published criteria to aid in the diagnosis of CS [30,31,32].
Nonetheless, the current tools and techniques for the diagnosis of CS have limitations. Foremost, a definitive gold standard remains elusive. EMB is invasive and suffers from low yield, given the patchy nature of the disorder. More importantly, cardiovascular imaging, while commonly utilized, does not offer 100% sensitivity, and findings are non-specific without the appropriate context or clinical suspicion. For instance, both cardiac MRI and FDG–PET evaluate fibrosis and inflammation, respectively, which is not specific to CS. Furthermore, limitations of FDG–PET include uptake of non-inflammatory myocardial uptake, while atrial fibrillation or conduction abnormalities may affect regional glucose utilization. In addition, there are risks associated with radiation exposure [33].
Accurate diagnosis of CS is challenging due to the overlap of clinical and imaging findings with infiltrative, inflammatory, and genetic cardiomyopathies (Table 1, Figure 2). Distinguishing between giant cell myocarditis (GCM) and CS can present the most significant challenge, as both disorders often demonstrate similar cardiac MRI and histopathological findings [34,35]. In view of this, a high degree of clinical suspicion, while being attentive to the clinical course, is essential in the differentiation between GCM and CS. Furthermore, recent advances in hybrid cardiovascular imaging have been crucial to the diagnosis and risk stratification of CS [36]. For instance, PET has a higher diagnostic accuracy for detecting cardiac lesions secondary to CS, which may be overlooked by cardiac MRI [37].

Table 1.
Differential diagnosis of cardiac sarcoidosis.
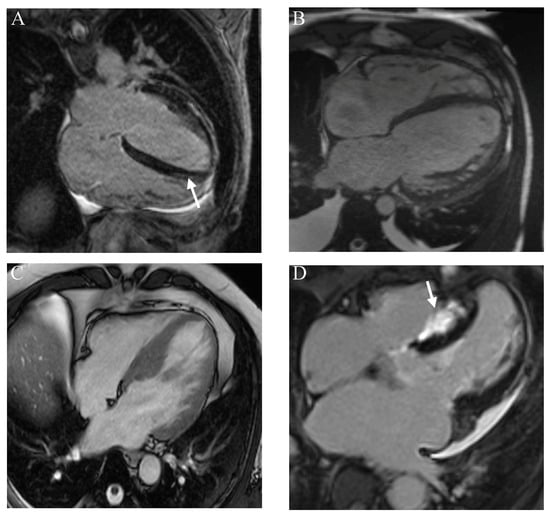
Figure 2.
Cardiac magnetic resonance (CMR) imaging showing mid/apical late gadolinium enhancement (LGE) in (A) myocarditis. CMR demonstrating dilated cardiomyopathy (B) and hypertrophic cardiomyopathy (C). CMR demonstrates extreme left ventricular hypertrophy with (D) extensive LGE.
3.2. Epidemiology of Sarcoidosis
Sarcoidosis occurs worldwide, affecting individuals of all ages, genders, and races. Owing to the diagnostic criteria’s ambiguity and variability in presentation, estimating its global burden remains a challenge. Nonetheless, the highest rates are reported in Northern Europeans and African Americans, with 70% of patients aged between 25 and 45 years. Conversely, the prevalence is lower in South America, India, and Japan and is rare in individuals younger than 15 or older than 70, with a female-to-male ratio of 1:20:1:75, suggesting the variability of risk among ethnic groups, gender and age [8,13,38]. The pattern of organ involvement also differs among ethnic and racial groups, with African Americans presenting more severely. These differences may be attributed to several factors, which include genetic susceptibility among populations, environmental factors, such as hormonal variation, occupational exposure, gender-based activities, and, more importantly, diagnostic practices [39]. Regardless, how geographic variation impacts the incidence of sarcoidosis should be further explored.
Up to half of sarcoidosis cases achieve spontaneous remission in 5 years, and as such, may be classified as acute (≤2 years) or chronic (≥3–5 years). The challenging aspect of CS is that it is often subclinical and under-recognized [40]. It is estimated that 20–25% of individuals with pulmonary/systemic sarcoidosis have silent cardiac disease [40]. Moreover, there has been an increase in CS prevalence and incidence of patients who underwent cardiac transplantation, further emphasizing the importance of recognizing the implications of this disorder [41].
3.3. Pathogenesis
The pathophysiology of sarcoidosis is complex and poorly understood. Both organic and inorganic triggers, in conjunction with a dysregulated immune response, are believed to play a central role in the pathogenesis of sarcoidosis [13]. Exposure to transmissible agents, such as musty odors, pine pollen, and insecticides, as well as occupational exposure to metals, talc, or silica, are risk factors in the development of sarcoidosis [8]. Furthermore, the aggregation and persistence of microbial-induced host responses to mycobacteria or propionibacteria may form the nidus for granuloma formation. Inflammatory mechanisms include upregulated expression and function of major histocompatibility complex class II (MHC-2) molecules and costimulatory molecules, such as Cluster of Differentiation 86 (CD86), CD80, Intercellular Adhesion Molecule (ICAM), CD14, and CD40 [41]. Furthermore, there is an increased tumor necrosis factor α (TNFα) response when stimulated by Toll-like receptor 4 (TLR4) and an influx of CXCR3-positive T-helper 1 cells [42]. T lymphocyte activation induces interferon- γ, TNFα, and interleukin 2. The result is that an epithelioid-cell rich granuloma is purported to trap the remnants of causative agents that cannot be further degraded.
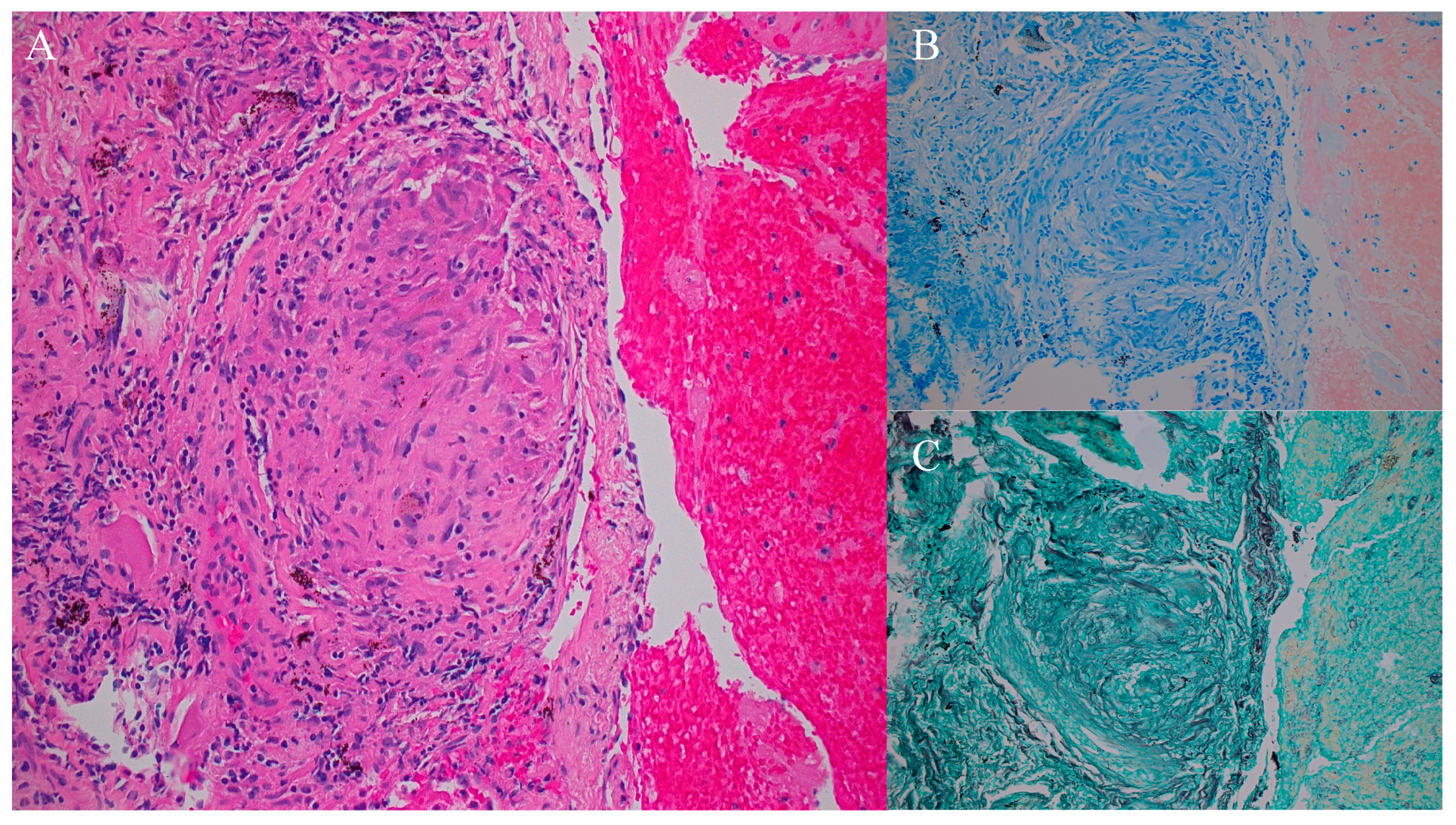
The histopathological hallmark of sarcoidosis is the presence of non-necrotizing granulomas, which are discrete, well-circumscribed aggregates of macrophages, CD4+ T lymphocytes, multi-nucleated giant cells, and epithelial cells that form nodules (Figure 3). Although the inflammatory cascade is implicated, the exact pattern of activation and differentiation remains unclear [13].
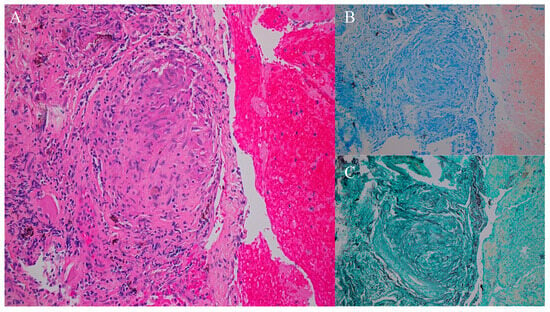
Figure 3.
Transbronchial lung biopsy, with light micrograph demonstrating a non-necrotizing granuloma (A). Acid-fast bacteria (AFB) (B) and Grocott silver staining (C) did not suggest fungal or tuberculosis as causes, respectively, suggesting the likely etiology being sarcoidosis.
3.4. Cardiac Sarcoidosis
It is essential to recognize CS due to the high reported rates of SCD, which may be as significant as 14% [43,44,45]. However, there is significant variation in the reported incidence of CS. For instance, post-mortem studies have reported a prevalence of cardiac involvement ranging from 25% to 58% [9]. Isolated CS, also known as granulomatous myocarditis, is defined as the absence of extra-cardiac manifestations and has a prevalence of as high as 27–52%, which is naturally associated with a poor outcome [13,14,46]. It is important to note that noncaseating granulomas are not unique for sarcoidosis and have also been described in several distinct cardiomyopathies, including myocarditis. CS patients may present with heart failure and are often accompanied by a reduced left ejection fraction (<50%). The severity of symptoms is often proportionate to the extent of myocardial involvement [13]. Although the right ventricle (RV) may also be impacted, it is rare, and its prognostic relevance is unknown. Nonetheless, RV involvement is associated with VAs, which are indicative of worse outcomes [13,47].
In patients with biopsy-proven sarcoidosis, the presence of abnormal PET, MRI, or arrhythmias is suggestive of CS. However, a negative study is insufficient to exclude the possibility of early or subclinical disease. Increased uptake of 18F–FDG is reflective of an augmented risk of VAs, high-grade AV blocks, and SCD [13]. Electrocardiographic (ECG) abnormalities, VAs, and SCD are associated with fibrosis, granulomatous infiltration, and edema [13,48]. Despite the importance of cardiac involvement in sarcoidosis, screening patients is often controversial; it is only considered a Class III recommendation [13]. More importantly, imaging biomarkers cannot always grade the severity of the disease nor diagnose subclinical disease. Therefore, it is more valuable to assess for biomarkers beyond imaging.
The emergence of COVID-19 has led to a hypothesis that the hyperinflammation induced by SARS-CoV-2 infection may accelerate the onset or trigger autoimmune disorders, including sarcoidosis. A shared pathogenic mechanism includes a dysregulated immune system marked by an abundance of IL-17 and IFN-γ [49]. Notably, COVID-19 has been associated with an increased incidence of myocarditis, with rates ranging from 150 to 4000 cases per 100,000 individuals, which is at least 15 times higher than pre-COVID levels [50]. This raises the possibility that the incidence of CS may also increase. One study alluded that COVID-19 myocarditis may be more common in patients with sarcoidosis [51]. Moreover, while a few case reports and series have reported a hypothetical link between COVID-19 and cardiac sarcoidosis, the exact incidence of this association is unknown [52]. Therefore, it is necessary to conduct further prospective and long-term studies to ascertain the long-term sequelae of COVID-19 and the incidence of CS.
3.5. Genetics
The premise of genetic susceptibility in sarcoidosis is strengthened by familial clustering, higher incidence within specific ethnic groups, and studies involving monozygotic twins [53]. Although sarcoidosis is typically sporadic, it is familial in 3.6–9.6% of cases [8]. The observed 80-fold increase in the risk of disease in monozygotic twins provides further evidence supporting the role of a genetic etiology [54]. Further, there is a higher incidence and prevalence of sarcoidosis among black patients, suggesting an inherent genetic susceptibility [55]. For instance, first-degree relatives of black patients with sarcoidosis have a three-fold risk of acquiring the disease. The Sarcoidosis Genetic Linkage Study Consortium (SAGA) and A Case-Control Etiologic Study of Sarcoidosis (ACCESS) identified eight chromosomal regions for increased susceptibility and familial clustering of sarcoidosis, respectively [56,57]. Therefore, these observations account for a synergistic role between environmental factors and the genetic background for triggering sarcoidosis.
Several susceptible loci have been investigated, which include human leucocyte antigen (HLA) genes located in the class II major histocompatibility complex on chromosome 6. In addition, other genes implicated include those influencing antigen processing and presentation, T-cell recruitment and activation, and granulomatous inflammation [55]. One specific HLA allele that increases the likelihood of sarcoidosis and radiographic progression among black families includes DQB1*0602 [58,59]. Butyrophilin-like 2 (BTNL2), located in the class II MHC region on chromosome 6, also confers an increased risk, along with other genetic variants, as detailed in Table 1 [60]. The ACCESS project was important in demonstrating the role of both HLA-DRB1*1101 and HLA-DPB1*0101 as significant risk factors for the development of sarcoidosis [61].
Genome-wide association studies (GWAS) play a crucial role in identifying genetic loci linked to rare diseases [62]. Furthermore, whole exome sequencing (WES) is essential in the search for de novo mutations [63]. Although there may be distinct genes associated with sarcoidosis, it is likely that multiple genes are involved in its susceptibility, disease expression, and progression (Table 2). The significance of these genetic imprints is important in the phenotypic classification of patients and in recognizing the predictive value of the prognosis of sarcoidosis.
Table 2.
Genetic variants associated with sarcoidosis.
More importantly, given the genetic diversity present in sarcoidosis, it may be more prudent to identify genetic changes in inflammatory regulatory pathways. For instance, mTOR and Rac1, which impede the clearance of pathogens or non-organic particles, can alter both macrophage and T-cell responses. Therefore, genetic modifications encoding these regulatory pathways may result in the development of severe sarcoidosis. For instance, mutations in DDIT4 (DNA damage-inducible transcript 4 gene) have been present in a family with severe sarcoidosis [93]. The analysis of the transcriptome enables the possibility of evaluating the loss of expression at the level of the messenger RNA, as well as bridging the gap between genomic data and functional studies. Here, dysregulation in the STAT1 signaling pathway is noted, which highlights the role of the JAK inhibitor, Tofacitinib [1].
Other discrete genetic variants that may play a role in the development of sarcoidosis include 2p25, 2p25.2, 5p15.2, 5p13.1, 5q35.2, 5q35.3, 11q12-13, 17q23, 20q13.2, and 20q13.32 [99,105,106,107].
The Role of Genetics in the Development of Cardiac Sarcoidosis
The literature review has revealed that certain genetic variants (BTNL2, TNF-α, HLA-DRB1, and HLA-DQB1*0601) are associated with the development of cardiac sarcoidosis. This has significant implications in the screening and management of patients with systemic sarcoidosis, as detecting these variants may help in risk stratification for the development of CS. Further, it may enable the earlier use of advanced cardiovascular imaging to aid in diagnosis as well as to tailor treatment that may be individualized to the patient. More importantly, CS is a disorder that may present as SCD. Thus, the identification of positive genetic variants may prompt a lower threshold for the evaluation of arrhythmias and the possibility of implementing an implantable cardioverter defibrillator (ICD). Furthermore, given the possibility of iCS and the link between myocarditis and inherited cardiomyopathies, it may be judicious to investigate whether the genetic architecture of myocarditis may be secondary to sarcoidosis [108,109].
3.6. Treatment of Sarcoidosis
Sarcoidosis patients have a lower survival rate than the general population, with the mortality being reported to be 7.6%. Most fatalities are due to pulmonary fibrosis but may be secondary to cardiac disease. In Japan, the leading cause of mortality is cardiac involvement, accounting for 77% of deaths [8]. Although sarcoidosis may remain stable in many patients, between 20 and 70% require systemic therapy. The treatment of CS is multifactorial, necessitating a combination of systemic therapy and pharmacotherapy directed towards arrhythmias and heart failure in addition to device placement and consideration for cardiac transplantation. The mainstay of medical therapy is immunosuppression, which ranges from corticosteroids to cytotoxic drugs, namely methotrexate, azathioprine, mycophenolate, or leflunomide [13,15]. In severe cases, manipulation of the cytokine network through monoclonal antibodies, such as TNFα antibodies, is important for managing sarcoidosis.
The initial treatment for active CS includes corticosteroids (e.g., prednisolone 1 mg/kg/day), which have been demonstrated to increase long-term survival and recovery of AV conduction [110]. There is no consensus on the dosage of corticosteroids, but these regimes are tailored toward treatment response, which is assessed through clinical events and imaging. Typically, this is often tapered and may be maintained for 12–24 months [110]. However, no impact was noted in terms of recovery of LV function [111]. If not responsive, or patients are experiencing adverse effects, steroid-sparing agents, in isolation or combination, may be considered in a stepwise fashion. The commonly used agents include methotrexate and mycophenolate mofetil. Biologic agents have a longstanding history in the treatment of systemic sarcoidosis but are associated with increased harm in patients with advanced heart failure [112]. Reassuringly, there have been a few studies that have noted improvement in LV ejection fraction with TNFα inhibitors [113].
In addition to immunosuppression, it is essential that patients with CS who experience heart failure are treated with guideline-directed medical therapies (GDMTs). The level of evidence is dependent on whether the LV ejection fraction is reduced, with the four pillars of treatment being an angiotensin-converting enzyme (ACE) inhibitor, angiotensin receptor blocker (ARB), or an angiotensin receptor/neprilysin inhibitor (ARNI), in combination with a mineralocorticoid receptor antagonist (MRA), sodium-glucose cotransporter-2 (SGLT2) inhibitor and beta-blocker. Volume overload is managed by diuretics, with mechanical assist devices and heart transplantation being reserved for those with a fulminant course or terminal heart failure [110]. Electrophysiologic management of CS includes anti-arrhythmic therapy, catheter-directed ablation, or implantable cardiac devices.
4. Discussion
Although often stable, sarcoidosis may exhibit severe symptoms in certain ethnicities, suggesting the need for the identification of genetic influences. Genetic testing has evolved from single gene to next-generation sequencing, providing improved detection of phenotypic expression. Furthermore, it may lead to cascade screening, with possible subsequent evidence-based recommendations that may influence disease progression or targeted therapies aiming to improve both morbidity and mortality. The traditional management of inherited cardiomyopathy has divided the approach to inflammatory cardiomyopathies. Therefore, identifying possible genetic factors and the ability to modify them may be integral to disease prevention, risk stratification, and management.
The aforementioned genetic data confirms the significant genetic influence of sarcoidosis, with BTNL2, TNF-α, HLA-DRB1, and HLA-DQB1*0601 being associated with the development of cardiac sarcoidosis [78,82,113]. Despite the extensive data available, early diagnosis and the definition of genetic profiles associated with severe and chronic CS remain a challenge. More importantly, while classical Mendelian diseases are caused by specific mutations, complex diseases, such as sarcoidosis, involve multiple genes, each contributing an effect of varying magnitude. Furthermore, there are over 7000 specific combinations of HLA variants, which makes it challenging to truly identify a specific genetic insult to the development of sarcoidosis [114]. Nonetheless, HLA alleles may aid clinical decisions, as they may provide information about the chronicity, subtypes and risk of developing cardiac sarcoidosis. More importantly, it may be useful to decide whether aggressive treatment or active surveillance is warranted. Beyond variation in the HLA system, other genetic factors identified through GWAS may be more useful in understanding the pathogenesis and, thus, treatment of cardiac sarcoidosis.
Notably, Castrichini et al. demonstrated that co-existing genetic variants associated with inherited cardiomyopathies, including LMNA, DSP, myosin binding protein C3 (MYBPC3), myosin heavy chain 7 (MHY7), and TTN, may be present in CS patients [115,116]. Although not useful for disease stratification for CS, the presence of these genes either indicates a clinical overlap or a diagnosis of an inherited cardiomyopathy mimicking CS. Therefore, management should focus on the specific cardiomyopathy rather than one of immunosuppression.
It should be noted that genetic testing and screening has its limitations. For instance, variants of uncertain significance (VUS) are common and have yet to be reported as either benign or disease-provoking. While current guidelines do not recommend genetic testing in inflammatory cardiomyopathies, identification of specific genes may improve risk stratification and family screening. More importantly, although ethnic and familial clustering has been observed, there has not been a monogenic cause of sarcoidosis. Furthermore, although CS case studies have implicated certain genetic variants, this cannot be generalized to the entire sarcoid population.
5. Conclusions
The incidence of sarcoidosis is characterized by a high degree of variability, which poses a significant challenge in accurately diagnosing this elusive disorder and, subsequently, managing it effectively. Refined assessment based on genetic evaluation may have a significant impact on risk stratification and management protocols. Increasing evidence highlights the crucial role of genetic variants in cardiac sarcoidosis, which not only plays a key role in pathophysiology but may also guide risk stratification and management. While it remains to be established whether genetics may institute a therapeutic target in cardiac sarcoidosis, continued investment in its role may prove fruitful when targeted gene therapy is available. Further prospective studies are needed to identify whether certain immunomodulators may be more appropriate in achieving disease remission in patients with certain genetic variants.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/cardiogenetics14020009/s1, Figure S1: PRISMA flow diagram describing the selection of studies for review [117].
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data sharing is not applicable to this article.
Acknowledgments
We are grateful to Aditya Talwar for the assistance in preparation of the pathology figures.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Calender, A.; Weichhart, T.; Valeyre, D.; Pacheco, Y. Current Insights in Genetics of Sarcoidosis: Functional and Clinical Impacts. J. Clin. Med. 2020, 9, 2633. [Google Scholar] [CrossRef] [PubMed]
- Mahmoud, A.R.; Dahy, A.; Dibas, M.; Abbas, A.S.; Ghozy, S.; El-Qushayri, A.E. Association between sarcoidosis and cardiovascular comorbidity: A systematic review and meta-analysis. Heart Lung 2020, 49, 512–517. [Google Scholar] [CrossRef] [PubMed]
- Soto-Gomez, N.; Peters, J.I.; Nambiar, A.M. Diagnosis and Management of Sarcoidosis. Am. Fam. Physician 2016, 93, 840–848. [Google Scholar] [PubMed]
- Kobak, S. Catch the rainbow: Prognostic factor of sarcoidosis. Lung India 2020, 37, 425–432. [Google Scholar] [CrossRef] [PubMed]
- Grunewald, J.; Grutters, J.C.; Arkema, E.V.; Saketkoo, L.A.; Moller, D.R.; Müller-Quernheim, J. Sarcoidosis. Nat. Rev. Dis. Primers 2019, 5, 45. [Google Scholar] [CrossRef] [PubMed]
- Arkema, E.V.; Cozier, Y.C. Sarcoidosis epidemiology: Recent estimates of incidence, prevalence and risk factors. Curr. Opin. Pulm. Med. 2020, 26, 527–534. [Google Scholar] [CrossRef] [PubMed]
- Westney, G.E.; Judson, M.A. Racial and ethnic disparities in sarcoidosis: From genetics to socioeconomics. Clin. Chest Med. 2006, 27, 453–462. [Google Scholar] [CrossRef]
- Valeyre, D.; Prasse, A.; Nunes, H.; Uzunhan, Y.; Brillet, P.Y.; Müller-Quernheim, J. Sarcoidosis. Lancet 2014, 383, 1155–1167. [Google Scholar] [CrossRef] [PubMed]
- Hulten, E.; Aslam, S.; Osborne, M.; Abbasi, S.; Bittencourt, M.S.; Blankstein, R. Cardiac sarcoidosis-state of the art review. Cardiovasc. Diagn. Ther. 2016, 6, 50–63. [Google Scholar] [CrossRef]
- Birnie, D.H.; Nery, P.B.; Ha, A.C.; Beanlands, R.S. Cardiac Sarcoidosis. J. Am. Coll. Cardiol. 2016, 68, 411–421. [Google Scholar] [CrossRef]
- Lehtonen, J.; Uusitalo, V.; Pöyhönen, P.; Mäyränpää, M.I.; Kupari, M. Cardiac sarcoidosis: Phenotypes, diagnosis, treatment, and prognosis. Eur. Heart J. 2023, 44, 1495–1510. [Google Scholar] [CrossRef] [PubMed]
- Uemura, A.; Morimoto, S.; Hiramitsu, S.; Kato, Y.; Ito, T.; Hishida, H. Histologic diagnostic rate of cardiac sarcoidosis: Evaluation of endomyocardial biopsies. Am. Heart J. 1999, 138 Pt 1, 299–302. [Google Scholar] [CrossRef] [PubMed]
- Trivieri, M.G.; Spagnolo, P.; Birnie, D.; Liu, P.; Drake, W.; Kovacic, J.C.; Baughman, R.; Fayad, Z.A.; Judson, M.A. Challenges in Cardiac and Pulmonary Sarcoidosis: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2020, 76, 1878–1901. [Google Scholar] [CrossRef] [PubMed]
- Bernardinello, N.; Petrarulo, S.; Balestro, E.; Cocconcelli, E.; Veltkamp, M.; Spagnolo, P. Pulmonary Sarcoidosis: Diagnosis and Differential Diagnosis. Diagnostics 2021, 11, 1558. [Google Scholar] [CrossRef] [PubMed]
- McKinzie, B.P.; Bullington, W.M.; Mazur, J.E.; Judson, M.A. Efficacy of short-course, low-dose corticosteroid therapy for acute pulmonary sarcoidosis exacerbations. Am. J. Med. Sci. 2010, 339, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Voortman, M.; Hendriks, C.M.R.; Elfferich, M.D.P.; Bonella, F.; Møller, J.; De Vries, J.; Costabel, U.; Drent, M. The Burden of Sarcoidosis Symptoms from a Patient Perspective. Lung 2019, 197, 155–161. [Google Scholar] [CrossRef] [PubMed]
- Ungprasert, P.; Carmona, E.M.; Crowson, C.S.; Matteson, E.L. Diagnostic Utility of Angiotensin-Converting Enzyme in Sarcoidosis: A Population-Based Study. Lung 2016, 194, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Vanmaris, R.M.M.; Rijkers, G.T. Biological role of the soluble interleukin-2 receptor in sarcoidosis. Sarcoidosis Vasc. Diffus. Lung Dis. 2017, 34, 122–129. [Google Scholar] [CrossRef] [PubMed]
- Kraaijvanger, R.; Janssen Bonás, M.; Vorselaars, A.D.M.; Veltkamp, M. Biomarkers in the Diagnosis and Prognosis of Sarcoidosis: Current Use and Future Prospects. Front. Immunol. 2020, 11, 1443. [Google Scholar] [CrossRef]
- Prabhakar, H.B.; Rabinowitz, C.B.; Gibbons, F.K.; O’Donnell, W.J.; Shepard, J.A.; Aquino, S.L. Imaging features of sarcoidosis on MDCT, FDG PET, and PET/CT. AJR Am. J. Roentgenol. 2008, 190 (Suppl. S3), S1–S6. [Google Scholar] [CrossRef]
- Casella, M.; Dello Russo, A.; Bergonti, M.; Catto, V.; Conte, E.; Sommariva, E.; Gasperetti, A.; Vettor, G.; Tundo, F.; Sicuso, R.; et al. Diagnostic Yield of Electroanatomic Voltage Mapping in Guiding Endomyocardial Biopsies. Circulation 2020, 142, 1249–1260. [Google Scholar] [CrossRef]
- Benz, D.C.; Gräni, C.; Antiochos, P.; Heydari, B.; Gissler, M.C.; Ge, Y.; Cuddy, S.A.M.; Dorbala, S.; Kwong, R.Y. Cardiac magnetic resonance biomarkers as surrogate endpoints in cardiovascular trials for myocardial diseases. Eur. Heart J. 2023, 44, 4738–4747. [Google Scholar] [CrossRef]
- Marschner, C.A.; Aloufi, F.; Aitken, M.; Cheung, E.; Thavendiranathan, P.; Iwanochko, R.M.; Balter, M.; Moayedi, Y.; Duero Posada, J.; Hanneman, K. Combined FDG PET/MRI versus Standard-of-Care Imaging in the Evaluation of Cardiac Sarcoidosis. Radiol. Cardiothorac. Imaging 2023, 5, e220292. [Google Scholar] [CrossRef]
- Kurashima, S.; Kitai, T.; Xanthopoulos, A.; Skoularigis, J.; Triposkiadis, F.; Izumi, C. Diagnosis of cardiac sarcoidosis: Histological evidence vs. imaging. Expert. Rev. Cardiovasc. Ther. 2023, 21, 693–702. [Google Scholar] [CrossRef]
- Hervier, E.; Glessgen, C.; Nkoulou, R.; François Deux, J.; Vallee, J.P.; Adamopoulos, D. Hybrid PET/MR in Cardiac Imaging. Magn. Reson. Imaging Clin. N. Am. 2023, 31, 613–624. [Google Scholar] [CrossRef]
- Shrivastav, R.; Hajra, A.; Krishnan, S.; Bandyopadhyay, D.; Ranjan, P.; Fuisz, A. Evaluation and Management of Cardiac Sarcoidosis with Advanced Imaging. Heart Fail. Clin. 2023, 19, 475–489. [Google Scholar] [CrossRef]
- Puntmann, V.O.; Isted, A.; Hinojar, R.; Foote, L.; Carr-White, G.; Nagel, E. T1 and T2 Mapping in Recognition of Early Cardiac Involvement in Systemic Sarcoidosis. Radiology 2017, 285, 63–72. [Google Scholar] [CrossRef]
- Okafor, J.; Khattar, R.; Sharma, R.; Kouranos, V. The Role of Echocardiography in the Contemporary Diagnosis and Prognosis of Cardiac Sarcoidosis: A Comprehensive Review. Life 2023, 13, 1653. [Google Scholar] [CrossRef]
- Dweck, M.R.; Abgral, R.; Trivieri, M.G.; Robson, P.M.; Karakatsanis, N.; Mani, V.; Palmisano, A.; Miller, M.A.; Lala, A.; Chang, H.L.; et al. Hybrid Magnetic Resonance Imaging and Positron Emission Tomography with Fluorodeoxyglucose to Diagnose Active Cardiac Sarcoidosis. JACC Cardiovasc. Imaging 2018, 11, 94–107. [Google Scholar] [CrossRef]
- Birnie, D.H.; Sauer, W.H.; Bogun, F.; Cooper, J.M.; Culver, D.A.; Duvernoy, C.S.; Judson, M.A.; Kron, J.; Mehta, D.; Cosedis Nielsen, J.; et al. HRS expert consensus statement on the diagnosis and management of arrhythmias associated with cardiac sarcoidosis. Heart Rhythm. 2014, 11, 1305–1323. [Google Scholar] [CrossRef]
- Terasaki, F.; Azuma, A.; Anzai, T.; Ishizaka, N.; Ishida, Y.; Isobe, M.; Inomata, T.; Ishibashi-Ueda, H.; Eishi, Y.; Kitakaze, M.; et al. JCS 2016 Guideline on Diagnosis and Treatment of Cardiac Sarcoidosis—Digest Version. Circ. J. 2019, 83, 2329–2388. [Google Scholar] [CrossRef]
- Savale, L.; Huitema, M.; Shlobin, O.; Kouranos, V.; Nathan, S.D.; Nunes, H.; Gupta, R.; Grutters, J.C.; Culver, D.A.; Post, M.C.; et al. WASOG statement on the diagnosis and management of sarcoidosis-associated pulmonary hypertension. Eur. Respir. Rev. 2022, 31, 210165. [Google Scholar] [CrossRef]
- Bokhari, S.; Sheikh, T. Cardiac sarcoidosis: Advantages and limitations of advanced cardiac imaging. J. Nucl. Cardiol. 2022, 29, 2145–2148. [Google Scholar] [CrossRef]
- Pöyhönen, P.; Nordenswan, H.K.; Lehtonen, J.; Syväranta, S.; Shenoy, C.; Kupari, M. Cardiac magnetic resonance in giant cell myocarditis: A matched comparison with cardiac sarcoidosis. Eur. Heart J. Cardiovasc. Imaging 2023, 24, 404–412. [Google Scholar] [CrossRef]
- Ekström, K.; Räisänen-Sokolowski, A.; Lehtonen, J.; Nordenswan, H.K.; Mäyränpää, M.I.; Kupari, M. Idiopathic giant cell myocarditis or cardiac sarcoidosis? A retrospective audit of a nationwide case series. ESC Heart Fail. 2020, 7, 1362–1370. [Google Scholar] [CrossRef]
- Trivieri, M.G.; Robson, P.M.; Vergani, V.; LaRocca, G.; Romero-Daza, A.M.; Abgral, R.; Devesa, A.; Azoulay, L.-D.; Karakatsanis, N.A.; Parikh, A.; et al. Hybrid Magnetic Resonance Positron Emission Tomography Is Associated with Cardiac-Related Outcomes in Cardiac Sarcoidosis. JACC Cardiovasc. Imaging 2024, 17, 411–424. [Google Scholar] [CrossRef]
- Jeudy, J.; Burke, A.P.; White, C.S.; Kramer, G.B.; Frazier, A.A. Cardiac sarcoidosis: The challenge of radiologic-pathologic correlation: From the radiologic pathology archives. Radiographics 2015, 35, 657–679. [Google Scholar] [CrossRef]
- Morimoto, T.; Azuma, A.; Abe, S.; Usuki, J.; Kudoh, S.; Sugisaki, K.; Oritsu, M.; Nukiwa, T. Epidemiology of sarcoidosis in Japan. Eur. Respir. J. 2008, 31, 372–379. [Google Scholar] [CrossRef]
- Birnbaum, A.D.; Rifkin, L.M. Sarcoidosis: Sex-dependent variations in presentation and management. J. Ophthalmol. 2014, 2014, 236905. [Google Scholar] [CrossRef]
- Giblin, G.T.; Murphy, L.; Stewart, G.C.; Desai, A.S.; Di Carli, M.F.; Blankstein, R.; Givertz, M.M.; Tedrow, U.B.; Sauer, W.H.; Hunninghake, G.M.; et al. Cardiac Sarcoidosis: When and How to Treat Inflammation. Card. Fail. Rev. 2021, 7, e17. [Google Scholar] [CrossRef]
- Zhang, H.; Costabel, U.; Dai, H. The Role of Diverse Immune Cells in Sarcoidosis. Front. Immunol. 2021, 12, 788502. [Google Scholar] [CrossRef]
- Schnerch, J.; Prasse, A.; Vlachakis, D.; Schuchardt, K.L.; Pechkovsky, D.V.; Goldmann, T.; Gaede, K.I.; Müller-Quernheim, J.; Zissel, G. Functional Toll-Like Receptor 9 Expression and CXCR3 Ligand Release in Pulmonary Sarcoidosis. Am. J. Respir. Cell Mol. Biol. 2016, 55, 749–757. [Google Scholar] [CrossRef]
- Chahal, C.A.A.; Brady, P.A.; Cooper LTJr Lin, G.; Somers, V.K.; Crowson, C.S.; Matteson, E.L.; Ungprasert, P. Risk of Sudden Death in a General Unbiased Epidemiological Cohort of Sarcoidosis. J. Am. Heart Assoc. 2022, 11, e025479. [Google Scholar] [CrossRef]
- Narasimhan, B.; Patel, N.; Ho, K.; Amgai, B.; Okada, D.R.; Bandyopadhyay, D.; Krittanawong, C.; Wu, L.; Bhatia, K.; Shah, R.; et al. Incidence and Predictors of Sudden Cardiac Arrest in Sarcoidosis: A Nationwide Analysis. JACC Clin. Electrophysiol. 2021, 7, 1087–1095. [Google Scholar] [CrossRef]
- Ekström, K.; Lehtonen, J.; Nordenswan, H.K.; Mäyränpää, M.I.; Räisänen-Sokolowski, A.; Kandolin, R.; Simonen, P.; Pietilä-Effati, P.; Alatalo, A.; Utriainen, S.; et al. Sudden death in cardiac sarcoidosis: An analysis of nationwide clinical and cause-of-death registries. Eur. Heart J. 2019, 40, 3121–3128. [Google Scholar] [CrossRef]
- Okada, D.R.; Bravo, P.E.; Vita, T.; Agarwal, V.; Osborne, M.T.; Taqueti, V.R.; Skali, H.; Chareonthaitawee, P.; Dorbala, S.; Stewart, G.; et al. Isolated cardiac sarcoidosis: A focused review of an under-recognized entity. J. Nucl. Cardiol. 2018, 25, 1136–1146. [Google Scholar] [CrossRef]
- Smedema, J.P.; van Geuns, R.J.; Ainslie, G.; Ector, J.; Heidbuchel, H.; Crijns, H.J.G.M. Right ventricular involvement in cardiac sarcoidosis demonstrated with cardiac magnetic resonance. ESC Heart Fail. 2017, 4, 535–544. [Google Scholar] [CrossRef]
- Okada, D.R.; Smith, J.; Derakhshan, A.; Gowani, Z.; Misra, S.; Berger, R.D.; Calkins, H.; Tandri, H.; Chrispin, J. Ventricular Arrhythmias in Cardiac Sarcoidosis. Circulation 2018, 138, 1253–1264. [Google Scholar] [CrossRef]
- Vij, O.; Dey, M.; Morrison, K.; Kouranloo, K. Incidence, management and prognosis of new-onset sarcoidosis post COVID-19 infection. Sarcoidosis Vasc. Diffus. Lung Dis. 2024, 41, e2024004. [Google Scholar] [CrossRef]
- Fairweather, D.; Beetler, D.J.; Di Florio, D.N.; Musigk, N.; Heidecker, B.; Cooper, L.T., Jr. COVID-19, Myocarditis and Pericarditis. Circ. Res. 2023, 132, 1302–1319. [Google Scholar] [CrossRef]
- Zadeh, A.V.; Redondo, A.; Carrero, R.C.; Collado, E.; Larned, J.M. The impact of sarcoidosis on the risk of COVID-19-related myocarditis. J. Am. Coll. Cardiol. 2024, 83 (Suppl. 113), 678. [Google Scholar] [CrossRef]
- Bollano, E.; Polte, C.L.; Mäyränpää, M.I.; Oldfors, A.; Bergh, N.; Lehtonen, J.; Kandolin, R. Cardiac sarcoidosis and giant cell myocarditis after COVID-19 infection. ESC Heart Fail. 2022, 9, 4298–4303. [Google Scholar] [CrossRef]
- Ueberham, L.; Hagendorff, A.; Klingel, K.; Paetsch, I.; Jahnke, C.; Kluge, T.; Ebbinghaus, H.; Hindricks, G.; Laufs, U.; Dinov, B. Pathophysiological Gaps, Diagnostic Challenges, and Uncertainties in Cardiac Sarcoidosis. J. Am. Heart Assoc. 2023, 12, e027971. [Google Scholar] [CrossRef]
- Sverrild, A.; Backer, V.; Kyvik, K.O.; Kaprio, J.; Milman, N.; Svendsen, C.B.; Thomsen, S.F. Heredity in sarcoidosis: A registry-based twin study. Thorax 2008, 63, 894–896. [Google Scholar] [CrossRef] [PubMed]
- Hena, K.M. Sarcoidosis Epidemiology: Race Matters. Front. Immunol. 2020, 11, 537382. [Google Scholar] [CrossRef]
- Iannuzzi, M.C.; Iyengar, S.K.; Gray-McGuire, C.; Elston, R.C.; Baughman, R.P.; Donohue, J.F.; Hirst, K.; Judson, M.A.; Kavuru, M.S.; Maliarik, M.J.; et al. Genome-wide search for sarcoidosis susceptibility genes in African Americans. Genes Immun. 2005, 6, 509–518. [Google Scholar] [CrossRef]
- Semenzato, G. ACCESS: A Case Control Etiologic Study of Sarcoidosis. Sarcoidosis Vasc. Diffus. Lung Dis. 2005, 22, 83–86. [Google Scholar]
- Sikorova, K.; Osoegawa, K.; Kocourkova, L.; Strnad, A.; Petrkova, J.; Fernández-Viña, M.A.; Doubkova, M.; Petrek, M. Association between sarcoidosis and HLA polymorphisms in a Czech population from Central Europe: Focus on a relationship with clinical outcome and treatment. Front. Med. 2023, 10, 1094843. [Google Scholar] [CrossRef]
- Voorter, C.E.; Drent, M.; van den Berg-Loonen, E.M. Severe pulmonary sarcoidosis is strongly associated with the haplotype HLA-DQB1*0602-DRB1*150101. Hum. Immunol. 2005, 66, 826–835. [Google Scholar] [CrossRef]
- Becker, C.D.; Sridhar, P.; Iannuzzi, M.C. Cardiac sarcoidosis associated with BTNL2. Cardiology 2009, 112, 76–79. [Google Scholar] [CrossRef]
- Rossman, M.D.; Thompson, B.; Frederick, M.; Maliarik, M.; Iannuzzi, M.C.; Rybicki, B.A.; Pandey, J.P.; Newman, L.S.; Magira, E.; Beznik-Cizman, B.; et al. HLA-DRB1*1101: A significant risk factor for sarcoidosis in blacks and whites. Am. J. Hum. Genet. 2003, 73, 720–735. [Google Scholar] [CrossRef]
- Dehghan, A. Genome-Wide Association Studies. Methods Mol. Biol. 2018, 1793, 37–49. [Google Scholar] [CrossRef]
- Jaganathan, D.; Bohra, A.; Thudi, M.; Varshney, R.K. Fine mapping and gene cloning in the post-NGS era: Advances and prospects. Theor. Appl. Genet. 2020, 133, 1791–1810. [Google Scholar] [CrossRef]
- Zorzetto, M.; Bombieri, C.; Ferrarotti, I.; Medaglia, S.; Agostini, C.; Tinelli, C.; Malerba, G.; Carrabino, N.; Beretta, A.; Casali, L.; et al. Complement receptor 1 gene polymorphisms in sarcoidosis. Am. J. Respir. Cell Mol. Biol. 2002, 27, 17–23. [Google Scholar] [CrossRef]
- Hill, M.R.; Papafili, A.; Booth, H.; Lawson, P.; Hubner, M.; Beynon, H.; Read, C.; Lindahl, G.; Marshall, R.P.; McAnulty, R.J.; et al. Functional prostaglandin-endoperoxide synthase 2 polymorphism predicts poor outcome in sarcoidosis. Am. J. Respir. Crit. Care Med. 2006, 174, 915–922. [Google Scholar] [CrossRef]
- Lahtela, E.; Kankainen, M.; Sinisalo, J.; Selroos, O.; Lokki, M.L. Exome Sequencing Identifies Susceptibility Loci for Sarcoidosis Prognosis. Front. Immunol. 2019, 10, 2964. [Google Scholar] [CrossRef]
- Kim, H.S.; Choi, D.; Lim, L.L.; Allada, G.; Smith, J.R.; Austin, C.R.; Doyle, T.M.; Goodwin, K.A.; Rosenbaum, J.T.; Martin, T.M. Association of interleukin 23 receptor gene with sarcoidosis. Dis. Markers 2011, 31, 17–24. [Google Scholar] [CrossRef]
- Spagnolo, P.; Maier, L.A. Genetics in sarcoidosis. Curr. Opin. Pulm. Med. 2021, 27, 423–429. [Google Scholar] [CrossRef]
- Karakaya, B.; van Moorsel, C.H.M.; Veltkamp, M.; Roodenburg-Benschop, C.; Kazemier, K.M.; van der Helm-van Mil, A.H.M.; Huizinga, T.W.J.; Grutters, J.C.; Rijkers, G.T. A Polymorphism in C-C Chemokine Receptor 5 (CCR5) Associates with Löfgren’s Syndrome and Alters Receptor Expression as well as Functional Response. Cells 2021, 10, 1967. [Google Scholar] [CrossRef]
- Garman, L.; Pezant, N.; Pastori, A.; Savoy, K.A.; Li, C.; Levin, A.M.; Iannuzzi, M.C.; Rybicki, B.A.; Adrianto, I.; Montgomery, C.G. Genome-Wide Association Study of Ocular Sarcoidosis Confirms HLA Associations and Implicates Barrier Function and Autoimmunity in African Americans. Ocul. Immunol. Inflamm. 2021, 29, 244–249. [Google Scholar] [CrossRef]
- Drent, M.; van den Berg, R.; Haenen, G.R.; van den Berg, H.; Wouters, E.F.; Bast, A. NF-kappaB activation in sarcoidosis. Sarcoidosis Vasc. Diffus. Lung Dis. 2001, 18, 50–56. [Google Scholar]
- Gray-McGuire, C.; Sinha, R.; Iyengar, S.; Millard, C.; Rybicki, B.A.; Elston, R.C.; Iannuzzi, M.C.; SAGA Study Consortium. Genetic characterization and fine mapping of susceptibility loci for sarcoidosis in African Americans on chromosome 5. Hum. Genet. 2006, 120, 420–430. [Google Scholar] [CrossRef]
- Ozyilmaz, E.; Ozturk, O.G.; Durmaz, A.; Othman Hasan, O.; Guzelbaba, B.; Seydaoglu, G.; Kuleci, S.; Hanta, I.; Erken, E.; Kocabas, A. Early prediction of sarcoidosis prognosis with HLA typing: A 5 year follow-up study. Sarcoidosis Vasc. Diffus. Lung Dis. 2018, 35, 184–191. [Google Scholar] [CrossRef]
- Hedfors, E.; Lindström, F. HLA-B8/DR3 in sarcoidosis. Correlation to acute onset disease with arthritis. Tissue Antigens 1983, 22, 200–203. [Google Scholar] [CrossRef]
- Zhou, Y.; Shen, L.; Zhang, Y.; Jiang, D.; Li, H. Human leukocyte antigen-A, -B, and -DRB1 alleles and sarcoidosis in Chinese Han subjects. Hum. Immunol. 2011, 72, 571–575. [Google Scholar] [CrossRef]
- Sato, H.; Woodhead, F.A.; Ahmad, T.; Grutters, J.C.; Spagnolo, P.; van den Bosch, J.M.; Maier, L.A.; Newman, L.S.; Nagai, S.; Izumi, T.; et al. Sarcoidosis HLA class II genotyping distinguishes differences of clinical phenotype across ethnic groups. Hum. Mol. Genet. 2010, 19, 4100–4111. [Google Scholar] [CrossRef]
- Liao, S.Y.; Jacobson, S.; Hamzeh, N.Y.; Culver, D.A.; Barkes, B.Q.; Mroz, M.; Macphail, K.; Pacheco, K.; Patel, D.C.; Wasfi, Y.S.; et al. Genome-wide association study identifies multiple HLA loci for sarcoidosis susceptibility. Hum. Mol. Genet. 2023, 32, 2669–2678. [Google Scholar] [CrossRef] [PubMed]
- Naruse, T.K.; Matsuzawa, Y.; Ota, M.; Katsuyama, Y.; Matsumori, A.; Hara, M.; Nagai, S.; Morimoto, S.; Sasayama, S.; Inoko, H. HLA-DQB1*0601 is primarily associated with the susceptibility to cardiac sarcoidosis. Tissue Antigens 2000, 56, 52–57. [Google Scholar] [CrossRef]
- Levin, A.M.; Adrianto, I.; Datta, I.; Iannuzzi, M.C.; Trudeau, S.; Li, J.; Drake, W.P.; Montgomery, C.G.; Rybicki, B.A. Association of HLA-DRB1 with Sarcoidosis Susceptibility and Progression in African Americans. Am. J. Respir. Cell Mol. Biol. 2015, 53, 206–216. [Google Scholar] [CrossRef]
- Darlington, P.; Gabrielsen, A.; Sörensson, P.; Tallstedt, L.; Padyukov, L.; Eklund, A.; Grunewald, J. HLA-alleles associated with increased risk for extra-pulmonary involvement in sarcoidosis. Tissue Antigens 2014, 83, 267–272. [Google Scholar] [CrossRef]
- Li, Y.; Wollnik, B.; Pabst, S.; Lennarz, M.; Rohmann, E.; Gillissen, A.; Vetter, H.; Grohé, C. BTNL2 gene variant and sarcoidosis. Thorax 2006, 61, 273–274. [Google Scholar] [CrossRef]
- Meyer, T.; Lauschke, J.; Ruppert, V.; Richter, A.; Pankuweit, S.; Maisch, B. Isolated cardiac sarcoidosis associated with the expression of a splice variant coding for a truncated BTNL2 protein. Cardiology 2008, 109, 117–121. [Google Scholar] [CrossRef]
- Bogunia-Kubik, K.; Koscinska, K.; Suchnicki, K.; Lange, A. HSP70-hom gene single nucleotide (+2763 G/A and +2437 C/T) polymorphisms in sarcoidosis. Int. J. Immunogenet. 2006, 33, 135–140. [Google Scholar] [CrossRef]
- Casanova, N.G.; Gonzalez-Garay, M.L.; Sun, B.; Bime, C.; Sun, X.; Knox, K.S.; Crouser, E.D.; Sammani, N.; Gonzales, T.; Natt, B.; et al. Differential transcriptomics in sarcoidosis lung and lymph node granulomas with comparisons to pathogen-specific granulomas. Respir. Res. 2020, 21, 321. [Google Scholar] [CrossRef]
- McDougal, K.E.; Fallin, M.D.; Moller, D.R.; Song, Z.; Cutler, D.J.; Steiner, L.L.; Cutting, G.R.; ACCESS Research Group. Variation in the lymphotoxin-alpha/tumor necrosis factor locus modifies risk of erythema nodosum in sarcoidosis. J. Investig. Dermatol. 2009, 129, 1921–1926. [Google Scholar] [CrossRef]
- Davoudi, S.; Chang, V.S.; Navarro-Gomez, D.; Stanwyck, L.K.; Sevgi, D.D.; Papavasileiou, E.; Ren, A.; Uchiyama, E.; Sullivan, L.; Lobo, A.M.; et al. Association of genetic variants in RAB23 and ANXA11 with uveitis in sarcoidosis. Mol. Vis. 2018, 24, 59–74. [Google Scholar]
- Foley, P.J.; Lympany, P.A.; Puscinska, E.; Zielinski, J.; Welsh, K.I.; du Bois, R.M. Analysis of MHC encoded antigen-processing genes TAP1 and TAP2 polymorphisms in sarcoidosis. Am. J. Respir. Crit. Care Med. 1999, 160, 1009–1014. [Google Scholar] [CrossRef]
- Medica, I.; Kastrin, A.; Maver, A.; Peterlin, B. Role of genetic polymorphisms in ACE and TNF-alpha gene in sarcoidosis: A meta-analysis. J. Hum. Genet. 2007, 52, 836–847. [Google Scholar] [CrossRef]
- Gialafos, E.; Triposkiadis, F.; Kouranos, V.; Rapti, A.; Kosmas, I.; Manali, E.; Giamouzis, G.; Elezoglou, A.; Peros, I.; Anagnostopoulou, O.; et al. Relationship between tumor necrosis factor-α (TNFA) gene polymorphisms and cardiac sarcoidosis. In Vivo 2014, 28, 1125–1129. [Google Scholar]
- Meguro, A.; Ishihara, M.; Petrek, M.; Yamamoto, K.; Takeuchi, M.; Mrazek, F.; Kolek, V.; Benicka, A.; Yamane, T.; Shibuya, E.; et al. Genetic control of CCL24, POR, and IL23R contributes to the pathogenesis of sarcoidosis. Commun. Biol. 2020, 3, 465. [Google Scholar] [CrossRef]
- Akahoshi, M.; Ishihara, M.; Remus, N.; Uno, K.; Miyake, K.; Hirota, T.; Nakashima, K.; Matsuda, A.; Kanda, M.; Enomoto, T.; et al. Association between IFNA genotype and the risk of sarcoidosis. Hum. Genet. 2004, 114, 503–509. [Google Scholar] [CrossRef] [PubMed]
- Pabst, S.; Baumgarten, G.; Stremmel, A.; Lennarz, M.; Knüfermann, P.; Gillissen, A.; Vetter, H.; Grohé, C. Toll-like receptor (TLR) 4 polymorphisms are associated with a chronic course of sarcoidosis. Clin. Exp. Immunol. 2006, 143, 420–426. [Google Scholar] [CrossRef] [PubMed]
- Calender, A.; Lim, C.X.; Weichhart, T.; Buisson, A.; Besnard, V.; Rollat-Farnier, P.A.; Bardel, C.; Roy, P.; Cottin, V.; Devouassoux, G.; et al. Exome sequencing and pathogenicity-network analysis of five French families implicate mTOR signalling and autophagy in familial sarcoidosis. Eur. Respir. J. 2019, 54, 1900430. [Google Scholar] [CrossRef] [PubMed]
- Thompson, C.L.; Rybicki, B.A.; Iannuzzi, M.C.; Elston, R.C.; Iyengar, S.K.; Gray-McGuire, C.; Sarcoidosis Genetic Analysis Consortium (SAGA). Reduction of sample heterogeneity through use of population substructure: An example from a population of African American families with sarcoidosis. Am. J. Hum. Genet. 2006, 79, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Ohchi, T.; Shijubo, N.; Kawabata, I.; Ichimiya, S.; Inomata, S.; Yamaguchi, A.; Umemori, Y.; Itoh, Y.; Abe, S.; Hiraga, Y.; et al. Polymorphism of Clara cell 10-kD protein gene of sarcoidosis. Am. J. Respir. Crit. Care Med. 2004, 169, 180–186. [Google Scholar] [CrossRef] [PubMed]
- Fischer, A.; Schmid, B.; Ellinghaus, D.; Nothnagel, M.; Gaede, K.I.; Schürmann, M.; Lipinski, S.; Rosenstiel, P.; Zissel, G.; Höhne, K.; et al. A novel sarcoidosis risk locus for Europeans on chromosome 11q13. 1. Am. J. Respir. Crit. Care Med. 2012, 186, 877–885. [Google Scholar] [CrossRef] [PubMed]
- Stjepanovic, M.I.; Mihailovic-Vucinic, V.; Spasovski, V.; Milin-Lazovic, J.; Skodric-Trifunovic, V.; Stankovic, S.; Andjelkovic, M.; Komazec, J.; Momcilovic, A.; Santric-Milicevic, M.; et al. Genes and metabolic pathway of sarcoidosis: Identification of key players and risk modifiers. Arch. Med. Sci. 2019, 15, 1138–1146. [Google Scholar] [CrossRef] [PubMed]
- Fischer, A.; Ellinghaus, D.; Nutsua, M.; Hofmann, S.; Montgomery, C.G.; Iannuzzi, M.C.; Rybicki, B.A.; Petrek, M.; Mrazek, F.; Pabst, S.; et al. Identification of Immune-Relevant Factors Conferring Sarcoidosis Genetic Risk. Am. J. Respir. Crit. Care Med. 2015, 192, 727–736. [Google Scholar] [CrossRef]
- Hofmann, S.; Fischer, A.; Nothnagel, M.; Jacobs, G.; Schmid, B.; Wittig, M.; Franke, A.; Gaede, K.I.; Schürmann, M.; Petrek, M.; et al. Genome-wide association analysis reveals 12q13.3-q14.1 as new risk locus for sarcoidosis. Eur. Respir. J. 2013, 41, 888–900. [Google Scholar] [CrossRef]
- Pabst, S.; Fränken, T.; Schönau, J.; Stier, S.; Nickenig, G.; Meyer, R.; Skowasch, D.; Grohé, C. Transforming growth factor-{beta} gene polymorphisms in different phenotypes of sarcoidosis. Eur. Respir. J. 2011, 38, 169–175. [Google Scholar] [CrossRef]
- Lareau, C.A.; Adrianto, I.; Levin, A.M.; Iannuzzi, M.C.; Rybicki, B.A.; Montgomery, C.G. Fine mapping of chromosome 15q25 implicates ZNF592 in neurosarcoidosis patients. Ann. Clin. Transl. Neurol. 2015, 2, 972–977. [Google Scholar] [CrossRef] [PubMed]
- Davoudi, S.; Navarro-Gomez, D.; Shen, L.; Ung, C.; Ren, A.; Sullivan, L.; Kwong, M.; Janessian, M.; Comander, J.; Gai, X.; et al. NOD2 genetic variants and sarcoidosis-associated uveitis. Am. J. Ophthalmol. Case Rep. 2016, 3, 39–42. [Google Scholar] [CrossRef] [PubMed]
- Levin, A.M.; Iannuzzi, M.C.; Montgomery, C.G.; Trudeau, S.; Datta, I.; Adrianto, I.; Chitale, D.A.; McKeigue, P.; Rybicki, B.A. Admixture fine-mapping in African Americans implicates XAF1 as a possible sarcoidosis risk gene. PLoS ONE 2014, 9, e92646. [Google Scholar] [CrossRef] [PubMed]
- Bello, G.A.; Adrianto, I.; Dumancas, G.G.; Levin, A.M.; Iannuzzi, M.C.; Rybicki, B.A.; Montgomery, C. Role of NOD2 Pathway Genes in Sarcoidosis Cases with Clinical Characteristics of Blau Syndrome. Am. J. Respir. Crit. Care Med. 2015, 192, 1133–1135. [Google Scholar] [CrossRef] [PubMed]
- Schürmann, M.; Reichel, P.; Müller-Myhsok, B.; Schlaak, M.; Müller-Quernheim, J.; Schwinger, E. Results from a genome-wide search for predisposing genes in sarcoidosis. Am. J. Respir. Crit. Care Med. 2001, 164, 840–846. [Google Scholar] [CrossRef] [PubMed]
- Iannuzzi, M.C.; Rybicki, B.A. Genetics of sarcoidosis: Candidate genes and genome scans. Proc. Am. Thorac. Soc. 2007, 4, 108–116. [Google Scholar] [CrossRef] [PubMed]
- Garman, L.; Montgomery, C.G.; Rivera, N.V. Recent advances in sarcoidosis genomics: Epigenetics, gene expression, and gene by environment (G×E) interaction studies. Curr. Opin. Pulm. Med. 2020, 26, 544–553. [Google Scholar] [CrossRef] [PubMed]
- Arbustini, E.; Narula, N.; Giuliani, L.; Di Toro, A. Genetic Basis of Myocarditis: Myth. or Reality? In Myocarditis; Published 7 March 2020; Springer: Cham, Switzerland, 2020; pp. 45–89. [Google Scholar] [CrossRef]
- Lota, A.S.; Hazebroek, M.R.; Theotokis, P.; Wassall, R.; Salmi, S.; Halliday, B.P.; Tayal, U.; Verdonschot, J.; Meena, D.; Owen, R.; et al. Genetic Architecture of Acute Myocarditis and the Overlap with Inherited Cardiomyopathy. Circulation 2022, 146, 1123–1134. [Google Scholar] [CrossRef] [PubMed]
- Korthals, D.; Bietenbeck, M.; Könemann, H.; Doldi, F.; Ventura, D.; Schäfers, M.; Mohr, M.; Wolfes, J.; Wegner, F.; Yilmaz, A.; et al. Cardiac Sarcoidosis-Diagnostic and Therapeutic Challenges. J. Clin. Med. 2024, 13, 1694. [Google Scholar] [CrossRef]
- Sohn, D.W.; Park, J.B. Cardiac sarcoidosis. Heart 2023, 109, 1132–1138. [Google Scholar] [CrossRef]
- Serei, V.D.; Fyfe, B. The Many Faces of Cardiac Sarcoidosis. Am. J. Clin. Pathol. 2020, 153, 294–302. [Google Scholar] [CrossRef] [PubMed]
- Takashige, N.; Naruse, T.K.; Matsumori, A.; Hara, M.; Nagai, S.; Morimoto, S.; Hiramitsu, S.; Sasayama, S.; Inoko, H. Genetic polymorphisms at the tumour necrosis factor loci (TNFA and TNFB) in cardiac sarcoidosis. Tissue Antigens 1999, 54, 191–193. [Google Scholar] [CrossRef]
- Fischer, A.; Rybicki, B.A. Granuloma genes in sarcoidosis: What is new? Curr. Opin. Pulm. Med. 2015, 21, 510–516. [Google Scholar] [CrossRef] [PubMed]
- Scheel, P.J., 3rd; Cartella, I.; Murray, B.; Gilotra, N.A.; Ammirati, E. Role of genetics in inflammatory cardiomyopathy. Int. J. Cardiol. 2024, 400, 131777. [Google Scholar] [CrossRef] [PubMed]
- Castrichini, M.; Agboola, K.M.; Vyas, H.; Abou Ezzeddine, O.F.; Siontis, K.C.; Giudicessi, J.R.; Rosenbaum, A.N.; Pereira, N.L. Cardiac Sarcoidosis Mimickers: Genetic Testing in Undifferentiated Inflammatory Cardiomyopathies. Circ. Genom. Precis. Med. 2023, 16, 478–479. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).