
Applying Patient Segmentation Using Primary Care Electronic Medical Records to Develop a Virtual Peer-to-Peer Intervention for Patients with Type 2 Diabetes

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Patient Segmentation and Characterization
2.3. Experiment
3. Results
3.1. Characterization of Patient Segments
3.2. Workshop Discussion and Survey
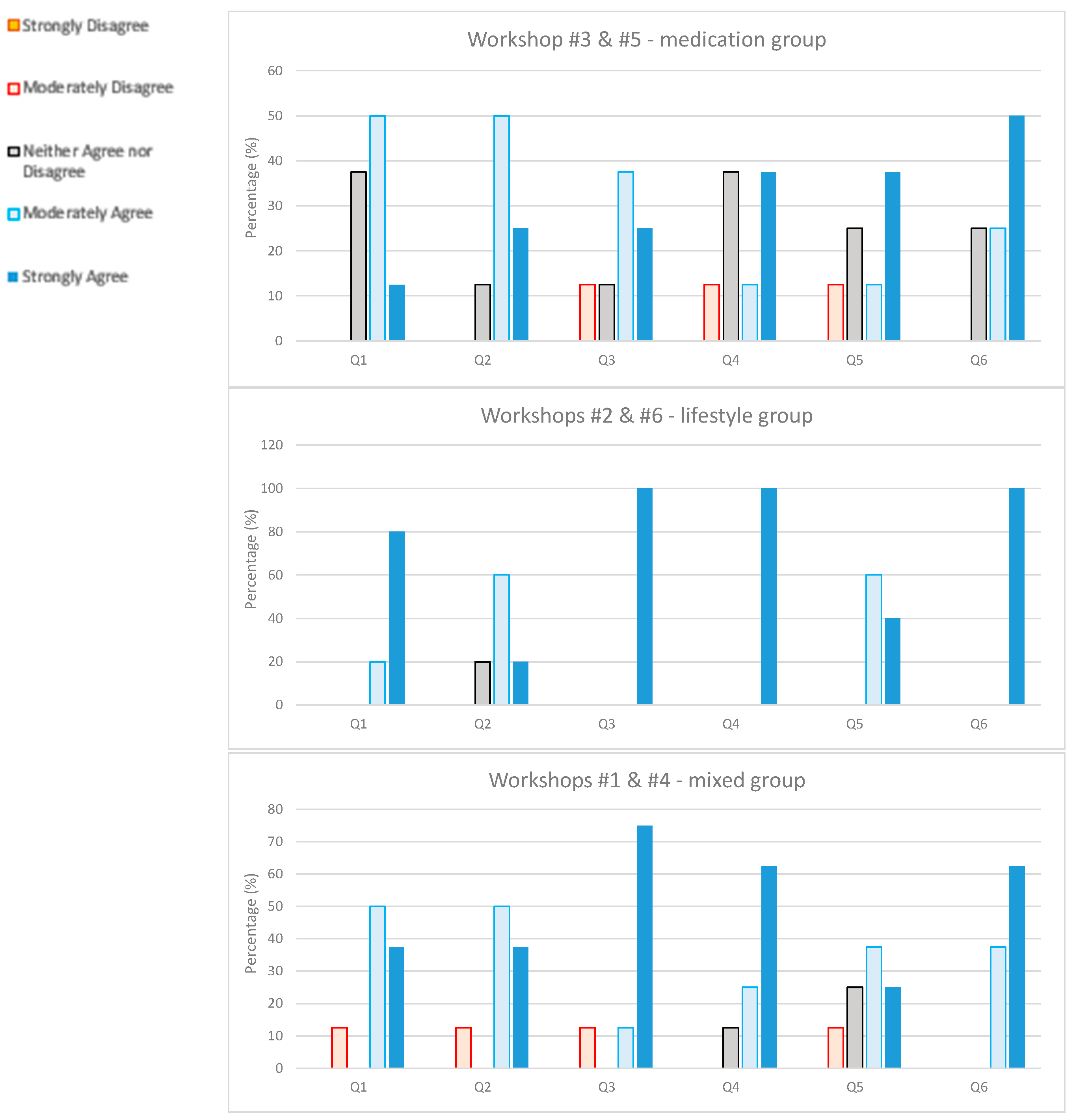
3.3. Post-Workshop Survey
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
- background, (e.g., family size, age, time in Canada, etc.) and
- current employment, hobbies, pass times, or other things you are interested at the moment.
- My Refresher Activity: … (Walkabout on first thoughts. List of words participants react to.) (5 min.) Elicit patient responses on key terms related to diabetes to get them warmed up to the workshop.Key words: 1. Diabetes, 2. Exercise, 3. Diet, 4. Nutrition, 5. Wellness
- Storytelling: …Everyone tells their story about their condition and actions. (40 min.)PROBE;
- How did you learn about their diabetes?
- What were your first thoughts and feelings?
- How did you handle your diabetes?
- What worked for you?
- What are your current goals?
- Discussion on Issues Identified: … Hot topics discussed from storytelling. (20 min.)
- What topics discussed were most meaningful to you?
- What were your thoughts and feelings about the topics?
- QUESTIONNAIRE. Provide questionnaire. We are trying to assess participant learning and engagement with individual assessment using an online survey via Microsoft Forms (see Workshop survey for specific questions). Please complete it now.
- Discussion of learnings from questionnaire (10 min)
- IDEA GENERATION: … Now, I would like you to help us understand how best to spread this type of “collective intelligence”. (20 min). You have learned more about how others handle diabetes, that information may help you in the future. Let’s discuss how we can spread this type of knowledge more widely.
- To do this we will have two brainstorming sessions where 2–3 of you can work together to generate different ideas on how to do this. It is important at this stage that we do not make judgements on these ideas during your session. We will have chance after the session to evaluate and prioritize these ideas. Facilitator asks the participants to form 2 small groups of 3 people each to conduct brainstorming and report back to the group. You will be given a link to a shared mural where you can write down your thoughts. The goal is to identify how average people can share their thoughts, insights, ideas and solutions on how they handle their diabetes. You will have ten minutes to come up with your 5 best ideas. Be creative! Start.
- After session; Sub-groups present on their ideas (while our research assistant will be sharing the murals on the screen)
- Problem Detection on best ideas: …Problem solve solutions. (10 min)
- Participants prioritize the most promising ideas
- Participants then put on their negative hats to identify barriers to implementing their ideas
- Identify Optimal Solution: …Build on optimal solution. (10 min)
- Participants brainstorm solutions to identified barriers
- Participants pick 1 or more solutions that seem the most promising
- Participants define criteria for ideal solutions
- Reality vs. Ideal: …Discussion on ideal vs. current situation. (10 min)
- Participants discuss feasibility of solutions and why some ideal solutions may not be implementable.
- Participants discuss likelihood of ideal solutions being implemented
- What is the 1 thing that we each learned that was most powerful and effective for us as a group? (10 min)
- Finally, are you comfortable at this point to share a goal that you’d like to achieve in the next 3 months? If you are comfortable, please share with us your goal and how you plan to achieve it. (5 min)Thank and Close.
Appendix B
- After this workshop I feel better about managing my condition
- I learned new information during the workshop
- The information and interactions during the workshop were useful to me
- I plan to act on the information I obtained in the workshop
- I believe I will achieve my goal within the next three months
- I am motivated to set a goal for improving my diabetes.
- Strongly Disagree
- Moderately Disagree
- Neither Agree nor Disagree
- Moderately Agree
- Strongly Agree
References
- Aziz, Z.; Riddell, M.A.; Absetz, P.; Brand, M.; Oldenburg, B. Peer support to improve diabetes care: An implementation evaluation of the Australasian Peers for Progress Diabetes Program. BMC Public Health 2018, 18, 262. [Google Scholar] [CrossRef] [PubMed]
- International Diabetes Federation (IDF) Diabetes Atlas 10th ed. Available online: https://diabetesatlas.org (accessed on 16 February 2023).
- Alyami, M.; Serlachius, A.; O’Donovan, C.E.; Werf, B.; Broadbent, E. A systematic review of illness perception interventions in type 2 diabetes: Effects on glycaemic control and illness perceptions. Diabet. Med. 2020, 38, e14495. [Google Scholar] [CrossRef] [PubMed]
- Dale, J.R.; Williams, S.M.; Bowyer, V. What is the effect of peer support on diabetes outcomes in adults? A systematic review. Diabet. Med. 2012, 29, 1361–1377. [Google Scholar] [CrossRef] [PubMed]
- Kong, L.; Hu, P.; Rn, Q.Z.; Yao, H.; Chen, S. Effect of peer support intervention on diabetes distress in people with type 2 diabetes: A systematic review and meta-analysis. Int. J. Nurs. Pract. 2020, 26, e12830. [Google Scholar] [CrossRef] [PubMed]
- Shita, N.G.; Iyasu, A.S. Glycemic control and its associated factors in type 2 diabetes patients at Felege Hiwot and Debre Markos Referral Hospitals. Sci. Rep. 2022, 12, 9459. [Google Scholar] [CrossRef] [PubMed]
- Paglialonga, A.; Theal, R.; Barber, D.; Kyba, R.; Guergachi, A.; Keshavjee, K. Behavioral Segmentation for Enhanced Peer-to-Peer Patient Education. Stud. Health Technol. Inform. 2022, 294, 125–126. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.J.; Park, C.; Sharp, L.K.; Quinn, L.; Bronas, U.G.; Gruss, V.; Fritschi, C. Impact of worries associated with COVID-19 on diabetes-related psychological symptoms in older adults with Type 2 diabetes. Geriatr. Nurs. 2022, 43, 58–63. [Google Scholar] [CrossRef]
- Harada, M.; Nishi, T.; Maeda, T.; Tanno, K.; Nishiya, N.; Arima, H. How do patients with chronic illnesses respond to a public health crisis? Evidence from diabetic patients in Japan during the COVID-19 pandemic. SSM—Popul. Health 2021, 16, 100961. [Google Scholar] [CrossRef]
- Smith, W.R. Product Differentiation and Market Segmentation as Alternative Marketing Strategies. J. Mark. 1956, 21, 3–8. [Google Scholar] [CrossRef]
- Chong, J.L.; Lim, K.K.; Matchar, D.B. Population segmentation based on healthcare needs: A systematic review. Syst. Rev. 2019, 8, 202. [Google Scholar] [CrossRef]
- Brommels, M. Patient Segmentation: Adjust the Production Logic to the Medical Knowledge Applied and the Patient’s Ability to Self-Manage—A Discussion Paper. Front. Public Health 2020, 8, 195. [Google Scholar] [CrossRef]
- Paglialonga, A.; Patel, A.A.; Pinto, E.; Mugambi, D.; Keshavjee, K. The Healthcare System Perspective in mHealth. In m_Health Current and Future Applications; Springer: Cham, Switzerland, 2019; pp. 127–142. [Google Scholar] [CrossRef]
- Golkhandan, E.; Paglialonga, A.; Guergachi, A.; Lussier, M.-T.; Richard, C.; Dube, L.; Zenlea, I.; Kyba, R.; Mittal, M.; Smokey Thomas, W.; et al. Design for a Virtual Peer-to-Peer Knowledge to Action Platform for Type 2 Diabetes. Stud. Health Technol. Inform. 2022, 294, 614–618. [Google Scholar] [CrossRef]
- Rose, A.J.; McCullough, M.B. A Practical Guide to Using the Positive Deviance Method in Health Services Research. Health Serv. Res. 2016, 52, 1207–1222. [Google Scholar] [CrossRef]
- Baxter, R.; Taylor, N.; Kellar, I.; Lawton, R. What methods are used to apply positive deviance within healthcare organisations? A systematic review. BMJ Qual. Saf. 2015, 25, 190–201. [Google Scholar] [CrossRef]
- Hendryx, M.; Guerra-Reyes, L.; Holland, B.D.; McGinnis, M.D.; Meanwell, E.; Middlestadt, S.E.; Yoder, K.M. A county-level cross-sectional analysis of positive deviance to assess multiple population health outcomes in Indiana. BMJ Open 2017, 7, e017370. [Google Scholar] [CrossRef]
- Standards of Medical Care in Diabetes—2011. Diabetes Care 2011, 34, S11–S61. [CrossRef]
- Paglialonga, A. Segment-Based Collective Intelligence for Population Health Improvement (SCI-PHI), Final Report. 31 July 2021; Unpublished Work. [Google Scholar]
- Cocosila, M.; Coursaris, C.; Yuan, Y. M-healthcare for patient self-management: A case for diabetics. Int. J. Electron. Health 2004, 1, 221–241. [Google Scholar] [CrossRef] [PubMed]
- Vuik, S.I. On the Application of Data-Driven Population Segmentation to Design Patient-Centred Integrated Care. Ph.D. Thesis, Imperial College London, London, UK. [CrossRef]
- A 360-Degree Approach to Patient Adherence. Available online: http://www.mckinsey.com/industries/pharmaceuticals-and-medical-products/our-insights/a-360-degree-approach-to-patient-adherence. (accessed on 16 February 2023).


{kind=link}
| Medication | Lifestyle | Whole Sample | |
|---|---|---|---|
| N. (%) of patients | 261 (31.6%) | 123 (14.9%) | 825 (100%) |
| % male | 48.3% | 49.6% | 48.8% |
| n. of comorbidities: mean (±s.d.) | 1.5 (±1.08) | 1.5 (±1.18) | 1.4 (±1.09) |
| Age: mean (±s.d.) | 68.7 (±11.62) | 69.0 (±12.95) | 68.6 (±11.69) |
| BMI: mean (±s.d.) | 31.8 (±6.88) | 31.6 (±6.62) | 31.8 (±7.18) |
| HbA1c: mean (±s.d.) | 7.2 (±1.41) | 7.5 (±1.54) | 7.2 (± 1.18) |
| LDL: mean (±s.d.) | 2.1 (±1.02) | 2.0 (±1.11) | 2.0 (±0.97) |
| sBP: mean (±s.d.) | 130.0 (±13.6) | 130.4 (±14.5) | 129.8 (±13.3) |
| dBP: mean (±s.d.) | 74.5 (±9.3) | 74.8 (±8.5) | 74.5 (±8.8) |
| Medication | Lifestyle | Mixed Group | |
| 1. Did you learn something new that you had not heard about before? | 1/8: Nothing at all 1/8: Maybe 2/8: A little 3/8: A few things 1/8: A lot | 0/7: Nothing at all 0/7: Maybe 1/7: A little 5/7: A few things 1/7: A lot | 0/9: Nothing at all 0/9: Maybe 3/9: A little 6/9: A few things 0/9: A lot |
| 2. Which topics were most interesting to you? | 2/8: Diet 3/8: Exercise 3/8: Stress management 1/8: Medications 3/8: Management of symptoms 3/8: Other (heart disease, how to keep people on track, mental health components of diabetes) | 5/7: Diet 6/7: Exercise 0/7: Stress management 0/7: Medications 3/7: Management of symptoms 1/7: Other (changing of mindset, motivation to change behavior) | 6/9: Diet 9/9: Exercise 2/9: Stress management 1/9: Medications 4/9: Management of symptoms |
| 3. Did you hear something you would like to try? | 1/8: Yes 3/8: No 4/8: I don’t know | 4/7: Yes 2/7: No 1/7: I don’t know | 5/9: Yes 2/9: No 2/9: I don’t know |
| 4. How do you feel about your condition, following this conversation? | 7/8: I feel better 0/8: I feel worse 1/8: I don’t know | 6/7: I feel better 0/7: I feel worse 1/7: I don’t know | 6/9: I feel better 1/9: I feel worse 2/9: I don’t know |
| 5. Would you recommend this workshop? | 4/8: Yes 3/8: No 1/8: Prefer not to say | 7/7: Yes 0/7: No 0/7: Prefer not to say | 8/9: Yes 0/9: No 1/9: Prefer not to say |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Paglialonga, A.; Theal, R.; Knox, B.; Kyba, R.; Barber, D.; Guergachi, A.; Keshavjee, K. Applying Patient Segmentation Using Primary Care Electronic Medical Records to Develop a Virtual Peer-to-Peer Intervention for Patients with Type 2 Diabetes. Future Internet 2023, 15, 149. https://doi.org/10.3390/fi15040149
Paglialonga A, Theal R, Knox B, Kyba R, Barber D, Guergachi A, Keshavjee K. Applying Patient Segmentation Using Primary Care Electronic Medical Records to Develop a Virtual Peer-to-Peer Intervention for Patients with Type 2 Diabetes. Future Internet. 2023; 15(4):149. https://doi.org/10.3390/fi15040149
Chicago/Turabian StylePaglialonga, Alessia, Rebecca Theal, Bruce Knox, Robert Kyba, David Barber, Aziz Guergachi, and Karim Keshavjee. 2023. "Applying Patient Segmentation Using Primary Care Electronic Medical Records to Develop a Virtual Peer-to-Peer Intervention for Patients with Type 2 Diabetes" Future Internet 15, no. 4: 149. https://doi.org/10.3390/fi15040149
APA StylePaglialonga, A., Theal, R., Knox, B., Kyba, R., Barber, D., Guergachi, A., & Keshavjee, K. (2023). Applying Patient Segmentation Using Primary Care Electronic Medical Records to Develop a Virtual Peer-to-Peer Intervention for Patients with Type 2 Diabetes. Future Internet, 15(4), 149. https://doi.org/10.3390/fi15040149