Encapsulated Cells Expressing a Chemotherapeutic Activating Enzyme Allow the Targeting of Subtoxic Chemotherapy and Are Safe and Efficacious: Data from Two Clinical Trials in Pancreatic Cancer

Abstract
:
1. Introduction
2. Results of Clinical Trials
2.1. Objectives of the Two Clinical Trials

{kind=link}
{kind=link}
{kind=link}
| Phase I/II Trial | Number of Patients |
| A. pancreatica dorsalis | −2 patients |
| A. pancreaticoduodenalis | −4 patients |
| Rami anterior of A. pancreaticoduodenalis + accessory branch + branch of A. pancreatico-dorsalis | −1 patient |
| Anterior pancreatic arcade | −2 patients |
| Posterior pancreatic arcade | −1 patient |
| A. pancreatico-duodenalis superior | −1 patient |
| Dorsal arcade of pancreatic head | −1 patient |
| A. gastroduodenalis inferior | −1 patient |
| Rami pancreatici of A. lienalis | −1 patient |
| Phase II Trial | Number of Patients |
| Anterior and posterior pancreatic arcade + tumor vessel which infiltrated the liver | −1 patient |
| A. pancreaticoduodenalis inferior and transversa accessoria | −1 patient |
| A. pancreaticoduodenalis inferior and A. pancreatica dorsalis | −1 patient |
| A. pancreatico duodenalis inferior | −1 patient |
| A. pancreaticoduodenalis superior | −1 patient |
| A. pancreaticoduodenalis superior ramus posterior + ramus ventralis, A gastroduodenalis | −1 patient |
| A. pancreaticoduodenalis caudal branches I and II + transversal branch | −1 patient |
| A. pancreatica dorsalis | −1 patient |
| A. mesenterica superior | −1 patient |
| A. gastroduodenalis | −2 patients |
| A. pancreatica transversalis | −2 patients |
| Center | Patients | ||||
|---|---|---|---|---|---|
| Screened | Enrolled | Treated | No. Capsules + | Ifosfamide Dose | |
| Rostock 1 | 51 | 17 | 14 | 300 * | 1 g/m2 |
| Rostock 2 | 8 | 7 | 7 | 221 | 2 g/m2 |
| Berlin 2 | 5 | 1 | 1 | 250 | 2 g/m2 |
| Munich 2 | 6 | 3 | 3 | 343 | 2 g/m2 |
| Berne 2 | 2 | 2 | 2 | 300 | 2 g/m2 |
| Total | 72 | 30 | 27 | Mean = 244 $ | |
2.2. Safety Parameters and Results
2.3. Serious Adverse Events
| Patient No. | Days After Instillation | Description |
|---|---|---|
| Death # | ||
| 2-1 | 96 | Liver metastases, death for unknown reason |
| 2-2 | 66 | Occult bleeding from eroded tumor vessel |
| 2-5 | 36 | Tumor progression |
| Other SAEs | ||
| 2-1 | 11 | Complete obstruction of duodenal passage by tumor |
| 22 | Bile duct obstruction by tumor | |
| 2-2 | 48 | Incomplete obstruction of duodenal passage by tumor |
| 2-3 | 71 | Elective hospitalization to change bile duct stent |
| 113 | Gastric outlet stenosis | |
| 2-5 | 3 | Somnolence in the context of an ifosfamide-induced encephalopathy |
| 2-6 | 5 | Stent occlusion |
| 14 | Duodenal stenosis | |
| 36 | Acute renal failure | |
| 2-10 | 52 | Incomplete obstruction of the bile duct by the tumor, with fever, leukocytosis, cholestasis |
| 2-12 | 111 | Peritoneal carcinomatosis in the context of a planned relaparotomy after marked improvement of the pancreatic tumor |
| 2-13 | 90 | Jaundice |
| 105 | Liver abscess | |
2.4. Tumor Reductions
| Patient | TNM | Stage | Metastases | Tumor | Survival Weeks $ | Notes |
|---|---|---|---|---|---|---|
| 1 | T4N1Mx | IV | n | SD | 102 | |
| 2 | T4N1Mx | IV | n | PR | 39 | |
| 3 | TN4xMx | IV | n | SD * | 64 | |
| 4 | T3NxM1 | IV | y | SD | 29 | |
| 5 | T3N1M1 | IV | y | SD * | 67 | |
| 6 | T4N1M1 | IV | y | SD | 20 | |
| 7 | T4N1M0 | IV | n | SD | 65 | |
| 8 | T4N1M1 | IV | y | PR | 28 | |
| 9 | T3NxMx | IV | n | SD | 44 | |
| 10 | T3N0M0 | III | n | SD | 33 | |
| 11 | T4N1M0 | IV | n | SD | 112 | |
| 12 | T4N1M1 | IV | y | SD | 6 | |
| 13 | T3N0M0 | III | y | SD | 35 | |
| 14 | T4N1Mx | IV | n | SD | 41 | |
| 2-1 | T4N1a/bM0 | IV | y | PD | 14 | |
| 2-2 | T4N1a/bM0 | IV | y | 9 | ||
| 2-3 | T4N1a/bM0 | IV | y | PD | 34 | |
| 2-4 | T4N1bM0 | IV | y | SD * | 47 # | Single infusion ^ |
| 2-5 | T4N1bM0 | IV | y | 5 | No 2nd ifosfamide cycle | |
| 2-6 | T4N1bM0 | IV | y | SD * | 67 # | Three cycles ^ |
| 2-7 | T4N1a/bM0 | IV | n | SD * | 114 + | Two cycles ^ |
| 2-8 | T4N1bM0 | IV | n | 57 # | Two cycles ^ | |
| 2-9 | T4N0M0 | IV | y | PD | 26 # | |
| 2-10 | T3N1M0 | III | y | 27 # | ||
| 2-11 | T4N0M0 | IV | y | SD | 20 @ | |
| 2-12 | T4NXM0 | IV | y | SD | 56 #,@ | |
| 2-13 | T4NXM0 | IV | n | PD | 26 |
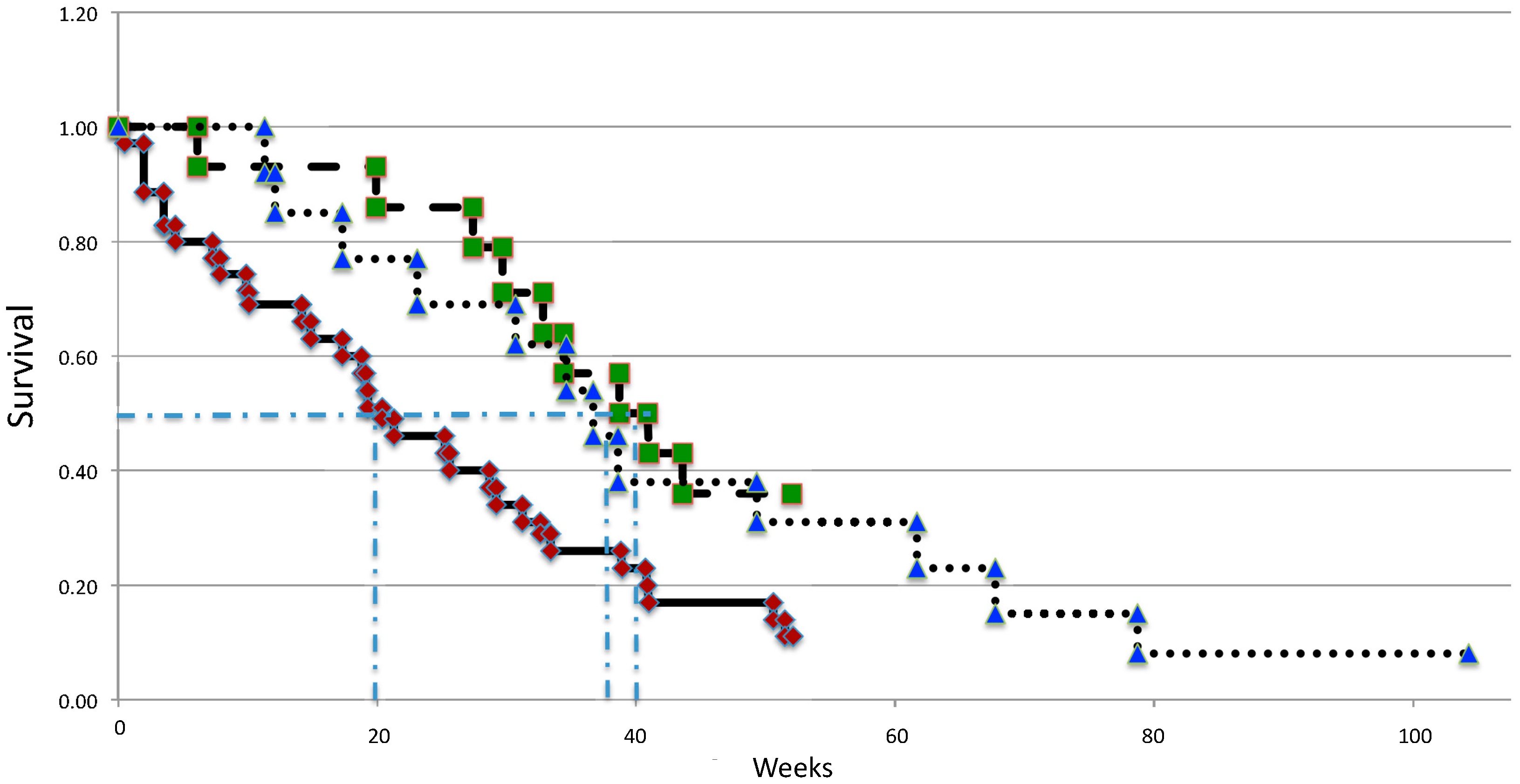
2.5. Median Survival
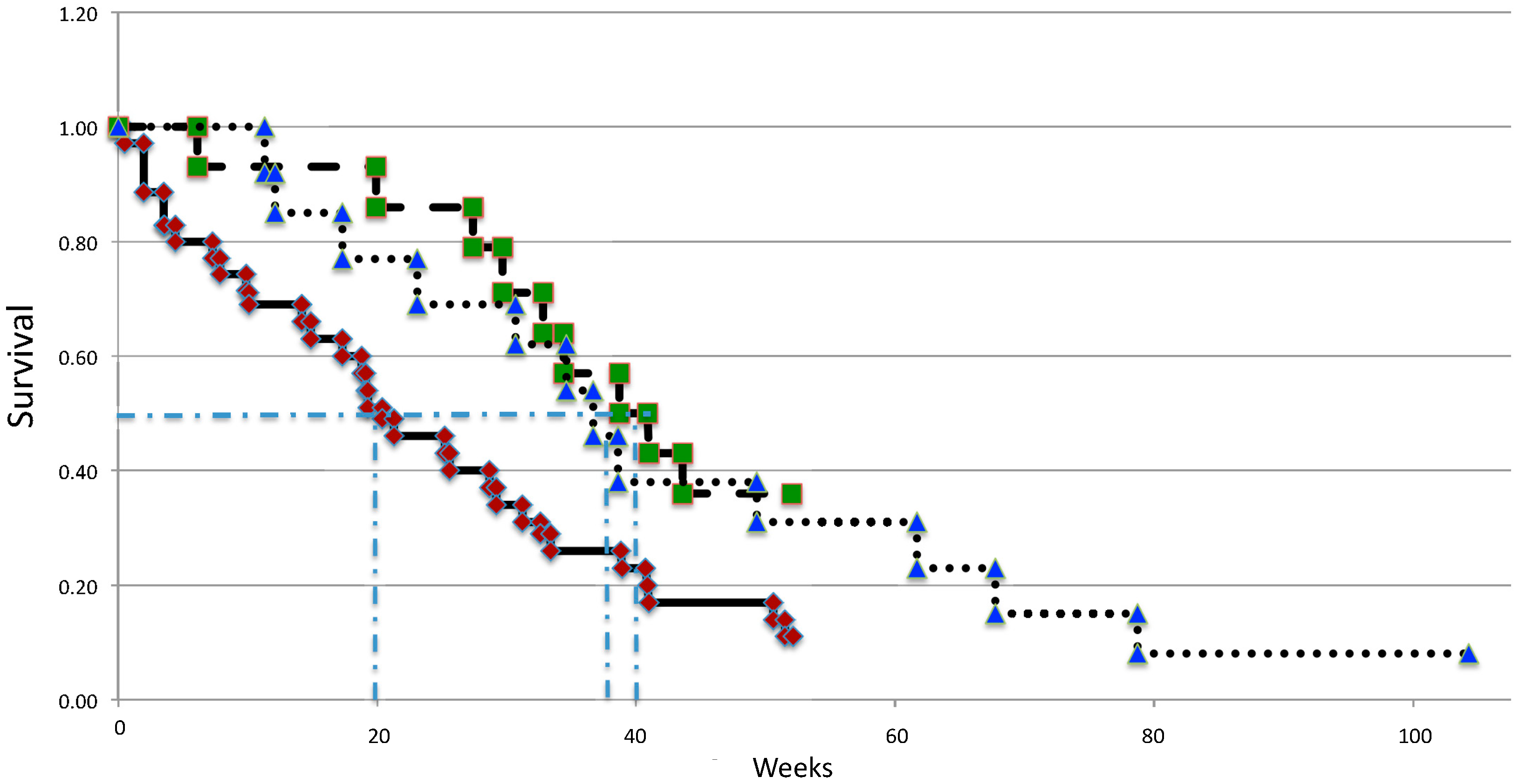
| Treatment | N | Phase | Median Survival | 1 Year Survival | Notes |
|---|---|---|---|---|---|
| Encapsulated cells | |||||
| +1 g/m2/day ifosfamide | 14 | 1/2 | 10 months | 36% | Single center |
| +2 g/m2/day ifosfamide | 13 | 2 | 9.5 months | 23% | Multiple centers |
| Control | 36 | n/a | 5 months | 11% | Historical data |
| Gemcitabine | 63 | 3 | 7 months # | 18% | Pivotal study |
2.6. Quality of Life
3. Discussion
| Treatment | Control | Phase | Median Survival | One-Year Survival | Side Effects | FDA Approval | ||
|---|---|---|---|---|---|---|---|---|
| Therapy | Control | Therapy | Control | |||||
| gemcitabine | 5-fluorouracil | 3 | 5.7 | 4.2 | 18% | 2% | more favorable than 5-fluorouracil | 1996 |
| gemcitabine + erlotinib hydrochloride (Tarceva) | gemcitabine | 3 | 6.4 | 6 | 24% | 19% | less favorable than gemcitabine | 2005 |
| gemcitabine + protein-bound paclitaxel (Abraxane) | gemcitabine | 3 | 8.5 | 6.7 | 35% | 22% | less favorable than gemcitabine | 2013 |
| FOLFIRINOX * | gemcitabine | 2/3 | 11.1 | 6.8 | 48.4 | 20.6 | less favorable than gemcitabine | n/a |
| cell encapsulation + ifosfamide | 5-fluorouracil | 2 | 10 | 5 | 36% | 18% | more favorable than 5-fluorouracil or gemcitabine # | n/a |
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Dabernat, S.; Lafitte, M.; Bedel, A.; de Verneuil, H.; Moreau-Gaudry, F. Gene therapy of pancreatic cancer. J. Genet. Syndr. Gene Ther. 2013, 4, 138. [Google Scholar]
- Amercian Cancer Society, Cancer Facts & Figures. 2013. Available online: http://www.cancer.org/acs/groups/content/@epidemiologysurveilance/documents/document/acspc-036845.pdf (accessed on 24 March 2014).
- Günzburg, W.H.; Löhr, M.; Salmons, B. Novel treatments and therapies in development for pancreatic cancer. Expert Opin. Investig. Drugs 2002, 11, 769–786. [Google Scholar] [CrossRef]
- Klein, A.P. Identifying people at a high risk of developing pancreatic cancer. Nat. Rev. Cancer 2013, 13, 66–74. [Google Scholar] [CrossRef]
- Vincent, A.; Herman, J.; Schulick, R.; Hruban, R.H.; Goggins, M. Pancreatic cancer. Lancet 2011, 378, 607–620. [Google Scholar] [CrossRef]
- Yachida, S.; Jones, S.; Bozic, I.; Antal, T.; Leary, R.; Fu, B.; Kamiyama, M.; Hruban, R.H.; Eshleman, J.R.; Nowak, M.A.; et al. Distant metastasis occurs late during the genetic evolution of pancreatic cancer. Nature 2010, 467, 1114–1117. [Google Scholar] [CrossRef]
- Campbell, P.J.; Yachida, S.; Mudie, L.J.; Stephens, P.J.; Pleasance, E.D.; Stebbings, L.A.; Morsberger, L.A.; Latimer, C.; McLaren, S.; Lin, M.L.; et al. The patterns and dynamics of genomic instability in metastatic pancreatic cancer. Nature 2010, 467, 1109–1113. [Google Scholar] [CrossRef]
- Salmons, B.; Brandtner, E.M.; Hettrich, K.; Wagenknecht, W.; Volkert, B.; Fischer, S.; Dangerfield, J.A.; Gunzburg, W.H. The use of encapsulated cells to focus the metabolic activation of anti-cancer drugs. Curr. Opin. Mol. Ther. 2010, 12, 450–460. [Google Scholar]
- Fillat, C.; Jose, A.; Bofill-De Ros, X.; Mato-Berciano, A.; Maliandi, M.V.; Sobrevals, L. Pancreatic cancer gene therapy: From molecular targets to delivery systems cancers. Cancers 2011, 3, 368–395. [Google Scholar] [CrossRef]
- Iovanna, J.; Mallmann, M.C.; Gonçalves, A.; Turrini, O.; Dagorn, J.C. Current knowledge on pancreatic cancer. Front. Oncol. 2012, 2, 6. [Google Scholar]
- Baxter Product Monograph. Available online: http://www.baxter.ca/en/downloads/product_information/IFEX_PM_APR052012_EN.pdf (accessed on 24 March 2014).
- Klastersky, J. Side effects of ifosfamide. Oncology 2003, 65, 7–10. [Google Scholar] [CrossRef]
- Cacheux, W.; Gourmel, B.; Alexandre, J.; Germann, N.; Rabillon, F.; Duffau, B.; Goldwasser, F. An original administration of ifosfamide given once every other week: A clinical and pharmacological study. Anticancer Drugs 2008, 19, 295–302. [Google Scholar] [CrossRef]
- Gad-El-Mawla, N.; Ziegler, J.L. Ifosfamide treatment of pancreatic cancer. Cancer Treat. Rep. 1981, 65, 357–358. [Google Scholar]
- Gad-El-Mawla, N. Ifosfamide in advanced pancreatic cancer. Cancer Chemother. Pharmacol. 1986, 18, 55–56. [Google Scholar] [CrossRef]
- Ajani, J.A.; Abbruzzese, J.L.; Goudeau, P.; Faintuch, J.S.; Yeomans, A.C.; Boman, B.M.; Nicaise, C.; Levin, B. Ifosfamide and mesna: Marginally active in patients with advanced carcinoma of the pancreas. J. Clin. Oncol. 1988, 6, 1703–1707. [Google Scholar]
- Wils, J.A.; Kok, T.; Wagener, D.J.; Francois, E.; Selleslags, J.; Duez, N. Phase II trial with ifosfamide in pancreatic cancer. Eur. J. Cancer 1993, 29A, 290. [Google Scholar]
- Keizer, H.J.; Ouwerkerk, J.; Welvaart, K.; van der Velde, C.J.; Cleton, F.J. Ifosfamide treatment as a 10-day continuous intravenous infusion. J. Cancer Res. Clin. Oncol. 1995, 121, 297–302. [Google Scholar]
- Cerny, T.; Martinelli, G.; Goldhirsch, A.; Terrier, F.; Joss, R.; Fey, M.F.; Brunner, K.W.; Kupfer, A. Continuous 5-day infusion of ifosfamide with mesna in inoperable pancreatic cancer patients: A phase II study. J. Cancer Res. Clin. Oncol. 1991, 117, S135–S138. [Google Scholar]
- Kurowski, V.; Wagner, T. Comparative pharmacokinetics of ifosfamide, 4-hydroxyifosfamide, chloroacetaldehyde, and 2- and 3-dechloroethylifosfamide in patients on fractionated intravenous ifosfamide therapy. Cancer Chemother. Pharmacol. 1993, 33, 36–42. [Google Scholar] [CrossRef]
- Dirven, H.A.; van Ommen, B.; van Bladeren, P.J. Glutathione conjugation of alkylating cytostatic drugs with a nitrogen mustard group and the role of glutathione S-transferases. Chem. Res. Toxicol. 1996, 9, 351–360. [Google Scholar] [CrossRef]
- Loehrer, P.J., Sr.; Williams, S.D.; Einhorn, L.H.; Ansari, R. Ifosfamide: An active drug in the treatment of adenocarcinoma of the pancreas. J. Clin. Oncol. 1985, 3, 367–372. [Google Scholar]
- Lokiec, F. Ifosfamide: Pharmacokinetic properties for central nervous system metastasis prevention. Ann. Oncol. 2006, 17, iv33–iv36. [Google Scholar] [CrossRef]
- Storme, T.; Deroussent, A.; Mercier, L.; Prost, E.; Re, M.; Munier, F.; Martens, T.; Bourget, P.; Vassal, G.; Royer, J.; et al. New ifosfamide analogs designed for lower associated neurotoxicity and nephrotoxicity with modified alkylating kinetics leading to enhanced in vitro anticancer activity. J. Pharmacol. Exp. Ther. 2009, 328, 598–609. [Google Scholar] [CrossRef]
- Newton, H.B. Neurological complications of chemotherapy to the central nervous system. Handb. Clin. Neurol. 2012, 105, 903–916. [Google Scholar] [CrossRef]
- Lewis, D.F.V. Guide to Cytochromes: Structure and Function; Taylor & Francis: London, UK, 1996; p. 109. [Google Scholar]
- Code, E.L.; Crespi, C.L.; Penman, B.W.; Gonzalez, F.J.; Chang, T.K.; Waxman, D.J. Human cytochrome P4502B6: Interindividual hepatic expression, substrate specificity, and role in procarcinogen activation. Drug Metab. Dispos. 1997, 25, 985–993. [Google Scholar]
- Löhr, M.; Müller, P.; Karle, P.; Stange, J.; Mitzner, S.; Jesnowski, R.; Nizze, H.; Nebe, B.; Liebe, S.; Salmons, B.; et al. Targeted chemotherapy by intratumour injection of encapsulated cells engineered to produce CYP2B1, an ifosfamide activating cytochrome P450. Gene Ther. 1998, 5, 1070–1078. [Google Scholar]
- Chen, L.; Waxman, D.J. Intratumoral activation and enhanced chemotherapeutic effect of oxazaphoshorines following cytochrome P450 gene transfer: Development of a combined chemotherapy/cancer gene therapy strategy. Cancer Res. 1995, 581–589. [Google Scholar]
- Chen, L.; Waxman, D.J.; Chen, D.; Kufe, D.W. Sensitization of human breast cancer cells to cyclophosphamide and ifosfamide by transfer of a liver cytochrome P450 gene. Cancer Res. 1996, 56, 1331–1340. [Google Scholar]
- Karle, P.; Müller, P.; Renz, R.; Jesnowski, R.; Saller, R.M.; von Rombs, K.; Nizze, H.; Liebe, S.; Günzburg, W.H.; Salmons, B.; et al. Intratumour injection of encapsulated cells producing an ifosfamide activating cytochrome P450 for targeted chemotherapy. Adv. Exp. Med. Biol. 1998, 451, 97–106. [Google Scholar] [CrossRef]
- Günzburg, W.H.; Karle, P.; Renz, R.; Salmons, B.; Renner, M. Characterisation of a human cell clone expressing cytochrome P450 for safe use in human somatic cell therapy. Annu. N. Y. Acad. Sci. 1999, 880, 326–336. [Google Scholar]
- Dautzenberg, H.; Schuldt, U.; Grasnick, G.; Karle, P.; Müller, P.; Löhr, M.; Pelegrin, M.; Piechaczyk, M.; von Rombs, K.; Günzburg, W.H.; et al. Development of cellulose sulphate based polyelectrolyte complex microcapsules for medical applications. Annu. N. Y. Acad. Sci. 1999, 875, 46–63. [Google Scholar] [CrossRef]
- Kroger, J.-C.; Muller, P.; Jesnowski, R.; Karle, P.; Renz, R.; Saller, R.; Stein, H.; Puschel, K.; von Rombs, K.; Nizze, H.; et al. Injection of encapsulated cells producing an ifosfamide-activating cytochrome P450 for targeted chemotherapy to pancreatic tumors. Ann. N. Y. Acad. Sci. 1999, 880, 337–351. [Google Scholar] [CrossRef]
- Kröger, J.-C.; Benz, S.; Hoffmeyer, A.; Bago, Z.; Bergmeister, H.; Günzburg, W.H.; Karle, P.; Klöppel, G.; Losert, U.; Müller, P.; et al. Intra-arterial instillation of microencapsulated, ifosfamide activating cells in the pig pancreas for chemotherapeutic targeting. Pancreatology 2003, 3, 55–63. [Google Scholar] [CrossRef]
- Löhr, J.M.; Bago, Z.T.; Bergmeister, H.; Ceijka, M.; Freund, M.; Gelbmann, W.; Günzburg, W.H.; Hain, J.; Hauenstein, K.; Henniger, W.; et al. Cell therapy using microencapsulated 293 cells transfected with a gene construct expressing CYP2B1, an ifosfamide converting enzyme, instilled intra-arterially in patients with advanced stage pancreatic carcinoma: Phase I/II study. J. Mol. Med. 1999, 77, 393–398. [Google Scholar] [CrossRef]
- Löhr, J.M.; Hoffmeyer, A.; Kröger, J.-C.; Freund, M.; Hain, J.; Holle, A.; Karle, P.; Knöfel, W.T.; Liebe, S.; Müller, P.; et al. Microencapsulated cell mediated therapy of inoperable pancreatic carcinoma. Lancet 2001, 357, 1591–1592. [Google Scholar] [CrossRef]
- Löhr, J.M.; Kröger, J.-C.; Hoffmeyer, A.; Freund, M.; Hain, J.; Holle, A.; Knöfel, W.T.; Liebe, S.; Nizze, H.; Renner, M.; et al. Safety, feasibility and clinical benefit of localized chemotherapy using microencapsulated cells for inoperable pancreatic carcinoma in a phase I/II trial. Cancer Ther. 2003, 1, 121–131. [Google Scholar]
- Salmons, B.; Löhr, M.; Günzburg, W.H. Treatment of inoperable pancreatic carcinoma using a cell based local chemotherapy: Results of a phase I/II clinical trial. J. Gastroenterol. 2003, 38, 78–84. [Google Scholar]
- Cereda, S.; Reni, M.; Rognone, A.; Fugazza, C.; Ghidini, M.; Ceraulo, D.; Brioschi, M.; Nicoletti, R.; Villa, E. Salvage therapy with mitomycin and ifosfamide in patients with gemcitabine-resistant metastatic pancreatic cancer: A phase II trial. Chemotherapy 2011, 57, 156–161. [Google Scholar] [CrossRef]
- Sultana, A.; Smith, C.T.; Cunningham, D.; Starling, N.; Neoptolemos, J.P.; Ghaneh, P. Meta-analyses of chemotherapy for locally advanced and metastatic pancreatic cancer. J. Clin. Oncol. 2007, 25, 2607–2615. [Google Scholar] [CrossRef]
- Bloechle, C.; Izbicki, J.R.; Knoefel, W.T.; Kuechler, T.; Broelsch, C.E. Quality of life in chronic pancreatitis—Results after duodenum-preserving resection of the head of the pancreas. Pancreas 1995, 11, 77–85. [Google Scholar] [CrossRef]
- Fayers, P.; Aaronson, N.; Bjordal, K.; Curran, D.; Groenveld, M.; On behalf of the EORTC Quality of Life Study Group. EORTC QLQ-C30 Scoring Manual, 2nd ed.; EORTC Monograph: Brussels, Belgium, 1999. [Google Scholar]
- Ghiringhelli, F.; Apetoh, L. The interplay between the immune system and chemotherapy: Emerging methods for optimizing therapy. Expert Rev. Clin. Immunol. 2014, 10, 19–30. [Google Scholar] [CrossRef]
- Salmons, B.; Hauser, O.; Gunzburg, W.H.; Tabotta, W. GMP production of an encapsulated cell therapy product: Issues and considerations. BioProcess. J. 2007, 4, 36–43. [Google Scholar]
- Dangerfield, J.A.; Salmons, B.; Corteling, R.; Abastado, J.-P.; Sinden, J.; Gunzburg, W.H.; Brandtner, E.M. The diversity of cellulose sulphate encapsulation. In Bioencapsulation of Living Cells for Diverse Medical Applications; Dangerfield, J., Brandtner, E.M., Eds.; Bentham E-Book: Oak Park, IL, USA, 2013; pp. 70–92. [Google Scholar]
- Karle, P.; Renner, M.; Salmons, B.; Günzburg, W.H. Necrotic, rather than apoptotic, cell death caused by cytochrome P450 activated ifosfamide. Cancer Gene Ther. 2001, 8, 220–230. [Google Scholar] [CrossRef]
- Vanden Berghe, T.; Grootjans, S.; Goossens, V.; Dondelinger, Y.; Krysko, D.V.; Takahashi, N.; Vandenabeele, P. Determination of apoptotic and necrotic cell death in vitro and in vivo. Methods 2013, 61, 117–129. [Google Scholar] [CrossRef]
- Buckwalter, M.R.; Srivastava, P.K. Mechanism of dichotomy between CD8+ responses elicited by apoptotic and necrotic cells. Cancer Immun. 2013, 13, 2. [Google Scholar]
- Penel, N.; Adenis, A.; Bocci, G. Cyclophosphamide-based metronomic chemotherapy: After 10 years of experience, where do we stand and where are we going? Crit. Rev. Oncol. Hematol. 2012, 82, 40–50. [Google Scholar] [CrossRef]
- Winiarczyk, S.; Gradski, Z.; Kosztolich, B.; König, G.; Günzburg, W.H.; Salmons, B.; Hain, J. A clinical protocol for treatment of canine mammary tumors using encapsulated, cytochrome P450 synthesizing cells activating cyclophosphamide: A phase I/II study. J. Mol. Med. 2002, 80, 610–614. [Google Scholar] [CrossRef]
- Wojciechowski, M.; Winiarczyk, S.; Adaszek, L.; Grądzki, Z.; Salmons, B.; Gunzburg, W.H. Phase I/II clinical trial of encapsulated, cytochrome P450 expressing cells as local activators of cyclophosphamide for the treatment of spontaneous canine mammary tumours. PLoS One 2014, 9, e102061. [Google Scholar]
- Conroy, T.; Desseigne, F.; Ychou, M.; Bouché, O.; Guimbaud, R.; Bécouarn, Y.; Adenis, A.; Raoul, J.-L.; Gourgou-Bourgade, S.; de la Fouchardière, C.; et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N. Engl. J. Med. 2001, 364, 1817–1825. [Google Scholar]
- Von Hoff, D.D.; Ervin, T.; Arena, F.P.; Gabriela Chiorean, E.; Infante, J.; Moore, M.; Seay, T.; Tjulandin, S.A.; Ma, W.W.; Saleh, M.N.; et al. Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine. N. Engl. J. Med. 2013, 369, 1691–1703. [Google Scholar] [CrossRef]
- Salmons, B.; Gunzburg, W.H. Therapeutic application of cell microencapsulation in cancer. Adv. Exp. Med. Biol. 2010, 670, 92–103. [Google Scholar] [CrossRef]
- Herreros-Villanueva, M.; Bujanda, L.; Billadeau, D.D.; Zhang, J.S. Embryonic stem cell factors and pancreatic cancer. World J. Gastroenterol. 2014, 20, 2247–2254. [Google Scholar] [CrossRef]
- Fitzgerald, T.L.; McCubrey, J.A. Pancreatic cancer stem cells: Association with cell surface markers, prognosis, resistance, metastasis and treatment. Adv. Biol. Regul. 2014. [Google Scholar] [CrossRef]
- Kim, S.K.; Kim, H.; Lee, D.H.; Kim, T.S.; Kim, T.; Chung, C.; Koh, G.Y.; Kim, H.; Lim, D.S. Reversing the intractable nature of pancreatic cancer by selectively targeting ALDH-high, therapy-resistant cancer cells. PLoS One 2013, 8, e78130. [Google Scholar]
- Duong, H.Q.; Yi, Y.W.; Kang, H.J.; Bae, I.; Jang, Y.J.; Kwak, S.J.; Seong, Y.S. Combination of dasatinib and gemcitabine reduces the ALDH1A1 expression and the proliferation of gemcitabine-resistant pancreatic cancer MIA PaCa-2 cells. Int. J. Oncol. 2014, 44, 2132–2138. [Google Scholar]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Löhr, J.M.; Haas, S.L.; Kröger, J.C.; Friess, H.M.; Höft, R.; Goretzki, P.E.; Peschel, C.; Schweigert, M.; Salmons, B.; Gunzburg, W.H. Encapsulated Cells Expressing a Chemotherapeutic Activating Enzyme Allow the Targeting of Subtoxic Chemotherapy and Are Safe and Efficacious: Data from Two Clinical Trials in Pancreatic Cancer. Pharmaceutics 2014, 6, 447-466. https://doi.org/10.3390/pharmaceutics6030447
Löhr JM, Haas SL, Kröger JC, Friess HM, Höft R, Goretzki PE, Peschel C, Schweigert M, Salmons B, Gunzburg WH. Encapsulated Cells Expressing a Chemotherapeutic Activating Enzyme Allow the Targeting of Subtoxic Chemotherapy and Are Safe and Efficacious: Data from Two Clinical Trials in Pancreatic Cancer. Pharmaceutics. 2014; 6(3):447-466. https://doi.org/10.3390/pharmaceutics6030447
Chicago/Turabian StyleLöhr, J. Matthias, Stephan L. Haas, Jens C. Kröger, Helmut M. Friess, Raimund Höft, Peter E. Goretzki, Christian Peschel, Markus Schweigert, Brian Salmons, and Walter H. Gunzburg. 2014. "Encapsulated Cells Expressing a Chemotherapeutic Activating Enzyme Allow the Targeting of Subtoxic Chemotherapy and Are Safe and Efficacious: Data from Two Clinical Trials in Pancreatic Cancer" Pharmaceutics 6, no. 3: 447-466. https://doi.org/10.3390/pharmaceutics6030447
APA StyleLöhr, J. M., Haas, S. L., Kröger, J. C., Friess, H. M., Höft, R., Goretzki, P. E., Peschel, C., Schweigert, M., Salmons, B., & Gunzburg, W. H. (2014). Encapsulated Cells Expressing a Chemotherapeutic Activating Enzyme Allow the Targeting of Subtoxic Chemotherapy and Are Safe and Efficacious: Data from Two Clinical Trials in Pancreatic Cancer. Pharmaceutics, 6(3), 447-466. https://doi.org/10.3390/pharmaceutics6030447