
Hydrogel Containing Biogenic Silver Nanoparticles and Origanum vulgare Essential Oil for Burn Wounds: Antimicrobial Efficacy Using Ex Vivo and In Vivo Methods Against Multidrug-Resistant Microorganisms

 , , , , , ,
, , , , , ,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Bacterial Isolates
2.2. Antimicrobial Sensitivity Profile
2.3. Antimicrobial Compounds
2.4. In Vitro Analysis of the Antibacterial Activity of OEO and Bio-AgNP
2.5. Antimicrobial Combination Assay
2.6. Hydrogel Development
2.7. Pharmacotechnical Characterization of Hydrogels
2.7.1. Pre-Stability Test
2.7.2. Organoleptic Characterization
2.7.3. Physical–Chemical Evaluation
- M0: mass of the empty pycnometer;
- M1: mass of the pycnometer with the sample diluted in purified water;
- M2: mass of the pycnometer with pure water.
2.7.4. Spreadability
- Ei: spreadability of the sample for a given weight i (mm2);
- d: average diameter (mm).
2.7.5. Preliminary Stability Test
2.8. Evaluation of In Vitro Antimicrobial Activity
2.9. Evaluation of Antimicrobial Activity in an Ex Vivo Model
2.9.1. Preparation of the Porcine Skin
2.9.2. Treatment with Antimicrobial Formulation on Porcine Skin
2.9.3. Viable Cell Count
2.10. Evaluation of Antimicrobial Activity in an In Vivo Model
2.10.1. Management of Larvae
2.10.2. Antimicrobial Assessment
2.11. Statistical Analysis
3. Results
3.1. Antimicrobial Sensitivity Profile
3.2. Antimicrobial Combination Test
3.3. Development of Hydrogels
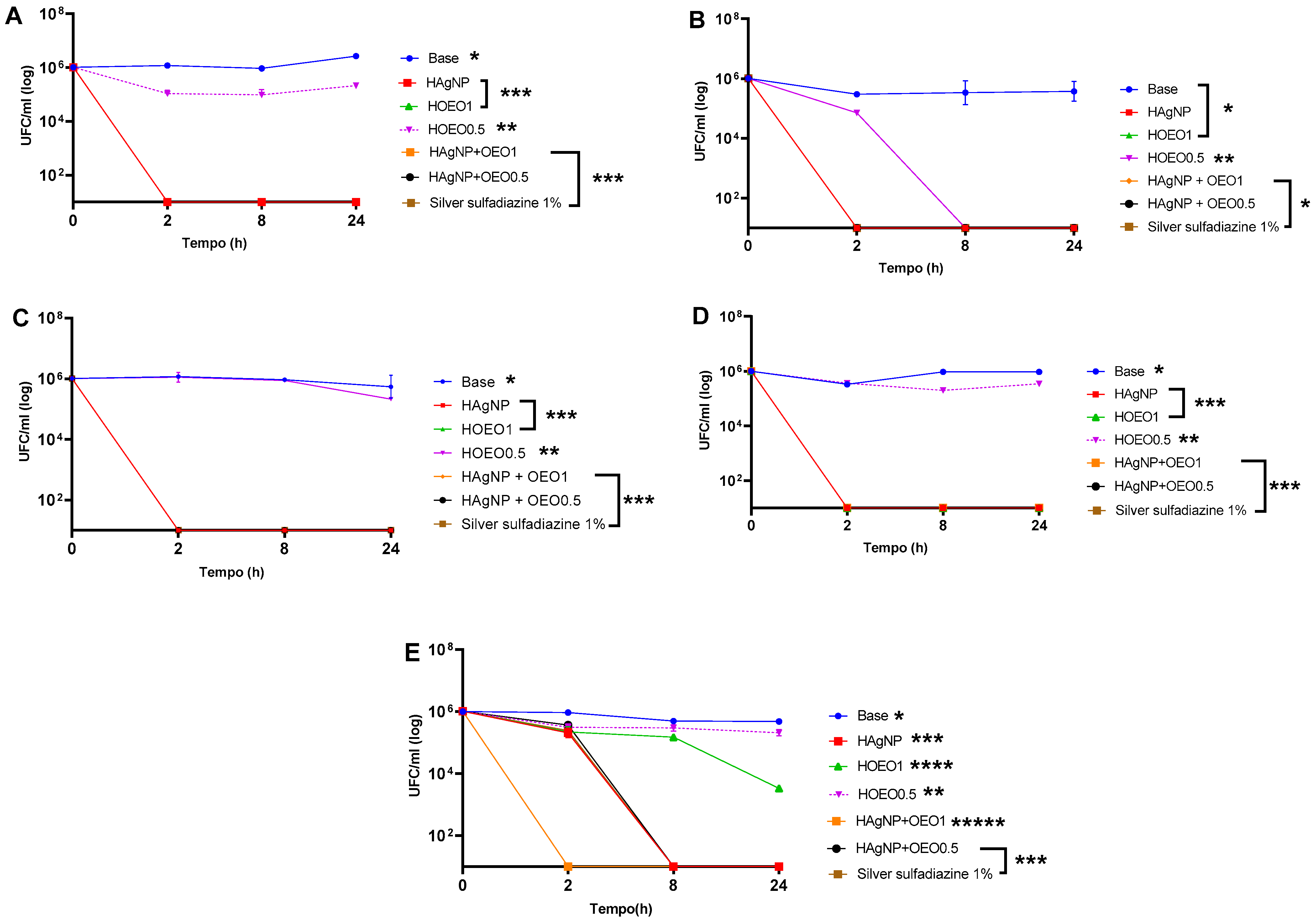
3.4. Evaluation of Antimicrobial Activity In Vitro
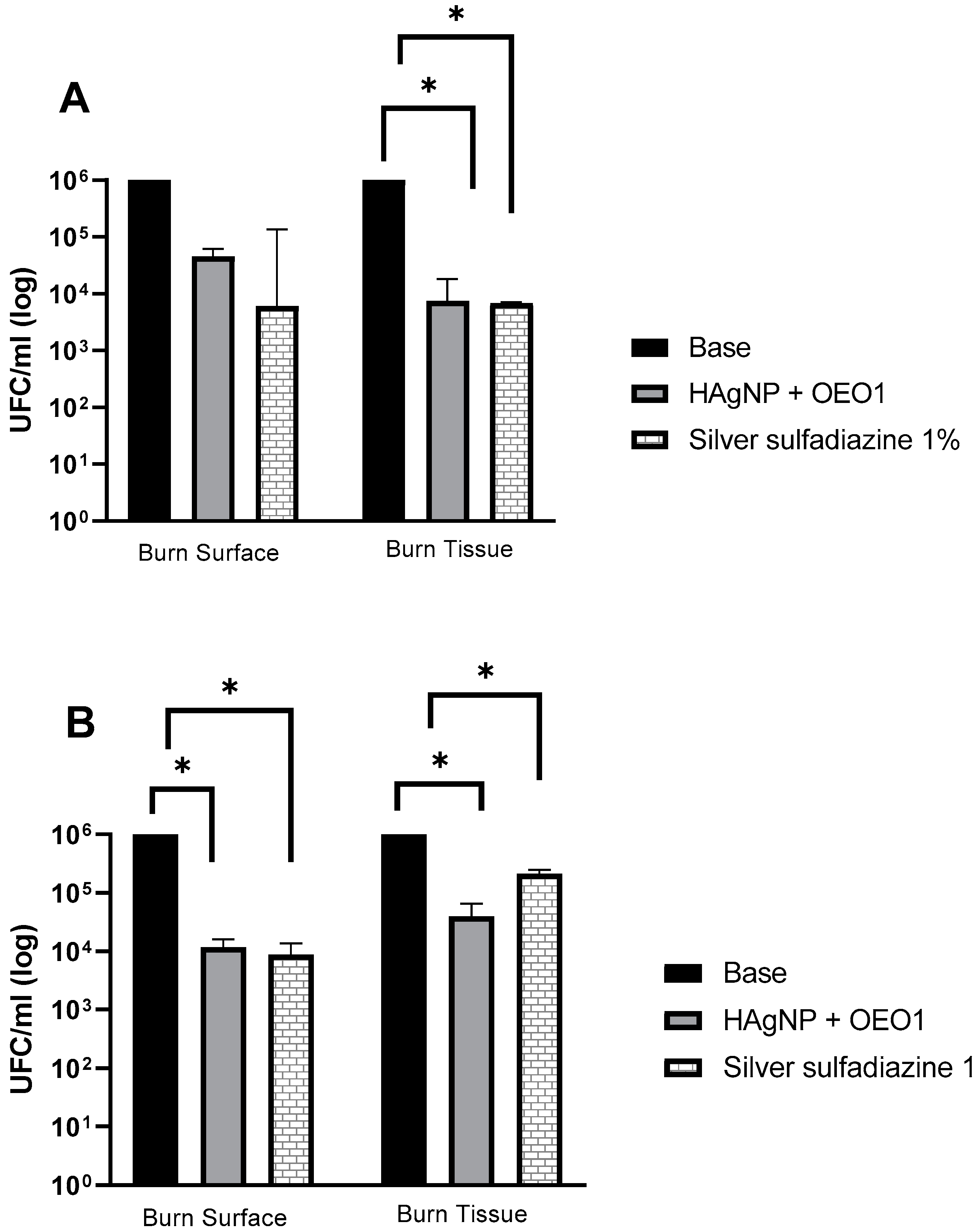
3.5. Ex Vivo Model Analysis
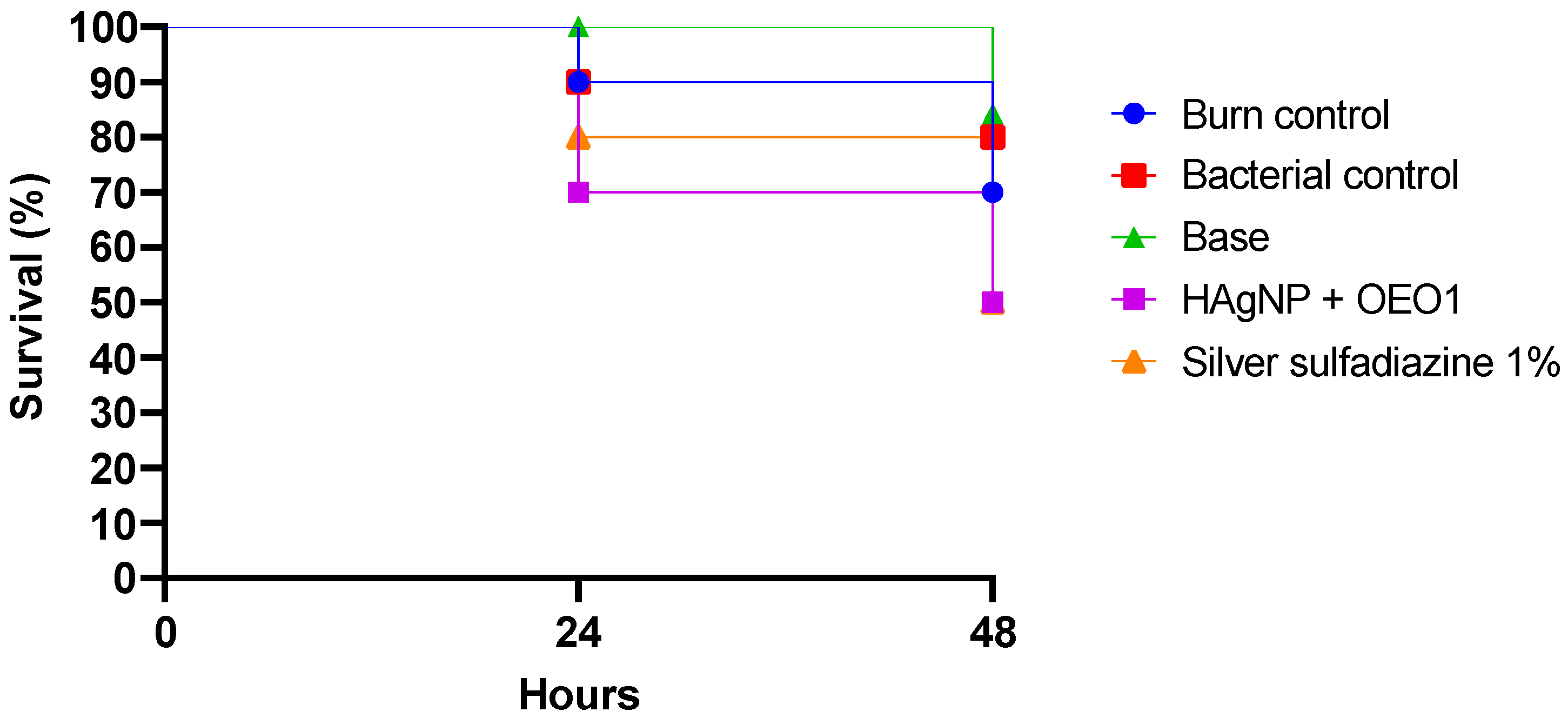
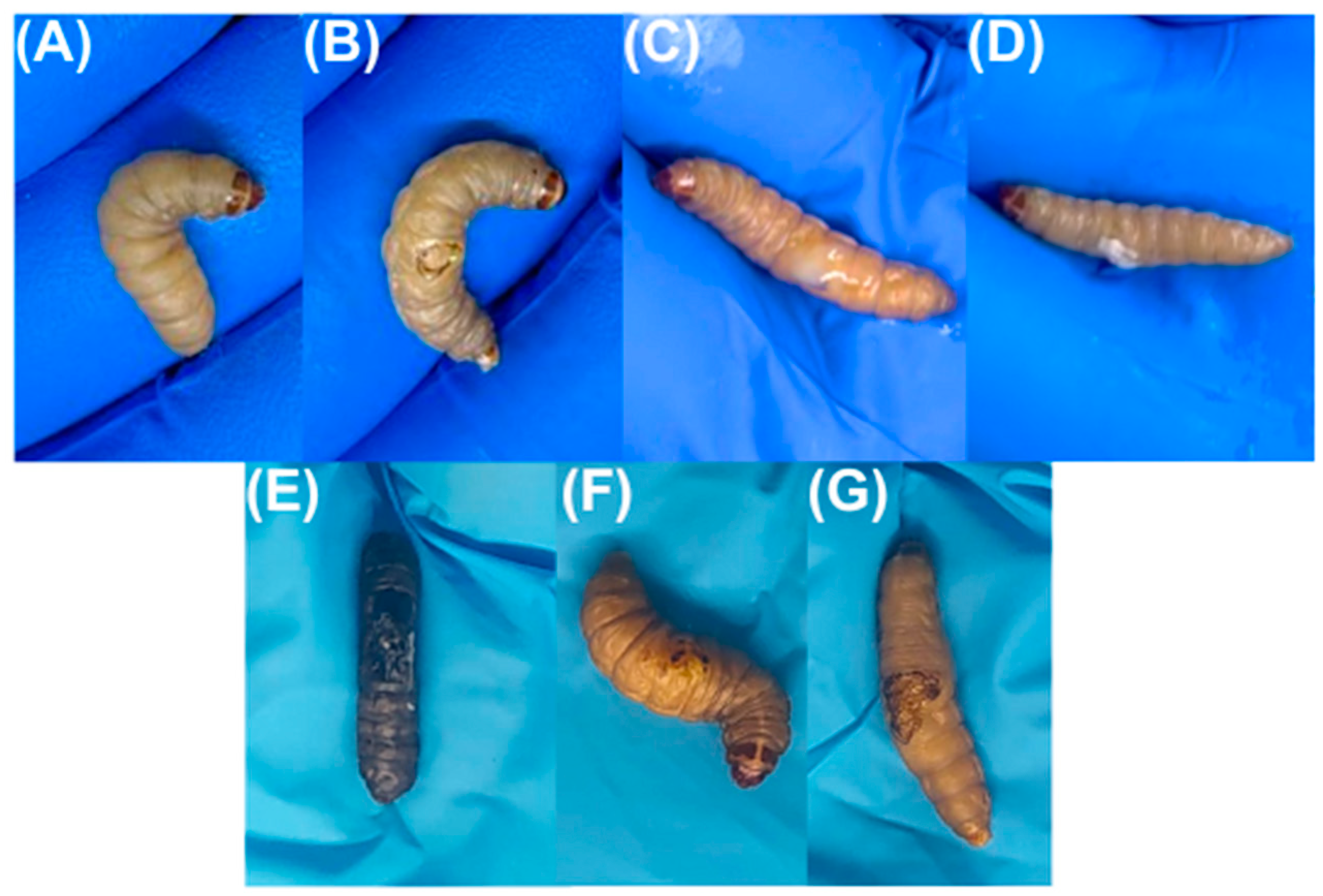
3.6. In Vivo Model Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dyring-Andersen, B.; Løvendorf, M.B.; Coscia, F.; Santos, A.; Møller, L.B.P.; Colaço, A.R.; Niu, L.; Bzorek, M.; Doll, S.; Andersen, J.L.; et al. Spatially and Cell-Type Resolved Quantitative Proteomic Atlas of Healthy Human Skin. Nat. Commun. 2020, 11, 5587. [Google Scholar] [CrossRef]
- Duim, E.; De Sá, F.H.C.; De Oliveira Duarte, Y.A.; De Oliveira, R.D.C.B.; Lebrão, M.L. Prevalência e Características Das Feridas Em Pessoas Idosas Residentes Na Comunidade. Rev. Esc. Enferm. USP 2015, 49, 51–57. [Google Scholar] [CrossRef]
- Chambers, E.S.; Vukmanovic-Stejic, M. Skin Barrier Immunity and Ageing. Immunology 2020, 160, 116. [Google Scholar] [CrossRef]
- Grice, E.A.; Segre, J.A. The Skin Microbiome. Nat. Rev. Microbiol. 2011, 9, 244–253. [Google Scholar] [CrossRef]
- Harris-Tryon, T.A.; Grice, E.A. Microbiota and Maintenance of Skin Barrier Function. Science 2022, 376, 940–945. [Google Scholar] [CrossRef]
- Oryan, A.; Alemzadeh, E.; Moshiri, A. Burn Wound Healing: Present Concepts, Treatment Strategies and Future Directions. J. Wound Care 2017, 26, 5–19. [Google Scholar] [CrossRef]
- Brasil, Ministério da Saúde, Secretaria de Vigilância em Saúde. Boletim Epidemiológico 2022, 53, 47. Available online: https://www.gov.br/saude/pt-br/centrais-de-conteudo/publicacoes/boletins/epidemiologicos/edicoes/2022/boletim-epidemiologico-vol-53-no47/view (accessed on 11 March 2024).
- OMS Global Burn Registry. Available online: https://www.who.int/teams/social-determinants-of-health/safety-and-mobility/burns/global-burn-registry (accessed on 11 March 2024).
- Jeschke, M.G.; van Baar, M.E.; Choudhry, M.A.; Chung, K.K.; Gibran, N.S.; Logsetty, S. Burn Injury. Nat. Rev. Dis. Primers 2020, 6, 11. [Google Scholar] [CrossRef]
- Orbay, H.; Ziembicki, J.A.; Yassin, M.; Egro, F.M. Prevention and Management of Wound Infections in Burn Patients. Clin. Plast. Surg. 2024, 51, 255–265. [Google Scholar] [CrossRef]
- Żwierełło, W.; Piorun, K.; Skórka-Majewicz, M.; Maruszewska, A.; Antoniewski, J.; Gutowska, I. Burns: Classification, Pathophysiology, and Treatment: A Review. Int. J. Mol. Sci. 2023, 24, 3749. [Google Scholar] [CrossRef]
- Yang, Y.; Qu, L.; Mijakovic, I.; Wei, Y. Advances in the Human Skin Microbiota and Its Roles in Cutaneous Diseases. Microb. Cell Fact. 2022, 21, 176. [Google Scholar] [CrossRef]
- Lachiewicz, A.M.; Hauck, C.G.; Weber, D.J.; Cairns, B.A.; van Duin, D. Bacterial Infections After Burn Injuries: Impact of Multidrug Resistance. Clin. Infect. Dis. 2017, 65, 2130–2136. [Google Scholar] [CrossRef]
- Ladhani, H.A.; Yowler, C.J.; Claridge, J.A. Burn Wound Colonization, Infection, and Sepsis. Surg. Infect. 2021, 22, 44–48. [Google Scholar] [CrossRef]
- Cartotto, R. Topical Antimicrobial Agents for Pediatric Burns. Burn. Trauma 2017, 5, 33. [Google Scholar] [CrossRef]
- Tsolakidis, S.; Freytag, D.L.; Dovern, E.; Alharbi, Z.; Kim, B.-S.; Houschyar, K.S.; Reumuth, G.; Schäfer, B.; Rennekampff, H.-O.; Pallua, N.; et al. Infections in Burn Patients: A Retrospective View over Seven Years. Medicina 2022, 58, 1066. [Google Scholar] [CrossRef]
- Markiewicz-Gospodarek, A.; Kozioł, M.; Tobiasz, M.; Baj, J.; Radzikowska-Büchner, E.; Przekora, A. Burn Wound Healing: Clinical Complications, Medical Care, Treatment, and Dressing Types: The Current State of Knowledge for Clinical Practice. Int. J. Environ. Res. Public Health 2022, 19, 1338. [Google Scholar] [CrossRef]
- Gupta, M.; Naik, A.K.; Singh, S.K. Bacteriological Profile and Antimicrobial Resistance Patterns of Burn Wound Infections in a Tertiary Care Hospital. Heliyon 2019, 5, e02956. [Google Scholar] [CrossRef]
- Haider, M.H.; McHugh, T.D.; Roulston, K.; Arruda, L.B.; Sadouki, Z.; Riaz, S. Detection of Carbapenemases BlaOXA48-BlaKPC-BlaNDM-BlaVIM and Extended-Spectrum-β-Lactamase BlaOXA1-BlaSHV-BlaTEM Genes in Gram-Negative Bacterial Isolates from ICU Burns Patients. Ann. Clin. Microbiol. Antimicrob. 2022, 21, 18. [Google Scholar] [CrossRef]
- O’Neill, J. Antimicrobial Resistance: Tackling a Crisis for the Health and Wealth of Nations. Rev. Antimicrob. Resist. 2014. Available online: https://amr-review.org/sites/default/files/AMR%20Review%20Paper%20-%20Tackling%20a%20crisis%20for%20the%20health%20and%20wealth%20of%20nations_1.pdf (accessed on 11 March 2024).
- Bruna, T.; Maldonado-Bravo, F.; Jara, P.; Caro, N. Silver Nanoparticles and Their Antibacterial Applications. Int. J. Mol. Sci. 2021, 22, 7202. [Google Scholar] [CrossRef]
- More, P.R.; Pandit, S.; Filippis, A.D.; Franci, G.; Mijakovic, I.; Galdiero, M. Silver Nanoparticles: Bactericidal and Mechanistic Approach against Drug Resistant Pathogens. Microorganisms 2023, 11, 369. [Google Scholar] [CrossRef]
- Sánchez-López, E.; Gomes, D.; Esteruelas, G.; Bonilla, L.; Lopez-Machado, A.L.; Galindo, R.; Cano, A.; Espina, M.; Ettcheto, M.; Camins, A.; et al. Metal-Based Nanoparticles as Antimicrobial Agents: An Overview. Nanomaterials 2020, 10, 292. [Google Scholar] [CrossRef]
- Yin, I.X.; Zhang, J.; Mie, M.L.; Li, Q.; Chu, C.H. The Antibacterial Mechanism of Silver Nanoparticles and Its Application in Dentistry. Int. J. Nanomed. 2020, 15, 2555–2562. [Google Scholar] [CrossRef]
- Bollenbach, T. Antimicrobial interactions: Mechanisms and implications for drug discovery and resistance evolution. Curr. Opin. Microbiol. 2015, 27, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Rai, M.; Paralikar, P.; Jogee, P.; Agarkar, G.; Ingle, A.P.; Derita, M.; Zacchino, S. Synergistic antimicrobial potential of essential oils in combination with nanoparticles: Emerging trends and future perspectives. Int. J. Pharm. 2017, 519, 67–78. [Google Scholar] [CrossRef] [PubMed]
- Lombrea, A.; Antal, D.; Ardelean, F.; Avram, S.; Pavel, I.Z.; Vlaia, L.; Mut, A.-M.; Diaconeasa, Z.; Dehelean, C.A.; Soica, C.; et al. A Recent Insight Regarding the Phytochemistry and Bioactivity of Origanum vulgare L. Essential Oil. Int. J. Mol. Sci. 2020, 21, 9653. [Google Scholar] [CrossRef] [PubMed]
- Scandorieiro, S.; de Camargo, L.C.; Lancheros, C.A.C.; Yamada-Ogatta, S.F.; Nakamura, C.V.; de Oliveira, A.G.; Andrade, C.G.T.J.; Duran, N.; Nakazato, G.; Kobayashi, R.K.T. Synergistic and Additive Effect of Oregano Essential Oil and Biological Silver Nanoparticles against Multidrug-Resistant Bacterial Strains. Front. Microbiol. 2016, 7, 760. [Google Scholar] [CrossRef]
- Alven, S.; Peter, S.; Aderibigbe, B.A. Polymer-Based Hydrogels Enriched with Essential Oils: A Promising Approach for the Treatment of Infected Wounds. Polymers 2022, 14, 3772. [Google Scholar] [CrossRef]
- Kim, H.; Shin, S.; Han, D. Review of History of Basic Principles of Burn Wound Management. Medicina 2022, 58, 400. [Google Scholar] [CrossRef]
- Heyneman, A.; Hoeksema, H.; Vandekerckhove, D.; Pirayesh, A.; Monstrey, S. The Role of Silver Sulphadiazine in the Conservative Treatment of Partial Thickness Burn Wounds: A Systematic Review. Burns 2016, 42, 1377–1386. [Google Scholar] [CrossRef]
- Oaks, R.J.; Cindass, R. Silver Sulfadiazine. Available online: https://www.ncbi.nlm.nih.gov/books/NBK556054/ (accessed on 27 May 2023).
- Casarini, T.P.A.; Frank, L.A.; Benin, T.; Onzi, G.; Puhlmann, A.R.; Guterres, S.S. Innovative hydrogel containing polymeric nanocapsules loaded with phloretin: Enhanced skin penetration and adhesion. Mater. Sci. Eng. C 2021, 120, 111681. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, N.; Bukhari, S.N.A.; Hussain, M.A.; Ejaz, H.; Munir, M.U.; Amjad, M.W. Nanoparticles Incorporated Hydrogels for Delivery of Antimicrobial Agents: Developments and Trends. RSC Adv. 2024, 14, 13535–13564. [Google Scholar] [CrossRef] [PubMed]
- Hu, C.; Yang, W. Alternatives to Animal Models to Study Bacterial Infections. Folia Microbiol. 2023, 68, 703–739. [Google Scholar] [CrossRef]
- Jorjão, A.L.; Oliveira, L.D.; Scorzoni, L.; Figueiredo-Godoi, L.M.A.; Cristina, A.; Prata, M.; Jorge, A.O.C.; Junqueira, J.C. From Moths to Caterpillars: Ideal Conditions for Galleria mellonella Rearing for in Vivo Microbiological Studies. Virulence 2018, 9, 383–389. [Google Scholar] [CrossRef]
- Maslova, E.; Shi, Y.; Sjöberg, F.; Azevedo, H.S.; Wareham, D.W.; McCarthy, R.R. An Invertebrate Burn Wound Model That Recapitulates the Hallmarks of Burn Trauma and Infection Seen in Mammalian Models. Front. Microbiol. 2020, 11, 998. [Google Scholar] [CrossRef] [PubMed]
- Alves, D.R.; Booth, S.P.; Scavone, P.; Schellenberger, P.; Salvage, J.; Dedi, C.; Thet, N.-T.; Jenkins, A.T.A.; Waters, R.; Ng, K.W.; et al. Development of a High-Throughput Ex-Vivo Burn Wound Model Using Porcine Skin, and Its Application to Evaluate New Approaches to Control Wound Infection. Front. Cell. Infect. Microbiol. 2018, 8, 196. [Google Scholar] [CrossRef]
- Chen, P.; Sebastian, E.A.; Karna, S.L.R.; Leung, K.P. Development of a Stringent Ex Vivo-Burned Porcine Skin Wound Model to Screen Topical Antimicrobial Agents. Antibiotics 2024, 13, 1159. [Google Scholar] [CrossRef]
- Andersson, M.; Madsen, L.B.; Schmidtchen, A.; Puthia, M. Development of an Experimental Ex Vivo Wound Model to Evaluate Antimicrobial Efficacy of Topical Formulations. Int. J. Mol. Sci. 2021, 22, 5045. [Google Scholar] [CrossRef]
- CLSI M100; Performance Standards for Antimicrobial Susceptibility Testing. Clinical and Laboratory Standards Institute (CLSI): Wayne, PA, USA, 2023.
- CLSI M02; Performance Standards for Antimicrobial Disk Susceptibility Tests. Clinical and Laboratory Standards Institute (CLSI): Wayne, PA, USA, 2018.
- CLSI M07; Methods for Dilution Antimicrobial Susceptibility Tests for Bacteria That Grow Aerobically. Clinical and Laboratory Standards Institute (CLSI): Wayne, PA, USA, 2018.
- Chin, N.X.; Weitzman, I.; Della-Latta, P. In Vitro Activity of Fluvastatin, a Cholesterol-Lowering Agent, and Synergy with Fluconazole and Itraconazole against Candida Species and Cryptococcus neoformans. Antimicrob. Agents Chemother. 1997, 41, 850–852. [Google Scholar] [CrossRef]
- Percival, S.L.; McCarty, S.; Hunt, J.A.; Woods, E.J. The Effects of PH on Wound Healing, Biofilms, and Antimicrobial Efficacy. Wound Repair. Regen. 2014, 22, 174–186. [Google Scholar] [CrossRef]
- Brasil Guia de Estabilidade de Produtos Cosméticos. 2004; Volume 1, 52p. Available online: https://bvsms.saude.gov.br/bvs/publicacoes/cosmeticos.pdf. (accessed on 10 March 2022).
- Brasil Guia de Controle de Qualidade de Produtos Cosméticos. 2008; 120p. Available online: https://www.gov.br/anvisa/pt-br/centraisdeconteudo/publicacoes/cosmeticos/manuais-e-guias/guia-de-controle-de-qualidade-de-produtos-cosmeticos.pdf, (accessed on 10 March 2022).
- Borghetti, G.S.; Knorst, M.T. Desenvolvimento e Avaliação Da Estabilidade Física de Loções O/A Contendo Filtros Solares. Braz. J. Pharm. Sci. 2006, 42, 531–537. [Google Scholar] [CrossRef]
- NCCLS. Methods for Determinating Bactericidal Activity of Antimicrobial Agents; M26-A; NCCLS: Wayne, PA, USA, 1999; Volume 19. [Google Scholar]
- Sousa, M.A.D.S.D.; Ferreira, A.F.; da Silva, C.C.; Silva, M.A.; Bazan, T.A.X.N.; Monteiro, C.D.A.; Monteiro, A.D.S.; Sousa, J.C.D.S.; da Silva, L.C.N.; Zagmignan, A. Development and Characterization of Hydroxyethyl Cellulose-Based Gels Containing Lactobacilli Strains: Evaluation of Antimicrobial Effects in In Vitro and Ex Vivo Models. Pharmaceuticals 2023, 16, 468. [Google Scholar] [CrossRef]
- Firacative, C.; Khan, A.; Duan, S.; Ferreira-Paim, K.; Leemon, D.; Meyer, W. Rearing and Maintenance of Galleria mellonella and Its Application to Study Fungal Virulence. J. Fungi 2020, 6, 130. [Google Scholar] [CrossRef]
- Maslova, E.; Osman, S.; McCarthy, R.R. Using the Galleria mellonella Burn Wound and Infection Model to Identify and Characterize Potential Wound Probiotics. Microbiology 2023, 169, 001350. [Google Scholar] [CrossRef]
- Magiorakos, A.P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-Resistant, Extensively Drug-Resistant and Pandrug-Resistant Bacteria: An International Expert Proposal for Interim Standard Definitions for Acquired Resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef] [PubMed]
- Saeki, E.K.; Yamada, A.Y.; de Araujo, L.A.; Anversa, L.; Garcia, D.D.O.; de Souza, R.L.B.; Martins, H.M.; Kobayashi, R.K.T.; Nakazato, G. Subinhibitory Concentrations of Biogenic Silver Nanoparticles Affect Motility and Biofilm Formation in Pseudomonas aeruginosa. Front. Cell. Infect. Microbiol. 2021, 11, 656984. [Google Scholar] [CrossRef] [PubMed]
- Sumini, M.; Souza, C.R.D.; Andrade, G.J.S.; Oliveira, I.R.C.; Scandorieiro, S.; Tischer, C.A.; Kobayashi, R.K.T.; Nakazato, G. Cellulose Hydrogel with Hyaluronic Acid and Silver Nanoparticles: Sustained-Release Formulation with Antibacterial Properties against Pseudomonas aeruginosa. Antibiotics 2023, 12, 873. [Google Scholar] [CrossRef]
- da Cunha, K.F.; Oliveira Garcia, M.; Allend, S.O.; de Albernaz, D.F.T.; Panagio, L.A.; Neto, A.C.P.S.; Larré Oliveira, T.; Hartwig, D.D. Biogenic Silver Nanoparticles: In Vitro Activity against Staphylococcus aureus Methicillin-Resistant (MRSA) and Multidrug-Resistant Coagulase-Negative Staphylococcus (CoNS). Braz. J. Microbiol. 2023, 54, 2641–2650. [Google Scholar] [CrossRef]
- Cardozo, V.F.; Oliveira, A.G.; Nishio, E.K.; Perugini, M.R.; Andrade, C.G.; Silveira, W.D.; Durán, N.; Andrade, G.; Kobayashi, R.K.; Nakazato, G. Antibacterial Activity of Extracellular Compounds Produced by a Pseudomonas Strain against Methicillin-Resistant Staphylococcus aureus (MRSA) Strains. Ann. Clin. Microbiol. Antimicrob. 2013, 12, 12. [Google Scholar] [CrossRef]
- Saoudi, B.; Bariz, K.; Saci, S.; Belounis, Y.; Ait Issad, H.; Abbaci, M.; Mustapha, M.A.; Nabti, E.-H.; Alenazy, R.; Alhussaini, M.S.; et al. Enhancing Antibiotic Efficacy and Combating Biofilm Formation: Evaluating the Synergistic Potential of Origanum vulgare Essential Oil against Multidrug-Resistant Gram-Negative Bacteria. Microorganisms 2024, 12, 1651. [Google Scholar] [CrossRef]
- Hao, Y.; Li, J.; Shi, L. A Carvacrol-Rich Essential Oil Extracted From Oregano (Origanum vulgare “Hot & Spicy”) Exerts Potent Antibacterial Effects Against Staphylococcus aureus. Front. Microbiol. 2021, 12, 741861. [Google Scholar] [CrossRef]
- Tejada-Muñoz, S.; Cortez, D.; Rascón, J.; Chavez, S.G.; Caetano, A.C.; Díaz-Manchay, R.J.; Sandoval-Bances, J.; Huyhua-Gutierrez, S.; Gonzales, L.; Chenet, S.M.; et al. Antimicrobial Activity of Origanum vulgare Essential Oil against Staphylococcus aureus and Escherichia coli. Pharmaceuticals 2024, 17, 1430. [Google Scholar] [CrossRef] [PubMed]
- Nazzaro, F.; Fratianni, F.; De Martino, L.; Coppola, R.; De Feo, V. Effect of Essential Oils on Pathogenic Bacteria. Pharmaceuticals 2013, 6, 1451–1474. [Google Scholar] [CrossRef] [PubMed]
- Fikry, S.; Khalil, N.; Salama, O. Chemical Profiling, Biostatic and Biocidal Dynamics of Origanum vulgare L. Essential Oil. AMB Express 2019, 9, 41. [Google Scholar] [CrossRef]
- Burt, S. Essential Oils: Their Antibacterial Properties and Potential Applications in Foods—A Review. Int. J. Food Microbiol. 2004, 94, 223–253. [Google Scholar] [CrossRef]
- Scandorieiro, S.; Rodrigues, B.C.D.; Nishio, E.K.; Panagio, L.A.; de Oliveira, A.G.; Durán, N.; Nakazato, G.; Kobayashi, R.K.T. Biogenic Silver Nanoparticles Strategically Combined With Origanum vulgare Derivatives: Antibacterial Mechanism of Action and Effect on Multidrug-Resistant Strains. Front. Microbiol. 2022, 13, 842600. [Google Scholar] [CrossRef] [PubMed]
- Radzikowska-Büchner, E.; Łopuszyńska, I.; Flieger, W.; Tobiasz, M.; Maciejewski, R.; Flieger, J. An Overview of Recent Developments in the Management of Burn Injuries. Int. J. Mol. Sci. 2023, 24, 16357. [Google Scholar] [CrossRef]
- Dallo, M.; Patel, K.; Hebert, A.A. Topical Antibiotic Treatment in Dermatology. Antibiotics 2023, 12, 188. [Google Scholar] [CrossRef]
- Varaprasad, K.; Raghavendra, G.M.; Jayaramudu, T.; Yallapu, M.M.; Sadiku, R. A Mini Review on Hydrogels Classification and Recent Developments in Miscellaneous Applications. Mater. Sci. Eng. C 2017, 79, 958–971. [Google Scholar] [CrossRef]
- Arabpour, Z.; Abedi, F.; Salehi, M.; Baharnoori, S.M.; Soleimani, M.; Djalilian, A.R. Hydrogel-Based Skin Regeneration. Int. J. Mol. Sci. 2024, 25, 1982. [Google Scholar] [CrossRef]
- Han, G.; Ceilley, R. Chronic Wound Healing: A Review of Current Management and Treatments. Adv. Ther. 2017, 34, 599–610. [Google Scholar] [CrossRef]
- Lucas Meyer Cosmetics Lecigel—Technical File. Available online: https://www.lucasmeyercosmetics.com/en/products?title=Lecigel%E2%84%A2 (accessed on 10 April 2022).
- da Silva, J.A.; Apolinário, A.C.; Souza, M.S.R.; Damasceno, B.P.G.L.; Medeiros, A.C.D. Administração Cutânea de Fármacos: Desafios e Estratégias Para o Desenvolvimento de Formulações Transdérmicas. Rev. Cienc. Farm. Basica Apl. 2010, 31, 125–131. [Google Scholar]
- Xiao, G.; Li, J.; Sun, Z. The Combination of Antibiotic and Non-Antibiotic Compounds Improves Antibiotic Efficacy against Multidrug-Resistant Bacteria. Int. J. Mol. Sci. 2023, 24, 15493. [Google Scholar] [CrossRef]
- Aljaafari, M.N.; Alali, A.O.; Baqais, L.; Alqubaisy, M.; Alali, M.; Molouki, A.; Ong-Abdullah, J.; Abushelaibi, A.; Lai, K.S.; Lim, S.H.E. An Overview of the Potential Therapeutic Applications of Essential Oils. Molecules 2021, 26, 628. [Google Scholar] [CrossRef] [PubMed]
- Kaiser, K.G.; Delattre, V.; Frost, V.J.; Buck, G.W.; Phu, J.V.; Fernandez, T.G.; Pavel, I.E. Nanosilver: An Old Antibacterial Agent with Great Promise in the Fight against Antibiotic Resistance. Antibiotics 2023, 12, 1264. [Google Scholar] [CrossRef] [PubMed]
- Graves, J.L.; Tajkarimi, M.; Cunningham, Q.; Campbell, A.; Nonga, H.; Harrison, S.H.; Barrick, J.E. Rapid Evolution of Silver Nanoparticle Resistance in Escherichia coli. Front. Genet. 2015, 6, 42. [Google Scholar] [CrossRef] [PubMed]
- McNeilly, O.; Mann, R.; Hamidian, M.; Gunawan, C. Emerging Concern for Silver Nanoparticle Resistance in Acinetobacter baumannii and Other Bacteria. Front. Microbiol. 2021, 12, 652863. [Google Scholar] [CrossRef]
- Panáček, A.; Kvítek, L.; Smékalová, M.; Večeřová, R.; Kolář, M.; Röderová, M.; Dyčka, F.; Šebela, M.; Prucek, R.; Tomanec, O.; et al. Bacterial Resistance to Silver Nanoparticles and How to Overcome It. Nat. Nanotechnol. 2017, 13, 65–71. [Google Scholar] [CrossRef]
- Seaton, M.; Hocking, A.; Gibran, N.S. Porcine Models of Cutaneous Wound Healing. ILAR J. 2015, 56, 127–138. [Google Scholar] [CrossRef]
- Dai, T.; Kharkwal, G.B.; Tanaka, M.; Huang, Y.Y.; Bil de Arce, V.J.; Hamblin, M.R. Animal Models of External Traumatic Wound Infections. Virulence 2011, 2, 296. [Google Scholar] [CrossRef]
- Gjødsbøl, K.; Christensen, J.J.; Karlsmark, T.; Jørgensen, B.; Klein, B.M.; Krogfelt, K.A. Multiple Bacterial Species Reside in Chronic Wounds: A Longitudinal Study. Int. Wound J. 2006, 3, 225–231. [Google Scholar] [CrossRef] [PubMed]
- dos Santos, W.B.; Silva Araujo, M.G.; Da Silva, J.C.; Bernardo, T.H.L.; De Assis Bastos, M.L.; Veríssimo, R.C.S.S. Microbiota Infectante De Feridas Cirúrgicas: Análise Da Produção Científica Nacional E Internacional. Rev. Sobecc 2016, 21, 46. [Google Scholar] [CrossRef]
- McLaughlin, H.P.; Caly, D.L.; McCarthy, Y.; Ryan, R.P.; Dow, J.M. An Orphan Chemotaxis Sensor Regulates Virulence and Antibiotic Tolerance in the Human Pathogen Pseudomonas aeruginosa. PLoS ONE 2012, 7, e42205. [Google Scholar] [CrossRef] [PubMed]
- Peleg, A.Y.; Monga, D.; Pillai, S.; Mylonakis, E.; Moellering, R.C., Jr.; Eliopoulos, G.M. Reduced Susceptibility to Vancomycin Influences Pathogenicity in Staphylococcus aureus Infection. J. Infect. Dis. 2009, 199, 532–536. [Google Scholar] [CrossRef] [PubMed]
- Ménard, G.; Rouillon, A.; Cattoir, V.; Donnio, P.-Y. Galleria mellonella as a Suitable Model of Bacterial Infection: Past, Present and Future. Front. Cell. Infect. Microbiol. 2021, 11, 782733. [Google Scholar] [CrossRef]
- Pereira, M.F.; Rossi, C.C.; da Silva, G.C.; Rosa, J.N.; Bazzolli, D.M.S. Galleria mellonella as an Infection Model: An In-Depth Look at Why It Works and Practical Considerations for Successful Application. Pathog. Dis. 2020, 78, ftaa056. [Google Scholar] [CrossRef]
- Rossoni, R.D.; de Camargo Ribeiro, F.; dos Santos, H.F.S.; dos Santos, J.D.; de Sousa Oliveira, N.; dos Santos Dutra, M.T.; de Lapena, S.A.B.; Junqueira, J.C. Galleria mellonella as an Experimental Model to Study Human Oral Pathogens. Arch. Oral Biol. 2019, 101, 13–22. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Microorganism | Origin | ID | Resistance Profile to Antimicrobials | |
|---|---|---|---|---|
| Klebsiella pneumoniae | Tissue | 10904 | PPT, FEP, CTX, CPD, CAZ, CRO, CRX, LEV, CIP, TET, GEN, TOB, ETP, IPM, MEM, SUT, CLO | KPC MDR |
| Tissue | 11034 | PPT, FEP, CTX, CPD, CAZ, CRO, CRX, LEV, CIP, TET, GEN, TOB, ETP, IPM, MEM, SUT, AMI, CLO | KPC MDR | |
| Tissue | 11091 | PPT, FEP, CTX, CPD, CAZ, CRO, CRX, LEV *, CIP, TET, GEN, TOB, ETP, IPM, MEM, SUT, CLO * | KPC MDR | |
| Tissue | 11271 | PPT, FEP, CTX, CPD, CAZ, CRO, CRX, LEV, CIP, TET, GEN, TOB, ETP, IPM, MEM, AZI, SUT, CLO | KPC MDR | |
| Bone Fragment | 10797 | PPT, FEP, CTX, CPD, CAZ, CRO, CRX, LEV, CIP, TET, GEN, TOB, ETP, MEM, AZI, SUT, CLO | KPC MDR | |
| Pseudomonas aeruginosa | Urine | 2491 | LEV, CAZ, CIP, TOB, ATM, PPT, IPM, MEM | CR MDR |
| Tissue | 3167 | LEV, CAZ, CIP, TOB, ATM, PPT, IPM, MEM | CR MDR | |
| Tissue | 1461 | LEV, CAZ, CIP, TOB, ATM, PPT, IPM, MEM | CR MDR | |
| Tissue | 2815 | LEV, CAZ, CIP, TOB, ATM, PPT, IPM, MEM | CR MDR | |
| Urine | 117 | LEV, TGC, CAZ, CIP, ATM, PPT, IPM, MEM, GEN, NOR, NAL | CR MDR | |
| Human patient | 1634 | LEV, TGC, CAZ, CIP, TOB, ATM, PPT, IPM, MEM, GEN, NOR, NAL | CR MDR | |
| Staphylococcus aureus | Tissue | 373 | P, OX, AZI, CIP, CLO *, CLI, ERI, QD | MRSA |
| Tissue | 207 | P, OX, AZI, CIP, CLO *, CLI, ERI, QD | MRSA | |
| Tissue | 521 | P, OX, AZI, CIP, CLI, ERI, QD | MRSA | |
| Tissue | 999 | P, OX, AZI, CIP *, CLI, ERI, QD | MRSA | |
| Tissue | 336 | P, OX, AZI, CIP, SUL, CLI, ERI, QD | MRSA | |
| Bio-AgNP (mg/mL) | OEO (mg/mL) | FICI | Interaction | |||||
|---|---|---|---|---|---|---|---|---|
| MICind | MICcomb | FIC | MICind | MICcomb | FIC | |||
| P. aeruginosa 1461 | 0.0212 | 0.0026 | 0.12 | 4.75 | 1.18 | 0.25 | 0.37 | Sinergism |
| P. aeruginosa ATCC 27853 | 0.0053 | 0.0013 | 0.25 | 2.37 | 0.59 | 0.25 | 0.49 | Sinergism |
| P. aeruginosa 2491 | 0.0106 | 0.0013 | 0.25 | 4.75 | 1.18 | 0.13 | 0.38 | Aditism |
| P. aeruginosa 2815 | 0.0106 | 0.0013 | 0.12 | 9.50 | 2.37 | 0.25 | 0.37 | Sinergism |
| P. aeruginosa 117 | 0.0106 | 0.001 | 0.09 | 9.50 | 1.18 | 0.12 | 0.22 | Sinergism |
| P. aeruginosa 1634 | 0.0106 | 0.001 | 0.09 | 9.50 | 1.18 | 0.12 | 0.22 | Sinergism |
| PRSA 999 | 0.0106 | 0.0026 | 0.24 | 0.59 | 0.296 | 0.50 | 0.74 | Aditism |
| PRSA 207 | 0.0212 | 0.0026 | 0.12 | 1.18 | 0.59 | 0.50 | 0.62 | Aditism |
| PRSA 521 | 0.0212 | 0.0106 | 0.47 | 1.18 | 0.29 | 0.25 | 0.72 | Aditism |
| S.aureus ATCC 6538 | 0.0212 | 0.0026 | 0.12 | 1.18 | 0.59 | 0.50 | 0.62 | Aditism |
| MRSA N315 | 0.0212 | 0.0212 | 0.10 | 1.18 | 1.18 | 0.50 | 0.47 | Aditism |
| K.pneumoniae 11034 | 0.0212 | 0.0026 | 0.12 | 1.18 | 0.59 | 0.50 | 0.62 | Aditism |
| K.pneumoniae 10797 | 0.0212 | 0.0106 | 0.47 | 0.59 | 0.07 | 0.13 | 0.60 | Aditism |
| K.pneumoniae ATCC 700603 | 0.0212 | 0.0026 | 0.12 | 1.18 | 0.59 | 0.50 | 0.62 | Aditism |
| Color | Odor | Aspect | ||||
|---|---|---|---|---|---|---|
| Formulation | T0 | T15 | T0 | T15 | T0 | T15 |
| Base | White | N | Odorless | N | Homogeneous | N |
| HAgNP | Caramel | LM | Odorless | N | Homogeneous | N |
| HO1 | White | N | OEO | N | Homogeneous | N |
| HO0.5 | White | N | OEO | N | Homogeneous | N |
| HagNP + OEO1 | Caramel | LM | OEO | N | Homogeneous | N |
| HagNP + OEO0.5 | Caramel | LM | OEO | N | Homogeneous | N |
| pH | Density | |||
|---|---|---|---|---|
| Formulation | T0 | T15 | T0 | T15 |
| Base | 6.95 ± 0.03 | 6.83 ± 0.02 | 9.95 ± 0.01 | 9.91 ± 0.02 |
| HAgNP | 6.94 ± 0.02 | 6.53 ± 0.02 | 10.10 ± 0.02 | 9.99 ± 0.01 |
| HO1 | 6.92 ± 0.04 | 6.57 ± 0.01 | 10.06 ± 0.02 | 9.96 ± 0.02 |
| HO0.5 | 6.96 ± 0.02 | 6.59 ± 0.02 | 10.05 ± 0.02 | 9.99 ± 0.01 |
| HagNP + OEO1 | 6.94 ± 0.04 | 6.56 ± 0.03 | 10.14 ± 0.03 | 9.99 ± 0.01 |
| HagNP + OEO0.5 | 6.97 ± 0.03 | 6.87 ± 0.02 | 10.10 ± 0.02 | 10.02 ± 0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kimura, A.H.; Dahmer, D.; Isawa, L.A.; da Silva, A.B.O.; Souza, L.M.d.S.; Takata, P.H.; Scandorieiro, S.; Deonas, A.N.; Germiniani-Cardozo, J.; Vespero, E.C.; et al. Hydrogel Containing Biogenic Silver Nanoparticles and Origanum vulgare Essential Oil for Burn Wounds: Antimicrobial Efficacy Using Ex Vivo and In Vivo Methods Against Multidrug-Resistant Microorganisms. Pharmaceutics 2025, 17, 503. https://doi.org/10.3390/pharmaceutics17040503
Kimura AH, Dahmer D, Isawa LA, da Silva ABO, Souza LMdS, Takata PH, Scandorieiro S, Deonas AN, Germiniani-Cardozo J, Vespero EC, et al. Hydrogel Containing Biogenic Silver Nanoparticles and Origanum vulgare Essential Oil for Burn Wounds: Antimicrobial Efficacy Using Ex Vivo and In Vivo Methods Against Multidrug-Resistant Microorganisms. Pharmaceutics. 2025; 17(4):503. https://doi.org/10.3390/pharmaceutics17040503
Chicago/Turabian StyleKimura, Angela Hitomi, Débora Dahmer, Luana Ayumi Isawa, Ana Beatriz Olivetti da Silva, Lucas Marcelino dos Santos Souza, Pedro Henrique Takata, Sara Scandorieiro, Anastácia Nikolaos Deonas, Jennifer Germiniani-Cardozo, Eliana Carolina Vespero, and et al. 2025. "Hydrogel Containing Biogenic Silver Nanoparticles and Origanum vulgare Essential Oil for Burn Wounds: Antimicrobial Efficacy Using Ex Vivo and In Vivo Methods Against Multidrug-Resistant Microorganisms" Pharmaceutics 17, no. 4: 503. https://doi.org/10.3390/pharmaceutics17040503
APA StyleKimura, A. H., Dahmer, D., Isawa, L. A., da Silva, A. B. O., Souza, L. M. d. S., Takata, P. H., Scandorieiro, S., Deonas, A. N., Germiniani-Cardozo, J., Vespero, E. C., Perugini, M. R. E., Lincopan, N., Garcia Lonni, A. A. S., Nakazato, G., & Kobayashi, R. K. T. (2025). Hydrogel Containing Biogenic Silver Nanoparticles and Origanum vulgare Essential Oil for Burn Wounds: Antimicrobial Efficacy Using Ex Vivo and In Vivo Methods Against Multidrug-Resistant Microorganisms. Pharmaceutics, 17(4), 503. https://doi.org/10.3390/pharmaceutics17040503