Advances in Drug Delivery Integrated with Regenerative Medicine: Innovations, Challenges, and Future Frontiers



Abstract
1. Introduction
2. Fundamentals of Regenerative Medicine
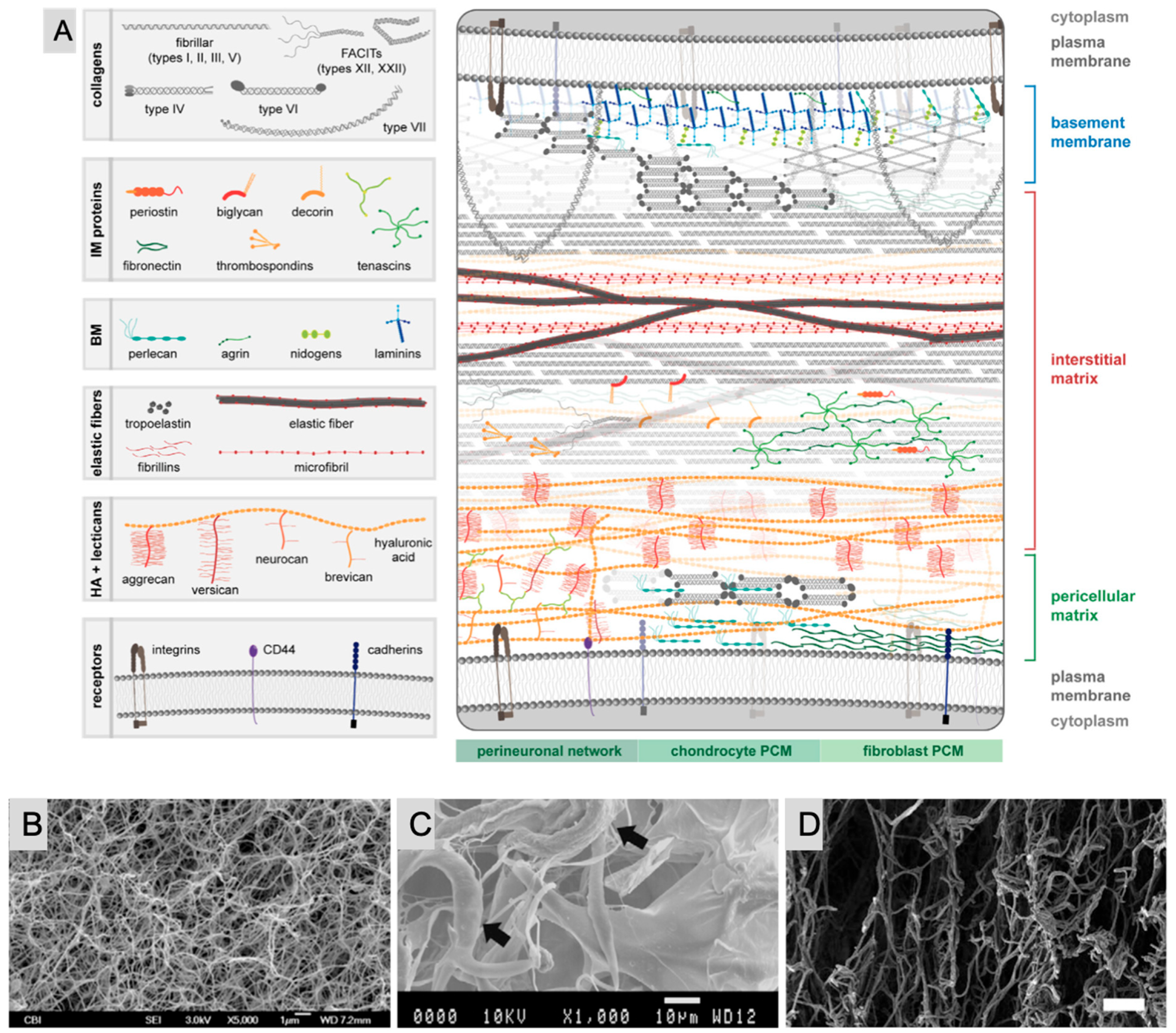
2.1. Extracellular Matrix (ECM)
2.2. Cellular Components: Cells Used in Regenerative Medicine
2.2.1. Stem Cells
Embryonic Stem Cells (ESCs)
Adult Stem Cells
Induced Pluripotent Stem Cells (iPSCs)
2.2.2. Progenitor Cells
2.2.3. Somatic Cells
2.2.4. Immune Cells
2.2.5. Endothelial Cells
2.2.6. Chondrocytes and Osteoblasts
2.2.7. Myocytes in Regenerative Medicine
2.3. Cell Sources and Applications
2.3.1. Cell Sources
2.3.2. Cell Isolation and Culture
2.3.3. Cell–Cell Interactions
2.3.4. Cell Delivery Methods
2.3.5. Regulatory and Ethical Issues
3. Drug Delivery Systems in Regenerative Medicine
3.1. Overview of Drug Delivery Approaches
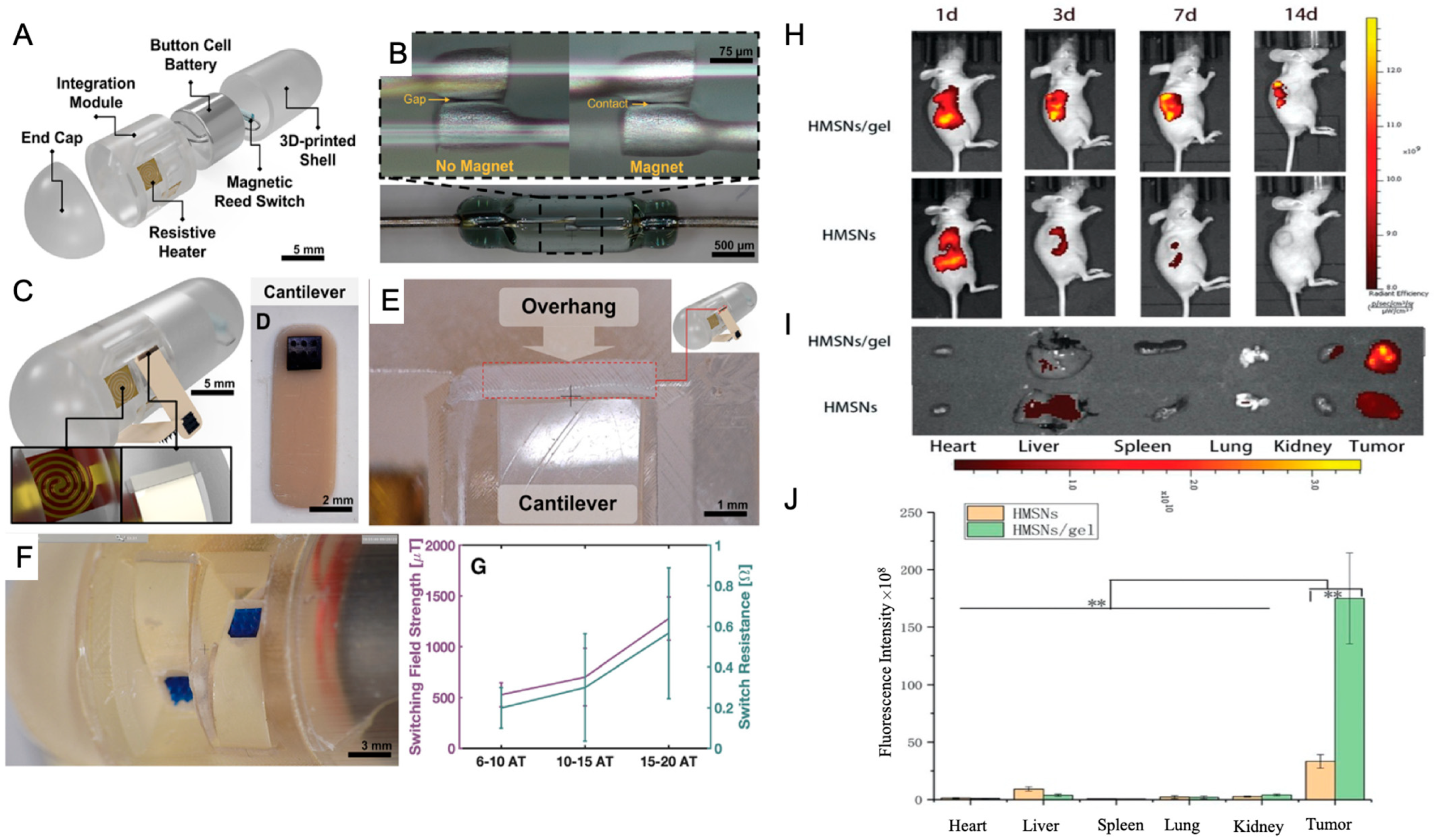
3.2. Localized Drug Delivery Techniques

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cell Type | Key Features | Applications in Regenerative Medicine | Integration with Drug Delivery Systems | Ref. |
|---|---|---|---|---|
| Stem Cells | ||||
| Embryonic Stem Cells (ESCs) | Pluripotent; potential for infinite growth; Derived from the embryonic inner cell mass | Spinal injury, cardiovascular diseases, and neurodegenerative disorders; Limited due to ethical and political concerns | Controlled-release systems for protecting and sustaining growth factors; Smart scaffolds for directed differentiation | [101,102] |
| Adult Stem Cells | Undifferentiated, found in most organs; Capable of tissue regeneration and self-renewal | Treat degenerative disorders and cancers; Effective in bone marrow and skin grafts | Bioactive scaffolds supporting tissue repair; Nanoparticles for precise delivery of therapeutic agents | [103,104] |
| Induced Pluripotent Stem Cells (iPSCs) | Reprogrammed adult cells resembling ESCs; Personalized, patient-specific | Used in disease modeling, drug screening, and patient-specific therapies | Biomaterials for controlled differentiation Smart patches delivering bioactive molecules | [59,61] |
| Progenitor Cells | Limited self-renewal and differentiation potential; Involved in tissue repair | Targeted tissue regeneration in neurodegenerative diseases, heart disease, and diabetes | Sustained release of differentiation factors via nanoparticles; Scaffolds mimicking native environments | [105] |
| Somatic Cells | Specialized non-reproductive cells; Replace and repair damaged cells | Tissue engineering for skin, liver, muscle, and nerve regeneration | Drug-loaded liposomes targeting specific cell types; Regenerative skin patches | [46,47] |
| Immune Cells | T cells: adaptive immunity, CAR-T therapies; Dendritic cells: antigen presentation | Cancer immunotherapy, vaccine development, and regenerative immunology | Nanoparticles enhancing antigen presentation; Engineered delivery vehicles targeting immune cells | [50] |
| Endothelial Cells | Line blood vessels; critical for angiogenesis | Vascularization in tissue engineering and wound healing | Targeted drug delivery for vascular diseases; Nanoparticles exploiting tumor vasculature for drug delivery | [53,54,55] |
| Chondrocytes | Maintain cartilage extracellular matrix | Cartilage regeneration and repair | Hydrogels for sustained release of anti-inflammatory agents; Scaffolds delivering growth factors | [56] |
| Osteoblasts | Bone formation and mineralization | Bone repair and regeneration | Scaffolds loaded with BMPs for accelerated healing; Controlled release of osteogenic agents | [57] |
| Myocytes | Muscle cells responsible for contraction | Muscle regeneration for degenerative diseases and injuries | Hydrogels releasing IGF-1 for enhanced regeneration; Nanoparticles delivering bioactive molecules | [58] |
3.3. Controlled Release Systems
Controlled Release Systems: Mathematical Models, Equations, and Applications
- I.
- Diffusion-Based Models
- II.
- Higuchi Model
- III.
- Peppas (Korsmeyer–Peppas) Model
- IV.
- First-Order Kinetics
- V.
- Zero-Order Kinetics
- VI.
- Weibull Model
- VII.
- Hixson-Crowell Model
- VIII.
- Hopfenberg Model
- IX.
- Sequential Layer Model
4. Challenges and Limitations
4.1. Biological Barriers
4.2. Safety Concerns in Drug Delivery Systems
4.3. Regulatory Hurdles
5. Future Directions and Emerging Technologies
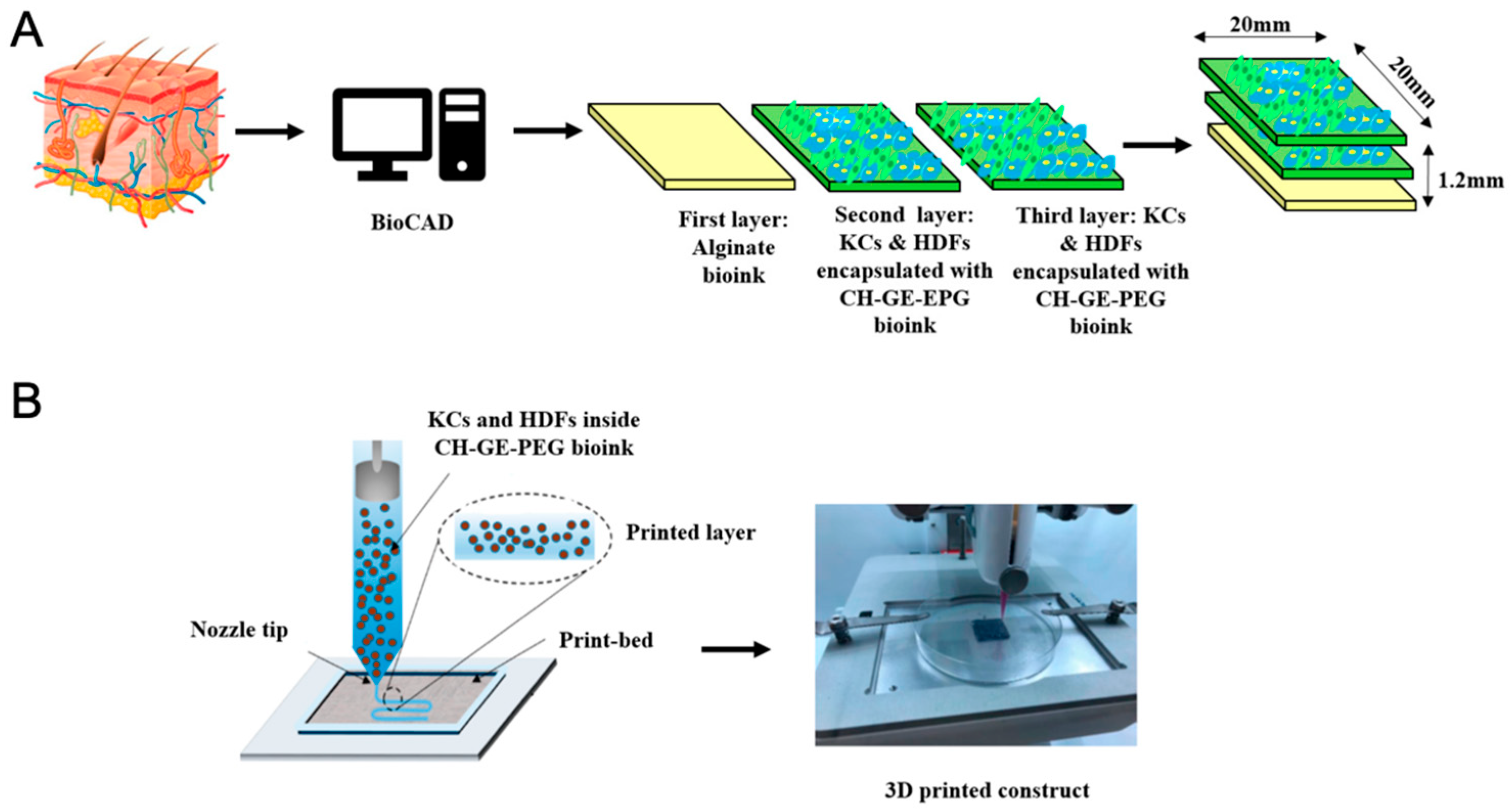
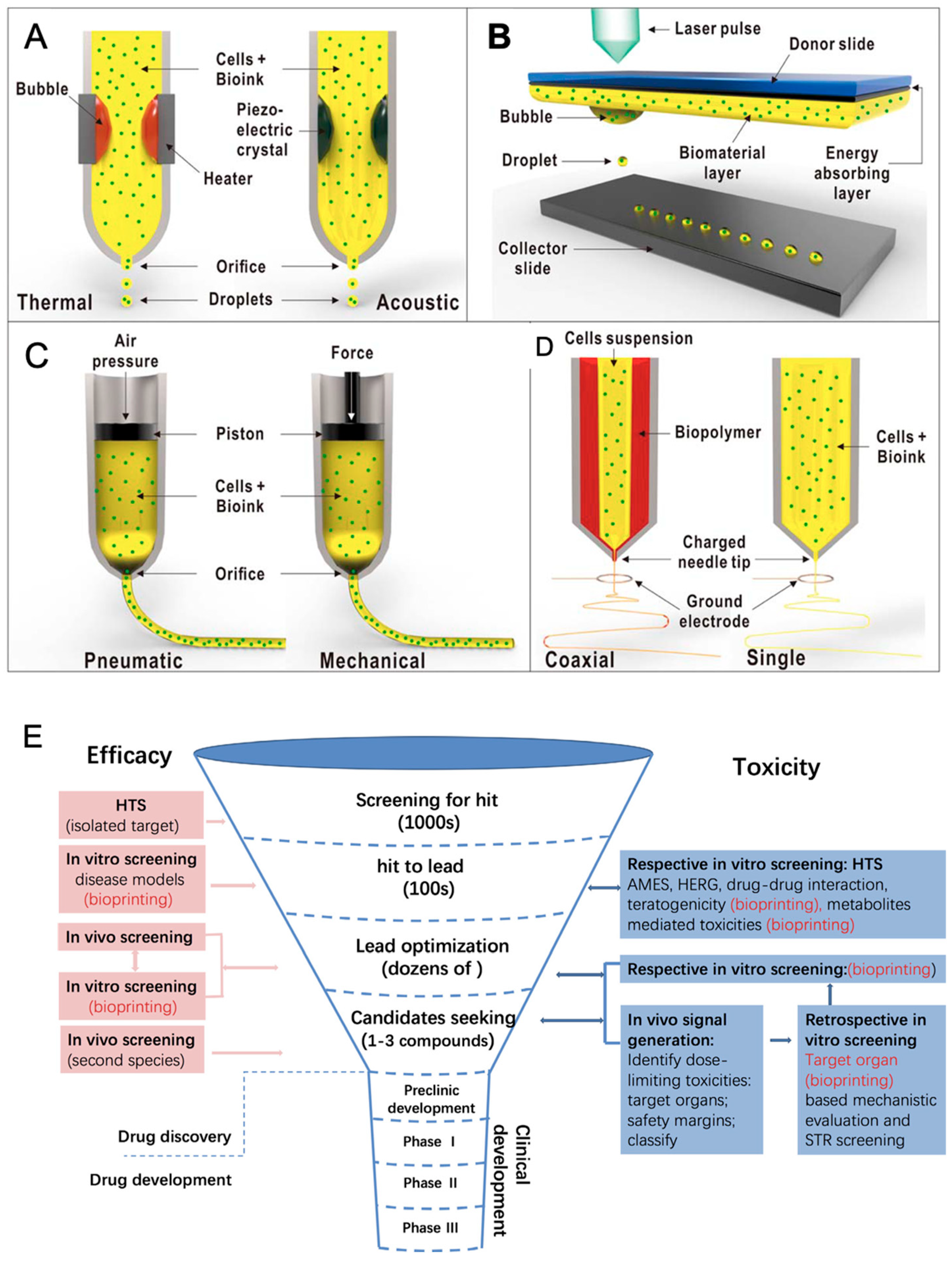
3D Bioprinting and Personalized Scaffolds
6. Conclusions and Perspectives
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| API | active pharmaceutical ingredients |
| BMP | bone morphogenetic proteins |
| CDDP | cisplatin (a chemotherapy drug) |
| CH-GE | chitosan–genipin bioink |
| c-Myc | Cellular Myc |
| CXCR4 | C-X-C Chemokine Receptor Type 4 (Chemokine receptor involved in signaling) |
| CPP | cell-penetrating peptide |
| DDSs | drug delivery systems |
| DOX | doxorubicin |
| DLP | digital light processing |
| ESCs | embryonic stem cells |
| ERT | Erlotinib |
| ECM | extracellular matrix |
| EHDA | electrohydrodynamic atomization |
| ES | electrospraying |
| EPR | enhanced permeation and retention |
| EVs | extracellular vesicles |
| FGFs | fibroblast growth factors |
| GI | gastrointestinal |
| GAGs | glycosaminoglycans |
| Hh | Hedgehog (regulates embryonic development, stem cells, and tissue patterning) |
| HMSNs | mesoporous silica nanoparticles |
| HA | hyaluronic acid |
| IGF-1 | insulin-like growth factor |
| IVIVC | in vitro–in vivo correlation |
| iPSCs | induced pluripotent stem cells |
| Klf4 | Kruppel-like factor 4 |
| MSCs | mesenchymal stem cells |
| MHT | magnetic hyperthermia |
| MNPs | magnetic nanoparticles |
| MTE | multi-tip emitter |
| NPs | nanoparticles |
| NSCLC | non-small cell lung cancer |
| Notch | controls cell fate, stem cell maintenance, and differentiation |
| Oct4 | Octamer-binding transcription factor 4 |
| PLGA | poly (lactic-co-glycolic acid) |
| PCL | polycaprolactone |
| PEG | polyethylene glycol |
| PLA | poly(lactide) |
| PDA | polydopamine |
| PEGDA | poly (ethylene glycol) diacrylate |
| PCa | prostate cancer |
| SPIONs | Superparamagnetic Iron Oxide Nanoparticles |
| Sox2 | [SRY (Sex-determining Region Y)-Box 2] |
| SMP | shape memory polymer |
| TMNPs | Trimagnetic Nanoparticles |
| Tg | glass transition temperature |
| VEGF | Vascular Endothelial Growth Factor |
| Wnt | Wingless/Int-1 (regulates cell growth, differentiation, stem cells, and tissue regeneration) |
| 3D | three-dimensional |
References
- Adepu, S.; Ramakrishna, S. Controlled Drug Delivery Systems: Current Status and Future Directions. Molecules 2021, 26, 5905. [Google Scholar] [CrossRef] [PubMed]
- Ezike, T.C.; Okpala, U.S.; Onoja, U.L.; Nwike, C.P.; Ezeako, E.C.; Okpara, O.J.; Okoroafor, C.C.; Eze, S.C.; Kalu, O.L.; Odoh, E.C.; et al. Advances in drug delivery systems, challenges and future directions. Heliyon 2023, 9, e17488. [Google Scholar] [CrossRef]
- Van Der Meel, R.; Sulheim, E.; Shi, Y.; Kiessling, F.; Mulder, W.J.M.; Lammers, T. Smart cancer nanomedicine. Nat. Nanotechnol. 2019, 14, 1007–1017. [Google Scholar] [CrossRef] [PubMed]
- Rasekh, M.; Pisapia, F.; Nokhodchi, A. Innovative applications of electrospun nanofibers in cancer research. J. Drug Deliv. Sci. Technol. 2024, 91, 105255. [Google Scholar]
- Dormont, F.; Varna, M.; Couvreur, P. Nanoplumbers: Biomaterials to fight cardiovascular diseases. Mater. Today 2018, 21, 122–143. [Google Scholar] [CrossRef]
- Laffleur, F.; Keckeis, V. Advances in drug delivery systems: Work in progress still needed? Int. J. Pharm. 2020, 590, 119912. [Google Scholar] [CrossRef]
- Hoffman, T.; Khademhosseini, A.; Langer, R. Chasing the Paradigm: Clinical Translation of 25 Years of Tissue Engineering. Tissue Eng. Part. A 2019, 25, 679–687. [Google Scholar] [CrossRef]
- Nie, T.; Wang, W.; Liu, X.; Wang, Y.; Li, K.; Song, X.; Zhang, J.; Yu, L.; He, Z. Sustained release systems for delivery of therapeutic peptide/protein. Biomacromolecules 2021, 22, 2299–2324. [Google Scholar] [CrossRef]
- Madl, C.M.; Heilshorn, S.C.; Blau, H.M. Bioengineering strategies to accelerate stem cell therapeutics. Nature 2018, 557, 335–342. [Google Scholar] [CrossRef]
- Salerno, A.; Netti, P.A. Review on computer-aided design and manufacturing of drug delivery scaffolds for cell guidance and tissue regeneration. Front. Bioeng. Biotechnol. 2021, 9, 682133. [Google Scholar]
- Ntege, E.H.; Sunami, H.; Shimizu, Y. Advances in regenerative therapy: A review of the literature and future directions. Regen. Ther. 2020, 14, 136–153. [Google Scholar] [PubMed]
- Hoogduijn, M.J.; Montserrat, N.; van der Laan, L.J.; Dazzi, F.; Perico, N.; Kastrup, J.; Gilbo, N.; Ploeg, R.J.; Roobrouck, V.; Casiraghi, F.; et al. The emergence of regenerative medicine in organ transplantation: 1st European Cell Therapy and Organ Regeneration Section meeting. Transplant. Int. 2020, 33, 833–840. [Google Scholar]
- Muzzio, N.; Moya, S.; Romero, G. Multifunctional scaffolds and synergistic strategies in tissue engineering and regenerative medicine. Pharmaceutics 2021, 13, 792. [Google Scholar] [CrossRef]
- Filipczak, N.; Yalamarty, S.S.K.; Li, X.; Khan, M.M.; Parveen, F.; Torchilin, V. Lipid-based drug delivery systems in regenerative medicine. Materials 2021, 14, 5371. [Google Scholar] [CrossRef] [PubMed]
- Del Amo, E.M.; Rimpelä, A.K.; Heikkinen, E.; Kari, O.K.; Ramsay, E.; Lajunen, T.; Schmitt, M.; Pelkonen, L.; Bhattacharya, M.; Richardson, D.; et al. Pharmacokinetic aspects of retinal drug delivery. Prog. Retin. Eye Res. 2017, 57, 134–185. [Google Scholar]
- Lage, O.M.; Ramos, M.C.; Calisto, R.; Almeida, E.; Vasconcelos, V.; Vicente, F. Current Screening Methodologies in Drug Discovery for Selected Human Diseases. Mar. Drugs. 2018, 16, 279. [Google Scholar]
- Ingber, D.E. Human organs-on-chips for disease modelling, drug development and personalized medicine. Nat. Rev. Genet. 2022, 23, 467–491. [Google Scholar]
- Li, C.; Wang, J.; Wang, Y.; Gao, H.; Wei, G.; Huang, Y.; Yu, H.; Gan, Y.; Wang, Y.; Mei, L.; et al. Recent progress in drug delivery. Acta Pharm. Sin. B. 2019, 9, 1145–1162. [Google Scholar]
- Mansour, A.; Romani, M.; Acharya, A.B.; Rahman, B.; Verron, E.; Badran, Z. Drug Delivery Systems in Regenerative Medicine: An Updated Review. Pharmaceutics 2023, 15, 695. [Google Scholar]
- Ramadon, D.; McCrudden, M.T.C.; Courtenay, A.J.; Donnelly, R.F. Enhancement strategies for transdermal drug delivery systems: Current trends and applications. Drug Deliv. Transl. Res. 2022, 12, 758–791. [Google Scholar]
- Mansoor, I.; Mohammed, K.H.A.; El-Fattah, M.A.A.; Abdo, M.H.; Rashad, E.; Eassa, H.A.; Saleh, A.; Amin, O.M.; Nounou, M.I.; Ghoneim, O. Microneedle-based vaccine delivery: Review of an emerging technology. Aaps Pharmscitech 2022, 23, 103. [Google Scholar]
- Moore, E.M.; Maestas, D.R.; Comeau, H.Y.; Elisseeff, J.H. The immune system and its contribution to variability in regenerative medicine. Tissue Eng. Part B Rev. 2021, 27, 39–47. [Google Scholar]
- Panda, P.K.; Fahrner, A.; Vats, S.; Seranova, E.; Sharma, V.; Chipara, M.; Desai, P.; Torresi, J.; Rosenstock, T.; Kumar, D.; et al. Chemical screening approaches enabling drug discovery of autophagy modulators for biomedical applications in human diseases. Front. Cell Dev. Biol. 2019, 7, 38. [Google Scholar]
- Vacanti, J.P.; Otte, J.B.; Wertheim, J.A. Introduction: Regenerative medicine and solid organ transplantation from a historical perspective. In Regenerative Medicine Applications in Organ Transplantation; Orlando, G., Lerut, J., Soker, S., Stratta, R.J., Eds.; Academic Press: Cambridge, MA, USA, 2014; pp. 1–15. [Google Scholar] [CrossRef]
- Mao, A.S.; Mooney, D.J. Regenerative medicine: Current therapies and future directions. Proc. Natl. Acad. Sci. USA 2015, 112, 14452–14459. [Google Scholar]
- Tonti, O.R.; Larson, H.; Lipp, S.N.; Luetkemeyer, C.M.; Makam, M.; Vargas, D.; Wilcox, S.M.; Calve, S. Tissue-specific parameters for the design of ECM-mimetic biomaterials. Acta Biomater. 2021, 132, 83–102. [Google Scholar] [PubMed]
- Tabata, Y. Current status of regenerative medical therapy based on drug delivery technology. Reprod. Biomed. Online 2008, 16, 70–80. [Google Scholar] [PubMed]
- Xing, H.; Lee, H.; Luo, L.; Kyriakides, T.R. Extracellular matrix-derived biomaterials in engineering cell function. Biotechnol. Adv. 2020, 42, 107421. [Google Scholar]
- Urbanczyk, M.; Layland, S.L.; Schenke-Layland, K. The role of extracellular matrix in biomechanics and its impact on bioengineering of cells and 3D tissues. Matrix Biol. 2020, 85, 1–14. [Google Scholar]
- Liang, R.; Yang, G.; Kim, K.E.; D’Amore, A.; Pickering, A.N.; Zhang, C.; Woo, S.L. Positive effects of an extracellular matrix hydrogel on rat anterior cruciate ligament fibroblast proliferation and collagen mRNA expression. J. Orthop. Transl. 2015, 3, 114–122. [Google Scholar]
- Grover, C.N.; Cameron, R.E.; Best, S.M. Investigating the morphological, mechanical and degradation properties of scaffolds comprising collagen, gelatin and elastin for use in soft tissue engineering. J. Mech. Behav. Biomed. Mater. 2012, 10, 62–74. [Google Scholar]
- Young, D.A.; Bajaj, V.; Christman, K.L. Decellularized adipose matrix hydrogels stimulate in vivo neovascularization and adipose formation. J. Biomed. Mater. Research. Part. A 2014, 102, 1641–1651. [Google Scholar] [CrossRef]
- Shroff, G.; Gupta, R. Human embryonic stem cells in the treatment of patients with spinal cord injury. Ann. Neurosci. 2015, 22, 208. [Google Scholar]
- Calabrese, E.J. Hormesis and embryonic stem cells. Chem. -Biol. Interact. 2022, 352, 109783. [Google Scholar] [CrossRef] [PubMed]
- Hyun, I. The bioethics of stem cell research and therapy. J. Clin. Investig. 2010, 120, 71–75. [Google Scholar] [PubMed]
- Calabrese, E.J. Hormesis and adult adipose-derived stem cells. Pharmacol. Res. 2021, 172, 105803. [Google Scholar] [PubMed]
- Calabrese, E.J. Hormesis and bone marrow stem cells: Enhancing cell proliferation, differentiation and resilience to inflammatory stress. Chem.-Biol. Interact. 2022, 351, 109730. [Google Scholar]
- Cable, J.; Fuchs, E.; Weissman, I.; Jasper, H.; Glass, D.; Rando, T.A.; Blau, H.; Debnath, S.; Oliva, A.; Park, S.; et al. Adult stem cells and regenerative medicine- a symposium report. Ann. N. Y. Acad. Sci. 2020, 1462, 27–36. [Google Scholar]
- Oringanje, C.; Nemecek, E.; Oniyangi, O. Hematopoietic stem cell transplantation for people with sickle cell disease. Cochrane Database Syst. Rev. 2020, 7, CD007001. [Google Scholar] [CrossRef]
- Takahashi, K.; Yamanaka, S. Induction of pluripotent stem cells from mouse embryonic and adult fibroblast cultures by defined factors. Cell 2006, 126, 663–676. [Google Scholar] [CrossRef]
- Takahashi, K.; Tanabe, K.; Ohnuki, M.; Narita, M.; Ichisaka, T.; Tomoda, K.; Yamanaka, S. Induction of pluripotent stem cells from adult human fibroblasts by defined factors. Cell 2007, 131, 861–872. [Google Scholar] [CrossRef]
- Thanaskody, K.; Jusop, A.S.; Tye, G.J.; Wan, K.; Zaman, W.S.; Dass, S.A.; Nordin, F. MSCs vs. iPSCs: Potential in therapeutic applications. Front. Cell Dev. Biol. 2022, 10, 1005926. [Google Scholar]
- Rowe, R.G.; Daley, G.Q. Induced pluripotent stem cells in disease modelling and drug discovery. Nat. Rev. Genet. 2019, 20, 377–388. [Google Scholar] [PubMed]
- Fernandes, T.G.; Rodrigues, C.A.; Diogo, M.M.; Cabral, J.M. Stem cell bioprocessing for regenerative medicine. J. Chem. Technol. Biotechnol. 2014, 89, 34–47. [Google Scholar]
- Wang, Y.; Tang, Z.; Gu, P. Stem/progenitor cell-based transplantation for retinal degeneration: A review of clinical trials. Cell Death Dis. 2020, 11, 793. [Google Scholar] [PubMed]
- Mao, J.; Saiding, Q.; Qian, S.; Liu, Z.; Zhao, B.; Zhao, Q.; Lu, B.; Mao, X.; Zhang, L.; Zhang, Y.; et al. Reprogramming stem cells in regenerative medicine. Smart Med. 2022, 1, e20220005. [Google Scholar]
- Rossi, F.; Noren, H.; Jove, R.; Beljanski, V.; Grinnemo, K.H. Differences and similarities between cancer and somatic stem cells: Therapeutic implications. Stem Cell Res. Ther. 2020, 11, 489. [Google Scholar]
- Sur, D.; Havasi, A.; Cainap, C.; Samasca, G.; Burz, C.; Balacescu, O.; Lupan, I.; Deleanu, D.; Irimie, A. Chimeric antigen receptor T-cell therapy for colorectal cancer. J. Clin. Med. 2020, 9, 182. [Google Scholar] [CrossRef]
- Najafi, S.; Mortezaee, K. Advances in dendritic cell vaccination therapy of cancer. Biomed. Pharmacother. 2023, 164, 114954. [Google Scholar]
- Dang, B.T.N.; Kwon, T.K.; Lee, S.; Jeong, J.H.; Yook, S. Nanoparticle-based immunoengineering strategies for enhancing cancer immunotherapy. J. Control. Release 2024, 365, 773–800. [Google Scholar]
- Dudley, A.C.; Griffioen, A.W. Pathological angiogenesis: Mechanisms and therapeutic strategies. Angiogenesis 2023, 26, 313–347. [Google Scholar]
- Custodia, A.; Ouro, A.; Romaus-Sanjurjo, D.; Pías-Peleteiro, J.M.; de Vries, H.E.; Castillo, J.; Sobrino, T. Endothelial progenitor cells and vascular alterations in Alzheimer’s disease. Front. Aging Neurosci. 2022, 13, 811210. [Google Scholar]
- Al-Zoubi, M.S.; Al-Zoubi, R.M. Nanomedicine tactics in cancer treatment: Challenge and hope. Crit. Rev. Oncol. Hematol. 2022, 174, 103677. [Google Scholar] [PubMed]
- Aghda, N.H.; Dabbaghianamiri, M.; Tunnell, J.W.; Betancourt, T. Design of smart nanomedicines for effective cancer treatment. Int. J. Pharm. 2022, 621, 121791. [Google Scholar]
- de Lázaro, I.; Mooney, D.J. Obstacles and opportunities in a forward vision for cancer nanomedicine. Nat. Mater. 2021, 20, 1469–1479. [Google Scholar]
- Mardones, R.; Jofré, C.M.; Minguell, J.J. Cell therapy and tissue engineering approaches for cartilage repair and/or regeneration. Int. J. Stem Cells 2015, 8, 48–53. [Google Scholar]
- Salhotra, A.; Shah, H.N.; Levi, B.; Longaker, M.T. Mechanisms of bone development and repair. Nat. Rev. Mol. Cell Biol. 2020, 21, 696–711. [Google Scholar]
- Judson, R.N.; Rossi, F.M. Towards stem cell therapies for skeletal muscle repair. NPJ Regen. Med. 2020, 5, 10. [Google Scholar]
- Zhao, S.; Chen, J.; Wu, L.; Tao, X.; Yaqub, N.; Chang, J. Induced Pluripotent Stem Cells for Tissue-Engineered Skeletal Muscles. Int. J. Mol. Sci. 2023, 24, 11520. [Google Scholar] [CrossRef]
- Atala, A.; Lanza, R.; Mikos, T.; Nerem, R. (Eds.) Principles of Regenerative Medicine; Academic press: Cambridge, MA, USA, 2018. [Google Scholar]
- Bashor, C.J.; Hilton, I.B.; Bandukwala, H.; Smith, D.M.; Veiseh, O. Engineering the next generation of cell-based therapeutics. Nat. Rev. Drug Discov. 2022, 21, 655–675. [Google Scholar]
- De Pieri, A.; Rochev, Y.; Zeugolis, D.I. Scaffold-free cell-based tissue engineering therapies: Advances, shortfalls and forecast. NPJ Regen. Med. 2021, 6, 18. [Google Scholar]
- Yu, J.; Park, S.A.; Kim, W.D.; Ha, T.; Xin, Y.Z.; Lee, J.; Lee, D. Current advances in 3D bioprinting technology and its applications for tissue engineering. Polymers 2020, 12, 2958. [Google Scholar] [CrossRef] [PubMed]
- He, D.; Li, H. Biomaterials affect cell-cell interactions in vitro in tissue engineering. J. Mater. Sci. Technol. 2021, 63, 62–72. [Google Scholar] [CrossRef]
- Tan, S.; Yang, J.; Hu, S.; Lei, W. Cell-cell interactions in the heart: Advanced cardiac models and omics technologies. Stem Cell Res. Ther. 2024, 15, 362. [Google Scholar] [CrossRef]
- Yang, J.; Yamato, M.; Nishida, K.; Ohki, T.; Kanzaki, M.; Sekine, H.; Shimizu, T.; Okano, T. Cell delivery in regenerative medicine: The cell sheet engineering approach. J. Control. Release 2006, 116, 193–203. [Google Scholar] [CrossRef] [PubMed]
- de la Torre, P.; Pérez-Lorenzo, M.J.; Alcázar-Garrido, Á.; Flores, A.I. Cell-based nanoparticles delivery systems for targeted cancer therapy: Lessons from anti-angiogenesis treatments. Molecules 2020, 25, 715. [Google Scholar] [CrossRef] [PubMed]
- de Kanter, A.-F.J.; Jongsma, K.R.; Verhaar, M.C.; Bredenoord, A.L. The Ethical Implications of Tissue Engineering for Regenerative Purposes: A Systematic Review. Tissue Eng. Part. B Rev. 2023, 29, 167–187. [Google Scholar] [CrossRef]
- Pontrelli, G.; Toniolo, G.; McGinty, S.; Peri, D.; Succi, S.; Chatgilialoglu, C. Mathematical modelling of drug delivery from pH-responsive nanocontainers. Comput. Biol. Med. 2021, 131, 104238. [Google Scholar] [CrossRef]
- Berten-Schunk, L.; Roger, Y.; Bunjes, H.; Hoffmann, A. Release of TGF-β3 from Surface-Modified PCL Fiber Mats Triggers a Dose-Dependent Chondrogenic Differentiation of Human Mesenchymal Stromal Cells. Pharmaceutics 2023, 15, 1303. [Google Scholar] [CrossRef]
- Makadia, H.K.; Siegel, S.J. Poly lactic-co-glycolic acid (PLGA) as biodegradable controlled drug delivery carrier. Polymers 2011, 3, 1377–1397. [Google Scholar] [CrossRef]
- Danhier, F.; Ansorena, E.; Silva, J.M.; Coco, R.; Le Breton, A.; Préat, V. PLGA-based nanoparticles: An overview of biomedical applications. J. Control. Release 2012, 161, 505–522. [Google Scholar] [CrossRef]
- Perinelli, D.R.; Cespi, M.; Bonacucina, G.; Palmieri, G.F. PEGylated polylactide (PLA) and poly (lactic-co-glycolic acid) (PLGA) copolymers for the design of drug delivery systems. J. Pharm. Investig. 2019, 49, 443–458. [Google Scholar]
- Gallo, N.; Quarta, S.; Massaro, M.; Carluccio, M.A.; Barca, A.; Cannoletta, D.; Siculella, L.; Salvatore, L.; Sannino, A. Development of L-Lysine-Loaded PLGA Microparticles as a Controlled Release System for Angiogenesis Enhancement. Pharmaceutics 2023, 15, 479. [Google Scholar] [CrossRef] [PubMed]
- Verron, E. Innovative Drug Delivery Systems for Regenerative Medicine. Pharmaceutics 2024, 16, 295. [Google Scholar] [CrossRef] [PubMed]
- Levy, J.A.; Straker, M.A.; Stine, J.M.; Beardslee, L.A.; Ghodssi, R. Magnetically Triggered Ingestible Capsule for Localized Microneedle Drug Delivery. Device 2024, 2. [Google Scholar] [CrossRef]
- Zhou, X.; He, X.; Shi, K.; Yuan, L.; Yang, Y.; Liu, Q.; Ming, Y.; Yi, C.; Qian, Z. Injectable Thermosensitive Hydrogel Containing Erlotinib-Loaded Hollow Mesoporous Silica Nanoparticles as a Localized Drug Delivery System for NSCLC Therapy. Adv. Sci. 2020, 7, 2001442. [Google Scholar]
- Hu, J.; Quan, Y.; Lai, Y.; Zheng, Z.; Hu, Z.; Wang, X.; Dai, T.; Zhang, Q.; Cheng, Y.A. Smart aminoglycoside hydrogel with tunable gel degradation, on-demand drug release, and high antibacterial activity. J. Control. Release 2017, 247, 145–152. [Google Scholar] [PubMed]
- Liang, J.; Ling, J.; Sun, D.; Wu, G.; Ouyang, X.K.; Wang, N.; Yang, G. Dextran-Based Antibacterial Hydrogel Dressings for Accelerating Infected Wound Healing by Reducing Inflammation Levels. Adv. Healthc. Mater. 2024, 13, 2400494. [Google Scholar]
- Censi, R.; Di Martino, P.; Vermonden, T.; Hennink, W.E. Hydrogels for protein delivery in tissue engineering. J. Control. Release 2012, 161, 680–692. [Google Scholar]
- Vilas-Boas, V.; Espiña, B.; Kolen’ko, Y.V.; Bañobre-López, M.; Brito, M.; Martins, V.; Duarte, J.A.; Petrovykh, D.Y.; Freitas, P.; Carvalho, F. Effectiveness and Safety of a Nontargeted Boost for a CXCR4-Targeted Magnetic Hyperthermia Treatment of Cancer Cells. ACS Omega 2019, 4, 1931–1940. [Google Scholar]
- Nica, V.; Marino, A.; Pucci, C.; Şen, Ö.; Emanet, M.; De Pasquale, D.; Carmignani, A.; Petretto, A.; Bartolucci, M.; Lauciello, S.; et al. Cell-Membrane-Coated and Cell-Penetrating Peptide-Conjugated Trimagnetic Nanoparticles for Targeted Magnetic Hyperthermia of Prostate Cancer Cells. ACS Appl. Mater. Interfaces 2023, 15, 30008–30028. [Google Scholar]
- Peng, W.; Datta, P.; Ayan, B.; Ozbolat, V.; Sosnoski, D.; Ozbolat, I.T. 3D Bioprinting for Drug Discovery and Development in Pharmaceutics. Acta Biomater. 2017, 57, 26–46. [Google Scholar]
- Hagenbuchner, J.; Nothdurfter, D.; Ausserlechner, M.J. 3D Bioprinting: Novel Approaches for Engineering Complex Human Tissue Equivalents and Drug Testing. Essays Biochem. 2021, 65, 417–427. [Google Scholar] [PubMed]
- Han, S.; Kim, S.; Chen, Z.; Shin, H.K.; Lee, S.Y.; Moon, H.E.; Paek, S.H.; Park, S. 3D Bioprinted Vascularized Tumour for Drug Testing. Int. J. Mol. Sci. 2020, 21, 2993. [Google Scholar] [CrossRef]
- Yao, Z.; Feng, X.; Wang, Z.; Zhan, Y.; Wu, X.; Xie, W.; Wang, Z.; Zhang, G. Techniques and Applications in 3D Bioprinting with Chitosan Bio-Inks for Drug Delivery: A Review. Int. J. Biol. Macromol. 2024, 278 Pt 4, 134752. [Google Scholar] [CrossRef] [PubMed]
- Lazaridou, M.; Bikiaris, D.N.; Lamprou, D.A. 3D Bioprinted Chitosan-Based Hydrogel Scaffolds in Tissue Engineering and Localised Drug Delivery. Pharmaceutics 2022, 14, 1978. [Google Scholar] [CrossRef] [PubMed]
- Intini, C.; Elviri, L.; Cabral, J.; Mros, S.; Bergonzi, C.; Bianchera, A.; Flammini, L.; Govoni, P.; Barocelli, E.; Bettini, R.; et al. 3D-Printed Chitosan-Based Scaffolds: An In Vitro Study of Human Skin Cell Growth and an In Vivo Wound Healing Evaluation in Experimental Diabetes in Rats. Carbohydr. Polym. 2018, 199, 593–602. [Google Scholar]
- Hafezi, F.; Shorter, S.; Tabriz, A.G.; Hurt, A.; Elmes, V.; Boateng, J.; Douroumis, D. Bioprinting and Preliminary Testing of Highly Reproducible Novel Bioink for Potential Skin Regeneration. Pharmaceutics 2020, 12, 550. [Google Scholar] [CrossRef]
- Haj-Ahmad, R.; Rasekh, M.; Nazari, K.; Li, Y.; Fu, Y.; Li, B.; Zhang, Q.; Xia, Z.; Liu, H.; Gu, T.; et al. EHDA Spraying: A Multi-Material Nano-Engineering Route. Curr. Pharm. Des. 2015, 21, 3239–3247. [Google Scholar]
- Ahmad, Z.; Nangrejo, M.; Rasekh, M.; Stride, E.; Edirisinghe, M. Novel Electrically Driven Direct-Writing Methods with Managed Control on In-Situ Shape and Encapsulation Polymer Forming. Int. J. Mater. Form. 2013, 6, 281–288. [Google Scholar]
- Haj-Ahmad, R.; Rasekh, M.; Nazari, K.; Onaiwu, E.V.; Yousef, B.; Morgan, S.; Evans, D.; Chang, M.W.; Hall, J.; Samwell, C.; et al. Stable Increased Formulation Atomization Using a Multi-Tip Nozzle Device. Drug Deliv. Transl. Res. 2018, 8, 1815–1827. [Google Scholar] [CrossRef]
- Rasekh, M.; Smith, A.; Arshad, M.S.; Gunduz, O.; Van der Merwe, S.M.; Smith, G.; Ahmad, Z. Electrohydrodynamic Preparation of Nanomedicines. Curr. Top. Med. Chem. 2015, 15, 2316–2327. [Google Scholar]
- Rasekh, M.; Nazari, K.; Arshad, M.S.; Kucuk, I.; Haj-Ahmad, R.; Hussain, A.; Morris, M.A.; Abbas, N.; Chang, M.W.; Li, X.; et al. Polymeric-Based Therapeutic Delivery Systems Prepared Using Electrohydrodynamic Processes. Curr. Pharm. Des. 2016, 22, 2873–2885. [Google Scholar] [PubMed]
- Ali, A.; Zafar, S.; Rasekh, M.; Chohan, T.A.; Pisapia, F.; Singh, N.; Qutachi, O.; Arshad, M.S.; Ahmad, Z. An Adaptive Approach in Polymer-Drug Nanoparticle Engineering Using Slanted Electrohydrodynamic Needles and Horizontal Spraying Planes. AAPS PharmSciTech 2024, 25, 1–22. [Google Scholar]
- Zhang, Y.S.; Yue, K.; Aleman, J.; Mollazadeh-Moghaddam, K.; Bakht, S.M.; Yang, J.; Jia, W.; Dell’Erba, V.; Assawes, P.; Shin, S.R.; et al. 3D bioprinting for tissue and organ fabrication. Ann. Biomed. Eng. 2017, 45, 148–163. [Google Scholar] [PubMed]
- Gupta, D.; Negi, N.P. 3D bioprinting: Printing the future and recent advances. Bioprinting 2022, 27, e00211. [Google Scholar]
- Ding, Z.; Tang, N.; Huang, J.; Cao, X.; Wu, S. Global hotspots and emerging trends in 3D bioprinting research. Front. Bioeng. Biotechnol. 2023, 11, 1169893. [Google Scholar]
- Hospodiuk, M.; Dey, M.; Sosnoski, D.; Ozbolat, I.T. The bioink: A comprehensive review on bioprintable materials. Biotechnol. Adv. 2017, 35, 217–239. [Google Scholar]
- Hong, N.; Yang, G.H.; Lee, J.; Kim, G. 3D Bioprinting and Its In Vivo Applications. J. Biomed. Mater. Res. B Appl. Biomater. 2018, 106, 444–459. [Google Scholar]
- Liu, L.; Zhou, X.; Xu, Y.; Zhang, W.; Liu, C.H.; Wang, X. Controlled Release of Growth Factors for Regenerative Medicine. Curr. Pharm. Des. 2015, 21, 1627–1632. [Google Scholar]
- Krishna, L.; Dhamodaran, K.; Jayadev, C.; Chatterjee, K.; Shetty, R.; Khora, S.S.; Das, D. Nanostructured Scaffold as a Determinant of Stem Cell Fate. Stem Cell Res. Ther. 2016, 7, 188. [Google Scholar]
- Shrestha, S.; Banstola, A.; Jeong, J.H.; Seo, J.H.; Yook, S. Targeting Cancer Stem Cells: Therapeutic and Diagnostic Strategies by the Virtue of Nanoparticles. J. Control. Release 2022, 348, 518–536. [Google Scholar]
- Pacelli, S.; Basu, S.; Whitlow, J.; Chakravarti, A.; Acosta, F.; Varshney, A.; Modaresi, S.; Berkland, C.; Paul, A. Strategies to Develop Endogenous Stem Cell-Recruiting Bioactive Materials for Tissue Repair and Regeneration. Adv. Drug Deliv. Rev. 2017, 120, 50–70. [Google Scholar]
- Zhao, C.; Tan, A.; Pastorin, G.; Ho, H.K. Nanomaterial Scaffolds for Stem Cell Proliferation and Differentiation in Tissue Engineering. Biotechnol. Adv. 2013, 31, 654–668. [Google Scholar]
- Kashkooli, F.M.; Soltani, M.; Souri, M. Controlled Anti-Cancer Drug Release Through Advanced Nano-Drug Delivery Systems: Static and Dynamic Targeting Strategies. J. Control. Release 2020, 327, 316–349. [Google Scholar]
- Wang, Z.; Yang, L. Natural-product-based, carrier-free, noncovalent nanoparticles for tumor chemo-photodynamic combination therapy. Pharmacol. Res. 2024, 203, 107150. [Google Scholar] [PubMed]
- Cai, S.S.; Li, T.; Akinade, T.; Zhu, Y.; Leong, K.W. Drug delivery carriers with therapeutic functions. Adv. Drug Deliv. Rev. 2021, 176, 113884. [Google Scholar]
- Yu, T.; Li, Y.; Gu, X.; Li, Q. Development of a Hyaluronic Acid-Based Nanocarrier Incorporating Doxorubicin and Cisplatin as a pH-Sensitive and CD44-Targeted Anti-Breast Cancer Drug Delivery System. Front. Pharmacol. 2020, 11, 532457. [Google Scholar]
- Sefidgar, M.; Soltani, M.; Raahemifar, K.; Sadeghi, M.; Bazmara, H.; Bazargan, M.; Naeenian, M.M. Numerical Modeling of Drug Delivery in a Dynamic Solid Tumor Microvasculature. Microvasc. Res. 2015, 99, 43–56. [Google Scholar]
- Yahya, I.; Atif, R.; Ahmed, L.; Eldeen, T.S.; Omara, A.; Eltayeb, M. Polymeric Nanoparticles as Drug Delivery Systems for Controlled Release. Adv. Sci. Eng. Med. 2020, 12, 263–270. [Google Scholar]
- Viswanadha, L.S.; Arcot, Y.; Lin, Y.T.; Akbulut, M.E. A Comparative Investigation of Release Kinetics of Paclitaxel from Natural Protein and Macromolecular Nanocarriers in Nanoscale Drug Delivery Systems. JCIS Open 2024, 15, 100120. [Google Scholar]
- Atiyah, N.A.; Albayati, T.M.; Atiya, M.A. Interaction Behavior of Curcumin Encapsulated onto Functionalized SBA-15 as an Efficient Carrier and Release in Drug Delivery. J. Mol. Struct. 2022, 1260, 132879. [Google Scholar] [CrossRef]
- Son, G.H.; Lee, B.J.; Cho, C.W. Mechanisms of Drug Release from Advanced Drug Formulations Such as Polymeric-Based Drug-Delivery Systems and Lipid Nanoparticles. J. Pharm. Investig. 2017, 47, 287–296. [Google Scholar] [CrossRef]
- Lisik, A.; Musiał, W. Conductomeric Evaluation of the Release Kinetics of Active Substances from Pharmaceutical Preparations Containing Iron Ions. Materials 2019, 12, 730. [Google Scholar] [CrossRef] [PubMed]
- Mircioiu, C.; Voicu, V.; Anuta, V.; Tudose, A.; Celia, C.; Paolino, D.; Fresta, M.; Sandulovici, R.; Mircioiu, I. Mathematical Modeling of Release Kinetics from Supramolecular Drug Delivery Systems. Pharmaceutics 2019, 11, 140. [Google Scholar] [CrossRef]
- Jennings, C.L.; Perry, E.K.; Dziubla, T.D.; Puleo, D.A. Sequential Release of Multiple Drugs from Flexible Drug Delivery Films. Int. J. Polym. Mater. Polym. Biomater. 2017, 66, 569–576. [Google Scholar] [CrossRef]
- Dreiss, C.A. Hydrogel Design Strategies for Drug Delivery. Curr. Opin. Colloid. Interface Sci. 2020, 48, 1–17. [Google Scholar] [CrossRef]
- Blanco, E.; Shen, H.; Ferrari, M. Principles of Nanoparticle Design for Overcoming Biological Barriers to Drug Delivery. Nat. Biotechnol. 2015, 33, 941–951. [Google Scholar] [PubMed]
- Ravichandiran, V.; Kesharwani, A.; Bhaskaran, M.; Parihar, V.K.; Bakhshi, S.; Velayutham, R.; Kumarasamy, M. Overcoming Biological Barriers: Precision Engineered Extracellular Vesicles for Personalized Neuromedicine. Precis. Med. Eng. 2024, 1, 100010. [Google Scholar]
- Kardani, S.L. Nanocarrier-Based Formulations: Regulatory Challenges, Ethical and Safety Considerations in Pharmaceuticals. Asian J. Pharm. (AJP) 2024, 18, 346. [Google Scholar] [CrossRef]
- Patel, M.; Patel, R.; Rai, M. Nanomedicines: Applications and Toxicological Concerns. Nanotechnol. Med. Toxic. Saf. 2021, 1, 1–28. [Google Scholar]
- Zhao, F.; Wang, J.; Zhang, Y.; Hu, J.; Li, C.; Liu, S.; Li, R.; Du, R. In vivo Fate of Targeted Drug Delivery Carriers. Int. J. Nanomed. 2024, 19, 6895–6929. [Google Scholar]
- Gaballa, S.A.; Naguib, Y.; Mady, F.M.; Khaled, K.A. Polyethylene glycol: Properties, applications, and challenges. J. Adv. Biomed. Pharm. Sci. 2024, 7, 26–36. [Google Scholar]
- Park, K.; Skidmore, S.; Hadar, J.; Garner, J.; Park, H.; Otte, A.; Soh, B.K.; Yoon, G.; Yu, D.; Yun, Y.; et al. Injectable, long-acting PLGA formulations: Analyzing PLGA and understanding microparticle formation. J. Control Release 2019, 304, 125–134. [Google Scholar]
- Salimi, M.; Sarkar, S.; Fathi, S.; Alizadeh, A.M.; Saber, R.; Moradi, F.; Delavari, H. Biodistribution, pharmacokinetics, and toxicity of dendrimer-coated iron oxide nanoparticles in BALB/c mice. Int. J. Nanomed. 2018, 13, 1483–1493. [Google Scholar]
- Moghaddam, S.P.H.; Mohammadpour, R.; Ghandehari, H. In vitro and in vivo evaluation of degradation, toxicity, biodistribution, and clearance of silica nanoparticles as a function of size, porosity, density, and composition. J. Control. Release 2019, 311, 1. [Google Scholar]
- Yang, G.; Phua, S.Z.F.; Bindra, A.K.; Zhao, Y. Degradability and clearance of inorganic nanoparticles for biomedical applications. Adv. Mater. 2019, 31, 1805730. [Google Scholar]
- Frantellizzi, V.; Conte, M.; Pontico, M.; Pani, A.; Pani, R.; De Vincentis, G. New frontiers in molecular imaging with superparamagnetic iron oxide nanoparticles (SPIONs): Efficacy, toxicity, and future applications. Nucl. Med. Mol. Imaging 2020, 54, 65–80. [Google Scholar]
- Klara, J.; Hinz, A.; Bzowska, M.; Horak, W.; Lewandowska-Łańcucka, J. In vitro/ex vivo evaluation of multifunctional collagen/chitosan/hyaluronic acid hydrogel-based alendronate delivery systems. Int. J. Biol. Macromol. 2024, 262, 130142. [Google Scholar]
- Assen, L.S.; Jongsma, K.R.; Isasi, R.; Tryfonidou, M.A.; Bredenoord, A.L. Roles and Responsibilities in Stem Cell Research: A Focus Group Study with Stem Cell Researchers and Patients. Regen. Med. 2022, 17, 445–459. [Google Scholar] [CrossRef]
- Qiu, T.; Hanna, E.; Dabbous, M.; Borislav, B.; Toumi, M. Regenerative medicine regulatory policies: A systematic review and international comparison. Health Policy 2020, 124, 701–713. [Google Scholar]
- Lam, E.H.Y.; Yu, F.; Zhu, S.; Wang, Z. 3D Bioprinting for Next-Generation Personalized Medicine. Int. J. Mol. Sci. 2023, 24, 6357. [Google Scholar] [CrossRef] [PubMed]
- Ho, D.; Quake, S.R.; McCabe, E.R.B.; Chng, W.J.; Chow, E.K.; Ding, X.; Gelb, B.D.; Ginsburg, G.S.; Hassenstab, J.; Ho, C.-M.; et al. Enabling Technologies for Personalized and Precision Medicine. Trends Biotechnol. 2020, 38, 497–518. [Google Scholar] [CrossRef] [PubMed]
- Gharibshahian, M.; Torkashvand, M.; Bavisi, M.; Aldaghi, N.; Alizadeh, A. Recent advances in artificial intelligent strategies for tissue engineering and regenerative medicine. Skin. Res. Technol. 2024, 30, e70016. [Google Scholar] [PubMed]
- Xing, F.; Xiang, Z.; Rommens, P.M.; Ritz, U. 3D Bioprinting for Vascularized Tissue-Engineered Bone Fabrication. Materials 2020, 13, 2278. [Google Scholar] [CrossRef]
- Guo, X.; Ma, Y.; Min, Y.; Sun, J.; Shi, X.; Gao, G.; Sun, L.; Wang, J. Progress and Prospect of Technical and Regulatory Challenges on Tissue-Engineered Cartilage as Therapeutic Combination Product. Bioact. Mater. 2023, 20, 501–518. [Google Scholar] [CrossRef]
- Diomede, F.; Gugliandolo, A.; Cardelli, P.; Merciaro, I.; Ettorre, V.; Traini, T.; Bedini, R.; Scionti, D.; Bramanti, A.; Nanci, A.; et al. Three-Dimensional Printed PLA Scaffold and Human Gingival Stem Cell-Derived Extracellular Vesicles: A New Tool for Bone Defect Repair. Stem Cell Res. Ther. 2018, 9, 104. [Google Scholar]
- Teixeira, B.N.; Aprile, P.; Mendonça, R.H.; Kelly, D.J.; Thiré, R.M.d.S.M. Evaluation of Bone Marrow Stem Cell Response to PLA Scaffolds Manufactured by 3D Printing and Coated with Polydopamine and Type I Collagen. J. Biomed. Mater. Res. B Appl. Biomater. 2019, 107, 37–49. [Google Scholar] [CrossRef]
- Wang, R.; Sun, M.; Wang, C.; Dong, A.; Zhang, J. A facile and versatile strategy for synthesis of dopamine-functionalized polymers. J. Polym. Sci. 2023, 61, 223–233. [Google Scholar] [CrossRef]
- Mezhuev, Y.O.; Varankin, A.V.; Luss, A.L.; Dyatlov, V.A.; Tsatsakis, A.M.; Shtilman, M.I.; Korshak, Y.V. Immobilization of dopamine on the copolymer of N-vinyl-2-pyrrolidone and allyl glycidyl ether and synthesis of new hydrogels. Polym. Int. 2020, 69, 1275–1282. [Google Scholar]
- Ge, Q.; Chen, Z.; Cheng, J.; Zhang, B.; Zhang, Y.F.; Li, H.; He, X.; Yuan, C.; Liu, J.; Magdassi, S.; et al. 3D printing of highly stretchable hydrogel with diverse UV curable polymers. Sci. Adv. 2021, 7, eaba4261. [Google Scholar] [CrossRef]
- Li, J.; Mooney, D.J. Designing hydrogels for controlled drug delivery. Nat. Rev. Mater. 2016, 1, 1–17. [Google Scholar]
- Steele, A.N.; Stapleton, L.M.; Farry, J.M.; Lucian, H.J.; Paulsen, M.J.; Eskandari, A.; Hironaka, C.E.; Thakore, A.D.; Wang, H.; Yu, A.C.; et al. A biocompatible therapeutic catheter-deliverable hydrogel for in situ tissue engineering. Adv. Healthc. Mater. 2019, 8, 1801147. [Google Scholar]
- Xia, Z.; Jin, S.; Ye, K. Tissue and organ 3D bioprinting. SLAS Technol. 2018, 23, 301–314. [Google Scholar] [PubMed]
- Mirshafiei, M.; Rashedi, H.; Yazdian, F.; Rahdar, A.; Baino, F. Advancements in tissue and organ 3D bioprinting: Current techniques, applications, and future perspectives. Mater. Des. 2024, 240, 112853. [Google Scholar]
- Lind, J.U.; Busbee, T.A.; Valentine, A.D.; Pasqualini, F.S.; Yuan, H.; Yadid, M.; Park, S.J.; Kotikian, A.; Nesmith, A.P.; Campbell, P.H.; et al. Instrumented cardiac microphysiological devices via multimaterial three-dimensional printing. Nat. Mater. 2017, 16, 303–308. [Google Scholar]
- Lee, A.R.H.A.; Hudson, A.R.; Shiwarski, D.J.; Tashman, J.W.; Hinton, T.J.; Yerneni, S.; Bliley, J.M.; Campbell, P.G.; Feinberg, A.W. 3D bioprinting of collagen to rebuild components of the human heart. Science 2019, 365, 482–487. [Google Scholar]
- Liu, J.; He, J.; Liu, J.; Ma, X.; Chen, Q.; Lawrence, N.; Zhu, W.; Xu, Y.; Chen, S. Rapid 3D bioprinting of in vitro cardiac tissue models using human embryonic stem cell-derived cardiomyocytes. Bioprinting 2019, 13, e00040. [Google Scholar]
- Khanna, A.; Ayan, B.; Undieh, A.A.; Yang, Y.P.; Huang, N.F. Advances in three-dimensional bioprinted stem cell-based tissue engineering for cardiovascular regeneration. J. Mol. Cell. Cardiol. 2022, 169, 13–27. [Google Scholar]
- Ma, W.C.; Lee, J.M.; An, J.; Yeong, W.Y. 3D printing in triggered drug delivery devices: A review. Biomed. Mater. Devices 2023, 1, 720–730. [Google Scholar]
- Rahimnejad, M.; Labonte-Dupuis, T.; Demarquette, N.R.; Lerouge, S. A rheological approach to assess the printability of thermosensitive chitosan-based biomaterial inks. Biomed. Mater. 2020, 16, 015003. [Google Scholar]





| Material | Toxicity Concerns | Metabolic Degradation Pathway | Reference |
|---|---|---|---|
| Liposomes | Mild immunogenicity, potential for allergic reactions | Enzymatic breakdown by phospholipases | [123] |
| Polyethylene Glycol (PEG) | Accumulation concerns, potential hypersensitivity reactions | Renal clearance (low MW) or liver metabolism (high MW) | [124] |
| Chitosan | Low toxicity; may trigger mild immune responses | Degraded by lysozyme and excreted via urine | [123] |
| Poly (lactic-co-glycolic acid) (PLGA) | Minimal toxicity, risk of acidic degradation byproducts | Hydrolyzed into lactic and glycolic acid, metabolized by liver | [125] |
| Dendrimers | Cytotoxicity, at high concentrations, affects cell membranes | Renal clearance for low MW, hepatic metabolism for high MW | [126] |
| Silica Nanoparticles | Potential oxidative stress, long-term accumulation risks | Partial degradation in lysosomes, excretion in urine | [127] |
| Gold Nanoparticles | Long-term retention in tissues, concerns over chronic toxicity | Minimal biodegradation, excreted slowly via the hepatobiliary route | [128] |
| Superparamagnetic Iron Oxide Nanoparticles (SPIONs) | Oxidative stress, potential liver accumulation | Degraded by lysosomes and cleared by macrophages | [126,129] |
| Hydrogels (e.g., alginate, collagen, hyaluronic acid) | Generally biocompatible, rare allergic reactions | Enzymatic degradation (e.g., collagenase, hyaluronidase) | [130] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rasekh, M.; Arshad, M.S.; Ahmad, Z. Advances in Drug Delivery Integrated with Regenerative Medicine: Innovations, Challenges, and Future Frontiers. Pharmaceutics 2025, 17, 456. https://doi.org/10.3390/pharmaceutics17040456
Rasekh M, Arshad MS, Ahmad Z. Advances in Drug Delivery Integrated with Regenerative Medicine: Innovations, Challenges, and Future Frontiers. Pharmaceutics. 2025; 17(4):456. https://doi.org/10.3390/pharmaceutics17040456
Chicago/Turabian StyleRasekh, Manoochehr, Muhammad Sohail Arshad, and Zeeshan Ahmad. 2025. "Advances in Drug Delivery Integrated with Regenerative Medicine: Innovations, Challenges, and Future Frontiers" Pharmaceutics 17, no. 4: 456. https://doi.org/10.3390/pharmaceutics17040456
APA StyleRasekh, M., Arshad, M. S., & Ahmad, Z. (2025). Advances in Drug Delivery Integrated with Regenerative Medicine: Innovations, Challenges, and Future Frontiers. Pharmaceutics, 17(4), 456. https://doi.org/10.3390/pharmaceutics17040456