
Expanded Spectrum and Increased Incidence of Adverse Events Linked to COVID-19 Genetic Vaccines: New Concepts on Prophylactic Immuno-Gene Therapy, Iatrogenic Orphan Disease, and Platform-Inherent Challenges


Abstract
1. Introduction
2. The “Special Interest” Symptoms of Post-Vaccination Syndrome and Public Reaction
3. The Unique Features of mRNA Vaccines and Their Adverse Effects
4. Prevalence and Incidence of Adverse Events Caused by mRNA-LNP Vaccines: Inconsistent Statistics
5. Comparison of mRNA-LNP and Flu Vaccines
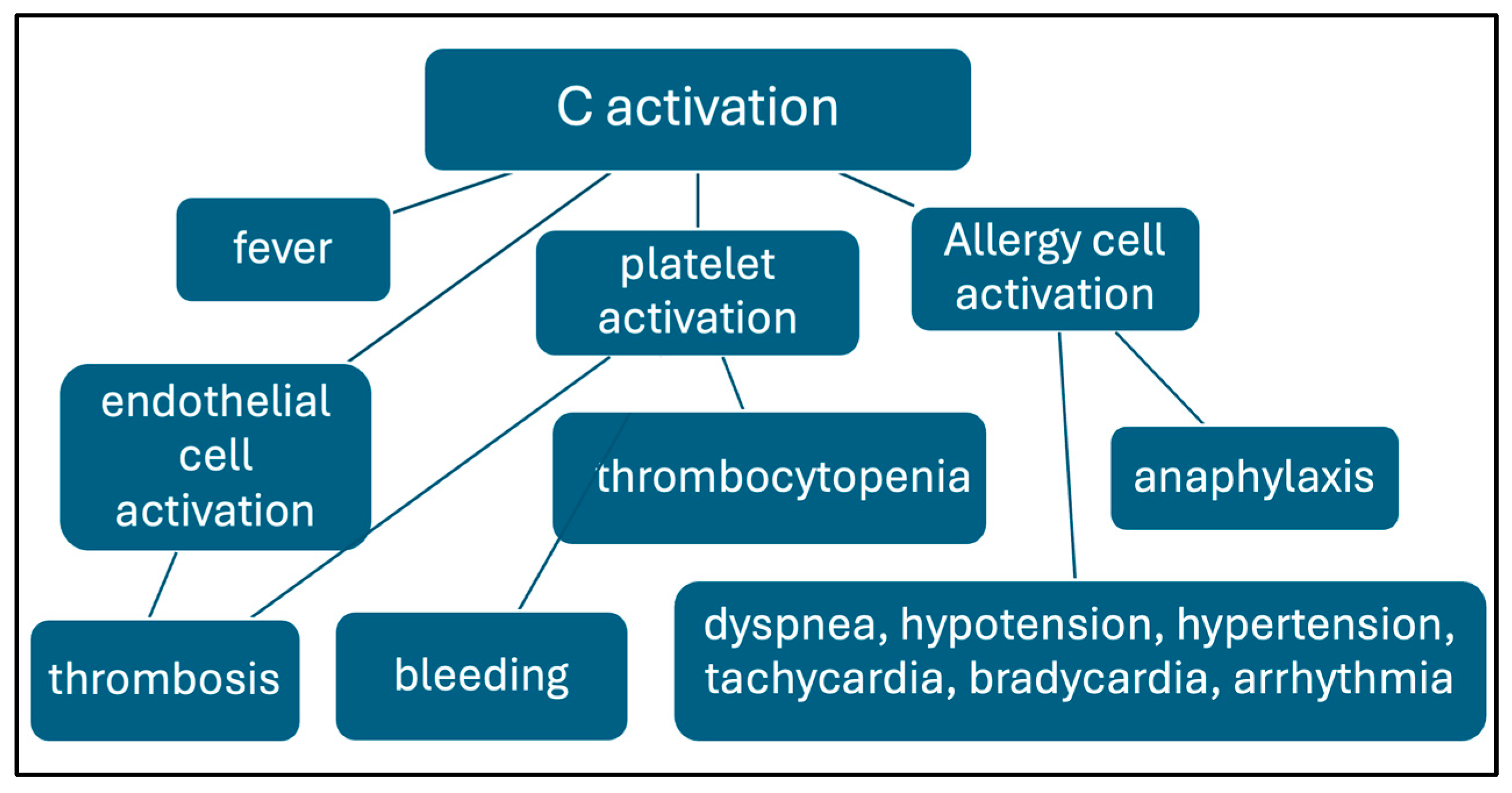
6. Complement Activation as a Possible Contributor to Acute AEs
7. Regulatory Classification of mRNA Vaccines
8. The Orphan Disease Proposition for Categorizing Persistent and/or Disabling Vaccine-Induced Chronic AEs
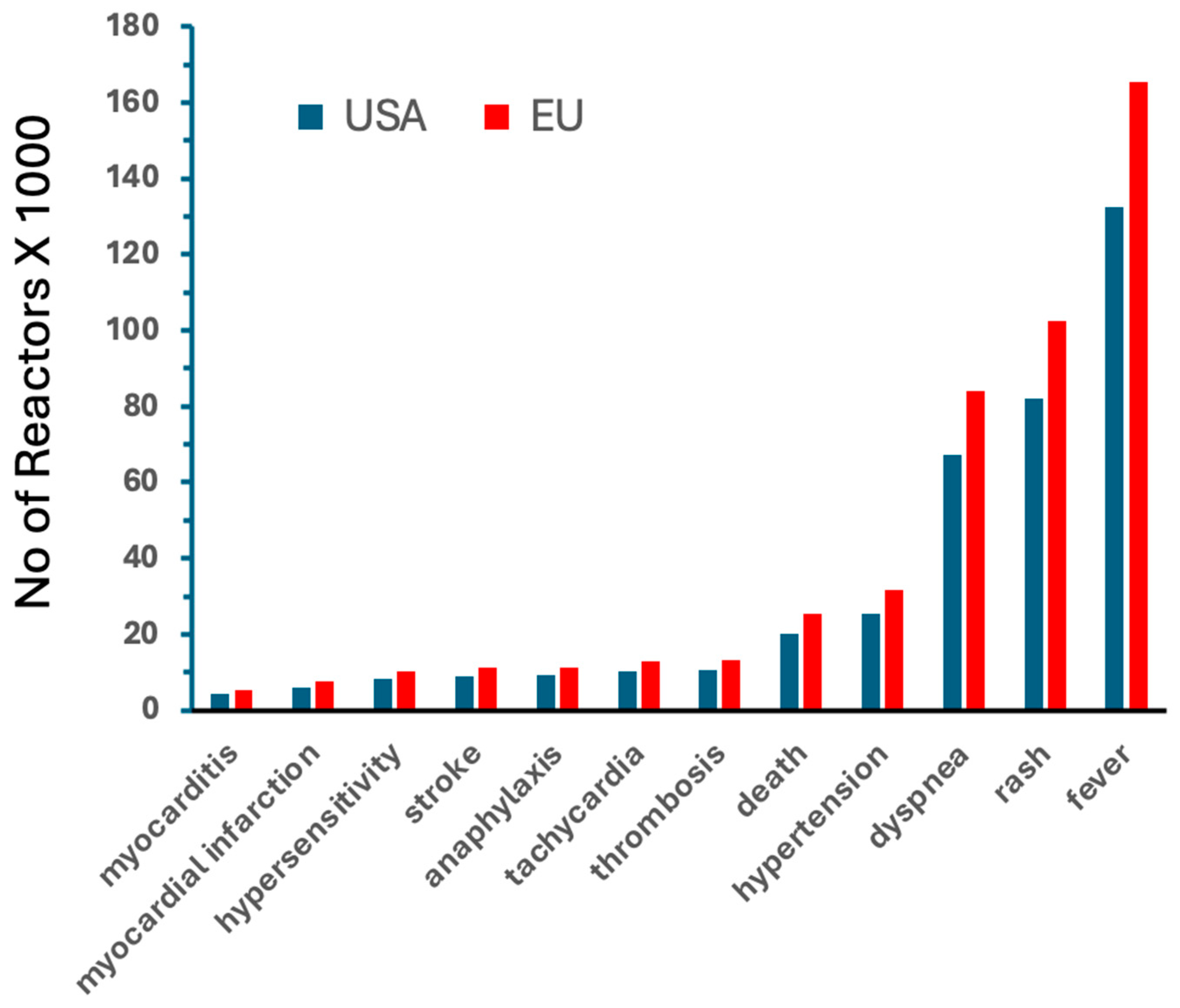
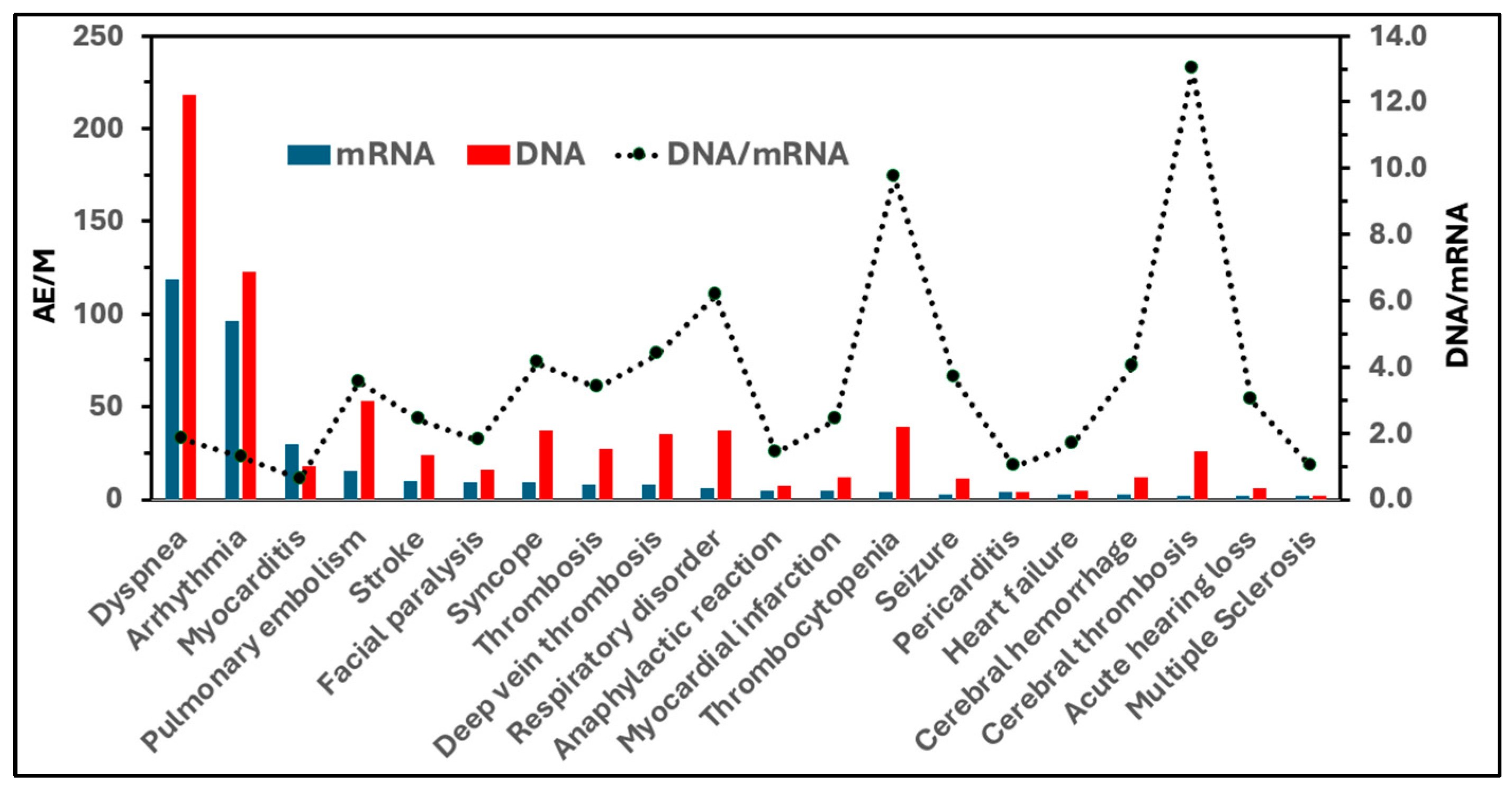
9. The European Experience: Paul-Ehrlich-Institute Statistics
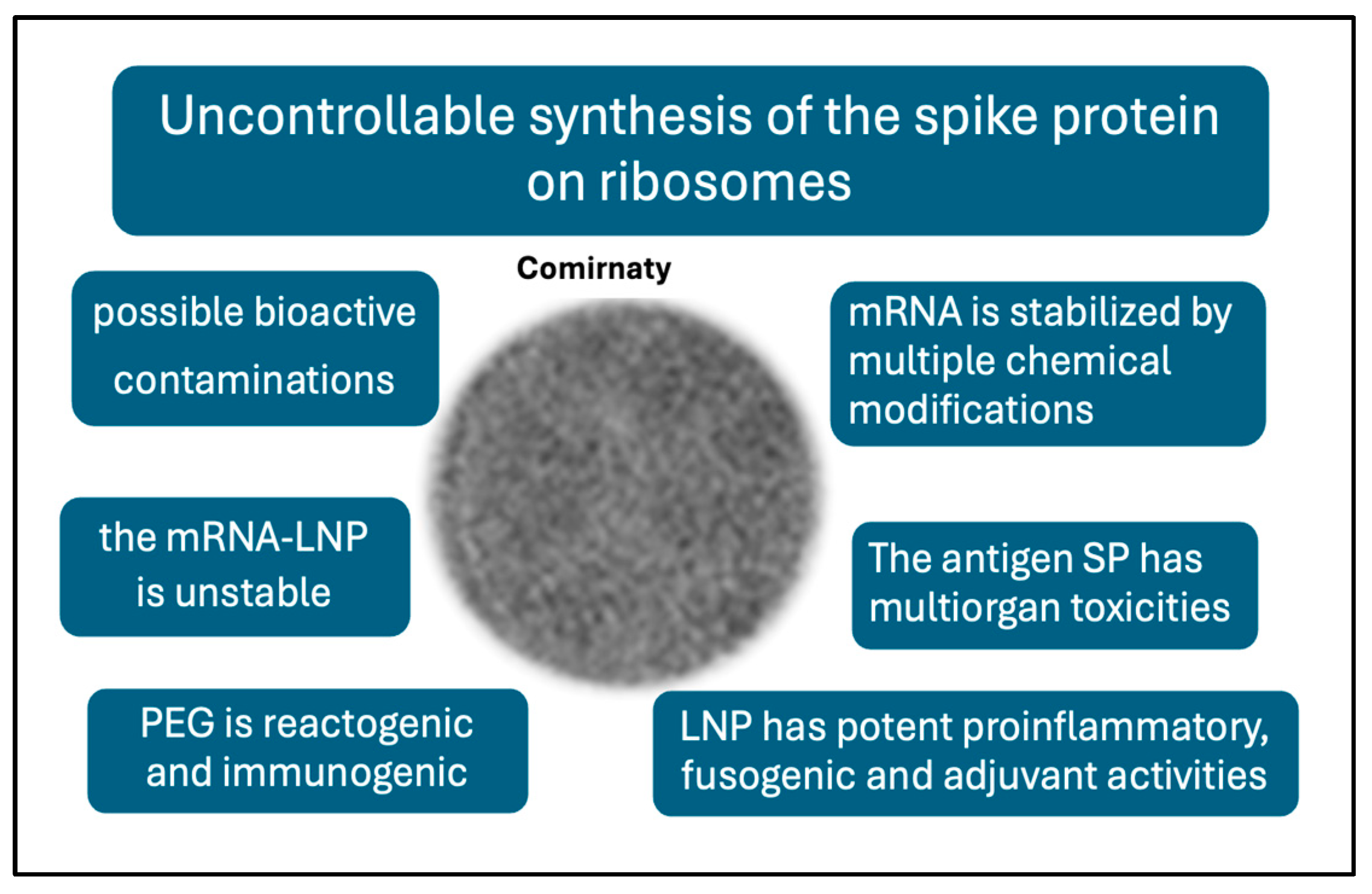
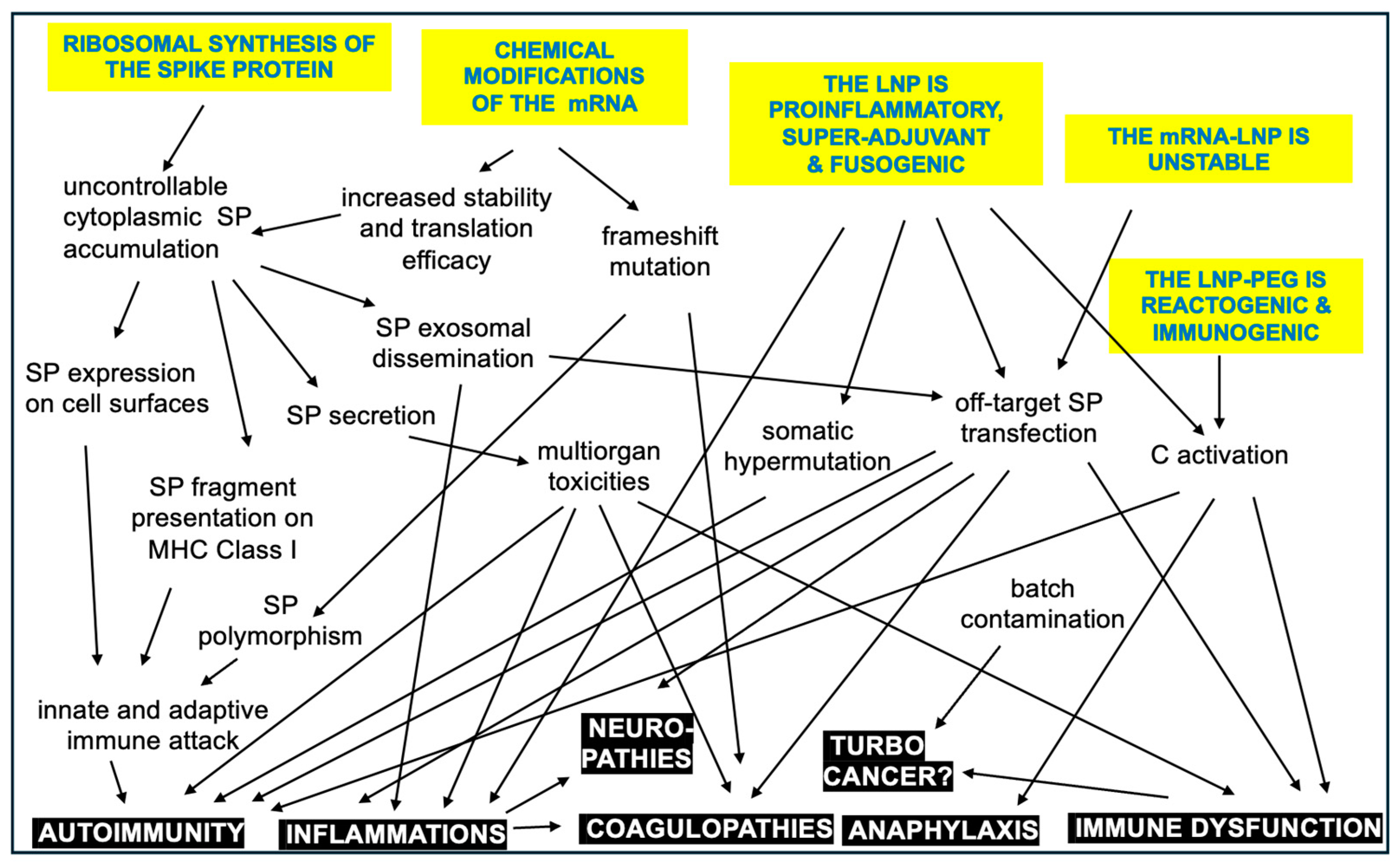
10. Potential Plausible Causes of Adverse Events Inherent to the mRNA-LNP Platform
11. Outlook
Funding
Acknowledgments
Conflicts of Interest
References
- Sahin, U.; Kariko, K.; Tureci, O. Mrna-Based Therapeutics—Developing a New Class of Drugs. Nat. Rev. Drug Discov. 2014, 13, 759–780. [Google Scholar] [PubMed]
- Kariko, K.; Whitehead, K.; van der Meel, R. What Does the Success of Mrna Vaccines Tell Us About the Future of Biological Therapeutics? Cell Syst. 2021, 12, 757–758. [Google Scholar] [PubMed]
- Cullis, P.R.; Felgner, P.L. The 60-Year Evolution of Lipid Nanoparticles for Nucleic Acid Delivery. Nat. Rev. Drug Discov. 2024, 23, 709–722. [Google Scholar]
- Igyarto, B.Z.; Jacobsen, S.; Ndeupen, S. Future Considerations for the Mrna-Lipid Nanoparticle Vaccine Platform. Curr. Opin. Virol. 2021, 48, 65–72. [Google Scholar]
- DeSantis, R.; Ladapo, J.A. Health Alert on Mrna COVID-19 Vaccine Safety. 2023. Available online: https://www.floridahealth.gov/_documents/newsroom/press-releases/2023/02/20230215-updated-health-alert.pdf (accessed on 15 February 2023).
- FDA. Fda Approves and Authorizes Updated Mrna COVID-19 Vaccines to Better Protect Against Currently Circulating Variants. FDA New Release. 2024. Available online: https://www.fda.gov/news-events/press-announcements/fda-approves-and-authorizes-updated-mrna-covid-19-vaccines-better-protect-against-currently (accessed on 15 February 2023).
- Oueijan, R.I.; Hill, O.R.; Ahiawodzi, P.D.; Fasinu, P.S.; Thompson, D.K. Rare Heterogeneous Adverse Events Associated with mRNA-Based COVID-19 Vaccines: A Systematic Review. Medicines 2022, 9, 43. [Google Scholar]
- Krumholz, H.M.; Wu, Y.; Sawano, M.; Shah, R.; Zhou, T.; Arun, A.S.; Khosla, P.; Kaleem, S.; Vashist, A.; Bhattacharjee, B.; et al. Post-Vaccination Syndrome: A Descriptive Analysis of Reported Symptoms and Patient Experiences after COVID-19 Immunization. medRxiv 2023. medRxiv:2023.11.09.23298266. [Google Scholar] [CrossRef]
- Palmer, M.; Bhakdi, S.; Hooker, B.; Holland, M.; DesBois, M.; Rasnick, D.; Fitts, C.A. Mrna Vaccine Toxicity; D4ce.Org. 2023. Available online: https://doctors4covidethics.org/mrna-vaccine-toxicity/ (accessed on 23 March 2025).
- Shrestha, Y.; Venkataraman, R. The Prevalence of Post-COVID-19 Vaccination Syndrome and Quality of Life among COVID-19-Vaccinated Individuals. Vacunas 2024, 25, 7–18. [Google Scholar]
- Law, B. Priority List of COVID-19 Adverse Events of Special Interest: Quarterly Update December 2020. Safety Platform for Emergency Vaccines (SPEAC). 2021. Available online: https://brightoncollaboration.org/wp-content/uploads/2023/08/SO2_D2.1.2_V1.2_COVID-19_AESI-update_V1.3-1.pdf (accessed on 23 March 2025).
- Fraiman, J.; Erviti, J.; Jones, M.; Greenland, S.; Whelan, P.; Kaplan, R.M.; Doshi, P. Serious Adverse Events of Special Interest Following mRNA COVID-19 Vaccination in Randomized Trials in Adults. Vaccine 2022, 40, 5798–5805. [Google Scholar]
- Faksova, K.; Walsh, D.; Jiang, Y.; Griffin, J.; Phillips, A.; Gentile, A.; Kwong, J.C.; Macartney, K.; Naus, M.; Grange, Z.; et al. COVID-19 Vaccines and Adverse Events of Special Interest: A Multinational Global Vaccine Data Network (Gvdn) Cohort Study of 99 Million Vaccinated Individuals. Vaccine 2024, 42, 2200–2211. [Google Scholar]
- Levitan, B.; Hadler, S.C.; Hurst, W.; Izurieta, H.S.; Smith, E.R.; Baker, N.L.; Bauchau, V.; Chandler, R.; Chen, R.T.; Craig, D.; et al. The Brighton Collaboration Standardized Module for Vaccine Benefit-Risk Assessment. Vaccine 2024, 42, 972–986. [Google Scholar]
- Mostert, S.; Hoogland, M.; Huibers, M.; Kaspers, G. Excess Mortality across Countries in the Western World since the COVID-19 Pandemic: ‘Our World in Data’ Estimates of January 2020 to December 2022. BMJ Public Health 2024, 2, e000282. [Google Scholar] [CrossRef]
- Rancourt, D.G.; Hickey, J.; Linard, C. Spatiotemporal Variation of Excess All-Cause Mortality in the World (125 Countries) During the COVID Period 2020-2023 Regarding Socio-Economic Factors and Public-Health and Medical Interventions. Correlation. 2024. Available online: https://correlation-canada.org/covid-excess-mortality-125-countries/ (accessed on 19 July 2024).
- Wang, S.; Zhang, K.; Du, J. Pubmed Captures More Fine-Grained Bibliographic Data on Scientific Commentary Than Web of Science: A Comparative Analysis. BMJ Health Care Inf. Inform. 2024, 31, e101017. [Google Scholar]
- Du, P.; Li, N.; Tang, S.; Zhou, Z.; Liu, Z.; Wang, T.; Li, J.; Zeng, S.; Chen, J. Development and Evaluation of Vaccination Strategies for Addressing the Continuous Evolution SARS-CoV-2 Based on Recombinant Trimeric Protein Technology: Potential for Cross-Neutralizing Activity and Broad Coronavirus Response. Heliyon 2024, 10, e34492. [Google Scholar] [PubMed]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Marc, G.P.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the Bnt162b2 Mrna COVID-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [PubMed]
- Worldwide Safety. Cumulative Analysis of Post-Authorization Adverse Event Reports of Pf-07302048 (Bnt162b2) Received through 28-Feb-2021. 2021. Available online: https://phmpt.org/wp-content/uploads/2021/11/5.3.6-postmarketing-experience.pdf?fbclid=IwAR2tWI7DKw0cc2lj8 (accessed on 23 March 2025).
- Thomas, S.J.; Moreira, E.D., Jr.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Marc, G.P.; Polack, F.P.; Zerbini, C.; et al. Safety and Efficacy of the Bnt162b2 mRNA COVID-19 Vaccine through 6 Months. N. Engl. J. Med. 2021, 385, 1761–1773. [Google Scholar]
- VAERS. Vaers Ids. 2023. Available online: https://vaers.hhs.gov/data/datasets.html (accessed on 23 March 2025).
- OpenVAERS. Vaers COVID Vaccine Adverse Event Reports. 2024. Available online: https://openvaers.com/covid-data (accessed on 23 March 2025).
- Rosenblum, H.G.; Gee, J.; Liu, R.; Marquez, P.L.; Zhang, B.; Strid, P.; Abara, W.E.; McNeil, M.M.; Myers, T.R.; Hause, A.M.; et al. Safety of Mrna Vaccines Administered During the Initial 6 Months of the Us COVID-19 Vaccination Programme: An Observational Study of Reports to the Vaccine Adverse Event Reporting System and V-Safe. Lancet Infect. Dis. 2022, 22, 802–812. [Google Scholar]
- Wikipedia. Timeline of the COVID-19 Pandemic in the United States. Wikipedia. 2025. Available online: https://en.wikipedia.org/wiki/Timeline_of_the_COVID-19_pandemic_in_the_United_States_%282021%29?utm_source=chatgpt.com (accessed on 23 March 2025).
- Ross, L.; Klompas, M. Electronic Support for Public Health–Vaccine Adverse Event Reporting System (Esp:Vaers). In Grant. Final. Report: Grant ID: R18 HS 017045. 2010. Available online: https://www.corruptedsystem.com/uploads/r18hs017045-lazarus-final-report-2011.pdf (accessed on 23 March 2025).
- Our World in Data. 2024. Available online: https://ourworldindata.org/grapher/covid-vaccine-doses-by-manufacturer?country=European+Union~HUN~USA (accessed on 23 March 2025).
- Institute, Paul Erlich. Safety Report. 2022. Available online: https://www.pei.de/SharedDocs/Downloads/EN/newsroom-en/dossiers/safety-reports/safety-report-27-december-2020-31-march-2022.pdf?__blob=publicationFile&v=8 (accessed on 23 March 2025).
- Mathieu, E.; Ritchie, H.; Ortiz-Ospina, E.; Roser, M.; Hasell, J.; Appel, C.; Giattino, C.; Rodes-Guirao, L. A Global Database of COVID-19 Vaccinations. Nat. Hum. Behav. 2021, 5, 947–953. [Google Scholar]
- Szebeni, J. Complement Activation-Related Pseudoallergy: A New Class of Drug-Induced Acute Immune Toxicity. Toxicology 2005, 216, 106–121. [Google Scholar]
- Szebeni, J. Complement Activation-Related Pseudoallergy: A Stress Reaction in Blood Triggered by Nanomedicines and Biologicals. Mol. Immunol. 2014, 61, 163–173. [Google Scholar] [PubMed]
- Szebeni, J.; Storm, G.; Ljubimova, J.Y.; Castells, M.; Phillips, E.J.; Turjeman, K.; Barenholz, Y.; Crommelin, D.J.A.; Dobrovolskaia, M.A. Applying Lessons Learned from Nanomedicines to Understand Rare Hypersensitivity Reactions to mRNA-Based SARS-CoV-2 Vaccines. Nat. Nanotechnol. 2022, 17, 337–346. [Google Scholar]
- Wolfram, R. Links between Complement Activation and Thrombosis. Blood 2019, 134 (Suppl. S1), SCI-40. [Google Scholar]
- Luo, S.; Hu, D.; Wang, M.; Zipfel, P.F.; Hu, Y. Complement in Hemolysis- and Thrombosis- Related Diseases. Front. Immunol. 2020, 11, 1212. [Google Scholar]
- Rawish, E.; Sauter, M.; Sauter, R.; Nording, H.; Langer, H.F. Complement, Inflammation and Thrombosis. Br. J. Pharmacol. 2021, 178, 2892–2904. [Google Scholar]
- Alosaimi, B.; Mubarak, A.; Hamed, M.E.; Almutairi, A.Z.; Alrashed, A.A.; AlJuryyan, A.; Enani, M.; Alenzi, F.Q.; Alturaiki, W. Complement Anaphylatoxins and Inflammatory Cytokines as Prognostic Markers for COVID-19 Severity and in-Hospital Mortality. Front. Immunol. 2021, 12, 668725. [Google Scholar]
- Lim, E.H.T.; van Amstel, R.B.E.; de Boer, V.V.; van Vught, L.A.; de Bruin, S.; Brouwer, M.C.; Vlaar, A.P.J.; van de Beek, D. Complement Activation in COVID-19 and Targeted Therapeutic Options: A Scoping Review. Blood Rev. 2023, 57, 100995. [Google Scholar]
- Siggins, M.K.; Davies, K.; Fellows, R.; Thwaites, R.S.; Baillie, J.K.; Semple, M.G.; Openshaw, P.J.M.; Zelek, W.M.; Harris, C.L.; Morgan, B.P.; et al. Alternative Pathway Dysregulation in Tissues Drives Sustained Complement Activation and Predicts Outcome across the Disease Course in COVID-19. Immunology 2023, 168, 473–492. [Google Scholar]
- Meroni, P.L.; Croci, S.; Lonati, P.A.; Pregnolato, F.; Spaggiari, L.; Besutti, G.; Bonacini, M.; Ferrigno, I.; Rossi, A.; Hetland, G.; et al. Complement Activation Predicts Negative Outcomes in COVID-19: The Experience from Northen Italian Patients. Autoimmun. Rev. 2023, 22, 103232. [Google Scholar] [PubMed]
- Ellsworth, C.R.; Chen, Z.; Xiao, M.T.; Qian, C.; Wang, C.; Khatun, M.S.; Liu, S.; Islamuddin, M.; Maness, N.J.; Halperin, J.A.; et al. Enhanced Complement Activation and Mac Formation Accelerates Severe COVID-19. Cell Mol. Life Sci. 2024, 81, 405. [Google Scholar]
- Mastellos, D.C.; Ricklin, D.; Hajishengallis, E.; Hajishengallis, G.; Lambris, J.D. Complement Therapeutics in Inflammatory Diseases: Promising Drug Candidates for C3-Targeted Intervention. Mol. Oral. Microbiol. 2016, 31, 3–17. [Google Scholar]
- Dezsi, L.; Meszaros, T.; Kozma, G.; H-Velkei, M.; Olah, C.Z.; Szabo, M.; Patko, Z.; Fulop, T.; Hennies, M.; Szebeni, M.; et al. A Naturally Hypersensitive Porcine Model May Help Understand the Mechanism of COVID-19 Mrna Vaccine-Induced Rare (Pseudo) Allergic Reactions: Complement Activation as a Possible Contributing Factor. Geroscience 2022, 44, 597–618. [Google Scholar]
- Bakos, T.; Meszaros, T.; Kozma, G.T.; Berenyi, P.; Facsko, R.; Farkas, H.; Dezsi, L.; Heirman, C.; de Koker, S.; Schiffelers, R.; et al. mRNA-LNP COVID-19 Vaccine Lipids Induce Complement Activation and Production of Proinflammatory Cytokines: Mechanisms, Effects of Complement Inhibitors, and Relevance to Adverse Reactions. Int. J. Mol. Sci. 2024, 25, 3595. [Google Scholar] [CrossRef] [PubMed]
- Barta, B.A.; Radovits, T.; Dobos, A.B.; Kozma, G.T.; Meszaros, T.; Berenyi, P.; Facsko, R.; Fulop, T.; Merkely, B.; Szebeni, J. Comirnaty-Induced Cardiopulmonary Distress and Other Symptoms of Complement-Mediated Pseudo-Anaphylaxis in a Hyperimmune Pig Model: Causal Role of Anti-Peg Antibodies. Vaccine X 2024, 19, 100497. [Google Scholar] [PubMed]
- Szebeni, J.; Baranyi, L.; Savay, S.; Bodo, M.; Milosevits, J.; Alving, C.R.; Bunger, R. Complement Activation-Related Cardiac Anaphylaxis in Pigs: Role of C5a Anaphylatoxin and Adenosine in Liposome-Induced Abnormalities in ECG and Heart Function. Am. J. Physiol. Heart Circ. Physiol. 2006, 290, H1050-8. [Google Scholar] [PubMed]
- Kozma, G.T.; Meszaros, T.; Berenyi, P.; Facsko, R.; Patko, Z.; Olah, C.Z.; Nagy, A.; Fulop, T.G.; Glatter, K.A.; Radovits, T.; et al. Role of Anti-Polyethylene Glycol (PEG) Antibodies in the Allergic Reactions to PEG-Containing COVID-19 Vaccines: Evidence for Immunogenicity of PEG. Vaccine 2023, 41, 4561–4570. [Google Scholar]
- Schanzenbacher, J.; Kohl, J.; Karsten, C.M. Anaphylatoxins Spark the Flame in Early Autoimmunity. Front. Immunol. 2022, 13, 958392. [Google Scholar]
- Ricklin, D.; Mastellos, D.C.; Lambris, J.D. Therapeutic Targeting of the Complement System. Nat. Rev. Drug Discov. 2019, 9, 10.1038. [Google Scholar]
- Kolev, M.; Kolu, N.; Yeh, M.; Parikh, A.; Deschatelets, P. The Future of Complement Therapeutics. Explor. Immunol. 2024, 4, 577–615. [Google Scholar]
- Kyte, J.A.; Gaudernack, G. Immuno-Gene Therapy of Cancer with Tumour-Mrna Transfected Dendritic Cells. Cancer Immunol. Immunother. 2006, 55, 1432–1442. [Google Scholar]
- Daniel, M.G.; Pawlik, T.M.; Fader, A.N.; Esnaola, N.F.; Makary, M.A. The Orphan Drug Act: Restoring the Mission to Rare Diseases. Am. J. Clin. Oncol. 2016, 39, 210–213. [Google Scholar]
- Gabay, M. The Orphan Drug Act: An Appropriate Approval Pathway for Treatments of Rare Diseases? Hosp. Pharm. 2019, 54, 283–284. [Google Scholar]
- Schouten, A. KEi Briefing Note 2020:4 Selected Government Definitions of Orphan or Rare Diseases. Knowledge Ecology International. Revised . 3 November 2020. Available online: https://www.keionline.org/wp-content/uploads/KEI-Briefing-Note-2020-4-Defining-Rare-Diseases.pdf?utm_source=chatgpt.com (accessed on 23 March 2025).
- Fermaglich, L.J.; Miller, K.L. A Comprehensive Study of the Rare Diseases and Conditions Targeted by Orphan Drug Designations and Approvals over the Forty Years of the Orphan Drug Act. Orphanet J. Rare Dis. 2023, 18, 163. [Google Scholar] [PubMed]
- Sanders, T.I. The Orphan Drug Act. Prog. Clin. Biol. Res. 1983, 127, 207–215. [Google Scholar] [PubMed]
- Tian, J.; Xu, Z.; Smith, J.S.; Hofherr, S.E.; Barry, M.A.; Byrnes, A.P. Adenovirus Activates Complement by Distinctly Different Mechanisms in Vitro and in Vivo: Indirect Complement Activation by Virions in Vivo. J. Virol. 2009, 83, 5648–5658. [Google Scholar] [PubMed]
- Radmer, A.; Bodurtha, J. Prospects, Realities, and Safety Concerns of Gene Therapy. Va. Med. Q. 1992, 119, 98–100. [Google Scholar]
- Szebeni, J. The Unique Features and Collateral Immune Effects of Mrna-Based COVID-19 Vaccines: Potential Plausible Causes of Adverse Events and Complications. Preprints. 2025. Available online: https://www.preprints.org/manuscript/202501.1462/v1 (accessed on 23 March 2025).
- Kariko, K.; Muramatsu, H.; Welsh, F.A.; Ludwig, J.; Kato, H.; Akira, S.; Weissman, D. Incorporation of Pseudouridine into mRNA Yields Superior Nonimmunogenic Vector with Increased Translational Capacity and Biological Stability. Mol. Ther. 2008, 16, 1833–1840. [Google Scholar]
- Kariko, K.; Muramatsu, H.; Ludwig, J.; Weissman, D. Generating the Optimal Mrna for Therapy: Hplc Purification Eliminates Immune Activation and Improves Translation of Nucleoside-Modified, Protein-Encoding Mrna. Nucleic Acids Res. 2011, 39, e142. [Google Scholar]
- Moghaddar, M.; Radman, R.; Macreadie, I. Severity, Pathogenicity and Transmissibility of Delta and Lambda Variants of SARS-CoV-2, Toxicity of Spike Protein and Possibilities for Future Prevention of COVID-19. Microorganisms 2021, 9, 2167. [Google Scholar] [CrossRef]
- Schwartz, L.; Aparicio-Alonso, M.; Henry, M.; Radman, M.; Attal, R.; Bakkar, A. Toxicity of the Spike Protein of COVID-19 Is a Redox Shift Phenomenon: A Novel Therapeutic Approach. Free Radic. Biol. Med. 2023, 206, 106–110. [Google Scholar]
- Boros, L.G.; Kyriakopoulos, A.M.; Brogna, C.; Piscopo, M.; McCullough, P.A.; Seneff, S. Long-Lasting, Biochemically Modified mRNA, and Its Frameshifted Recombinant Spike Proteins in Human Tissues and Circulation after COVID-19 Vaccination. Pharmacol. Res. Perspect. 2024, 12, e1218. [Google Scholar]
- Pardi, N.; Tuyishime, S.; Muramatsu, H.; Kariko, K.; Mui, B.L.; Tam, Y.K.; Madden, T.D.; Hope, M.J.; Weissman, D. Expression Kinetics of Nucleoside-Modified mRNA Delivered in Lipid Nanoparticles to Mice by Various Routes. J. Control Release 2015, 217, 345–351. [Google Scholar]
- Pfizer Australia Pty Ltd. Nonclinical Evaluation Report: Bnt162b2 [Mrna] COVID-19 Vaccine (Comirnatytm). 2021. Available online: https://www.tga.gov.au/sites/default/files/foi-2389-06.pdf (accessed on 23 March 2025).
- Sharma, P.; Hoorn, D.; Aitha, A.; Breier, D.; Peer, D. The Immunostimulatory Nature of Mrna Lipid Nanoparticles. Adv. Drug Deliv. Rev. 2024, 205, 115175. [Google Scholar] [CrossRef] [PubMed]
- Catenacci, L.; Rossi, R.; Sechi, F.; Buonocore, D.; Sorrenti, M.; Perteghella, S.; Peviani, M.; Bonferoni, M.C. Effect of Lipid Nanoparticle Physico-Chemical Properties and Composition on Their Interaction with the Immune System. Pharmaceutics 2024, 16, 1521. [Google Scholar] [CrossRef] [PubMed]
- Cullis, P.R.; Hope, M.J. Lipid Nanoparticle Systems for Enabling Gene Therapies. Mol. Ther. 2017, 25, 1467–1475. [Google Scholar]
- Ferraresso, F.; Badior, K.; Seadler, M.; Zhang, Y.; Wietrzny, A.; Cau, M.F.; Haugen, A.; Rodriguez, G.G.; Dyer, M.R.; Cullis, P.R.; et al. Protein Is Expressed in All Major Organs after Intravenous Infusion of Mrna-Lipid Nanoparticles in Swine. Mol. Ther. Methods Clin. Dev. 2024, 32, 101314. [Google Scholar] [PubMed]
- Szebeni, J.; Kiss, B.; Bozo, T.; Turjeman, K.; Levi-Kalisman, Y.; Barenholz, Y.; Kellermayer, M. Insights into the Structure of Comirnaty COVID-19 Vaccine: A Theory on Soft, Partially Bilayer-Covered Nanoparticles with Hydrogen Bond-Stabilized mRNA-Lipid Complexes. ACS Nano 2023, 17, 13147–13157. [Google Scholar]
- König, B.; Kirchner, J.O. Methodological Considerations Regarding the Quantification of DNA Impurities in the COVID-19 Mrna Vaccine Comirnaty®. Methods Protoc. 2024, 7, 41. [Google Scholar] [CrossRef]
- Diblasi, L.; Monteverde, M.; Nonis, D.; Sangorrín, M. At Least 55 Undeclared Chemical Elements Found in COVID-19 Vaccines from Astrazeneca, Cansino, Moderna, Pfizer, Sinopharm and Sputnik V, with Precise Icp-Ms. Int. J. Vaccine Theory Pract. Res. 2024, 3, 1367–1393. [Google Scholar]
- Verbeke, R.; Hogan, M.J.; Lore, K.; Pardi, N. Innate Immune Mechanisms of Mrna Vaccines. Immunity 2022, 55, 1993–2005. [Google Scholar]
- Fineberg, H.V. Swine Flu of 1976: Lessons from the Past. An Interview with Dr Harvey V Fineberg. Bull World Health Organ 2009, 87, 414–415. [Google Scholar]
- Wilson, E.; Goswami, J.; Baqui, A.H.; Doreski, P.A.; Perez-Marc, G.; Zaman, K.; Monroy, J.; Duncan, C.J.A.; Ujiie, M.; Ramet, M.; et al. Efficacy and Safety of an Mrna-Based Rsv Pref Vaccine in Older Adults. N. Engl. J. Med. 2023, 389, 2233–2244. [Google Scholar] [CrossRef]
- ModernaTX, Inc. Prescribing Information: Respiratory Syncytial Virus Vaccine) Injectable Suspension, for Intramuscular Use. 2024. Available online: https://www.fda.gov/media/179005/download?attachment=&utm_source=chatgpt.com (accessed on 23 March 2025).
- Wang, Y.S.; Kumari, M.; Chen, G.H.; Hong, M.H.; Yuan, J.P.; Tsai, J.L.; Wu, H.C. Mrna-Based Vaccines and Therapeutics: An in-Depth Survey of Current and Upcoming Clinical Applications. J. Biomed. Sci. 2023, 30, 84. [Google Scholar]
- Ladak, R.J.; He, A.J.; Huang, Y.H.; Ding, Y. The Current Landscape of Mrna Vaccines against Viruses and Cancer-a Mini Review. Front. Immunol. 2022, 13, 885371. [Google Scholar] [CrossRef] [PubMed]
- Sayour, E.J.; Boczkowski, D.; Mitchell, D.A.; Nair, S.K. Cancer Mrna Vaccines: Clinical Advances and Future Opportunities. Nat. Rev. Clin. Oncol. 2024, 21, 489–500. [Google Scholar] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Organ System | Adverse Events |
|---|---|
| Cardiovascular | acute coronary syndrome, aneurysm, arrhythmia, arrhythmias, arteriosclerosis, cardiac tamponade, coronary artery disease, deep vein thrombosis, cardiomyopathy, edema of the lip, tongue, face, endothelial dysfunction, heart failure, hypertension, hypotension, ischemia, large-vessel vasculitis, microangiopathy, myocardial infarction, myocarditis, non-bacterial thrombotic endocarditis, pericarditis, postural tachycardia syndrome, stroke, sudden death, Takotsubo syndrome (stress cardiomyopathy), vascular inflammation (Kawasaki disease) |
| Neurological | acute disseminated encephalomyelitis, ageusia, anosmia, aseptic meningitis, Bell’s palsy, cerebral venous sinus thrombosis, CNS bleed, chronic fatigue syndrome, cranial polyneuropathy, dysesthesia with exanthem, dysgeusia, encephalitis, encephalopathy, facial nerve palsy, Guillain-Barré syndrome, hypogeusia, hypoglossal nerve palsy, hyposmia, myalgic encephalomyelitis, myoclonus, myoclonus-ataxia, ophthalmoplegia, oropharyngeal dysphagia, persistent hiccups, seizures, sensorineural hearing loss, stroke (hemorrhagic, ischemic), vestibular neuritis |
| Respiratory | acute chest syndrome, acute respiratory distress syndrome, bronchospasm, bullous lung disease, coughing, dyspnea, pulmonary vasculitis, hemopneumothorax, hemoptysis, hilar lymphadenopathy, hoarseness, hypoxia, pediatric croup, platypnea orthodeoxia syndrome, pneumomediastinum, pneumothorax, pneumomediastinum, pulmonary embolism, stridor |
| Gastrointestinal | acute acalculous cholecystitis, angular cheilitis, appendicitis, cholecystitis, colitis, enteritis, enterocolitis, fulminant hepatic failure, hepatitis, intussusception, pancreatitis, paralytic ileus, parotitis, spontaneous hemoperitoneum, spontaneous splenic rupture, tongue ulcers |
| Musculoskeletal | arthralgia, arthritis, aseptic arthritis, muscle spasms, myalgia, myositis, rhabdomyolysis |
| Dermatological | chilblain, chronic urticaria, cutaneous vasculitis, dermatographia, dermatomyositis, epidermal necrolysis, erythema multiforme, follicular eruption, Gianotti-Crosti rash, Gilbert type erythema nodosum, Grover-like eruption, hyperkeratosis, lower extremity bullae, maculopapular rash, nail bed red half-moon sign, oral vesiculobullous lesions, painful cystic lesion, perniosis-like lesions ("COVID toes"), pityriasis rosea, pustular eruption, rash, seborrheic dermatitis, small fiber neuropathy, Steven-Johnson syndrome, unilateral thoracic exanthema, urticaria (hives), vasculitis. |
| Hematological | anemia, coagulopathy, cold agglutinin syndrome, hemophagocytic lymph histiocytosis, idiopathic thrombocytopenic purpura, lymphopenia, methemoglobinemia, stroke, thromboembolism, thrombocytopenia, thrombosis, thrombosis with thrombocytopenia |
| Endocrine/ Metabolic | adrenal injury, diabetes, hyperglycemia, myxedema, orchitis, pancreatitis, parotitis, prostatitis, prostatic infarction, sexual dysfunction, thyroiditis |
| Renal/ Genitourinary | glomerulopathy, hematuria, hypernatremia, IgA vasculitis with nephritis, nephrosis, proteinuria, renal failure, renal infarction, urinary retention, vasculitis with glomerulonephritis |
| Immune System | anaphylaxis, autoimmune flare-ups, autoimmune glomerulonephritis, autoimmune hemolytic anemia, autoimmune hepatitis, autoimmune rheumatological diseases, CARPA, hypersensitivity reactions, lymphadenopathy, multiorgan autoimmunity, multiorgan inflammation, persistent lymph-node enlargement, swelling and pain, peripheral lymphoedema formation and pain |
| General/Systemic | abscess, alopecia, hyperferritinemic syndrome, hyperglycemia, hyponatremia, multisystem inflammatory syndrome, sepsis, septic shock |
| Psychiatric | akathisia, altered mental status, catalepsy, convulsions, delirium, insomnia, mania, multiple sclerosis, narcolepsy, psychosis, seizures, status epilepticus, sudden and persistent dysphonia, suicide attempt |
| Ocular | bilateral macular bleed, bilateral visual loss, conjunctivitis, episcleritis, ocular myasthenia gravis, ocular/orbital inflammation, retinopathy, uveo-retinitis |
| Reproductive | abortion, ectopic pregnancy, fetal HELLP syndrome (hemolysis, elevated liver enzymes, and low platelet count) |
| Gynecological/ obstetric | amenorrhea, dysmenorrhea, endometritis, irregular bleeding, menorrhagia, metrorrhagia, multiple uterine myomatosis, oligomenorrhea, pelvic inflammatory disease, postmenopausal recurrent bleeding, premature bleeding, premenstrual syndrome |
| Oncological | acute lymphocytosis, lymphoid leukemias, “turbo cancer” |
| Vaccine | AE+ n * | Doses | AE+/M ** | AE−/AE+ *** | COVID/Flu |
|---|---|---|---|---|---|
| Comirnaty | 434,821 | 401,685,954 | 1082 | 924 | 20 |
| Spikevax | 426,714 | 251,852,502 | 1694 | 590 | 32 |
| Combined mRNA | 861,535 | 653,538,456 | 1318 | 759 | 25 |
| Jcovden (Janssen) | 54,728 | 18,991,177 | 2882 | 347 | 54 |
| All genetic | 934,959 | 672,529,633 | 1390 | 719 | 26 |
| Flu | 18,696 | 352,670,000 | 53 | 18,863 | 1 |
| Flu Vaccines | mRNA Vaccines | Fold Increase | ||||
|---|---|---|---|---|---|---|
| AE | AE/M | AE | AE/M | AE | AE/M | |
| fever | 4294 | 7.9 | 132,447 | 201.70 | 31 | 26 |
| rash | 1118 | 2.06 | 82,113 | 125.05 | 73 | 61 |
| dyspnea | 622 | 1.14 | 67,355 | 102.57 | 204 | 90 |
| hypertension | 160 | 0.29 | 25,292 | 38.52 | 158 | 133 |
| death | 74 | 0.14 | 20,227 | 30.8 | 273 | 220 |
| thrombosis | 19 | 0.03 | 10,439 | 15.9 | 549 | 530 |
| tachycardia | 52 | 0.1 | 10,205 | 15.54 | 196 | 155 |
| anaphylaxis | 117 | 0.22 | 9094 | 13.85 | 78 | 63 |
| stroke | 280 | 0.52 | 8939 | 13.61 | 32 | 26 |
| hypersensitivity | 122 | 0.22 | 8153 | 12.42 | 67 | 56 |
| myocardial infarction | 23 | 0.04 | 6067 | 9.24 | 264 | 231 |
| myocarditis | 3 | 0.01 | 4176 | 6.36 | 1392 | 636 |
| AE of Special Interest | AEs/Million | |||
|---|---|---|---|---|
| Comirnaty | Spikevax | Vaxzevria | Jcovden | |
| Dyspnea | 55 | 64 | 110 | 108 |
| Arrhythmia | 46 | 50 | 57 | 66 |
| Myocarditis | 14 | 16 | 6 | 12 |
| Pulmonary embolism | 8 | 7 | 33 | 20 |
| Stroke | 6 | 4 | 15 | 9 |
| Facial paralysis | 5 | 4 | 7 | 9 |
| Syncope | 5 | 4 | 25 | 12 |
| Thrombosis | 4 | 4 | 19 | 8 |
| Deep vein thrombosis | 4 | 4 | 27 | 8 |
| Respiratory disorder | 3 | 3 | 33 | 4 |
| Anaphylactic reaction | 3 | 2 | 4 | 3 |
| Myocardial infarction | 3 | 2 | 6 | 6 |
| Thrombocytopenia | 3 | 1 | 32 | 7 |
| Seizure | 2 | 1 | 7 | 4 |
| Pericarditis | 2 | 2 | 1 | 3 |
| Heart failure | 2 | 1 | 2 | 3 |
| Cerebral hemorrhage | 2 | 1 | 8 | 4 |
| Cerebral thrombosis | 1 | 1 | 20 | 6 |
| Acute hearing loss | 1 | 1 | 5 | 1 |
| Multiple Sclerosis | 1 | 1 | 1 | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Szebeni, J. Expanded Spectrum and Increased Incidence of Adverse Events Linked to COVID-19 Genetic Vaccines: New Concepts on Prophylactic Immuno-Gene Therapy, Iatrogenic Orphan Disease, and Platform-Inherent Challenges. Pharmaceutics 2025, 17, 450. https://doi.org/10.3390/pharmaceutics17040450
Szebeni J. Expanded Spectrum and Increased Incidence of Adverse Events Linked to COVID-19 Genetic Vaccines: New Concepts on Prophylactic Immuno-Gene Therapy, Iatrogenic Orphan Disease, and Platform-Inherent Challenges. Pharmaceutics. 2025; 17(4):450. https://doi.org/10.3390/pharmaceutics17040450
Chicago/Turabian StyleSzebeni, Janos. 2025. "Expanded Spectrum and Increased Incidence of Adverse Events Linked to COVID-19 Genetic Vaccines: New Concepts on Prophylactic Immuno-Gene Therapy, Iatrogenic Orphan Disease, and Platform-Inherent Challenges" Pharmaceutics 17, no. 4: 450. https://doi.org/10.3390/pharmaceutics17040450
APA StyleSzebeni, J. (2025). Expanded Spectrum and Increased Incidence of Adverse Events Linked to COVID-19 Genetic Vaccines: New Concepts on Prophylactic Immuno-Gene Therapy, Iatrogenic Orphan Disease, and Platform-Inherent Challenges. Pharmaceutics, 17(4), 450. https://doi.org/10.3390/pharmaceutics17040450