
Nanomedicine in the Diagnosis and Treatment of Pancreatic Cancer

Abstract
1. Introduction
1.1. Introduction of Nanomedicines
1.2. Challenges in Diagnosis and Treatment of PDAC
2. The Diagnosis of PDAC Based on Nanomedicine
2.1. Biomarkers Detection Based on Nanomedicine
2.1.1. Detection of Biomarkers in Body Fluids
2.1.2. Detection of Biomarkers in Cells and Tissues
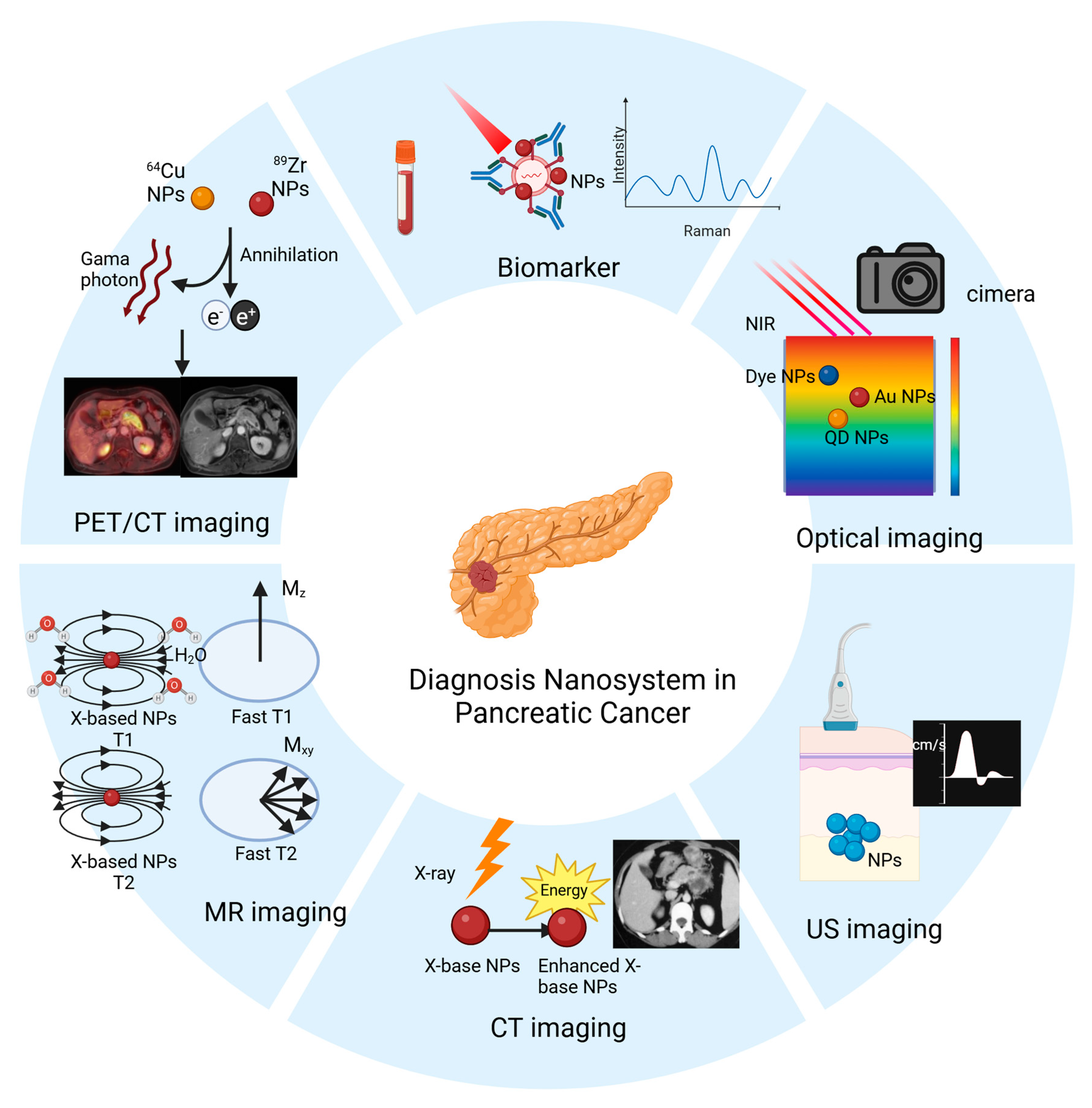
2.2. Imaging Examination Based on Nanomedicine
2.2.1. NIR Imaging
2.2.2. CT Imaging
2.2.3. MR Imaging
2.2.4. PET Imaging
3. The Treatment of PDAC Based on Nanomedicine
3.1. Polymeric Nanoparticle
3.1.1. Targeted Therapy Drugs
3.1.2. Cytotoxic Chemotherapeutic Drugs
3.2. Nanoliposomal
3.2.1. Nanoliposome Irinotecan
3.2.2. Nab-PTX
3.2.3. Targeted Therapy Drugs
3.2.4. Antifibrosis Drugs
3.3. Polymeric Micelles
3.3.1. Cytotoxic Chemotherapeutic Drugs
3.3.2. Targeted Therapy Drugs
3.3.3. Immunomodulators
3.3.4. Combination Drugs
3.4. Inorganic Nanoparticles
3.4.1. AuNPs
3.4.2. Iron Oxide NPs
3.4.3. Tungsten Oxide NPs
4. Summary and Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| PDAC | Pancreatic ductal adenocarcinoma |
| NPs | nanomedicines |
| EPR | Enhanced permeability and retention |
| GEM | gemcitabine |
| 5-FU | 5-fluorouracil |
| LV | leucovorin |
| CA19-9 | carbohydrate antigen 19-9 |
| CT | computed tomography |
| MRI | magnetic resonance imaging |
| PET | positron emission tomography |
| US | Ultrasound |
| AuNPs | gold nanoparticles |
| CEA | carcinoembryonic antigen |
| ssDNA | single-stranded DNA |
| HRP | Horseradish peroxidase |
| SERS | Surface-enhanced Raman scattering |
| miRs | microRNAs |
| LSPR | localized surface plasmon resonance |
| αHL | α-hemolysin |
| EV | Extracellular vesicle |
| QD | Quantum dots |
| EphA2 | Erythropoietin-producing hepatocellular A 2 |
| EpCAM | Epithelial cell adhesion molecule |
| AC | Alternating current |
| MIF | macrophage migration inhibitory factor |
| GPC1 | Glypican1 |
| EGFR | Epidermal growth factor receptor |
| LAMP | liposome based on isothermal amplification |
| REG1A | Regenerating Family Member 1 Alpha |
| PCR | Polymerase chain reaction |
| SPIDE | screen-printed interdigitated electrode |
| CNO | carbon nano-onions |
| GO | graphene oxide |
| mAFTN | modified apoferritin |
| ZnS | CdSe |
| Ni-NTA | nickel-nitrilotriacetic acid |
| PEG | polyethylene glycol |
| FAP | fibroblast activation protein |
| NIR | near-infrared |
| PAI | photoacoustic imaging |
| FA | folic acid |
| CR | croconaine |
| CDH17 | Cadherin 17 |
| HSA | human serum albumin |
| CCK-B | cholecystokinin B |
| ICG | indocyanine green |
| CPSNP | calcium phosphate silica nanoparticles |
| Bi | bismuth |
| Pt | platinum |
| BNTs | bismuth subcarbonate nanotubes |
| SPIONs | superparamagnetic iron oxide nanoparticles |
| NSF | nephrogenic systemic fibrosis |
| CXCR4 | Chemokine receptor 4 |
| ENO1 | enolase 1 |
| 18F | 18F-fluorodeoxyglucose |
| KRAS | Kirsten rats arcomaviral oncogene homolog |
| IGFR1 | insulin-like growth factor 1 receptor |
| TGF-β | transforming growth factor beta |
| OS | overall survival |
| CAFs | cancer-associated fibroblasts |
| PSCs | pancreatic stellate cells |
| TAMs | regulatory T cells, tumor-associated macrophages |
| TME | tumor microenvironment |
| EMT | Epithelial-mesenchymal transition |
| siRNA | small interfering RNA |
| iRGD | internalizing RGD peptide |
| PDCD4 | Programmed cell death protein 4 |
| PTEN | Phosphatase and tensin homolog deleted on chromosome ten |
| TPM1 | Tropomyosin 1 |
| PEI | polyethylenimine |
| Nab-PTX | Nab-paclitaxel |
| Hh | hedgehog |
| CPA | Cyclopamine |
| SMO | smoothened |
| DTX | docetaxel |
| NGH | nanogel |
| Dox | doxorubicin |
| ANPs | albumin nanoparticles |
| HF | halofuginone |
| OLA | olaparib |
| AA | ascorbic acid |
| nal-IRI | nanoparticles |
| α-SMA | α-smooth muscle actin |
| PTX | Paclitaxel |
| CDA | cytidine deaminase |
| AF | antibody fragment |
| PFS | progression-free survival |
| TE | thromboembolic |
| EA | ellagic acid |
| TSLs | thermosensitive liposomes |
| bi-shRNA | bifunctional short hairpin RNA |
| NF-κB | Nuclear factor kappa-B |
| MIT | Mithramycin |
| STING | Stimulator of Interferon Genes |
| β-CD | β-cyclodextrin |
| MMP-2 | matrix metalloproteinase-2 |
| MDSC | myeloid-derived suppressor cells |
| FUDR | fluorouridine |
| SHH | Sonic hedgehog |
| SAL | salinomycin |
| CSCs | cancer stem cells |
| I3A | Ingenol-3-mebutate |
| DC | dendritic cell |
| TPP+ | triphenylphosphine |
| ROS | reactive oxygen species |
| ATRA | all-trans retinoic acid |
| RLX | relaxin 2 |
References
- Quader, S.; Kataoka, K. Nanomaterial-Enabled Cancer Therapy. Mol. Ther. 2017, 25, 1501–1513. [Google Scholar] [CrossRef] [PubMed]
- Wong, X.Y.; Sena-Torralba, A.; Álvarez-Diduk, R.; Muthoosamy, K.; Merkoçi, A. Nanomaterials for Nanotheranostics: Tuning Their Properties According to Disease Needs. ACS Nano 2020, 14, 2585–2627. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Valdivieso, J.; Girotti, A.; Schneider, J.; Arias, F.J. Advanced nanomedicine and cancer: Challenges and opportunities in clinical translation. Int. J. Pharm. 2021, 599, 120438. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, S.M. Epidemiology of Cancer. Clin. Chem. 2024, 70, 140–149. [Google Scholar] [CrossRef] [PubMed]
- Riquelme, E.; Zhang, Y.; Zhang, L.; Montiel, M.; Zoltan, M.; Dong, W.; Quesada, P.; Sahin, I.; Chandra, V.; San Lucas, A.; et al. Tumor Microbiome Diversity and Composition Influence Pancreatic Cancer Outcomes. Cell 2019, 178, 795–806.e712. [Google Scholar] [CrossRef]
- Luo, G.; Fan, Z.; Cheng, H.; Jin, K.; Guo, M.; Lu, Y.; Yang, C.; Fan, K.; Huang, Q.; Long, J.; et al. New observations on the utility of CA19-9 as a biomarker in Lewis negative patients with pancreatic cancer. Pancreatology 2018, 18, 971–976. [Google Scholar] [CrossRef]
- Zhang, L.; Sanagapalli, S.; Stoita, A. Challenges in diagnosis of pancreatic cancer. World J. Gastroenterol. 2018, 24, 2047–2060. [Google Scholar] [CrossRef]
- Luo, G.; Jin, K.; Deng, S.; Cheng, H.; Fan, Z.; Gong, Y.; Qian, Y.; Huang, Q.; Ni, Q.; Liu, C.; et al. Roles of CA19-9 in pancreatic cancer: Biomarker, predictor and promoter. Biochim. Biophys. Acta Rev. Cancer 2021, 1875, 188409. [Google Scholar] [CrossRef]
- Chu, L.C.; Goggins, M.G.; Fishman, E.K. Diagnosis and Detection of Pancreatic Cancer. Cancer J. 2017, 23, 333–342. [Google Scholar] [CrossRef]
- Haqq, J.; Howells, L.M.; Garcea, G.; Metcalfe, M.S.; Steward, W.P.; Dennison, A.R. Pancreatic stellate cells and pancreas cancer: Current perspectives and future strategies. Eur. J. Cancer 2014, 50, 2570–2582. [Google Scholar] [CrossRef]
- Sindhwani, S.; Syed, A.M.; Ngai, J.; Kingston, B.R.; Maiorino, L.; Rothschild, J.; MacMillan, P.; Zhang, Y.; Rajesh, N.U.; Hoang, T.; et al. The entry of nanoparticles into solid tumours. Nat. Mater. 2020, 19, 566–575. [Google Scholar] [CrossRef] [PubMed]
- Farhangnia, P.; Khorramdelazad, H.; Nickho, H.; Delbandi, A.A. Current and future immunotherapeutic approaches in pancreatic cancer treatment. J. Hematol. Oncol. 2024, 17, 40. [Google Scholar] [CrossRef] [PubMed]
- Huang, Z.; Jiang, Z.; Zhao, C.; Han, W.; Lin, L.; Liu, A.; Weng, S.; Lin, X. Simple and effective label-free electrochemical immunoassay for carbohydrate antigen 19-9 based on polythionine-Au composites as enhanced sensing signals for detecting different clinical samples. Int. J. Nanomed. 2017, 12, 3049–3058. [Google Scholar] [CrossRef]
- Liu, M.; Jia, C.; Huang, Y.; Lou, X.; Yao, S.; Jin, Q.; Zhao, J.; Xiang, J. Highly sensitive protein detection using enzyme-labeled gold nanoparticle probes. Analyst 2010, 135, 327–331. [Google Scholar] [CrossRef]
- Krasnoslobodtsev, A.V.; Torres, M.P.; Kaur, S.; Vlassiouk, I.V.; Lipert, R.J.; Jain, M.; Batra, S.K.; Lyubchenko, Y.L. Nano-immunoassay with improved performance for detection of cancer biomarkers. Nanomedicine 2015, 11, 167–173. [Google Scholar] [CrossRef]
- Joshi, G.K.; Deitz-McElyea, S.; Liyanage, T.; Lawrence, K.; Mali, S.; Sardar, R.; Korc, M. Label-Free Nanoplasmonic-Based Short Noncoding RNA Sensing at Attomolar Concentrations Allows for Quantitative and Highly Specific Assay of MicroRNA-10b in Biological Fluids and Circulating Exosomes. ACS Nano 2015, 9, 11075–11089. [Google Scholar] [CrossRef]
- Xu, J.; Liao, K.; Fu, Z.; Xiong, Z. A new method for early detection of pancreatic cancer biomarkers: Detection of microRNAs by nanochannels. Artif. Cells Nanomed. Biotechnol. 2019, 47, 2634–2640. [Google Scholar] [CrossRef]
- Rodrigues, M.; Richards, N.; Ning, B.; Lyon, C.J.; Hu, T.Y. Rapid Lipid-Based Approach for Normalization of Quantum-Dot-Detected Biomarker Expression on Extracellular Vesicles in Complex Biological Samples. Nano Lett. 2019, 19, 7623–7631. [Google Scholar] [CrossRef]
- Lewis, J.M.; Vyas, A.D.; Qiu, Y.; Messer, K.S.; White, R.; Heller, M.J. Integrated Analysis of Exosomal Protein Biomarkers on Alternating Current Electrokinetic Chips Enables Rapid Detection of Pancreatic Cancer in Patient Blood. ACS Nano 2018, 12, 3311–3320. [Google Scholar] [CrossRef]
- Li, T.D.; Zhang, R.; Chen, H.; Huang, Z.P.; Ye, X.; Wang, H.; Deng, A.M.; Kong, J.L. An ultrasensitive polydopamine bi-functionalized SERS immunoassay for exosome-based diagnosis and classification of pancreatic cancer. Chem. Sci. 2018, 9, 5372–5382. [Google Scholar] [CrossRef]
- Tomita, N.; Mori, Y.; Kanda, H.; Notomi, T. Loop-mediated isothermal amplification (LAMP) of gene sequences and simple visual detection of products. Nat. Protoc. 2008, 3, 877–882. [Google Scholar] [CrossRef] [PubMed]
- Ibáñez-Redín, G.; Furuta, R.H.M.; Wilson, D.; Shimizu, F.M.; Materon, E.M.; Arantes, L.; Melendez, M.E.; Carvalho, A.L.; Reis, R.M.; Chaur, M.N.; et al. Screen-printed interdigitated electrodes modified with nanostructured carbon nano-onion films for detecting the cancer biomarker CA19-9. Mater. Sci. Eng. C Mater. Biol. Appl. 2019, 99, 1502–1508. [Google Scholar] [CrossRef] [PubMed]
- Eck, W.; Craig, G.; Sigdel, A.; Ritter, G.; Old, L.J.; Tang, L.; Brennan, M.F.; Allen, P.J.; Mason, M.D. PEGylated gold nanoparticles conjugated to monoclonal F19 antibodies as targeted labeling agents for human pancreatic carcinoma tissue. ACS Nano 2008, 2, 2263–2272. [Google Scholar] [CrossRef]
- Ma, M.Z.; Kong, X.; Weng, M.Z.; Cheng, K.; Gong, W.; Quan, Z.W.; Peng, C.H. Candidate microRNA biomarkers of pancreatic ductal adenocarcinoma: Meta-analysis, experimental validation and clinical significance. J. Exp. Clin. Cancer Res. 2013, 32, 71. [Google Scholar] [CrossRef]
- van Niel, G.; D’Angelo, G.; Raposo, G. Shedding light on the cell biology of extracellular vesicles. Nat. Rev. Mol. Cell Biol. 2018, 19, 213–228. [Google Scholar] [CrossRef]
- Hwang, M.P.; Lee, J.W.; Lee, K.E.; Lee, K.H. Think modular: A simple apoferritin-based platform for the multifaceted detection of pancreatic cancer. ACS Nano 2013, 7, 8167–8174. [Google Scholar] [CrossRef]
- Qiao, Y.; Wan, J.; Zhou, L.; Ma, W.; Yang, Y.; Luo, W.; Yu, Z.; Wang, H. Stimuli-responsive nanotherapeutics for precision drug delivery and cancer therapy. Wiley Interdiscip. Rev. Nanomed. Nanobiotechnol. 2019, 11, e1527. [Google Scholar] [CrossRef]
- Li, H.; Li, K.; Dai, Y.; Xu, X.; Cao, X.; Zeng, Q.; He, H.; Pang, L.; Liang, J.; Chen, X.; et al. In vivo near infrared fluorescence imaging and dynamic quantification of pancreatic metastatic tumors using folic acid conjugated biodegradable mesoporous silica nanoparticles. Nanomedicine 2018, 14, 1867–1877. [Google Scholar] [CrossRef]
- Dong, Y.; Xia, P.; Xu, X.; Shen, J.; Ding, Y.; Jiang, Y.; Wang, H.; Xie, X.; Zhang, X.; Li, W.; et al. Targeted delivery of organic small-molecule photothermal materials with engineered extracellular vesicles for imaging-guided tumor photothermal therapy. J. Nanobiotechnol. 2023, 21, 442. [Google Scholar] [CrossRef]
- Clawson, G.A.; Abraham, T.; Pan, W.; Tang, X.; Linton, S.S.; McGovern, C.O.; Loc, W.S.; Smith, J.P.; Butler, P.J.; Kester, M.; et al. A Cholecystokinin B Receptor-Specific DNA Aptamer for Targeting Pancreatic Ductal Adenocarcinoma. Nucleic Acid. Ther. 2017, 27, 23–35. [Google Scholar] [CrossRef]
- Trono, J.D.; Mizuno, K.; Yusa, N.; Matsukawa, T.; Yokoyama, K.; Uesaka, M. Size, concentration and incubation time dependence of gold nanoparticle uptake into pancreas cancer cells and its future application to X-Ray Drug Delivery System. J. Radiat. Res. 2011, 52, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Holbrook, R.J.; Rammohan, N.; Rotz, M.W.; MacRenaris, K.W.; Preslar, A.T.; Meade, T.J. Gd(III)-Dithiolane Gold Nanoparticles for T1-Weighted Magnetic Resonance Imaging of the Pancreas. Nano Lett. 2016, 16, 3202–3209. [Google Scholar] [CrossRef] [PubMed]
- He, Y.; Song, W.; Lei, J.; Li, Z.; Cao, J.; Huang, S.; Meng, J.; Xu, H.; Jin, Z.; Xue, H. Anti-CXCR4 monoclonal antibody conjugated to ultrasmall superparamagnetic iron oxide nanoparticles in an application of MR molecular imaging of pancreatic cancer cell lines. Acta Radiol. 2012, 53, 1049–1058. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Yin, H.; Bi, R.; Gao, G.; Li, K.; Liu, H.L. ENO1-targeted superparamagnetic iron oxide nanoparticles for detecting pancreatic cancer by magnetic resonance imaging. J. Cell Mol. Med. 2020, 24, 5751–5757. [Google Scholar] [CrossRef]
- Vahrmeijer, A.L.; Hutteman, M.; van der Vorst, J.R.; van de Velde, C.J.; Frangioni, J.V. Image-guided cancer surgery using near-infrared fluorescence. Nat. Rev. Clin. Oncol. 2013, 10, 507–518. [Google Scholar] [CrossRef]
- Han, H.; Wang, J.; Chen, T.; Yin, L.; Jin, Q.; Ji, J. Enzyme-sensitive gemcitabine conjugated albumin nanoparticles as a versatile theranostic nanoplatform for pancreatic cancer treatment. J. Colloid. Interface Sci. 2017, 507, 217–224. [Google Scholar] [CrossRef]
- Alves, C.G.; Lima-Sousa, R.; de Melo-Diogo, D.; Louro, R.O.; Correia, I.J. IR780 based nanomaterials for cancer imaging and photothermal, photodynamic and combinatorial therapies. Int. J. Pharm. 2018, 542, 164–175. [Google Scholar] [CrossRef]
- Abraham, T.; McGovern, C.O.; Linton, S.S.; Wilczynski, Z.; Adair, J.H.; Matters, G.L. Aptamer-Targeted Calcium Phosphosilicate Nanoparticles for Effective Imaging of Pancreatic and Prostate Cancer. Int. J. Nanomed. 2021, 16, 2297–2309. [Google Scholar] [CrossRef]
- Singhi, A.D.; Koay, E.J.; Chari, S.T.; Maitra, A. Early Detection of Pancreatic Cancer: Opportunities and Challenges. Gastroenterology 2019, 156, 2024–2040. [Google Scholar] [CrossRef]
- Liu, Y.; Ai, K.; Lu, L. Nanoparticulate X-ray computed tomography contrast agents: From design validation to in vivo applications. Acc. Chem. Res. 2012, 45, 1817–1827. [Google Scholar] [CrossRef]
- Hu, X.; Sun, J.; Li, F.; Li, R.; Wu, J.; He, J.; Wang, N.; Liu, J.; Wang, S.; Zhou, F.; et al. Renal-Clearable Hollow Bismuth Subcarbonate Nanotubes for Tumor Targeted Computed Tomography Imaging and Chemoradiotherapy. Nano Lett. 2018, 18, 1196–1204. [Google Scholar] [CrossRef] [PubMed]
- Davies, J.; Siebenhandl-Wolff, P.; Tranquart, F.; Jones, P.; Evans, P. Gadolinium: Pharmacokinetics and toxicity in humans and laboratory animals following contrast agent administration. Arch. Toxicol. 2022, 96, 403–429. [Google Scholar] [CrossRef] [PubMed]
- Zhou, M.; Tian, M.; Li, C. Copper-Based Nanomaterials for Cancer Imaging and Therapy. Bioconjugate Chem. 2016, 27, 1188–1199. [Google Scholar] [CrossRef]
- Yeh, R.; Dercle, L.; Garg, I.; Wang, Z.J.; Hough, D.M.; Goenka, A.H. The Role of 18F-FDG PET/CT and PET/MRI in Pancreatic Ductal Adenocarcinoma. Abdom. Radiol. 2018, 43, 415–434. [Google Scholar] [CrossRef]
- Chakrabarti, A.; Zhang, K.; Aruva, M.R.; Cardi, C.A.; Opitz, A.W.; Wagner, N.J.; Thakur, M.L.; Wickstrom, E. Radiohybridization PET imaging of KRAS G12D mRNA expression in human pancreas cancer xenografts with [(64)Cu]DO3A-peptide nucleic acid-peptide nanoparticles. Cancer Biol. Ther. 2007, 6, 948–956. [Google Scholar] [CrossRef]
- Pérez-Medina, C.; Abdel-Atti, D.; Tang, J.; Zhao, Y.; Fayad, Z.A.; Lewis, J.S.; Mulder, W.J.M.; Reiner, T. Nanoreporter PET predicts the efficacy of anti-cancer nanotherapy. Nat. Commun. 2016, 7, 11838. [Google Scholar] [CrossRef]
- Sharbeen, G.; McCarroll, J.A.; Akerman, A.; Kopecky, C.; Youkhana, J.; Kokkinos, J.; Holst, J.; Boyer, C.; Erkan, M.; Goldstein, D.; et al. Cancer-Associated Fibroblasts in Pancreatic Ductal Adenocarcinoma Determine Response to SLC7A11 Inhibition. Cancer Res. 2021, 81, 3461–3479. [Google Scholar] [CrossRef]
- Lo, J.H.; Hao, L.; Muzumdar, M.D.; Raghavan, S.; Kwon, E.J.; Pulver, E.M.; Hsu, F.; Aguirre, A.J.; Wolpin, B.M.; Fuchs, C.S.; et al. iRGD-guided Tumor-penetrating Nanocomplexes for Therapeutic siRNA Delivery to Pancreatic Cancer. Mol. Cancer Ther. 2018, 17, 2377–2388. [Google Scholar] [CrossRef]
- Ellermeier, J.; Wei, J.; Duewell, P.; Hoves, S.; Stieg, M.R.; Adunka, T.; Noerenberg, D.; Anders, H.J.; Mayr, D.; Poeck, H.; et al. Therapeutic efficacy of bifunctional siRNA combining TGF-β1 silencing with RIG-I activation in pancreatic cancer. Cancer Res. 2013, 73, 1709–1720. [Google Scholar] [CrossRef]
- Zhang, B.; Jiang, T.; Shen, S.; She, X.; Tuo, Y.; Hu, Y.; Pang, Z.; Jiang, X. Cyclopamine disrupts tumor extracellular matrix and improves the distribution and efficacy of nanotherapeutics in pancreatic cancer. Biomaterials 2016, 103, 12–21. [Google Scholar] [CrossRef]
- Liu, X.J.; Li, L.; Liu, X.J.; Li, Y.; Zhao, C.Y.; Wang, R.Q.; Zhen, Y.S. Mithramycin-loaded mPEG-PLGA nanoparticles exert potent antitumor efficacy against pancreatic carcinoma. Int. J. Nanomed. 2017, 12, 5255–5269. [Google Scholar] [CrossRef] [PubMed]
- Noorani, M.; Azarpira, N.; Karimian, K.; Heli, H. Erlotinib-loaded albumin nanoparticles: A novel injectable form of erlotinib and its in vivo efficacy against pancreatic adenocarcinoma ASPC-1 and PANC-1 cell lines. Int. J. Pharm. 2017, 531, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Liu, X.; Zhou, Q.; Sui, M.; Lu, Z.; Zhou, Z.; Tang, J.; Miao, Y.; Zheng, M.; Wang, W.; et al. Terminating the criminal collaboration in pancreatic cancer: Nanoparticle-based synergistic therapy for overcoming fibroblast-induced drug resistance. Biomaterials 2017, 144, 105–118. [Google Scholar] [CrossRef] [PubMed]
- Shabana, A.M.; Kambhampati, S.P.; Hsia, R.C.; Kannan, R.M.; Kokkoli, E. Thermosensitive and biodegradable hydrogel encapsulating targeted nanoparticles for the sustained co-delivery of gemcitabine and paclitaxel to pancreatic cancer cells. Int. J. Pharm. 2021, 593, 120139. [Google Scholar] [CrossRef]
- Yang, W.; Hu, Q.; Xu, Y.; Liu, H.; Zhong, L. Antibody fragment-conjugated gemcitabine and paclitaxel-based liposome for effective therapeutic efficacy in pancreatic cancer. Mater. Sci. Eng. C Mater. Biol. Appl. 2018, 89, 328–335. [Google Scholar] [CrossRef]
- Wei, Y.; Wang, Y.; Xia, D.; Guo, S.; Wang, F.; Zhang, X.; Gan, Y. Thermosensitive Liposomal Codelivery of HSA-Paclitaxel and HSA-Ellagic Acid Complexes for Enhanced Drug Perfusion and Efficacy Against Pancreatic Cancer. ACS Appl. Mater. Interfaces 2017, 9, 25138–25151. [Google Scholar] [CrossRef]
- Maniam, G.; Mai, C.W.; Zulkefeli, M.; Fu, J.Y. Co-encapsulation of gemcitabine and tocotrienols in nanovesicles enhanced efficacy in pancreatic cancer. Nanomedicine 2021, 16, 373–389. [Google Scholar] [CrossRef]
- Shaji, S.G.; Patel, P.; Mamani, U.F.; Guo, Y.; Koirala, S.; Lin, C.Y.; Alahmari, M.; Omoscharka, E.; Cheng, K. Delivery of a STING Agonist Using Lipid Nanoparticles Inhibits Pancreatic Cancer Growth. Int. J. Nanomed. 2024, 19, 8769–8778. [Google Scholar] [CrossRef]
- Ji, T.; Li, S.; Zhang, Y.; Lang, J.; Ding, Y.; Zhao, X.; Zhao, R.; Li, Y.; Shi, J.; Hao, J.; et al. An MMP-2 Responsive Liposome Integrating Antifibrosis and Chemotherapeutic Drugs for Enhanced Drug Perfusion and Efficacy in Pancreatic Cancer. ACS Appl. Mater. Interfaces 2016, 8, 3438–3445. [Google Scholar] [CrossRef]
- Zhao, J.; Xiao, Z.; Li, T.; Chen, H.; Yuan, Y.; Wang, Y.A.; Hsiao, C.H.; Chow, D.S.; Overwijk, W.W.; Li, C. Stromal Modulation Reverses Primary Resistance to Immune Checkpoint Blockade in Pancreatic Cancer. ACS Nano 2018, 12, 9881–9893. [Google Scholar] [CrossRef]
- Mondal, G.; Almawash, S.; Chaudhary, A.K.; Mahato, R.I. EGFR-Targeted Cationic Polymeric Mixed Micelles for Codelivery of Gemcitabine and miR-205 for Treating Advanced Pancreatic Cancer. Mol. Pharm. 2017, 14, 3121–3133. [Google Scholar] [CrossRef] [PubMed]
- Ray, P.; Confeld, M.; Borowicz, P.; Wang, T.; Mallik, S.; Quadir, M. PEG-b-poly (carbonate)-derived nanocarrier platform with pH-responsive properties for pancreatic cancer combination therapy. Colloids Surf. B Biointerfaces 2019, 174, 126–135. [Google Scholar] [CrossRef] [PubMed]
- Shen, J.; Sun, C.; Wang, Z.; Chu, Z.; Liu, C.; Xu, X.; Xia, M.; Zhao, M.; Wang, C. Sequential receptor-mediated mixed-charge nanomedicine to target pancreatic cancer, inducing immunogenic cell death and reshaping the tumor microenvironment. Int. J. Pharm. 2021, 601, 120553. [Google Scholar] [CrossRef] [PubMed]
- Xin, X.; Lin, F.; Wang, Q.; Yin, L.; Mahato, R.I. ROS-Responsive Polymeric Micelles for Triggered Simultaneous Delivery of PLK1 Inhibitor/miR-34a and Effective Synergistic Therapy in Pancreatic Cancer. ACS Appl. Mater. Interfaces 2019, 11, 14647–14659. [Google Scholar] [CrossRef]
- Han, X.; Li, Y.; Xu, Y.; Zhao, X.; Zhang, Y.; Yang, X.; Wang, Y.; Zhao, R.; Anderson, G.J.; Zhao, Y.; et al. Reversal of pancreatic desmoplasia by re-educating stellate cells with a tumour microenvironment-activated nanosystem. Nat. Commun. 2018, 9, 3390. [Google Scholar] [CrossRef]
- Mo, Y.; He, L.; Lai, Z.; Wan, Z.; Chen, Q.; Pan, S.; Li, L.; Li, D.; Huang, J.; Xue, F.; et al. Gold nano-particles (AuNPs) carrying miR-326 targets PDK1/AKT/c-myc axis in hepatocellular carcinoma. Artif. Cells Nanomed. Biotechnol. 2019, 47, 2830–2837. [Google Scholar] [CrossRef]
- Banik, B.L.; Fattahi, P.; Brown, J.L. Polymeric nanoparticles: The future of nanomedicine. Wiley Interdiscip. Rev. Nanomed. Nanobiotechnol. 2016, 8, 271–299. [Google Scholar] [CrossRef]
- Afzal, M.; Ameeduzzafar; Alharbi, K.S.; Alruwaili, N.K.; Al-Abassi, F.A.; Al-Malki, A.A.L.; Kazmi, I.; Kumar, V.; Kamal, M.A.; Nadeem, M.S.; et al. Nanomedicine in treatment of breast cancer—A challenge to conventional therapy. Semin. Cancer Biol. 2021, 69, 279–292. [Google Scholar] [CrossRef]
- Barman, S.; Fatima, I.; Singh, A.B.; Dhawan, P. Pancreatic Cancer and Therapy: Role and Regulation of Cancer Stem Cells. Int. J. Mol. Sci. 2021, 22, 4765. [Google Scholar] [CrossRef]
- McCarroll, J.A.; Sharbeen, G.; Liu, J.; Youkhana, J.; Goldstein, D.; McCarthy, N.; Limbri, L.F.; Dischl, D.; Ceyhan, G.O.; Erkan, M.; et al. βIII-tubulin: A novel mediator of chemoresistance and metastases in pancreatic cancer. Oncotarget 2015, 6, 2235–2249. [Google Scholar] [CrossRef]
- Teo, J.; McCarroll, J.A.; Boyer, C.; Youkhana, J.; Sagnella, S.M.; Duong, H.T.; Liu, J.; Sharbeen, G.; Goldstein, D.; Davis, T.P.; et al. A Rationally Optimized Nanoparticle System for the Delivery of RNA Interference Therapeutics into Pancreatic Tumors In Vivo. Biomacromolecules 2016, 17, 2337–2351. [Google Scholar] [CrossRef] [PubMed]
- Frampton, A.E.; Castellano, L.; Colombo, T.; Giovannetti, E.; Krell, J.; Jacob, J.; Pellegrino, L.; Roca-Alonso, L.; Funel, N.; Gall, T.M.; et al. MicroRNAs cooperatively inhibit a network of tumor suppressor genes to promote pancreatic tumor growth and progression. Gastroenterology 2014, 146, 268–277.e218. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Chen, Y.; Li, J.; Zhang, Z.; Huang, C.; Lian, G.; Yang, K.; Chen, S.; Lin, Y.; Wang, L.; et al. Co-delivery of microRNA-21 antisense oligonucleotides and gemcitabine using nanomedicine for pancreatic cancer therapy. Cancer Sci. 2017, 108, 1493–1503. [Google Scholar] [CrossRef] [PubMed]
- Taniguchi, H.; Natori, Y.; Miyagi, Y.; Hayashi, K.; Nagamura, F.; Kataoka, K.; Imai, K. Treatment of primary and metastatic breast and pancreatic tumors upon intravenous delivery of a PRDM14-specific chimeric siRNA/nanocarrier complex. Int. J. Cancer 2021, 149, 646–656. [Google Scholar] [CrossRef] [PubMed]
- Quiñonero, F.; Parra-Torrejón, B.; Ramírez-Rodríguez, G.B.; Garcés, V.; Delgado-López, J.M.; Jiménez-Luna, C.; Perazzoli, G.; Melguizo, C.; Prados, J.; Ortíz, R. Combining Olaparib and Ascorbic Acid on Nanoparticles to Enhance the Drug Toxic Effects in Pancreatic Cancer. Int. J. Nanomed. 2023, 18, 5075–5093. [Google Scholar] [CrossRef]
- Guo, H.; Hu, Z.; Yang, X.; Yuan, Z.; Wang, M.; Chen, C.; Xie, L.; Gao, Y.; Li, W.; Bai, Y.; et al. Smad4 regulates TGF-β1-mediated hedgehog activation to promote epithelial-to-mesenchymal transition in pancreatic cancer cells by suppressing Gli1 activity. Comput. Struct. Biotechnol. J. 2024, 23, 1189–1200. [Google Scholar] [CrossRef]
- Torres, C.; Linares, A.; Alejandre, M.J.; Palomino-Morales, R.J.; Delgado, J.R.; Perales, S. Interplay Between Gemcitabine and Erlotinib Over Pancreatic Adenocarcinoma Cells. Pancreas 2016, 45, 269–280. [Google Scholar] [CrossRef]
- Miyabayashi, K.; Ijichi, H.; Mohri, D.; Tada, M.; Yamamoto, K.; Asaoka, Y.; Ikenoue, T.; Tateishi, K.; Nakai, Y.; Isayama, H.; et al. Erlotinib prolongs survival in pancreatic cancer by blocking gemcitabine-induced MAPK signals. Cancer Res. 2013, 73, 2221–2234. [Google Scholar] [CrossRef]
- Li, J.M.; Chen, W.; Wang, H.; Jin, C.; Yu, X.J.; Lu, W.Y.; Cui, L.; Fu, D.L.; Ni, Q.X.; Hou, H.M. Preparation of albumin nanospheres loaded with gemcitabine and their cytotoxicity against BXPC-3 cells in vitro. Acta Pharmacol. Sin. 2009, 30, 1337–1343. [Google Scholar] [CrossRef]
- Ernsting, M.J.; Hoang, B.; Lohse, I.; Undzys, E.; Cao, P.; Do, T.; Gill, B.; Pintilie, M.; Hedley, D.; Li, S.D. Targeting of metastasis-promoting tumor-associated fibroblasts and modulation of pancreatic tumor-associated stroma with a carboxymethylcellulose-docetaxel nanoparticle. J. Control Release 2015, 206, 122–130. [Google Scholar] [CrossRef]
- Chen, D.; Zhu, X.; Tao, W.; Kong, Y.; Huag, Y.; Zhang, Y.; Liu, R.; Jiang, L.; Tang, Y.; Yu, H.; et al. Regulation of pancreatic cancer microenvironment by an intelligent gemcitabine@nanogel system via in vitro 3D model for promoting therapeutic efficiency. J. Control Release 2020, 324, 545–559. [Google Scholar] [CrossRef] [PubMed]
- Nie, Y.; Li, D.; Peng, Y.; Wang, S.; Hu, S.; Liu, M.; Ding, J.; Zhou, W. Metal organic framework coated MnO(2) nanosheets delivering doxorubicin and self-activated DNAzyme for chemo-gene combinatorial treatment of cancer. Int. J. Pharm. 2020, 585, 119513. [Google Scholar] [CrossRef] [PubMed]
- Shali, H.; Shabani, M.; Pourgholi, F.; Hajivalili, M.; Aghebati-Maleki, L.; Jadidi-Niaragh, F.; Baradaran, B.; Movassaghpour Akbari, A.A.; Younesi, V.; Yousefi, M. Co-delivery of insulin-like growth factor 1 receptor specific siRNA and doxorubicin using chitosan-based nanoparticles enhanced anticancer efficacy in A549 lung cancer cell line. Artif. Cells Nanomed. Biotechnol. 2018, 46, 293–302. [Google Scholar] [CrossRef] [PubMed]
- Yu, N.; Zhang, X.; Zhong, H.; Mu, J.; Li, X.; Liu, T.; Shi, X.; Liang, X.J.; Guo, S. Stromal Homeostasis-Restoring Nanomedicine Enhances Pancreatic Cancer Chemotherapy. Nano Lett. 2022, 22, 8744–8754. [Google Scholar] [CrossRef]
- Piwowarczyk, L.; Kucinska, M.; Tomczak, S.; Mlynarczyk, D.T.; Piskorz, J.; Goslinski, T.; Murias, M.; Jelinska, A. Liposomal Nanoformulation as a Carrier for Curcumin and pEGCG-Study on Stability and Anticancer Potential. Nanomaterials 2022, 12, 1274. [Google Scholar] [CrossRef]
- Ko, A.H. Nanomedicine developments in the treatment of metastatic pancreatic cancer: Focus on nanoliposomal irinotecan. Int. J. Nanomed. 2016, 11, 1225–1235. [Google Scholar] [CrossRef]
- Frese, K.K.; Neesse, A.; Cook, N.; Bapiro, T.E.; Lolkema, M.P.; Jodrell, D.I.; Tuveson, D.A. nab-Paclitaxel potentiates gemcitabine activity by reducing cytidine deaminase levels in a mouse model of pancreatic cancer. Cancer Discov. 2012, 2, 260–269. [Google Scholar] [CrossRef]
- Meng, H.; Wang, M.; Liu, H.; Liu, X.; Situ, A.; Wu, B.; Ji, Z.; Chang, C.H.; Nel, A.E. Use of a lipid-coated mesoporous silica nanoparticle platform for synergistic gemcitabine and paclitaxel delivery to human pancreatic cancer in mice. ACS Nano 2015, 9, 3540–3557. [Google Scholar] [CrossRef]
- Hingorani, S.R.; Zheng, L.; Bullock, A.J.; Seery, T.E.; Harris, W.P.; Sigal, D.S.; Braiteh, F.; Ritch, P.S.; Zalupski, M.M.; Bahary, N.; et al. HALO 202: Randomized Phase II Study of PEGPH20 Plus Nab-Paclitaxel/Gemcitabine Versus Nab-Paclitaxel/Gemcitabine in Patients With Untreated, Metastatic Pancreatic Ductal Adenocarcinoma. J. Clin. Oncol. 2018, 36, 359–366. [Google Scholar] [CrossRef]
- Rao, D.D.; Luo, X.; Wang, Z.; Jay, C.M.; Brunicardi, F.C.; Maltese, W.; Manning, L.; Senzer, N.; Nemunaitis, J. KRAS mutant allele-specific expression knockdown in pancreatic cancer model with systemically delivered bi-shRNA KRAS lipoplex. PLoS ONE 2018, 13, e0193644. [Google Scholar] [CrossRef]
- Wan, Z.; Huang, H.; West, R.E., 3rd; Zhang, M.; Zhang, B.; Cai, X.; Zhang, Z.; Luo, Z.; Chen, Y.; Zhang, Y.; et al. Overcoming pancreatic cancer immune resistance by codelivery of CCR2 antagonist using a STING-activating gemcitabine-based nanocarrier. Mater. Today 2023, 62, 33–50. [Google Scholar] [CrossRef]
- Hwang, D.; Ramsey, J.D.; Kabanov, A.V. Polymeric micelles for the delivery of poorly soluble drugs: From nanoformulation to clinical approval. Adv. Drug Deliv. Rev. 2020, 156, 80–118. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Zhou, W.; Liang, C.; Shi, S.; Yu, X.; Chen, Q.; Sun, T.; Lu, Y.; Zhang, Y.; Guo, Q.; et al. Codelivery Nanosystem Targeting the Deep Microenvironment of Pancreatic Cancer. Nano Lett. 2019, 19, 3527–3534. [Google Scholar] [CrossRef]
- Li, X.; Zhong, H.; Zheng, S.; Mu, J.; Yu, N.; Guo, S. Tumor-penetrating iRGD facilitates penetration of poly(floxuridine-ketal)-based nanomedicine for enhanced pancreatic cancer therapy. J. Control Release 2024, 369, 444–457. [Google Scholar] [CrossRef]
- Vetvicka, D.; Sivak, L.; Jogdeo, C.M.; Kumar, R.; Khan, R.; Hang, Y.; Oupický, D. Gene silencing delivery systems for the treatment of pancreatic cancer: Where and what to target next? J. Control Release 2021, 331, 246–259. [Google Scholar] [CrossRef]
- Kumar, V.; Mondal, G.; Slavik, P.; Rachagani, S.; Batra, S.K.; Mahato, R.I. Codelivery of small molecule hedgehog inhibitor and miRNA for treating pancreatic cancer. Mol. Pharm. 2015, 12, 1289–1298. [Google Scholar] [CrossRef]
- Daman, Z.; Montazeri, H.; Azizi, M.; Rezaie, F.; Ostad, S.N.; Amini, M.; Gilani, K. Polymeric Micelles of PEG-PLA Copolymer as a Carrier for Salinomycin Against Gemcitabine-Resistant Pancreatic Cancer. Pharm. Res. 2015, 32, 3756–3767. [Google Scholar] [CrossRef]
- Pittella, F.; Miyata, K.; Maeda, Y.; Suma, T.; Watanabe, S.; Chen, Q.; Christie, R.J.; Osada, K.; Nishiyama, N.; Kataoka, K. Pancreatic cancer therapy by systemic administration of VEGF siRNA contained in calcium phosphate/charge-conversional polymer hybrid nanoparticles. J. Control Release 2012, 161, 868–874. [Google Scholar] [CrossRef]
- Yu, M.; Zhao, M.; Yu, R.; Chu, S.; Xu, J.; Xia, M.; Wang, C. [Nanotechnology-mediated immunochemotherapy with Ingenol-3-Mebutate for Systematic Anti-tumor Effects]. J. Control Release 2019, 304, 242–258. [Google Scholar] [CrossRef]
- Zhao, J.; Wang, H.; Hsiao, C.H.; Chow, D.S.; Koay, E.J.; Kang, Y.; Wen, X.; Huang, Q.; Ma, Y.; Bankson, J.A.; et al. Simultaneous inhibition of hedgehog signaling and tumor proliferation remodels stroma and enhances pancreatic cancer therapy. Biomaterials 2018, 159, 215–228. [Google Scholar] [CrossRef]
- Sun, J.; Chen, Y.; Xu, J.; Song, X.; Wan, Z.; Du, Y.; Ma, W.; Li, X.; Zhang, L.; Li, S. High Loading of Hydrophobic and Hydrophilic Agents via Small Immunostimulatory Carrier for Enhanced Tumor Penetration and Combinational Therapy. Theranostics 2020, 10, 1136–1150. [Google Scholar] [CrossRef] [PubMed]
- Núñez, C.; Estévez, S.V.; Del Pilar Chantada, M. Inorganic nanoparticles in diagnosis and treatment of breast cancer. J. Biol. Inorg. Chem. 2018, 23, 331–345. [Google Scholar] [CrossRef] [PubMed]
- Mardhian, D.F.; Storm, G.; Bansal, R.; Prakash, J. Nano-targeted relaxin impairs fibrosis and tumor growth in pancreatic cancer and improves the efficacy of gemcitabine in vivo. J. Control Release 2018, 290, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Zhou, H.; Qian, W.; Uckun, F.M.; Wang, L.; Wang, Y.A.; Chen, H.; Kooby, D.; Yu, Q.; Lipowska, M.; Staley, C.A.; et al. IGF1 Receptor Targeted Theranostic Nanoparticles for Targeted and Image-Guided Therapy of Pancreatic Cancer. ACS Nano 2015, 9, 7976–7991. [Google Scholar] [CrossRef]
- Zheng, P.; Xu, D.; Cai, Y.; Zhu, L.; Xiao, Q.; Peng, W.; Chen, B. A multi-omic analysis reveals that Gamabufotalin exerts anti-hepatocellular carcinoma effects by regulating amino acid metabolism through targeting STAMBPL1. Phytomedicine 2024, 135, 156094. [Google Scholar] [CrossRef]
- Huo, D.; Liu, S.; Zhang, C.; He, J.; Zhou, Z.; Zhang, H.; Hu, Y. Hypoxia-Targeting, Tumor Microenvironment Responsive Nanocluster Bomb for Radical-Enhanced Radiotherapy. ACS Nano 2017, 11, 10159–10174. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Biomarker | Nanomaterials | Sample | Sources | Outcomes | Reference |
|---|---|---|---|---|---|
| CA19-9 | polythionine-Au composites | Serum | Human | a detection limit of 0.26 U/mL at a signal-to-noise ratio of 3 | [13] |
| CEA | a novel enzyme-labeled gold nanoparticle probe | Serum | Human | a detection limit of 12 ng/L | [14] |
| MUC4 | Au NP | Serum | Human | a high sensitive detection of a single AuNP | [15] |
| miRs | AuNP with a localized surface plasmon resonance sensor | Plasma | Human | allowed for the simultaneous measurement of multiple miRs | [16] |
| miRs | α-hemolysin (αHL) single nanopore | miRNA reagents | _ | distinguished complex molecular signals of miR-21, miR-155, and miR-196a | [17] |
| Evs | semiconductor nanomaterial-based rapid fluorescence immunoassay | Serum | Human | improved the ability of serum levels of EV EpCAM and EV EphA2 | [18] |
| Evs | lternating current (AC) electrokinetic microarray chip | Whole blood, serum, or plasma | Human | a detection of glypican-1 and CD 63 with 99%sensitivity and 82%specificity | [19] |
| Exosomes | polydopamine (PDA)-modified slide | Serum | Human | a detection limit of 9 × 10−19 mol/L, differentiated stage I-II from stage III tumors with a sensitivity of 95.7% | [20] |
| Regenerating Family Member 1 Alpha | nanobiotinylated liposome based on isothermal amplification | Urine | Human | a detection limit of 1 fg/mL | [21] |
| CA19-9 | screen-printed interdigitated electrodes immobilized with anti-CA19-9 antibodies | Whole cell lysates of colorectal adenocarcinoma | HT-29 cell lines, SW-620 cell lines | a detection limit of 0.12 U/mL | [22] |
| claudin-4 | nanoprobes based on modified apoferritin (mAFTN), functionalizing CdSe (ZnS), Quantum dots(QDs) | Cells | Capan-1 cells | a detection sensitivity 27 times higher than conventional organic fluorophores and 6 times higher than individual QDs | [20] |
| FAP | AuNPs with heterobifunctional polyethylene glycol (PEG) | Tissues | Human | labeled tumor stroma in approximately 5 µm thick | [23] |
| Imaging | Nanosystems | Targeting Molecular | Cell Lines | In Vivo Models | Outcomes | Reference |
|---|---|---|---|---|---|---|
| NIR imaging | bMSN@Cy7.5-FA NPs | Folate receptors | A549, HEPG2 and BxPC-3 cell lines | BxPC-3 orthotopic mouse model | reached a maximum at a post injection time-point of 12 h | [28] |
| NIR imaging | CR@E8-EVs | CDH17 | MKN45 and 4T1 cells | MKN45 orthotopic mouse model | exhibited strong NIR absorption and remarkable active tumor targeting capability | [29] |
| NIR imaging | AP1153-ICG-NJs | CCK-BR | Panc-1 cells | Panc-1 orthotopic mouse model | facilitated delivery of NPs tumors in vivo | [30] |
| CT imaging | AuNPs | _ | PK-1, PK-45, and Panc-1 cells | _ | showed preferential uptake by PDAC cells at an optimal diameter of 20 nm | [31] |
| MR imaging | Lip-Gd@AuNPs | _ | _ | C57 black mice model | identificated the pancreas with contrast-to-noise ratios exceeding 35:1 | [32] |
| MR imaging | CXCR4-USPIO | CXCR4 | AsPC-1, BxPC-3, CFPAC-1, and Panc-1 | _ | semi-quantitatively assessed the cellular CXCR4 expression levels | [33] |
| MR imaging | Dex-g-PCL/SPIO nanoparticles | enolase 1 | CFPAC-1 cell lines, MiaPaCa-2 cell lines | CFPAC-1 xenograft mouse model | enhance the detection of PDAC by in vivo and in vitro MRI | [34] |
| Naoncarriers | Polymers | Targeting Molecule | Drugs | Cell Lines | In Vivo Models | Outcomes | Reference |
|---|---|---|---|---|---|---|---|
| Polymeric NPs | poly(dimethylaminoethyl methacrylate) | SLC7A11 | SLC7A11 siRNA | mouse KPC PDAC cells, human CAFs | KC (Kras-mutated) and KPC (Kras- and p53-mutated) mouse models | reduced CAF activation, inhibited tumor growth and metastases | [47] |
| Polymeric NPs | iRGD TPNs with polyethylene glycol (PEG)-peptide | KRAS | KRAS siRNA | KPC-derived cell lines, MIA PaCa-2 cell lines | MIA PaCa-2 transgenic pancreatic cancer mouse models | enhanced tumor-penetrating ability, inhibit tumor growth | [48] |
| Polymeric NPs | polyethylenimine | TGF-β | TGF-β1 siRNA | PaCa-2 cell lines | PaCa-2 orthotopic pancreatic cancer transplant model | prolong survival, break tumor-induced CD8(+) T cell suppression | [49] |
| Polymeric NPs | PEG-poly (lactic acid) | SMO | CPA | Capan-2 cell lines | Capan-2 xenograft mouse models | improved tumor perfusion, inhibited tumor growth | [50] |
| Polymeric NPs | mPEG-PLGA | transcription factor Sp1 | MIT | BxPC-3 cells, MIA Paca-2 cells | BxPC-3 xenograft mouse models | enhanced tumor-penetrating ability, inhibit tumor growth | [51] |
| Polymeric NPs | albumin nanoparticles | EGFR | erlotinib | ASPC-1 cell lines, PNAC-1 cell lines | _ | reduced durgs dose for killing cells | [52] |
| Nanoliposomal | PEG | TOP1 | smart SN38 and GDC-0449 | PSCs, BxPC-3 cells and MIA PaCa-2 cells | _ | reduced tumor stroma, inhibited tumor growth | [53] |
| Nanoliposomal | poly(δ-valerolactone-co-D,L-lactide)-b-poly(ethylene glycol)-b-poly(δ-valerolactone-co-D,L-lactide) | _ | PTX and GEM | PANC-1 cell lines | _ | reduced toxic side effects, inhibited tumor gorwth, prolonged drug release | [54] |
| Nanoliposomal | 1,2- distearoyl-sn-glycero-3-phosphoethanolamine-N-[methoxy(polye thylene-glycol)-2000] and maleimide | _ | PTX and GEM | BxPC3 cells | _ | increased cytotoxic effect in pancreatic cancer cell, inhibited tumor growth | [55] |
| Nanoliposomal | HAS | _ | PTX and EA | HPaSteC cell lines, BxPC-3 cell lines | BxPC- and HPaSteC-bearing nude mouse model | enhanced tumor accumulation and matrix penetration | [56] |
| Nanoliposomal | smoke nanoparticles | NF-κB | GEM and tocotrienols | Panc 10.05, SW 1990, AsPC-1 and BxPC-3 cells | _ | increased the anti-proliferative effect of GEM | [57] |
| Nanoliposomal | cGAMP LNPs | an endoplasmic reticulum receptor STING | 2′3′-cGAMP, a high-affinity endogenous ligand of STING | Panc02 cells, NIH-3T3 cells, Human Pancreatic Duct Epithelial Cells, DC2.4 cells | Panc-02 and NIH-3T3 xenograft mouse models | increased the cellular uptake of 2′3′-cGAMP | [58] |
| Nanoliposomal | N-hydroxysuccinimide (NHS)/1-ethyl-3-[3-(dimethylamino)propyl] carbodiimide hydrochloride | PSCs | β-CD and MMP-2 | PSCs, Panc-1 cells | pancreatic coimplanted tumor model | increased drug perfusion, decreased the stromal barrier | [59] |
| Micelles | poly(ethylene glycol) with poly(ε-caprolactone) and pendent quaternary ammonium cations | SHH | CPA and PTX | Kras * cells | Kras * orthotopic murine models | enhanced tumor infiltration of CD8+ T cells, prolong the survival time | [60] |
| Micelles | malemido-poly(ethylene glycol)-block-poly(2-methyl-2-carboxyl-propylene carbonate-graft-dodecanol | C225 | GEM and miR205 | MIA PaCa-2R cells | Miapaca-2 orthotopic mouse models | enhanced tumor accumulation of C225-micelles, increased apoptosis and reduced EMT | [61] |
| Micelles | PEG-b-poly (carbonate) | Hh pathway | GEM and GDC-0449 | BxPC-3 cell lines, Mia PaCa-2 cell lines | BxPC-3 xenografts mouse models | suppressed tumor proliferation | [62] |
| Micelles | 2-3-((S)-5-amino-1-carboxy-pentyl)-ureido)-pentanedioate (ACUPA-) and tri-phenylphosphine (TPP+) | _ | I3A | MIAPaCa-2 cells, Panc02 cells | Panc02 PC orthopic mouse models | activated adaptive immunity, prolonged the survival time | [63] |
| Micelles | poly(ethylene glycol)-poly[aspartamidoethyl(p-boronobenzyl)diethylammonium bromide] (PEG-B-PAEBEA) | Bcl-2 | miR-34a mimic, PLK1 inhibitor volasertib (BI6727) | MIA PaCa-2R cell line | NSG mice harboring orthotopic pancreatic tumors model | inhibited tumor growth | [64] |
| Au NPs | PEGylated polyethylenimine-coated gold nanoparticles | PSCs | all-trans retinoic acid and siRNA targeting heat shock protein 47 | Panc-1 cell lines, Mia-PaCa-2 cell line | Panc-1 and PSCs xenograft tumour model | induced PSC quiescence and inhibited ECM hyperplasia | [65] |
| Iron oxide NPs | superparamagnetic iron oxide nanoparticle | CAFs | human relaxin-2 | Primary human pancreatic stellate cells | Panc-1 and hPSCs orthotopic tumor model | inhibited tumor growth | [66] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guo, K.; Li, S.; Wu, X.; Xiong, H. Nanomedicine in the Diagnosis and Treatment of Pancreatic Cancer. Pharmaceutics 2025, 17, 449. https://doi.org/10.3390/pharmaceutics17040449
Guo K, Li S, Wu X, Xiong H. Nanomedicine in the Diagnosis and Treatment of Pancreatic Cancer. Pharmaceutics. 2025; 17(4):449. https://doi.org/10.3390/pharmaceutics17040449
Chicago/Turabian StyleGuo, Kexin, Sicheng Li, Xinyu Wu, and Huihua Xiong. 2025. "Nanomedicine in the Diagnosis and Treatment of Pancreatic Cancer" Pharmaceutics 17, no. 4: 449. https://doi.org/10.3390/pharmaceutics17040449
APA StyleGuo, K., Li, S., Wu, X., & Xiong, H. (2025). Nanomedicine in the Diagnosis and Treatment of Pancreatic Cancer. Pharmaceutics, 17(4), 449. https://doi.org/10.3390/pharmaceutics17040449