
Camellia sinensis (L.) Kuntze Extract Attenuates Ovalbumin-Induced Allergic Asthma by Regulating Airway Inflammation and Mucus Hypersecretion

 , , , , , , , and
, , , , , , , and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Plant Materials
2.2. Extraction Procedure and Chemicals
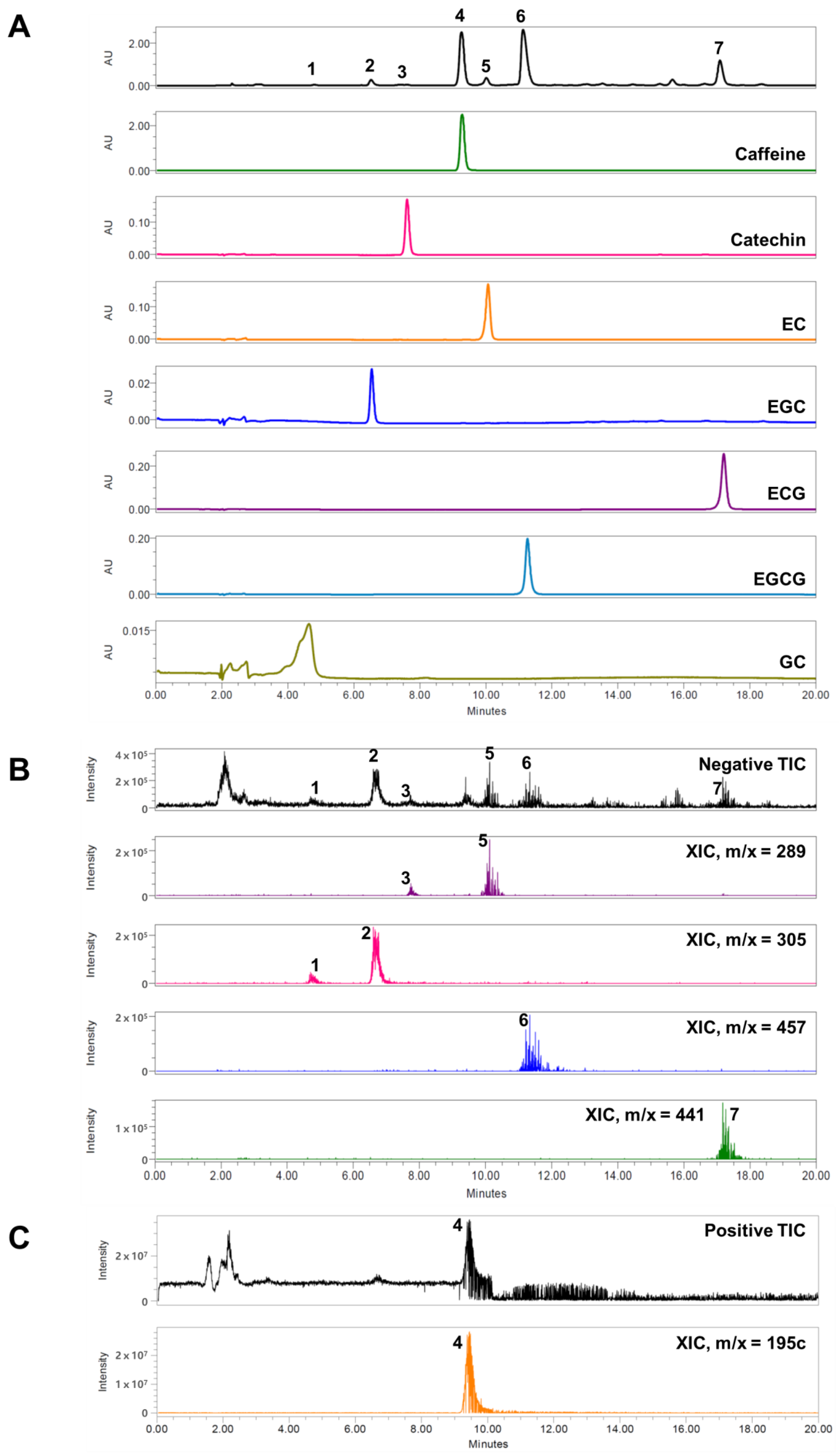
2.3. High-Performance Liquid Chromatography (HPLC) Analysis
2.4. Determination of Nitric Oxide (NO) Generation in RAW 264.7 Cells
2.5. Antioxidant Assay
2.5.1. 2,2-Diphenyl-1-picryl-hydrazyl-hydrate (DPPH) Radical Scavenging Assay
2.5.2. 2,2-Diphenyl-1-picryl-hydrazyl-hydrate (ABTS) Radical Scavenging Assay
2.5.3. Dichlorodihydrofluorescein-diacetate (DCFDA) Assay of the ROS-Scavenging Activity of the Aqueous Larval Extract
2.6. Animals
2.7. Experimental Procedures
2.8. Measurement of Inflammatory Cells in BALF
2.9. Measurement of IL-4 and IgE Levels in BALF
2.10. Histology
2.11. Statistical Analysis
3. Results
3.1. HPLC Analysis
3.2. Effects of CE on Lung Morphology and Mucus Hypersecretion
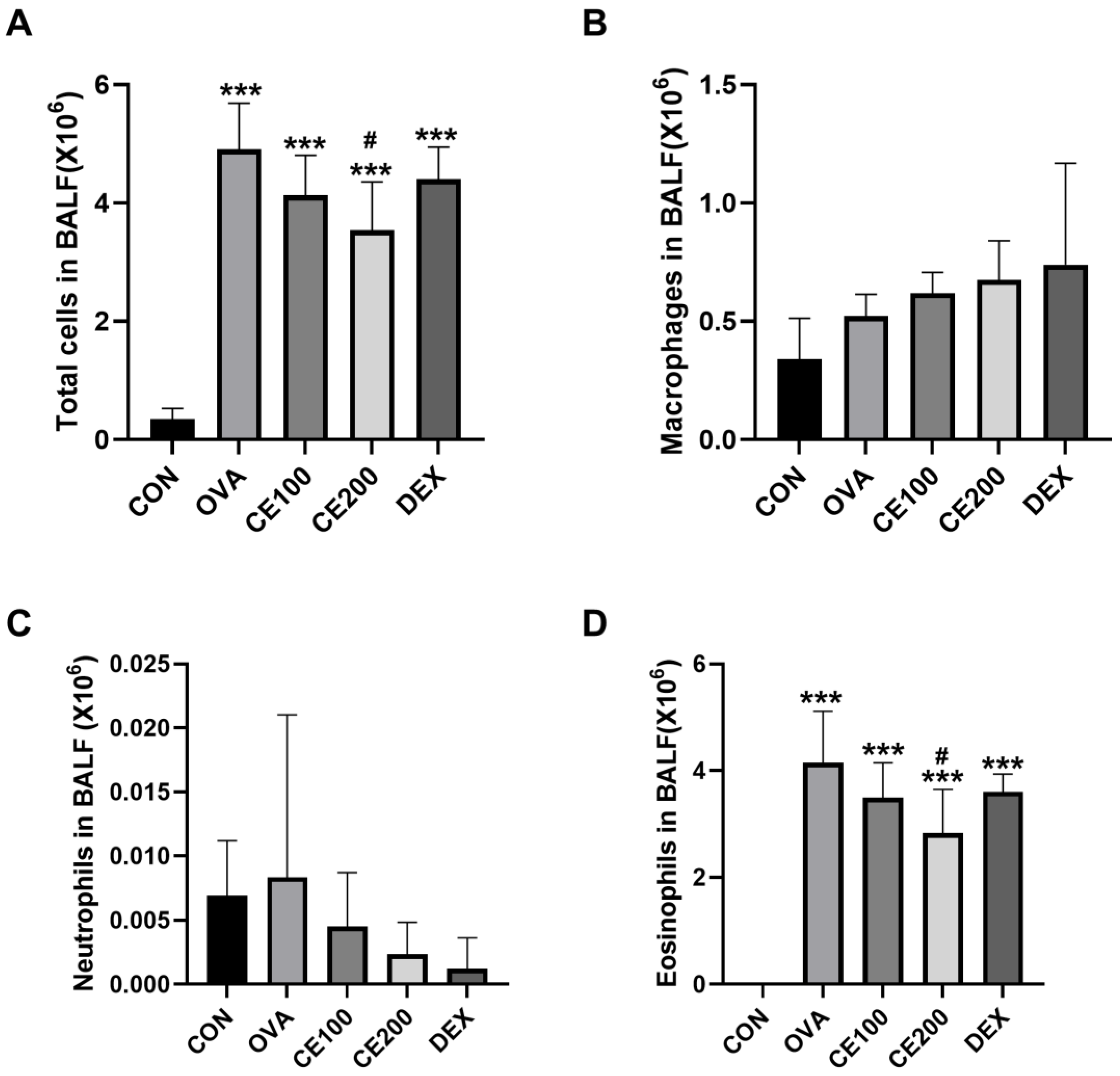
3.3. Effects of CE on Inflammatory Cell Numbers in the BALF of OVA-Induced Asthmatic Model Mice
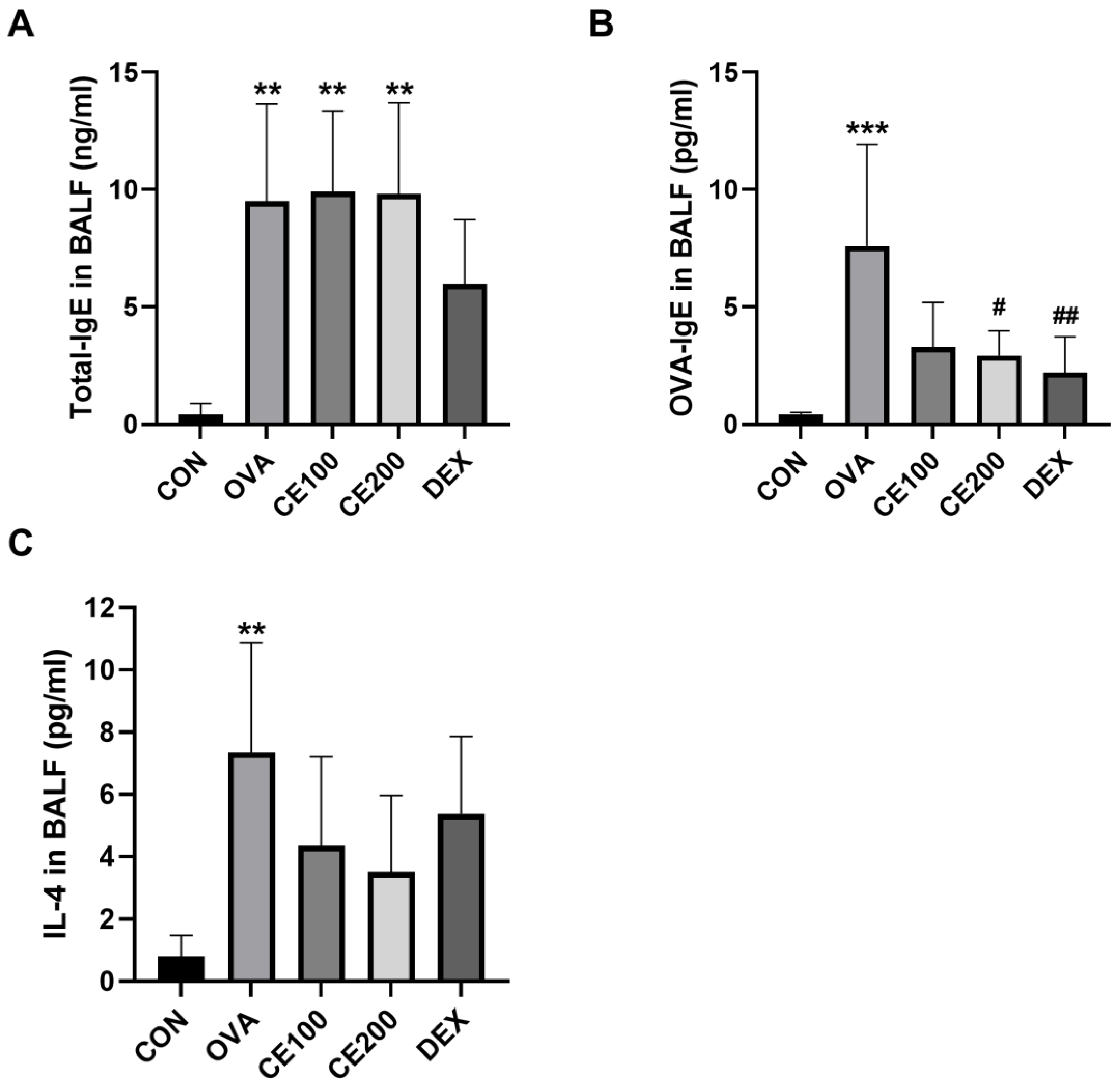
3.4. Effects of CE on IL-4 and IgE Levels in the BALF of Asthmatic Mice
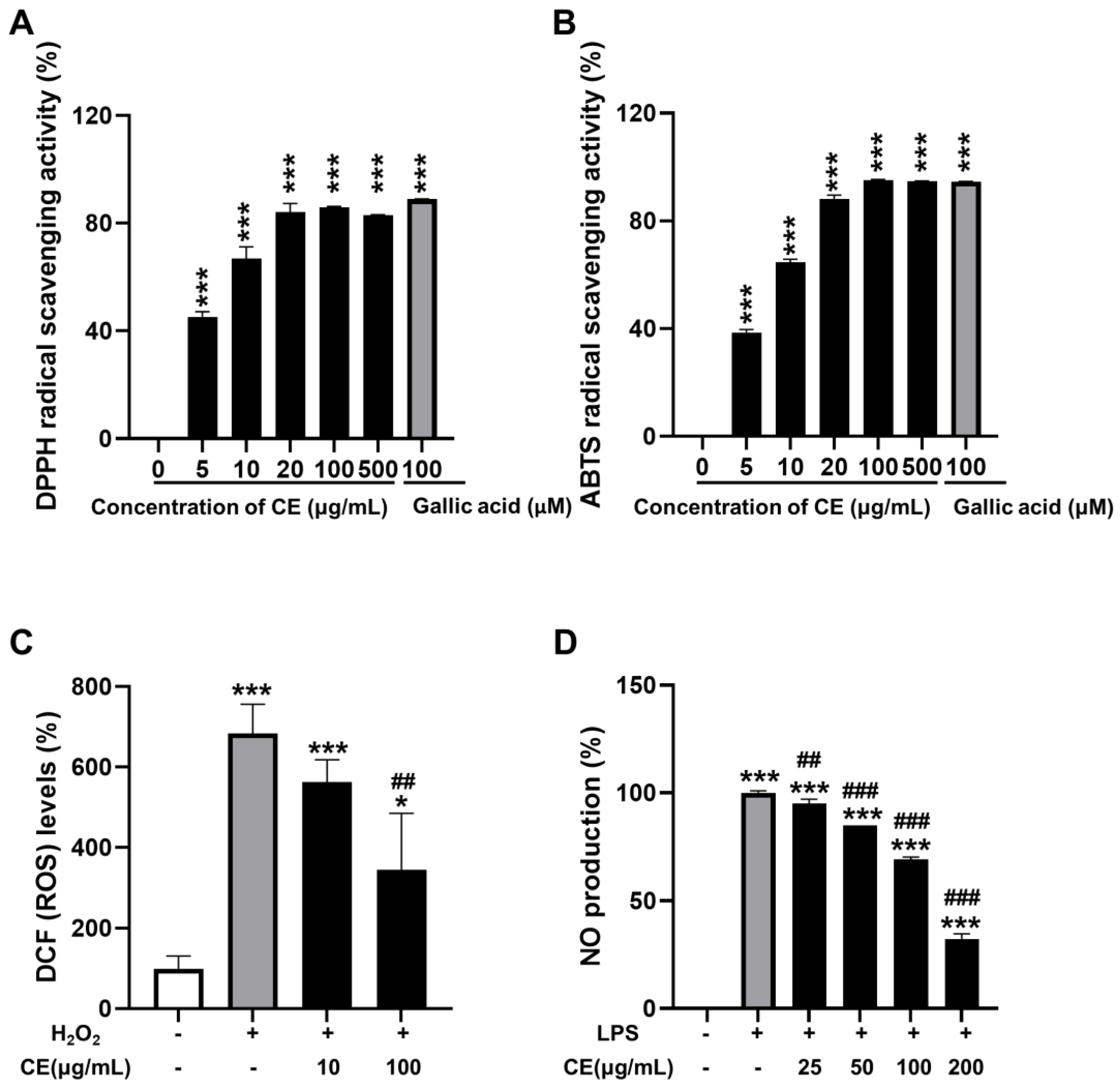
3.5. Effects of CE on Antioxidant and Anti-Inflammatory Activities
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dharmage, S.C.; Perret, J.L.; Custovic, A. Epidemiology of Asthma in Children and Adults. Front. Pediatr. 2019, 7, 246. [Google Scholar] [CrossRef]
- D’Amato, G.; Vitale, C.; Molino, A.; Stanziola, A.; Sanduzzi, A.; Vatrella, A.; Mormile, M.; Lanza, M.; Calabrese, G.; Antonicelli, L.; et al. Asthma-related deaths. Multidiscip. Respir. Med. 2016, 11, 37. [Google Scholar] [CrossRef]
- Papadopoulos, N.G.; Miligkos, M.; Xepapadaki, P. A Current Perspective of Allergic Asthma: From Mechanisms to Management. Handb. Exp. Pharm. 2022, 268, 69–93. [Google Scholar]
- Athari, S.S. Targeting cell signaling in allergic asthma. Signal. Transduct. Target. Ther. 2019, 4, 45. [Google Scholar] [CrossRef]
- Choi, Y.J.; Park, J.Y.; Lee, H.S.; Suh, J.; Song, J.Y.; Byun, M.K.; Cho, J.H.; Kim, H.J.; Lee, J.H.; Park, J.W.; et al. Effect of asthma and asthma medication on the prognosis of patients with COVID-19. Eur. Respir. J. 2021, 57, 2002226. [Google Scholar] [CrossRef]
- Xie, Y.Z.; Peng, C.W.; Su, Z.Q.; Huang, H.T.; Liu, X.H.; Zhan, S.F.; Huang, X.F. A Practical Strategy for Exploring the Pharmacological Mechanism of Luteolin Against COVID-19/Asthma Comorbidity: Findings of System Pharmacology and Bioinformatics Analysis. Front. Immunol. 2021, 12, 769011. [Google Scholar] [CrossRef] [PubMed]
- Boulet, L.P.; Boulay, M.E. Asthma-related comorbidities. Expert Rev. Respir. Med. 2011, 5, 377–393. [Google Scholar] [CrossRef]
- Chung, K.F. Targeting the interleukin pathway in the treatment of asthma. Lancet 2015, 386, 1086–1096. [Google Scholar] [CrossRef]
- Jo, W.S.; Kang, S.; Jeong, S.K.; Bae, M.J.; Lee, C.G.; Son, Y.; Lee, H.J.; Jeong, M.H.; Kim, S.H.; Moon, C.; et al. Low Dose Rate Radiation Regulates M2-like Macrophages in an Allergic Airway Inflammation Mouse Model. Dose Response 2022, 20, 15593258221117349. [Google Scholar] [CrossRef]
- Pak, S.W.; Lee, A.Y.; Seo, Y.S.; Lee, S.J.; Kim, W.I.; Shin, D.H.; Kim, J.C.; Kim, J.S.; Lim, J.O.; Shin, I.S. Anti-asthmatic effects of Phlomis umbrosa Turczaninow using ovalbumin induced asthma murine model and network pharmacology analysis. Biomed. Pharm. 2022, 145, 112410. [Google Scholar] [CrossRef]
- Dunn, R.M.; Wechsler, M.E. Anti-interleukin therapy in asthma. Clin. Pharm. Ther. 2015, 97, 55–65. [Google Scholar] [CrossRef]
- Cooper, V.; Metcalf, L.; Versnel, J.; Upton, J.; Walker, S.; Horne, R. Patient-reported side effects, concerns and adherence to corticosteroid treatment for asthma, and comparison with physician estimates of side-effect prevalence: A UK-wide, cross-sectional study. NPJ Prim. Care Respir. Med. 2015, 25, 15026. [Google Scholar] [CrossRef] [PubMed]
- Samanta, S. Potential Bioactive Components and Health Promotional Benefits of Tea (Camellia sinensis). J. Am. Nutr. Assoc. 2022, 41, 65–93. [Google Scholar] [CrossRef] [PubMed]
- Borah, A.; Hazarika, S.N.; Thakur, D. Potentiality of actinobacteria to combat against biotic and abiotic stresses in tea [Camellia sinensis (L) O. Kuntze]. J. Appl. Microbiol. 2022, 133, 2314–2330. [Google Scholar] [CrossRef] [PubMed]
- Grove, K.A.; Lambert, J.D. Laboratory, epidemiological, and human intervention studies show that tea (Camellia sinensis) may be useful in the prevention of obesity. J. Nutr. 2010, 140, 446–453. [Google Scholar] [CrossRef]
- Chen, F.C.; Shen, K.P.; Ke, L.Y.; Lin, H.L.; Wu, C.C.; Shaw, S.Y. Flavonoids from Camellia sinensis (L.) O. Kuntze seed ameliorates TNF-alpha induced insulin resistance in HepG2 cells. Saudi Pharm. J. 2019, 27, 507–516. [Google Scholar] [CrossRef]
- Koch, W.; Zagorska, J.; Marzec, Z.; Kukula-Koch, W. Applications of Tea (Camellia sinensis) and its Active Constituents in Cosmetics. Molecules 2019, 24, 4277. [Google Scholar] [CrossRef]
- Manian, R.; Anusuya, N.; Siddhuraju, P.; Manian, S. The antioxidant activity and free radical scavenging potential of two different solvent extracts of Camellia sinensis (L.) O. Kuntz, Ficus bengalensis L. and Ficus racemosa L. Food Chem. 2008, 107, 1000–1007. [Google Scholar] [CrossRef]
- Sanchez, M.; Gonzalez-Burgos, E.; Iglesias, I.; Lozano, R.; Gomez-Serranillos, M.P. The Pharmacological Activity of Camellia sinensis (L.) Kuntze on Metabolic and Endocrine Disorders: A Systematic Review. Biomolecules 2020, 10, 603. [Google Scholar] [CrossRef]
- Shivashankara, A.R.; Rao, S.; George, T.; Abraham, S.; Colin, M.D.; Palatty, P.L.; Baliga, M.S. Tea (Camellia sinensis L. Kuntze) as Hepatoprotective Agent: A Revisit. Dietary Interventions in Liver Disease; Elsevier: Amsterdam, The Netherlands, 2019; pp. 183–192. [Google Scholar]
- Ferrazzano, G.F.; Amato, I.; Ingenito, A.; Zarrelli, A.; Pinto, G.; Pollio, A. Plant polyphenols and their anti-cariogenic properties: A review. Molecules 2011, 16, 1486–1507. [Google Scholar] [CrossRef]
- Sharma, R.; Verma, S.; Kumar, D. Polyphenolics and therapeutic insights in different tissues extract and fractions of Camellia sinensis (L.) Kuntze (Kangra Tea). Food Biosci. 2021, 42, 101164. [Google Scholar] [CrossRef]
- Apriningsih, H.; Suradi, S.; Sutanto, Y.S. Effects of Green Tea to Absolute Neutrophil Count, MMP-9,% VEP1, and COPD Assessment Test Scores Stable COPD Patients. J. Respirologi Indones. 2018, 38, 7–15. [Google Scholar] [CrossRef]
- Chan, K.H.; Ho, S.P.; Yeung, S.C.; So, W.H.; Cho, C.H.; Koo, M.W.; Lam, W.K.; Ip, M.S.; Man, R.Y.; Mak, J.C. Chinese green tea ameliorates lung injury in cigarette smoke-exposed rats. Respir. Med. 2009, 103, 1746–1754. [Google Scholar] [CrossRef] [PubMed]
- Chan, K.H.; Chan, S.C.; Yeung, S.C.; Man, R.Y.; Ip, M.S.; Mak, J.C. Inhibitory effect of Chinese green tea on cigarette smoke-induced up-regulation of airway neutrophil elastase and matrix metalloproteinase-12 via antioxidant activity. Free Radic. Res. 2012, 46, 1123–1129. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Wen, J.X.; Hai, L.; Wang, Y.F.; Yan, L.; Gao, W.H.; Hu, Z.D.; Wang, Y.J. Preventive and therapeutic effects of green tea on lung cancer: A narrative review of evidence from clinical and basic research. J. Thorac. Dis. 2022, 14, 5029–5038. [Google Scholar] [CrossRef]
- LeBel, C.P.; Ischiropoulos, H.; Bondy, S.C. Evaluation of the probe 2’, 7’-dichlorofluorescin as an indicator of reactive oxygen species formation and oxidative stress. Chem. Res. Toxicol. 1992, 5, 227–231. [Google Scholar] [CrossRef]
- Azman, S.; Sekar, M.; Bonam, S.R.; Gan, S.H.; Wahidin, S.; Lum, P.T.; Dhadde, S.B. Traditional Medicinal Plants Conferring Protection Against Ovalbumin-Induced Asthma in Experimental Animals: A Review. J. Asthma Allergy 2021, 14, 641–662. [Google Scholar] [CrossRef]
- Cao, M.; Zhan, M.; Wang, Z.; Wang, Z.; Li, X.M.; Miao, M. Development of an Orally Bioavailable Isoliquiritigenin Self-Nanoemulsifying Drug Delivery System to Effectively Treat Ovalbumin-Induced Asthma. Int. J. Nanomed. 2020, 15, 8945–8961. [Google Scholar] [CrossRef]
- Nkhili, E.; Tomao, V.; El Hajji, H.; El Boustani, E.S.; Chemat, F.; Dangles, O. Microwave-assisted water extraction of green tea polyphenols. Phytochem. Anal. 2009, 20, 408–415. [Google Scholar] [CrossRef]
- Yusuf, N.; Irby, C.; Katiyar, S.K.; Elmets, C.A. Photoprotective effects of green tea polyphenols. Photodermatol. Photoimmunol. Photomed. 2007, 23, 48–56. [Google Scholar] [CrossRef]
- Mokra, D.; Adamcakova, J.; Mokry, J. Green Tea Polyphenol (-)-Epigallocatechin-3-Gallate (EGCG): A Time for a New Player in the Treatment of Respiratory Diseases? Antioxidants 2022, 11, 1566. [Google Scholar] [CrossRef] [PubMed]
- Hosseini, S.A.; Shateri, Z.; Abolnezhadian, F.; Maraghi, E.; Shoushtari, M.H.; Zilaee, M. Does pomegranate extract supplementation improve the clinical symptoms of patients with allergic asthma? A double-blind, randomized, placebo-controlled trial. Front. Pharmacol. 2023, 14, 1109966. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.; Patel, V. Inhibitory effects of catechin isolated from Acacia catechu on ovalbumin induced allergic asthma model: Role of histidine decarboxylase. Nutr. Food Sci. 2018, 49, 18–31. [Google Scholar] [CrossRef]
- Singh, A.; Demont, A.; Actis-Goretta, L.; Holvoet, S.; Lévêques, A.; Lepage, M.; Nutten, S.; Mercenier, A. Identification of epicatechin as one of the key bioactive constituents of polyphenol-enriched extracts that demonstrate an anti-allergic effect in a murine model of food allergy. Br. J. Nutr. 2014, 112, 358–368. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; Park, H.J.; Lee, C.M.; Choi, I.W.; Moon, D.O.; Roh, H.J.; Lee, H.K.; Park, Y.M. Epigallocatechin-3-gallate protects toluene diisocyanate-induced airway inflammation in a murine model of asthma. FEBS Lett. 2006, 580, 1883–1890. [Google Scholar] [CrossRef]
- Yang, N.; Shang, Y.X. Epigallocatechin gallate ameliorates airway inflammation by regulating Treg/Th17 imbalance in an asthmatic mouse model. Int. Immunopharmacol. 2019, 72, 422–428. [Google Scholar] [CrossRef]
- Kamihira-Ishijima, M.; Nakazawa, H.; Kira, A.; Naito, A.; Nakayama, T. Inhibitory mechanism of pancreatic amyloid fibril formation: Formation of the complex between tea catechins and the fragment of residues 22–27. Biochemistry 2012, 51, 10167–10174. [Google Scholar] [CrossRef]
- Saeki, K.; Hayakawa, S.; Nakano, S.; Ito, S.; Oishi, Y.; Suzuki, Y.; Isemura, M. In Vitro and In Silico Studies of the Molecular Interactions of Epigallocatechin-3-O-gallate (EGCG) with Proteins That Explain the Health Benefits of Green Tea. Molecules 2018, 23, 1295. [Google Scholar] [CrossRef]
- Ci, X.; Chu, X.; Wei, M.; Yang, X.; Cai, Q.; Deng, X. Different effects of farrerol on an OVA-induced allergic asthma and LPS-induced acute lung injury. PLoS ONE 2012, 7, e34634. [Google Scholar] [CrossRef]
- Lim, C.Y.; Moon, J.M.; Kim, B.Y.; Lim, S.H.; Lee, G.S.; Yu, H.S.; Cho, S.I. Comparative study of Korean White Ginseng and Korean Red Ginseng on efficacies of OVA-induced asthma model in mice. J. Ginseng Res. 2015, 39, 38–45. [Google Scholar] [CrossRef]
- Lee, J.W.; Min, J.H.; Kim, M.G.; Kim, S.M.; Kwon, O.K.; Oh, T.K.; Lee, J.K.; Kim, T.Y.; Lee, S.W.; Choi, S.; et al. Pistacia weinmannifolia root exerts a protective role in ovalbumin induced lung inflammation in a mouse allergic asthma model. Int. J. Mol. Med. 2019, 44, 2171–2180. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.Y.; Seo, C.S.; Lee, N.H.; Ha, H.; Lee, J.A.; Lee, H.; Lee, K.Y.; Shin, H.K. Anti-asthmatic effect of schizandrin on OVA-induced airway inflammation in a murine asthma model. Int. Immunopharmacol. 2010, 10, 1374–1379. [Google Scholar] [CrossRef] [PubMed]
- Chung, M.J.; Park, J.K.; Park, Y.I. Anti-inflammatory effects of low-molecular weight chitosan oligosaccharides in IgE-antigen complex-stimulated RBL-2H3 cells and asthma model mice. Int. Immunopharmacol. 2012, 12, 453–459. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Wang, L.; Chen, B.; Zhuo, Q.; Bao, C.; Lin, L. Propofol inhibits NF-kappaB activation to ameliorate airway inflammation in ovalbumin (OVA)-induced allergic asthma mice. Int. Immunopharmacol. 2017, 51, 158–164. [Google Scholar] [CrossRef]
- Steinke, J.W.; Borish, L. Th2 cytokines and asthma. Interleukin-4: Its role in the pathogenesis of asthma, and targeting it for asthma treatment with interleukin-4 receptor antagonists. Respir. Res. 2001, 2, 66–70. [Google Scholar] [CrossRef]
- Wang, J.; Fu, Y.; Wei, Z.; He, X.; Shi, M.; Kou, J.; Zhou, E.; Liu, W.; Yang, Z.; Guo, C. Anti-asthmatic activity of osthole in an ovalbumin-induced asthma murine model. Respir. Physiol. Neurobiol. 2017, 239, 64–69. [Google Scholar] [CrossRef]
- Governa, P.; Manetti, F.; Miraldi, E.; Biagi, M. Effects of in vitro simulated digestion on the antioxidant activity of different Camellia sinensis (L.) Kuntze leaves extracts. Eur. Food Res. Technol. 2021, 248, 119–128. [Google Scholar] [CrossRef]
- Kusmita, L.; Puspitaningrum, I.; Limantara, L. Identification, isolation and antioxidant activity of pheophytin from green tea (Camellia sinensis (L.) Kuntze). Procedia Chem. 2015, 14, 232–238. [Google Scholar] [CrossRef]
- Ohishi, T.; Goto, S.; Monira, P.; Isemura, M.; Nakamura, Y. Anti-inflammatory Action of Green Tea. Antiinflamm. Antiallergy Agents Med. Chem. 2016, 15, 74–90. [Google Scholar] [CrossRef]
- Coimbra, S.; Castro, E.; Rocha-Pereira, P.; Rebelo, I.; Rocha, S.; Santos-Silva, A. The effect of green tea in oxidative stress. Clin. Nutr. 2006, 25, 790–796. [Google Scholar] [CrossRef]
- Chacko, S.M.; Thambi, P.T.; Kuttan, R.; Nishigaki, I. Beneficial effects of green tea: A literature review. Chin. Med. 2010, 5, 13. [Google Scholar] [CrossRef] [PubMed]
- Cabrera, C.; Artacho, R.; Giménez, R. Beneficial effects of green tea—A review. J. Am. Coll. Nutr. 2006, 25, 79–99. [Google Scholar] [CrossRef] [PubMed]
- Prasanth, M.I.; Sivamaruthi, B.S.; Chaiyasut, C.; Tencomnao, T. A Review of the Role of Green Tea (Camellia sinensis) in Antiphotoaging, Stress Resistance, Neuroprotection, and Autophagy. Nutrients 2019, 11, 474. [Google Scholar] [CrossRef] [PubMed]
- Shirai, T.; Reshad, K.; Yoshitomi, A.; Chida, K.; Nakamura, H.; Taniguchi, M. Green tea-induced asthma: Relationship between immunological reactivity, specific and non-specific bronchial responsiveness. Clin. Exp. Allergy 2003, 33, 1252–1255. [Google Scholar] [CrossRef]
- Shirai, T.; Sato, A.; Hara, Y. Epigallocatechin gallate. The major causative agent of green tea-induced asthma. Chest 1994, 106, 1801–1805. [Google Scholar] [CrossRef]
- Al-Mekhlafi, F.A.; Abutaha, N.; Al-Doaiss, A.A.; Al-Keridis, L.A.; Alsayadi, A.I.; Mohamed, R.; Wadaan, M.A.; Ibrahim, K.E.; Al-Khalifa, M.S. Corrigendum to “Target and Non-target effects of Foeniculum vulgare and Matricaria chamomilla combined extract on Culex pipiens mosquitoes”. Saudi J. Biol. Sci. 2022, 29, 3263. [Google Scholar]
- Balaji, G.; Chalamaiah, M.; Hanumanna, P.; Vamsikrishna, B.; Jagadeesh Kumar, D.; Venu babu, V. Mast cell stabilizing and anti-anaphylactic activity of aqueous extract of green tea (Camellia sinensis). Int. J. Vet. Sci. Med. 2014, 2, 89–94. [Google Scholar] [CrossRef]
- Li, Q.S.; Wang, Y.Q.; Liang, Y.R.; Lu, J.L. The anti-allergic potential of tea: A review of its components, mechanisms and risks. Food Funct. 2021, 12, 57–69. [Google Scholar] [CrossRef]
- Sharangi, A.B. Medicinal and therapeutic potentialities of tea (Camellia sinensis L.)—A review. Food Res. Int. 2009, 42, 529–535. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kang, S.; Kim, H.-Y.; Lee, A.Y.; Kim, H.S.; Park, J.H.; Moon, B.C.; Nam, H.H.; Chae, S.-W.; Jung, B.; Moon, C.; et al. Camellia sinensis (L.) Kuntze Extract Attenuates Ovalbumin-Induced Allergic Asthma by Regulating Airway Inflammation and Mucus Hypersecretion. Pharmaceutics 2023, 15, 2355. https://doi.org/10.3390/pharmaceutics15092355
Kang S, Kim H-Y, Lee AY, Kim HS, Park JH, Moon BC, Nam HH, Chae S-W, Jung B, Moon C, et al. Camellia sinensis (L.) Kuntze Extract Attenuates Ovalbumin-Induced Allergic Asthma by Regulating Airway Inflammation and Mucus Hypersecretion. Pharmaceutics. 2023; 15(9):2355. https://doi.org/10.3390/pharmaceutics15092355
Chicago/Turabian StyleKang, Sohi, Hyun-Yong Kim, A Yeong Lee, Hyo Seon Kim, Jun Hong Park, Byeong Cheol Moon, Hyeon Hwa Nam, Sung-Wook Chae, Bokyung Jung, Changjong Moon, and et al. 2023. "Camellia sinensis (L.) Kuntze Extract Attenuates Ovalbumin-Induced Allergic Asthma by Regulating Airway Inflammation and Mucus Hypersecretion" Pharmaceutics 15, no. 9: 2355. https://doi.org/10.3390/pharmaceutics15092355
APA StyleKang, S., Kim, H.-Y., Lee, A. Y., Kim, H. S., Park, J. H., Moon, B. C., Nam, H. H., Chae, S.-W., Jung, B., Moon, C., Shin, I. S., Kim, J. S., & Seo, Y.-S. (2023). Camellia sinensis (L.) Kuntze Extract Attenuates Ovalbumin-Induced Allergic Asthma by Regulating Airway Inflammation and Mucus Hypersecretion. Pharmaceutics, 15(9), 2355. https://doi.org/10.3390/pharmaceutics15092355