

Photochemical Internalization with Fimaporfin: Enhanced Bleomycin Treatment for Head and Neck Cancer


Abstract
1. Introduction
2. Materials and Methods
2.1. Cell Culture
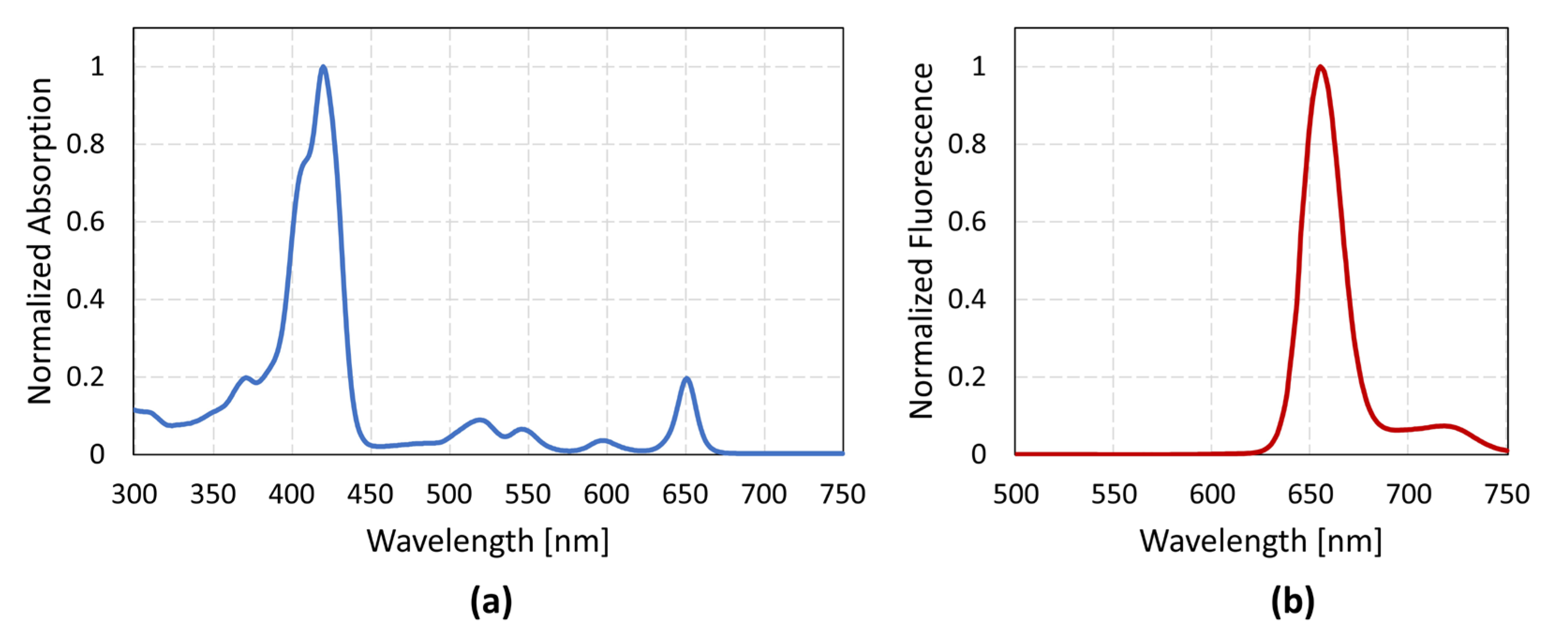
2.2. Photosensitizer and Drug
2.3. Cell Viability Assay—MTT
2.4. Cell Survival Assay—CFA
2.5. TuBB-9 Antibody and FITC Labeling
2.6. Cellular Uptake and Endosomal Release of the Antibody
3. Results
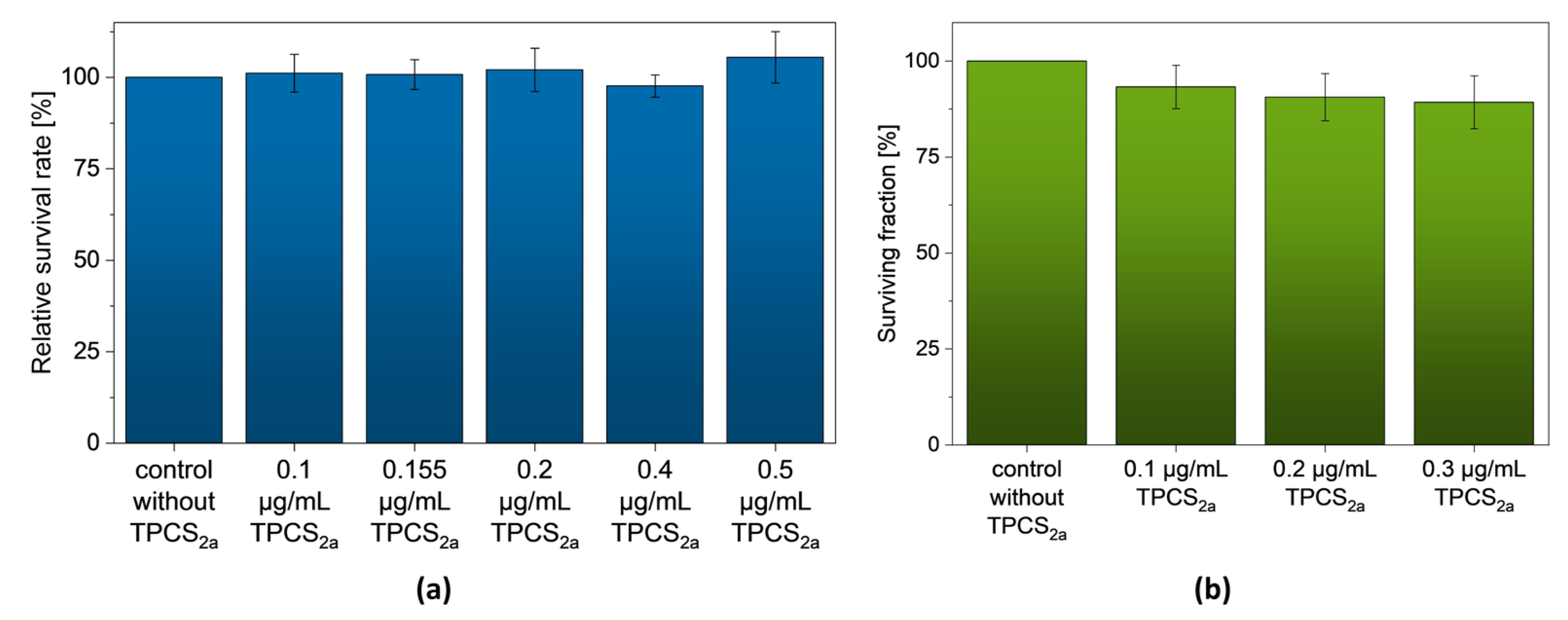
3.1. TPCS2a without Light Irradiation
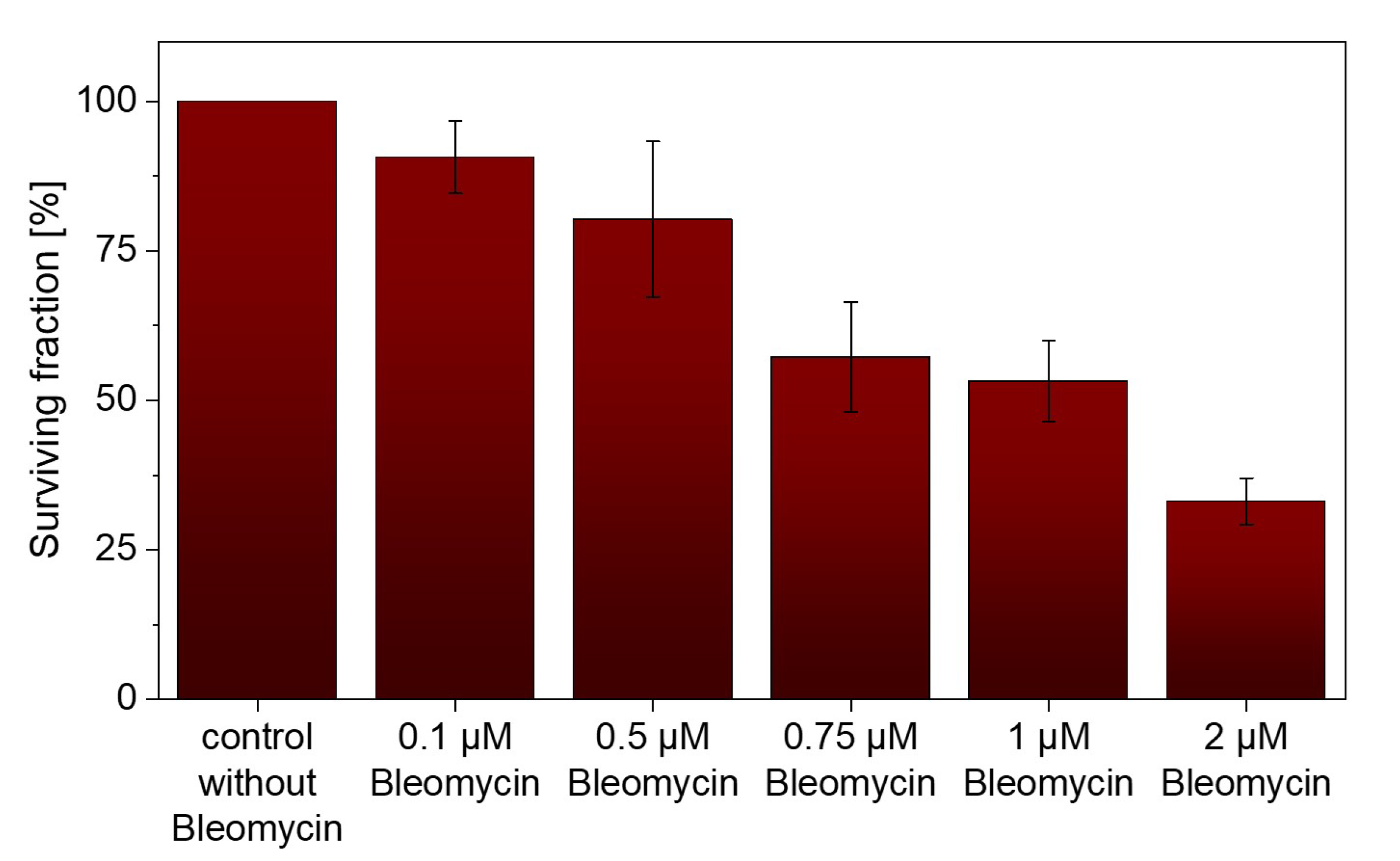
3.2. Bleomycin without Light Irradiation
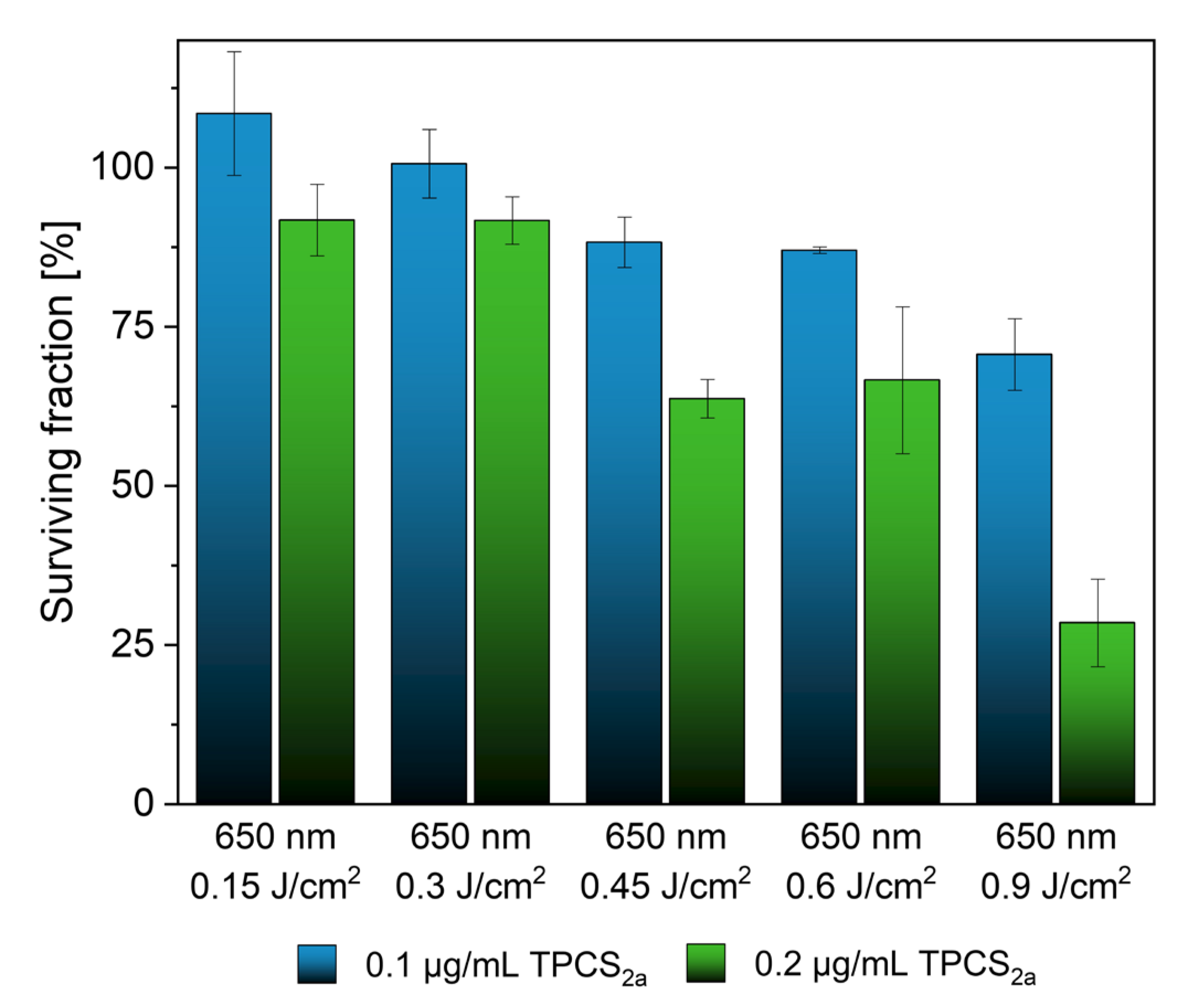
3.3. TPCS2a in Combination with Light Irradiation
3.4. Bleomycin with Irradiation
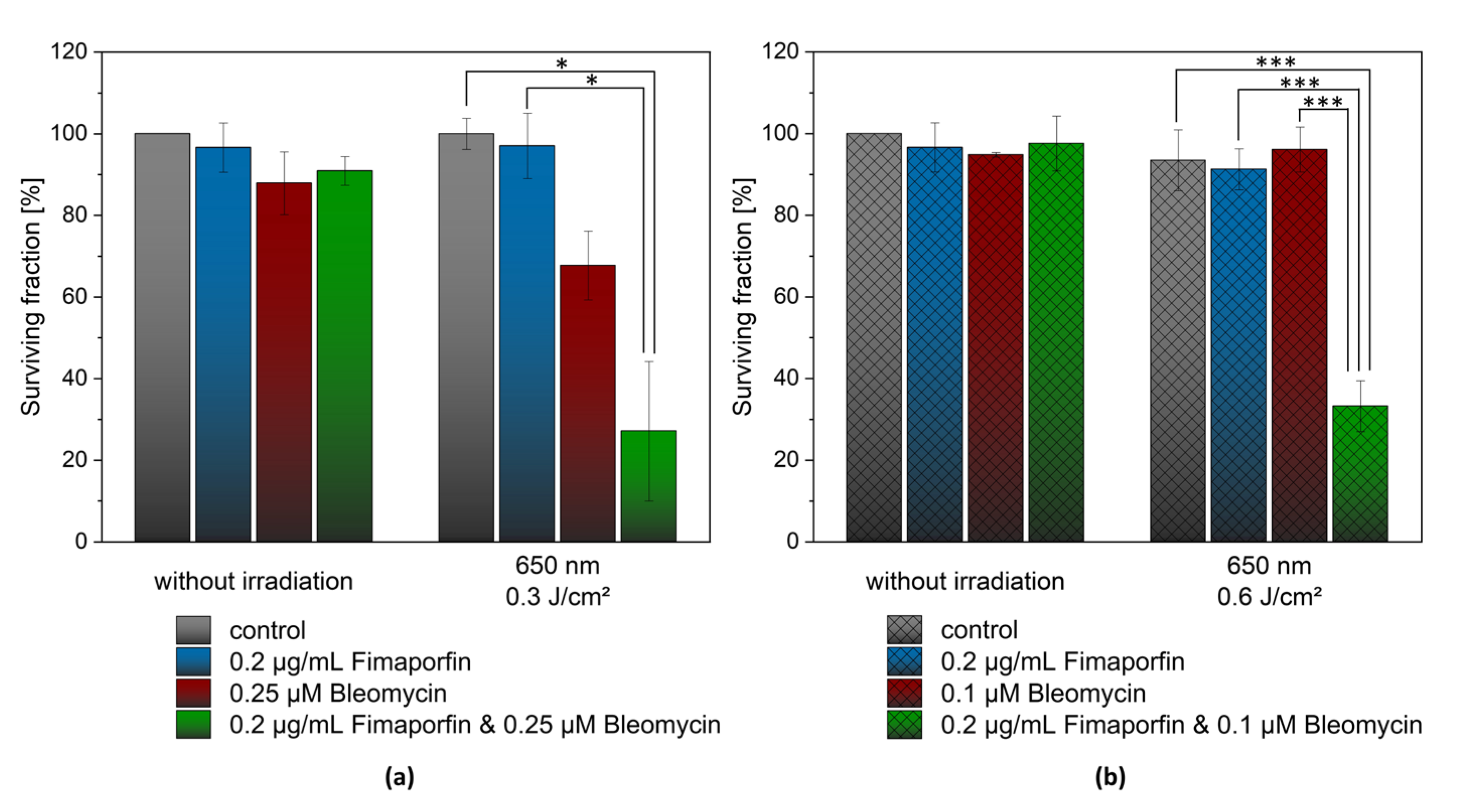
3.5. Combination of TPCS2a and Bleomycin with Light Irradiation
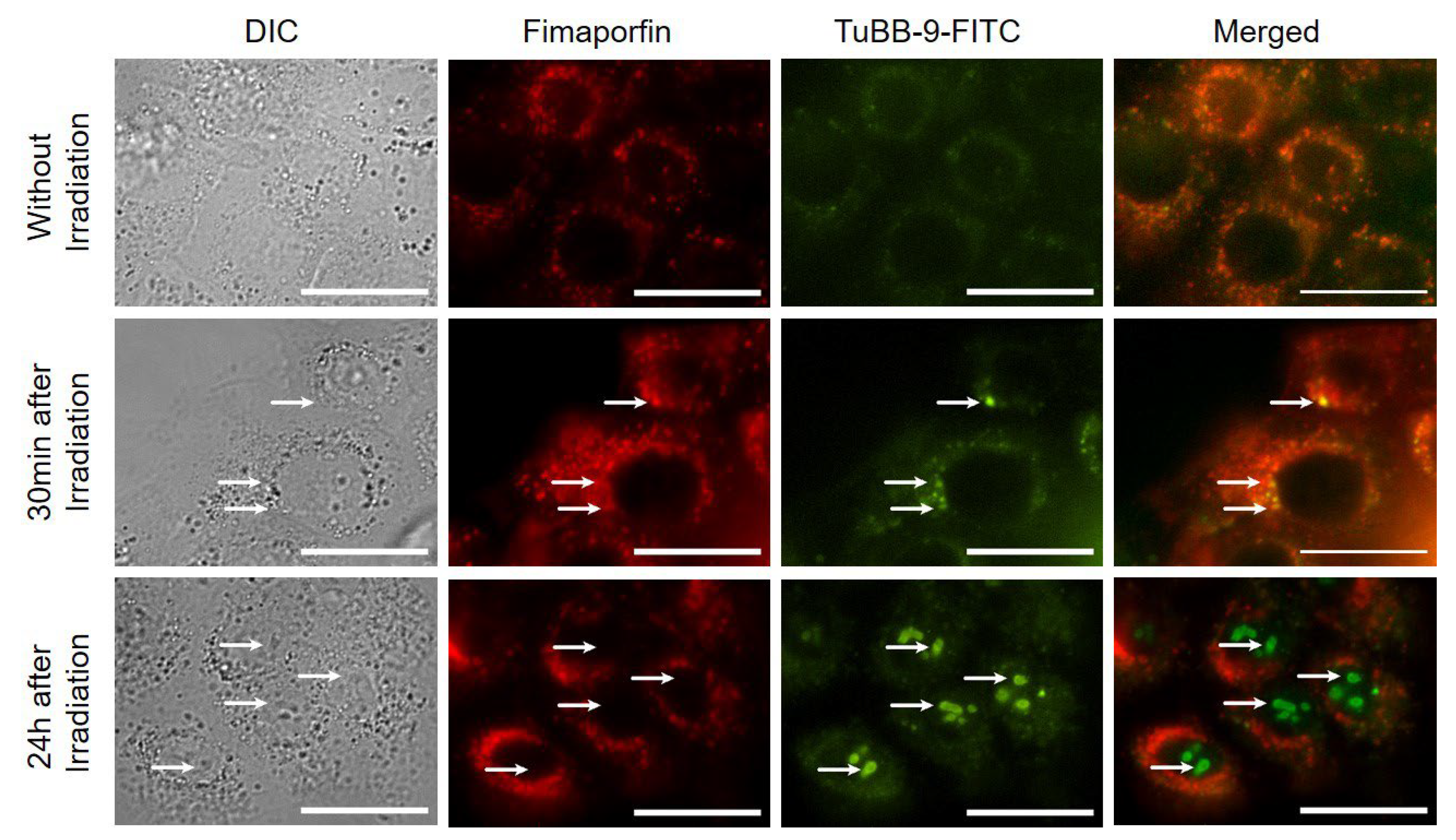
3.6. Microscopy of TPCS2a and TuBB-9-FITC after Irradiation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Méry, B.; Rancoule, C.; Guy, J.-B.; Espenel, S.; Wozny, A.-S.; Battiston-Montagne, P.; Ardail, D.; Beuve, M.; Alphonse, G.; Rodriguez-Lafrasse, C.; et al. Preclinical Models in HNSCC: A Comprehensive Review. Oral Oncol. 2017, 65, 51–56. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer Statistics, 2018. CA. Cancer J. Clin. 2018, 68, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Prince, M.E.P.; Ailles, L.E. Cancer Stem Cells in Head and Neck Squamous Cell Cancer. J. Clin. Oncol. 2008, 26, 2871–2875. [Google Scholar] [CrossRef] [PubMed]
- Chin, D.; Boyle, G.M.; Porceddu, S.; Theile, D.R.; Parsons, P.G.; Coman, W.B. Head and Neck Cancer: Past, Present and Future. Expert Rev. Anticancer Ther. 2006, 6, 1111–1118. [Google Scholar]
- Sharei, A.; Zoldan, J.; Adamo, A.; Sim, W.Y.; Cho, N.; Jackson, E.; Mao, S.; Schneider, S.; Han, M.-J.; Lytton-Jean, A.; et al. A Vector-Free Microfluidic Platform for Intracellular Delivery. Proc. Nat. Acad. Sci. USA 2013, 110, 2082–2087. [Google Scholar] [CrossRef]
- Erazo-Oliveras, A.; Muthukrishnan, N.; Baker, R.; Wang, T.-Y.; Pellois, J.-P.; Erazo-Oliveras, A.; Muthukrishnan, N.; Baker, R.; Wang, T.-Y.; Pellois, J.-P. Improving the Endosomal Escape of Cell-Penetrating Peptides and Their Cargos: Strategies and Challenges. Pharmaceuticals 2012, 5, 1177–1209. [Google Scholar] [CrossRef]
- Berg, K.; Høgset, A.; Prasmickaite, L.; Weyergang, A.; Bonsted, A.; Dietze, A.; Lou, P.J.; Bown, S.; Norum, O.J.; Møllergård, H.M.T.; et al. Photochemical Internalization (PCI): A Novel Technology for Activation of Endocytosed Therapeutic Agents. Med. Laser Appl. 2006, 21, 239–250. [Google Scholar] [CrossRef]
- Berg, K.; Weyergang, A.; Prasmickaite, L.; Bonsted, A.; Høgset, A.; Strand, M.T.R.; Wagner, E.; Selbo, P.K. Photochemical Internalization (PCI): A Technology for Drug Delivery. Methods Mol. Biol. 2010, 635, 133–145. [Google Scholar]
- Wang, S.; Hüttmann, G.; Zhang, Z.; Vogel, A.; Birngruber, R.; Tangutoori, S.; Hasan, T.; Rahmanzadeh, R. Light-Controlled Delivery of Monoclonal Antibodies for Targeted Photoinactivation of Ki-67. Mol. Pharm. 2015, 12, 3272–3281. [Google Scholar] [CrossRef]
- Wang, S.; Hüttmann, G.; Rudnitzki, F.; Diddens-Tschoeke, H.; Zhang, Z.; Rahmanzadeh, R. Indocyanine Green as Effective Antibody Conjugate for Intracellular Molecular Targeted Photodynamic Therapy. J. Biomed. Opt. 2016, 21, 078001. [Google Scholar] [CrossRef]
- Wang, S.; Hüttmann, G.; Scholzen, T.; Zhang, Z.; Vogel, A.; Hasan, T.; Rahmanzadeh, R. A Light-Controlled Switch after Dual Targeting of Proliferating Tumor Cells via the Membrane Receptor EGFR and the Nuclear Protein Ki-67. Sci. Rep. 2016, 6, 27032. [Google Scholar] [CrossRef]
- Enzian, P.; Schell, C.; Link, A.; Malich, C.; Pries, R.; Wollenberg, B.; Rahmanzadeh, R. Optically Controlled Drug Release from Light-Sensitive Liposomes with the New Photosensitizer 5,10-DiOH. Mol. Pharm. 2020, 17, 2779–2788. [Google Scholar] [CrossRef]
- Umezawa, H.; Maeda, K.; Takeuchi, T.; Okami, Y. New antibiotics, bleomycin A and B. J. Antibiot. 1966, 19, 200–209. [Google Scholar]
- Gederaas, O.A.; Sharma, A.; Mbarak, S.; Sporsheim, B.; Høgset, A.; Bogoeva, V.; Slupphaug, G.; Hagen, L. Proteomic analysis reveals mechanisms underlying increased efficacy of bleomycin by photochemical internalization in bladder cancer cells. Mol. Omics 2023. [Google Scholar] [CrossRef]
- Hendel, K.K.; Bagger, C.; Olesen, U.H.; Janfelt, C.; Hansen, S.H.; Haedersdal, M.; Lerche, C.M. Fractional laser-assisted topical delivery of bleomycin quantified by LC-MS and visualized by MALDI mass spectrometry imaging. Drug Deliv. 2019, 26, 244–251. [Google Scholar] [CrossRef]
- Du, L.; Sánchez, C.; Chen, M.; Edwards, D.J.; Shen, B. The biosynthetic gene cluster for the antitumor drug bleomycin from Streptomyces verticillus ATCC15003 supporting functional interactions between nonribosomal peptide synthetases and a polyketide synthase. Chem. Biol. 2000, 7, 623–642. [Google Scholar] [CrossRef]
- Soni, Y.; Sangwan, P.; Sharma, N.; Ahirwar, P.; Kamboj, S. Regulatory Status of Microbes as Antibiotics: An Overview. Glob. Acad. J. Pharm. Drug. Res. 2023, 5, 29–37. [Google Scholar] [CrossRef]
- Murray, V.; Chen, J.K.; Chung, L.H. The Interaction of the Metallo-Glycopeptide Anti-Tumour Drug Bleomycin with DNA. Int. J. Mol. Sci. 2018, 19, 1372. [Google Scholar] [CrossRef]
- Quada, J.C.; Zuber, G.F.; Hecht, S.M. Interaction of bleomycin with DNA. Pure Appl. Chem. 1998, 70, 307–311. [Google Scholar] [CrossRef][Green Version]
- Claussen, C.A.; Long, E.C. Nucleic Acid Recognition by Metal Complexes of Bleomycin. Chem. Rev. 1999, 99, 2797–2816. [Google Scholar] [CrossRef]
- Chen, J.; Stubbe, J. Bleomycins: Towards better therapeutics. Nat. Rev. Cancer. 2005, 5, 102–112. [Google Scholar] [CrossRef] [PubMed]
- Povirk, L.F. DNA damage and mutagenesis by radiomimetic DNA-cleaving agents: Bleomycin, neocarzinostatin and other ene-diynes. Mutat. Res. Fundam. Mol. Mech. Mutagen. 1996, 355, 71–89. [Google Scholar] [CrossRef]
- Berg, K.; Dietze, A.; Kaalhus, O.; Høgset, A. Site-Specific Drug Delivery by Photochemical Internalization Enhances the Antitumor Effect of Bleomycin. Clin. Cancer Res. 2005, 11, 8476–8485. [Google Scholar] [CrossRef] [PubMed]
- Norum, O.J.; Selbo, P.K.; Weyergang, A.; Giercksky, K.E.; Berg, K. Photochemical internalization (PCI) in cancer therapy: From bench towards bedside medicine. J. Photochem. Photobiol. B Biol. 2009, 96, 83–92. [Google Scholar] [CrossRef]
- Soe, T.H.; Watanabe, K.; Ohtsuki, T. Photoinduced endosomal escape mechanism: A view from photochemical internalization mediated by CPP-photosensitizer conjugates. Molecules 2021, 26, 36. [Google Scholar] [CrossRef] [PubMed]
- Berg, K.; Selbo, P.K.; Prasmickaite, L.; Tjelle, T.E.; Sandvig, K.; Moan, J.; Gaudernack, G.; Øystein, F.; Kjølsrud, S.; Anholt, H.; et al. Photochemical Internalization: A Novel Technology for Delivery of Macromolecules into Cytosol. Cancer Res. 1999, 59, 1180–1183. [Google Scholar]
- Selbo, P.K.; Weyergang, A.; Høgset, A.; Norum, O.J.; Berstad, M.B.; Vikdal, M.; Berg, K. Photochemical internalization provides time-and space-controlled endolysosomal escape of therapeutic molecules. J. Control. Release 2010, 148, 2–12. [Google Scholar] [CrossRef]
- Sultan, A.A.; Jerjes, W.; Berg, K.; Høgset, A.; Mosse, C.A.; Hamoudi, R.; Hamdoon, Z.; Simeon, C.; Carnell, D.; Forster, M.; et al. Disulfonated tetraphenyl chlorin (TPCS2a)-induced photochemical internalisation of bleomycin in patients with solid malignancies: A phase 1, dose-escalation, first-in-man trial. Lancet Oncol. 2016, 17, 1217–1229. [Google Scholar] [CrossRef]
- Baglo, Y.; Hagen, L.; Høgset, A.; Drabløs, F.; Otterlei, M.; Gederaas, O.A. Enhanced Efficacy of Bleomycin in Bladder Cancer Cells by Photochemical Internalization. BioMed Res. Int. 2014, 2014, 2314–6133. [Google Scholar] [CrossRef]
- Sellevold, S.; Peng, Q.; Fremstedal, A.S.V.; Berg, K. Photochemical internalization (PCI) of bleomycin is equally effective in two dissimilar leiomyosarcoma xenografts in athymic mice. Photodiagnosis Photodyn. Ther. 2017, 20, 95–106. [Google Scholar] [CrossRef]
- Norum, O.J.; Fremstedal, A.S.V.; Weyergang, A.; Golab, J.; Berg, K. Photochemical delivery of bleomycin induces T-cell activation of importance for curative effect and systemic anti-tumor immunity. J. Control. Release 2017, 268, 120–127. [Google Scholar] [CrossRef]
- Madsen, S.J.; Devarajan, A.G.; Chandekar, A.; Nguyen, L.; Hirschberg, H. Fibrin glue as a local drug and photosensitizer delivery system for photochemical internalization: Potential for bypassing the blood-brain barrier. Photodiagnosis Photodyn. Ther. 2023, 41, 103206. [Google Scholar] [CrossRef]
- Jerjes, W.; Hamdoon, Z.; Berg, K.; Høgset, A.; Hopper, C. Squamous cell carcinoma of the ear treated by photochemical internalization. Photodiagnosis Photodyn. Ther. 2021, 36, 102528. [Google Scholar] [CrossRef]
- Berg, K.; Nordstrand, S.; Selbo, P.K.; Tran, D.T.T.; Angell-Petersen, E.; Høgset, A. Disulfonated Tetraphenyl Chlorin (TPCS2a), a Novel Photosensitizer Developed for Clinical Utilization of Photochemical Internalization. Photochem. Photobiol. Sci. 2011, 10, 1637–1651. [Google Scholar] [CrossRef]
- Agostinis, P.; Berg, K.; Cengel, K.A.; Foster, T.H.; Girotti, A.W.; Gollnick, S.O.; Hahn, S.M.; Hamblin, M.R.; Juzeniene, A.; Kessel, D.; et al. Photodynamic Therapy of Cancer: An Update. CA. Cancer J. Clin. 2011, 61, 250–281. [Google Scholar] [CrossRef]
- Berg, K.; Moan, J. Lysosomes as photochemical targets. Int. J. Cancer 1994, 59, 814–822. [Google Scholar] [CrossRef]
- Franken, N.A.P.; Rodermond, H.M.; Stap, J.; Haveman, J.; van Bree, C. Clonogenic Assay of Cells in Vitro. Nat. Protoc. 2006, 1, 2315–2319. [Google Scholar] [CrossRef]
- Lund, K.; Bostad, M.; Skarpen, E.; Braunagel, M.; Kiprijanov, S.; Krauss, S.; Duncan, A.; Høgset, A.; Selbo, P.K. The novel EpCAM-targeting monoclonal antibody 3-17I linked to saporin is highly cytotoxic after photochemical internalization in breast, pancreas and colon cancer cell lines. MAbs 2014, 6, 1038–1050. [Google Scholar] [CrossRef]
- Mathews, M.S.; Blickenstaff, J.W.; Shih, E.-C.; Zamora, G.; Vo, V.; Sun, C.-H.; Hirschberg, H.; Madsen, S.J. Photochemical internalization of bleomycin for glioma treatment. J. Biomed. Opt. 2012, 17, 058001. [Google Scholar] [CrossRef]
- Shin, D.; Nguyen, L.; Le, M.T.; Ju, D.; Le, J.N.; Berg, K.; Hirschberg, H. The effects of low irradiance long duration photochemical internalization on glioma spheroids. Photodiagnosis Photodyn. Ther. 2019, 26, 442–447. [Google Scholar] [CrossRef]
- Petering, D.H.; Byrnes, R.W.M.; Antholine, W.E. The role of redox-active metals in the mechanism of action of bleomycin. Chem. Biol. Interact. 1990, 73, 133–182. [Google Scholar] [CrossRef] [PubMed]
- Pron, G.; Mahrour, N.; Orlowski, S.; Tounekti, O.; Poddevin, B.; Belehradek, J.; Mir, L.M. Internalisation of the bleomycin molecules responsible for bleomycin toxicity: A receptor-mediated endocytosis mechanism. Biochem. Pharmacol. 1999, 57, 45–56. [Google Scholar] [CrossRef] [PubMed]
- Nicolay, N.H.; Rühle, A.; Perez, R.L.; Trinh, T.; Sisombath, S.; Weber, K.J.; Ho, A.D.; Debus, J.; Saffrich, R.; Huber, P.E. Mesenchymal stem cells are sensitive to bleomycin treatment. Sci. Rep. 2016, 6, 26645. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, D.R.; Homanics, G.E.; Hoyt, D.G.; Klein, E.; Abernethy, J.; Lazo, J.S. The neutral cysteine protease bleomycin hydrolase is essential for epidermal integrity and bleomycin resistance. Proc. Natl. Acad. Sci. USA 1999, 96, 4680–4685. [Google Scholar] [CrossRef]
- O’Farrell, P.A.; Gonzalez, F.; Johnston, S.A.; Joshua-Tor, L. Crystal structure of human bleomycin hydrolase, a self-compartmentalizing cysteine protease. Structure 1999, 7, 619–627. [Google Scholar] [CrossRef]
- Akiyama, S.I.; Ikezaki, K.; Kuramochi, H.; Takahashi, K.; Kuwano, M. Bleomycin-resistant cells contain increased bleomycin-hydrolase activities. Biochem. Biophys. Res. Commun. 1981, 101, 55–60. [Google Scholar] [CrossRef]
- Crnovcic, I.; Gan, F.; Yang, D.; Dong, L.B.; Schultz, P.G.; Shen, B. Activities of recombinant human bleomycin hydrolase on bleomycins and engineered analogues revealing new opportunities to overcome bleomycin-induced pulmonary toxicity. Bioorganic Med. Chem. Lett. 2018, 28, 2670–2674. [Google Scholar] [CrossRef]
- Van Barneveld, P.W.C.; Van Der Mark, T.W.; Sleijfer, D.T.; Mulder, N.H.; Koops, H.S.; Sluiter, H.J.; Peset, R. Predictive factors for bleomycin-induced pneumonitis. Am. Rev. Respir. Dis. 1984, 130, 1078–1081. [Google Scholar]
- Wilson, M.S.; Wynn, T.A. Pulmonary fibrosis: Pathogenesis, etiology and regulation. Mucosal Immunol. 2009, 2, 103–121. [Google Scholar]
- Reinert, T.; Baldotto, C.S.D.R.; Nunes, F.A.P.; Scheliga, A.A.D.S. Bleomycin-induced lung injury. J. Cancer Res. 2013, 2013, 480608. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Treatment Group | Irradiation Parameters | Fimaporfin Concentration [µg/mL] | Bleomycin Concentration [µM] | ||
|---|---|---|---|---|---|
| Wavelength [nm] | Exposure Energy [J/cm2] | ||||
| Fimaporfin | A1 | no Irradiation | - | 0.1/0.155/0.2/0.3/ 0.4/0.5 | - |
| A2 | 650 nm | 0.15/0.3/0.45/0.6/0.9 | 0.1/0.2 | - | |
| Bleomycin | B1 | no Irradiation | - | - | 0.1/0.5/0.75/1/2 |
| B2 | 650 nm | 0.6/1.2/1.8 | - | 0.1/0.5/0.75/1 | |
| Combination | C1 | no Irradiation | - | 0.2 | 0.1/0.25 |
| C2 | 650 nm | 0.3/0.6 | 0.2 | 0.1/0.25 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Enzian, P.; Rahmanzadeh, R. Photochemical Internalization with Fimaporfin: Enhanced Bleomycin Treatment for Head and Neck Cancer. Pharmaceutics 2023, 15, 2040. https://doi.org/10.3390/pharmaceutics15082040
Enzian P, Rahmanzadeh R. Photochemical Internalization with Fimaporfin: Enhanced Bleomycin Treatment for Head and Neck Cancer. Pharmaceutics. 2023; 15(8):2040. https://doi.org/10.3390/pharmaceutics15082040
Chicago/Turabian StyleEnzian, Paula, and Ramtin Rahmanzadeh. 2023. "Photochemical Internalization with Fimaporfin: Enhanced Bleomycin Treatment for Head and Neck Cancer" Pharmaceutics 15, no. 8: 2040. https://doi.org/10.3390/pharmaceutics15082040
APA StyleEnzian, P., & Rahmanzadeh, R. (2023). Photochemical Internalization with Fimaporfin: Enhanced Bleomycin Treatment for Head and Neck Cancer. Pharmaceutics, 15(8), 2040. https://doi.org/10.3390/pharmaceutics15082040