

EHO-85, Novel Amorphous Antioxidant Hydrogel, Containing Olea europaea Leaf Extract—Rheological Properties, and Superiority over a Standard Hydrogel in Accelerating Early Wound Healing: A Randomized Controlled Trial

 , , , , and
, , , , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Rheological Study
Viscosity and Oscillatory Rheological Tests
2.2. Clinical Trial: Patients and Procedures
2.2.1. Design
2.2.2. Patient Inclusion and Exclusion Criteria
2.2.3. Product under Investigation, Comparator, and Treatment Description
2.2.4. Randomization and Stratification
2.2.5. Procedures
2.2.6. Effectiveness Assessment Criteria
2.2.7. Data Collection and Database and Statistical Analysis
3. Results
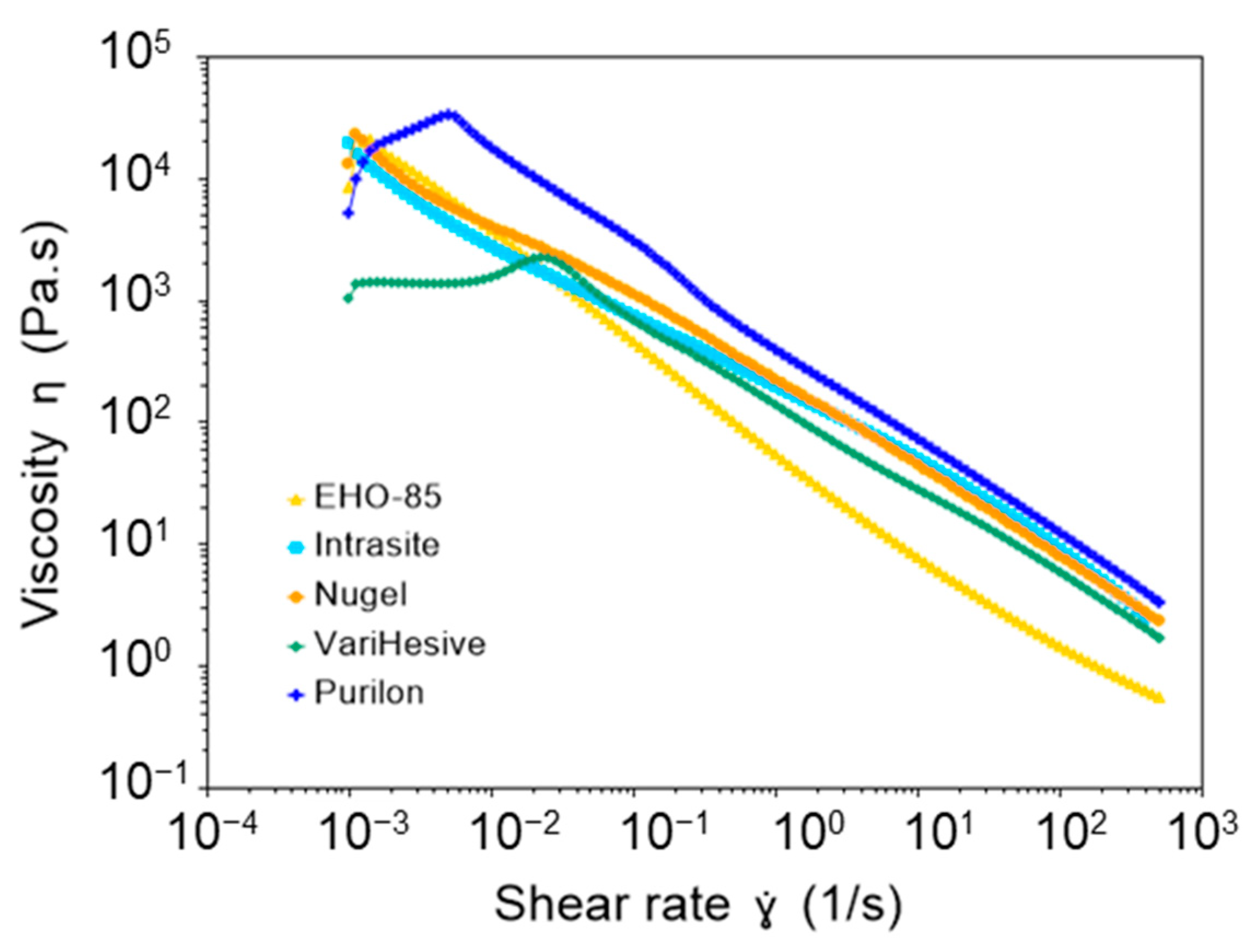
3.1. Viscosity and Oscillatory Rheological Tests
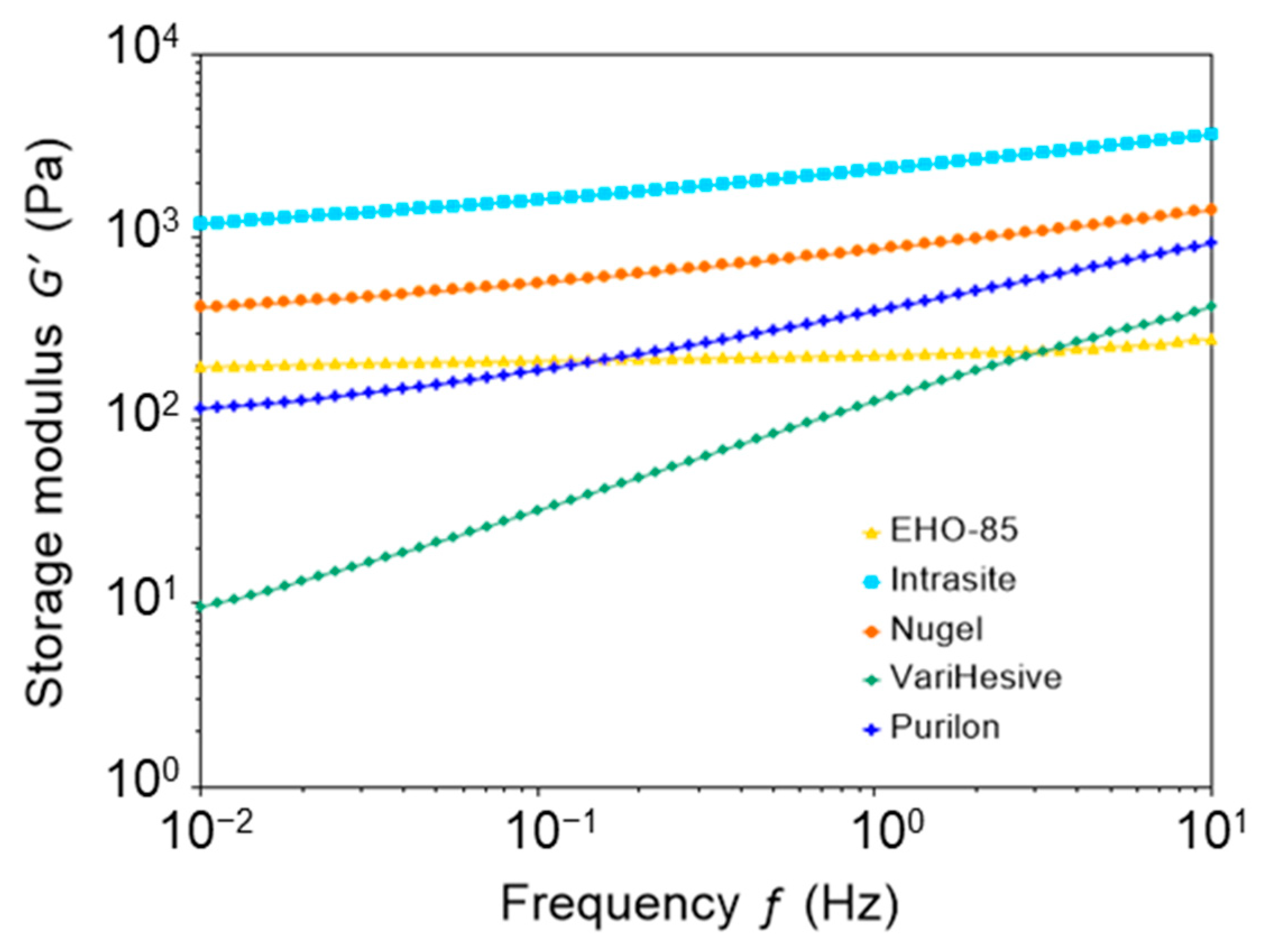
3.2. Viscoelastic Properties
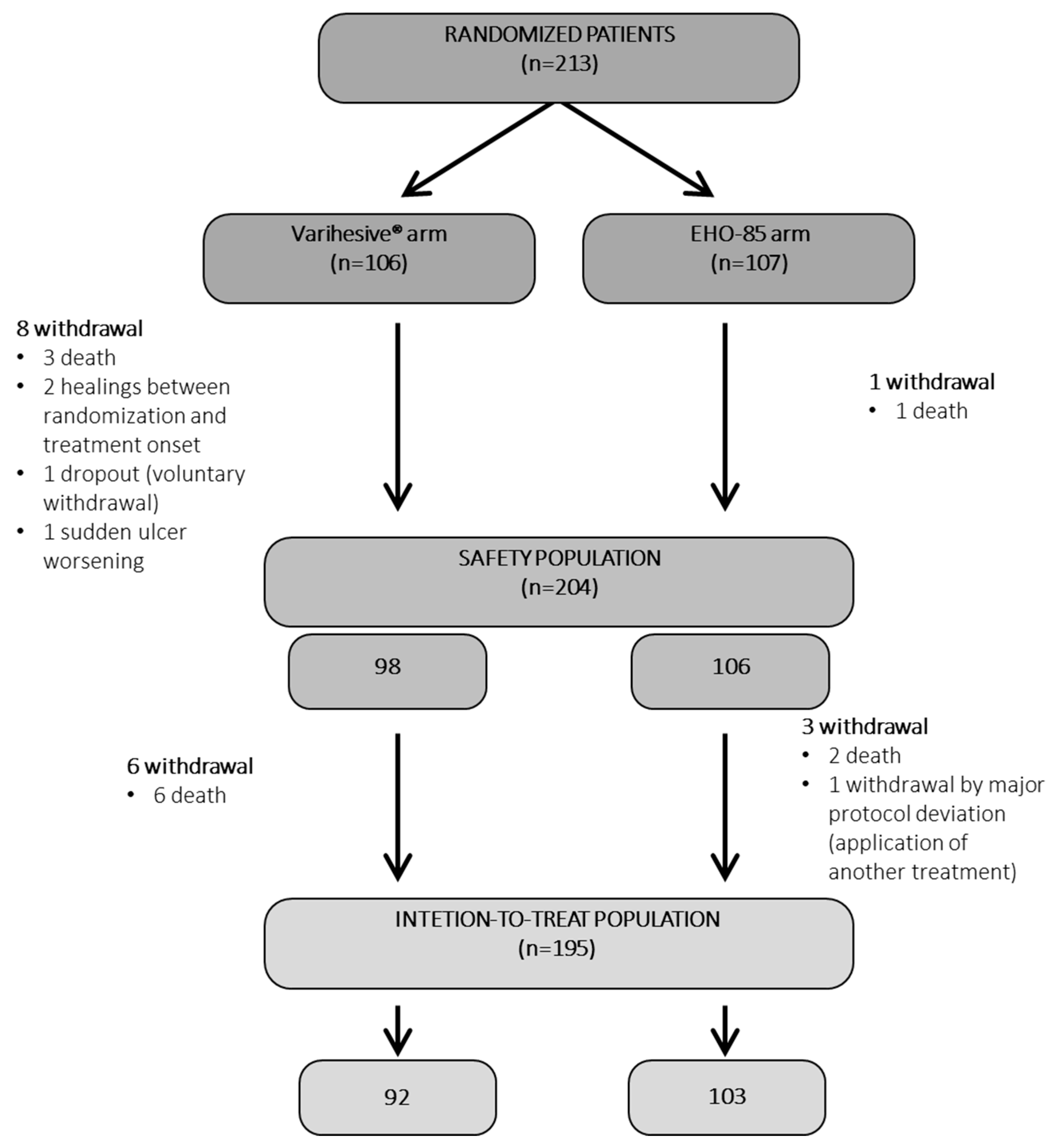
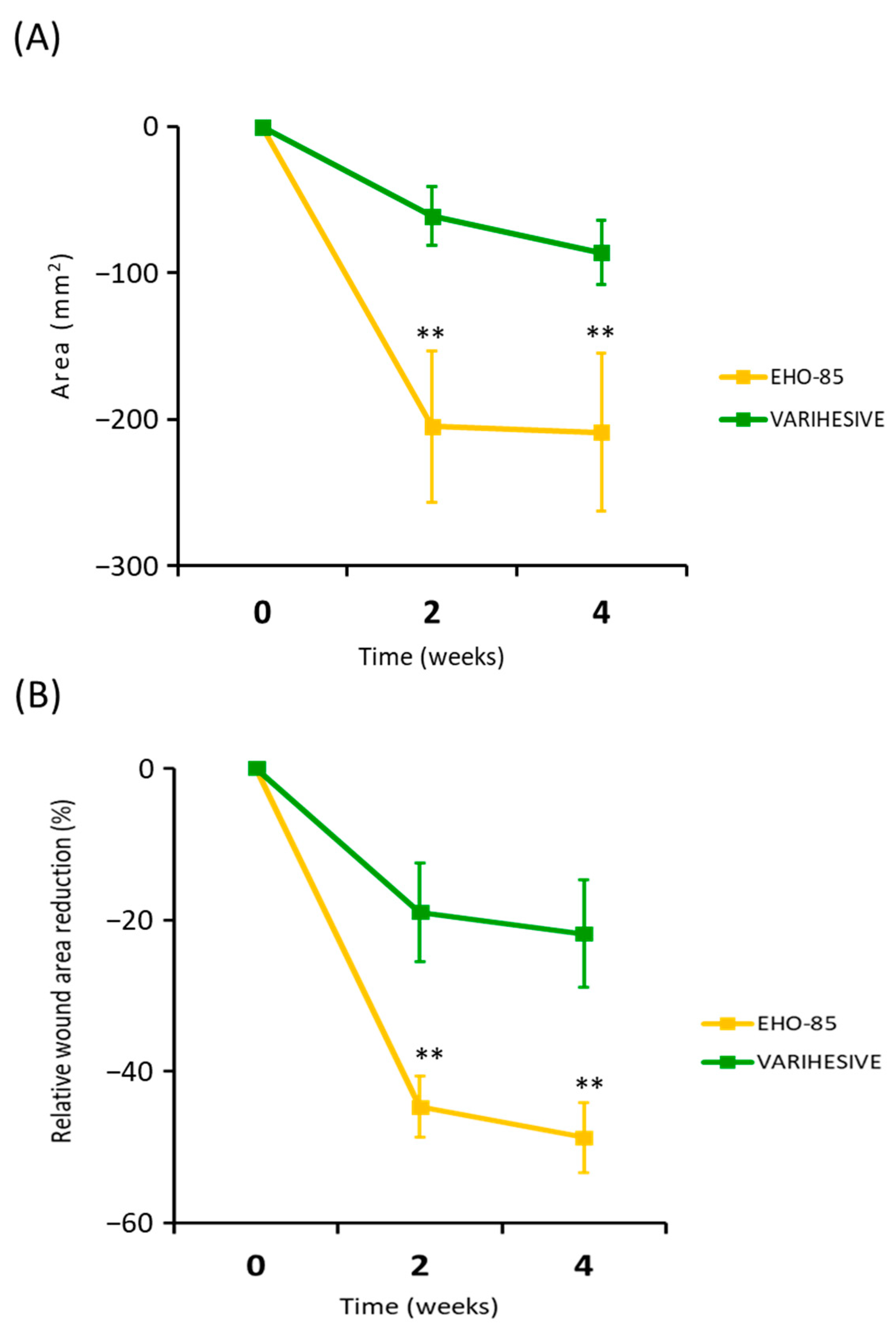
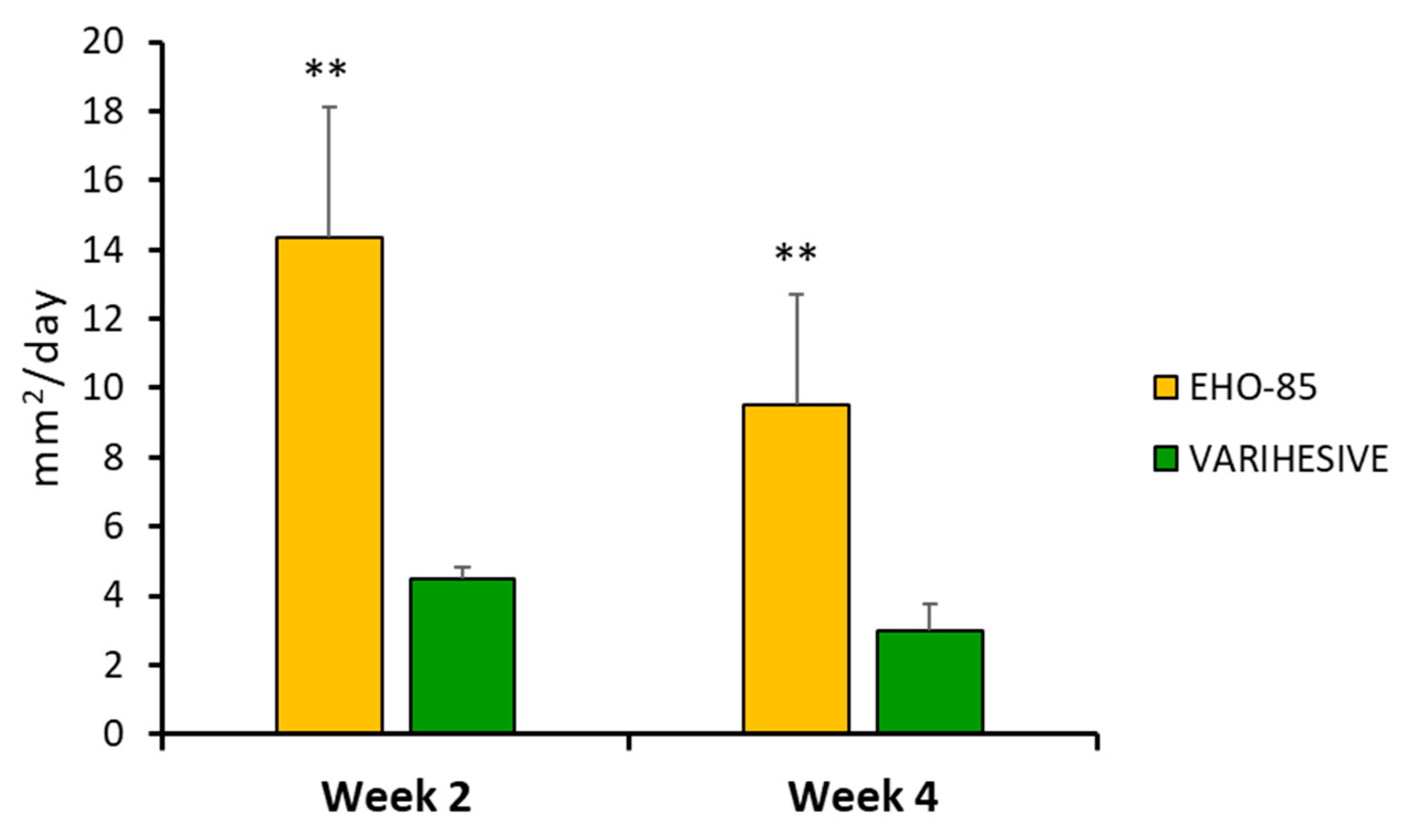
3.3. Clinical Trial Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gould, J. Superpowered skin. Nature 2018, 563, S84–S85. [Google Scholar] [CrossRef] [PubMed]
- Casado-Díaz, A.; Quesada-Gómez, J.M.; Dorado, G. Extracellular Vesicles Derived From Mesenchymal Stem Cells (MSC) in Regenerative Medicine: Applications in Skin Wound Healing. Front. Bioeng. Biotechnol. 2020, 8, 146. [Google Scholar] [CrossRef]
- Gantwerker, E.A.; Hom, D.B. Skin: Histology and physiology of wound healing. Facial Plast. Surg. Clin. N. Am. 2011, 19, 441–453. [Google Scholar] [CrossRef] [PubMed]
- Sen, C.; Roy, S.; Gordillo, G.M. Wound Healing. In Neligan Plastic Surgery: Volume One; Neligan, P., Ed.; Elsevier: Amsterdam, The Netherlands, 2017; ISBN 9780323356305. [Google Scholar]
- Gottrup, F. A specialized wound-healing center concept: Importance of a multidisciplinary department structure and surgical treatment facilities in the treatment of chronic wounds. Am. J. Surg. 2004, 187, S38–S43. [Google Scholar] [CrossRef] [PubMed]
- Sen, C.K. Human Wounds and Its Burden: An Updated Compendium of Estimates. Adv. Wound Care 2019, 8, 39–48. [Google Scholar] [CrossRef]
- Rani Raju, N.; Silina, E.; Stupin, V.; Manturova, N.; Chidambaram, S.B.; Achar, R.R. Multifunctional and Smart Wound Dressings—A Review on Recent Research Advancements in Skin Regenerative Medicine. Pharmaceutics 2022, 14, 1574. [Google Scholar] [CrossRef]
- Koehler, J.; Brandl, F.P.; Goepferich, A.M. Hydrogel wound dressings for bioactive treatment of acute and chronic wounds. Eur. Polym. J. 2018, 100, 1–11. [Google Scholar] [CrossRef]
- Bîrcă, A.C.; Chircov, C.; Niculescu, A.G.; Hildegard, H.; Baltă, C.; Roșu, M.; Mladin, B.; Gherasim, O.; Mihaiescu, D.E.; Vasile, B.Ș. H2O2-PLA-(Alg)2Ca Hydrogel Enriched in Matrigel® Promotes Diabetic Wound Healing. Pharmaceutics 2023, 15, 857. [Google Scholar] [CrossRef]
- Tavakoli, S.; Klar, A.S. Advanced Hydrogels as Wound Dressings. Biomolecules 2020, 10, 1169. [Google Scholar] [CrossRef]
- Fan, F.; Saha, S.; Hanjaya-Putra, D. Biomimetic Hydrogels to Promote Wound Healing. Front. Bioeng. Biotechnol. 2021, 9, 718377. [Google Scholar] [CrossRef]
- Casado-Díaz, A.; La Torre, M.; Priego-Capote, F.; Verdú-Soriano, J.; Lázaro-Martínez, J.L.; Rodríguez-Mañas, L.; Berenguer Pérez, M.; Tunez, I. EHO-85: A Multifunctional Amorphous Hydrogel for Wound Healing Containing Olea europaea Leaf Extract: Effects on Wound Microenvironment and Preclinical Evaluation. J. Clin. Med. 2022, 11, 1229. [Google Scholar] [CrossRef] [PubMed]
- Casado-Diaz, A.; Moreno-Rojas, J.M.; Verdú-Soriano, J.; Lázaro-Martínez, J.L.; Rodríguez-Mañas, L.; Tunez, I.; Torre, M.L.; Pérez, M.B.; Priego-Capote, F.; Pereira-Caro, G. Evaluation of Antioxidant and Wound-Healing Properties of EHO-85, a Novel Multifunctional Amorphous Hydrogel Containing Olea europaea Leaf Extract. Pharmaceutics 2022, 14, 349. [Google Scholar] [CrossRef]
- Verdú-soriano, J.; de Cristino-Espinar, M.; Luna-morales, S.; Dios-guerra, C.; Caballero-villarraso, J.; Moreno-moreno, P.; Casado-díaz, A.; Berenguer-pérez, M.; Guler-caamaño, I.; Laosa-zafra, O.; et al. Superiority of a Novel Multifunctional Amorphous Hydrogel Containing Olea europaea Leaf Extract (EHO-85) for the Treatment of Skin Ulcers: A Randomized, Active-Controlled Clinical Trial. J. Clin. Med. 2022, 11, 1260. [Google Scholar] [CrossRef]
- Ramsay, J.D.F.; Daish, S.R.; Wright, C.J. Structure and stability of concentrated boehmite sols. Faraday Discuss. Chem. Soc. 1978, 65, 65–75. [Google Scholar] [CrossRef]
- Tadros, T.F. Dispersion of Powders in Liquids and Stabilization of Suspensions; Wiley-VCH: Weinheim, Germany, 2012; ISBN 9783527329410. [Google Scholar]
- Panel, N.P.U.A.; Pacific, E.P.U.A.P.; Alliance, P.I. Prevention and Treatment of Pressure Ulcers: Quick Reference Guide, 2014th ed.; Haesler, E., Ed.; Cambridge Media: Osborne Park, Australia, 2014; ISBN 978-0-9579343-6-8. [Google Scholar]
- Wagner, F.W. The Dysvascular Foot: A System for Diagnosis and Treatment. Foot Ankle Int. 1981, 2, 64–122. [Google Scholar] [CrossRef]
- Islam, M.T.; Rodríguez-Hornedo, N.; Ciotti, S.; Ackermann, C. Rheological characterization of topical carbomer gels neutralized to different pH. Pharm. Res. 2004, 21, 1192–1199. [Google Scholar] [CrossRef]
- Anjum, A.; Sim, C.H.; Ng, S.F. Hydrogels Containing Antibiofilm and Antimicrobial Agents Beneficial for Biofilm-Associated Wound Infection: Formulation Characterizations and In vitro Study. AAPS PharmSciTech 2018, 19, 1219–1230. [Google Scholar] [CrossRef]
- Gregory, S.R. Physical Properties of Glycerine. In Glycerin: A Key Cosmetic Ingredient; Jungermann, E., Sonntag, N.O.V., Eds.; CRC Press: New York, NY, USA, 2018; Volume 1, pp. 113–156. ISBN 9780203753071. [Google Scholar]
- Péterszegi, G.; Isnard, N.; Robert, A.M.; Robert, L. Studies on skin aging. Preparation and properties of fucose-rich oligo- and polysaccharides. Effect on fibroblast proliferation and survival. Biomed. Pharmacother. 2003, 57, 187–194. [Google Scholar] [CrossRef]
- Margolis, D.J.; Berlin, J.A.; Strom, B.L. Which venous leg ulcers will heal with limb compression bandages? Am. J. Med. 2000, 109, 15–19. [Google Scholar] [CrossRef] [PubMed]
- Stacey, M.C.; Phillips, S.A.; Farrokhyar, F.; Swaine, J.M. Reliability and measurement error of digital planimetry for the measurement of chronic venous leg ulcers. Wound Repair Regen. 2017, 25, 901–905. [Google Scholar] [CrossRef] [PubMed]
- Mezger, T. The Rheology Handbook: For Users of Rotational and Oscillatory Rheometers; Vincentz Network: Hannover, Germany, 2020; ISBN 9783748603702. [Google Scholar]
- Jaworski, Z.; Spychaj, T.; Story, A.; Story, G. Carbomer microgels as model yield-stress fluids. Rev. Chem. Eng. 2022, 38, 881–919. [Google Scholar] [CrossRef]
- Kim, J.Y.; Song, J.Y.; Lee, E.J.; Park, S.K. Rheological properties and microstructures of Carbopol gel network system. Colloid Polym. Sci. 2003, 281, 614–623. [Google Scholar] [CrossRef]
- Nussbaum, S.R.; Carter, M.J.; Fife, C.E.; DaVanzo, J.; Haught, R.; Nusgart, M.; Cartwright, D. An Economic Evaluation of the Impact, Cost, and Medicare Policy Implications of Chronic Nonhealing Wounds. Value Health 2018, 21, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Kapp, S.; Miller, C.; Santamaria, N. The quality of life of people who have chronic wounds and who self-treat. J. Clin. Nurs. 2018, 27, 182–192. [Google Scholar] [CrossRef]
- Dumville, J.C.; Stubbs, N.; Keogh, S.J.; Walker, R.M.; Liu, Z. Hydrogel dressings for treating pressure ulcers. Cochrane Database Syst. Rev. 2015, 2015, CD011226. [Google Scholar] [CrossRef]
- Edmonds, M.; Lázaro-Martínez, J.L.; Alfayate-García, J.M.; Martini, J.; Petit, J.M.; Rayman, G.; Lobmann, R.; Uccioli, L.; Sauvadet, A.; Bohbot, S.; et al. Sucrose octasulfate dressing versus control dressing in patients with neuroischaemic diabetic foot ulcers (Explorer): An international, multicentre, double-blind, randomised, controlled trial. Lancet. Diabetes Endocrinol. 2018, 6, 186–196. [Google Scholar] [CrossRef]
- Meaume, S.; Truchetet, F.; Cambazard, F.; Lok, C.; Debure, C.; Dalac, S.; Lazareth, I.; Sigal, M.L.; Sauvadet, A.; Bohbot, S.; et al. A randomized, controlled, double-blind prospective trial with a Lipido-Colloid Technology-Nano-OligoSaccharide Factor wound dressing in the local management of venous leg ulcers. Wound Repair Regen. 2012, 20, 500–511. [Google Scholar] [CrossRef]
- Ribeiro, C.T.D.; Dias, F.A.L.; Fregonezi, G.A.F. Hydrogel dressings for venous leg ulcers. Cochrane Database Syst. Rev. 2022, 8, CD010738. [Google Scholar] [CrossRef] [PubMed]
- Wilson, I.A.; Henry, M.; Quill, R.; Byrne, P. The pH of varicose ulcer surfaces and its relationship to healing. Vasa 1979, 8, 339–342. [Google Scholar] [PubMed]
- Schneider, L.A.; Korber, A.; Grabbe, S.; Dissemond, J. Influence of pH on wound-healing: A new perspective for wound-therapy? Arch. Dermatol. Res. 2007, 298, 413–420. [Google Scholar] [CrossRef]
- Schäfer, M.; Werner, S. Oxidative stress in normal and impaired wound repair. Pharmacol. Res. 2008, 58, 165–171. [Google Scholar] [CrossRef]
- Xu, Z.; Han, S.; Gu, Z.; Wu, J. Advances and Impact of Antioxidant Hydrogel in Chronic Wound Healing. Adv. Healthc. Mater. 2020, 9, e1901502. [Google Scholar] [CrossRef]
- Johnson, J.B.; Broszczak, D.A.; Mani, J.S.; Anesi, J.; Naiker, M. A cut above the rest: Oxidative stress in chronic wounds and the potential role of polyphenols as therapeutics. J. Pharm. Pharmacol. 2021, 3, 38. [Google Scholar] [CrossRef]
- Boateng, J.; Catanzano, O. Advanced Therapeutic Dressings for Effective Wound Healing—A Review. J. Pharm. Sci. 2015, 104, 3653–3680. [Google Scholar] [CrossRef]
- Junker, J.P.E.; Kamel, R.A.; Caterson, E.J.; Eriksson, E. Clinical Impact Upon Wound Healing and Inflammation in Moist, Wet, and Dry Environments. Adv. Wound Care 2013, 2, 348–356. [Google Scholar] [CrossRef]
- Brumberg, V.; Astrelina, T.; Malivanova, T.; Samoilov, A. Modern Wound Dressings: Hydrogel Dressings. Biomedicines 2021, 9, 1235. [Google Scholar] [CrossRef]
- Opt Veld, R.C.; Walboomers, X.F.; Jansen, J.A.; Wagener, F.A.D.T.G. Design Considerations for Hydrogel Wound Dressings: Strategic and Molecular Advances. Tissue Eng.-Part B Rev. 2020, 26, 230–248. [Google Scholar] [CrossRef] [PubMed]
- Nagoba, B.S.; Suryawanshi, N.M.; Wadher, B.; Selkar, S. Acidic environment and wound healing: A review. Wounds 2015, 27, 5–11. [Google Scholar]
- Thomas, L.V.; Wimpenny, J.W.T.; Davis, J.G. Effect of three preservatives on the growth of Bacillus cereus, Vero cytotoxigenic Escherichia coli and Staphylococcus aureus, on plates with gradients of pH and sodium chloride concentration. Int. J. Food Microbiol. 1993, 17, 289–301. [Google Scholar] [CrossRef] [PubMed]
- Runeman, B.; Faergemann, J.; Larkö, O. Experimental Candida albicans lesions in healthy humans: Dependence on skin pH. Acta Derm. Venereol. 2000, 80, 421–424. [Google Scholar] [CrossRef]
- Sim, P.; Song, Y.; Yang, G.N.; Cowin, A.J.; Garg, S. In Vitro Wound Healing Properties of Novel Acidic Treatment Regimen in Enhancing Metabolic Activity and Migration of Skin Cells. Int. J. Mol. Sci. 2022, 23, 7188. [Google Scholar] [CrossRef]
- Leveen, H.H.; Falk, G.; Borek, B.; Diaz, C.; Lynfield, Y.; Wynkoop, B.J.; Mabunda, G.A.; Rubricius, J.L.; Christoudias, G.C. Chemical acidification of wounds. An adjuvant to healing and the unfavorable action of alkalinity and ammonia. Ann. Surg. 1973, 178, 745–753. [Google Scholar] [CrossRef]
- Sim, P.; Strudwick, X.L.; Song, Y.M.; Cowin, A.J.; Garg, S. Influence of Acidic pH on Wound Healing In Vivo: A Novel Perspective for Wound Treatment. Int. J. Mol. Sci. 2022, 23, 13655. [Google Scholar] [CrossRef]
- Honnegowda, T.M.; Kumar, P.; Padmanabha Udupa, E.G.; Sharan, A.; Singh, R.; Prasad, H.; Rao, P. Effects of limited access dressing in chronic wounds: A biochemical and histological study. Indian J. Plast. Surg. 2015, 48, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Tsukada, K. The pH changes of pressure ulcers related headling process of wound. Wounds 1992, 4, 16–20. [Google Scholar]
- Dunnill, C.; Patton, T.; Brennan, J.; Barrett, J.; Dryden, M.; Cooke, J.; Leaper, D.; Georgopoulos, N.T. Reactive oxygen species (ROS) and wound healing: The functional role of ROS and emerging ROS-modulating technologies for augmentation of the healing process. Int. Wound J. 2017, 14, 89–96. [Google Scholar] [CrossRef] [PubMed]
- Kontogianni, V.G.; Gerothanassis, I.P. Phenolic compounds and antioxidant activity of olive leaf extracts. Nat. Prod. Res. 2012, 26, 186–189. [Google Scholar] [CrossRef]
- Lee, O.H.; Lee, B.Y. Antioxidant and antimicrobial activities of individual and combined phenolics in Olea europaea leaf extract. Bioresour. Technol. 2010, 101, 3751–3754. [Google Scholar] [CrossRef] [PubMed]
- Mehraein, F.; Sarbishegi, M.; Aslani, A. Evaluation of effect of oleuropein on skin wound healing in aged male BALB/c mice. Cell J. 2014, 16, 25–30. [Google Scholar]
- Mehraein, F.; Sarbishegi, M.; Aslani, A. Therapeutic effects of oleuropein on wounded skin in young male Balb/c mice. Wounds 2014, 26, 83–88. [Google Scholar]
- Al-Basher, G.; Al-Otibi, F. Biological activity of olive leaf extract and regulation of tissue transglutaminase expression in diabetic wound healing. Int. J. Pharmacol. 2018, 14, 963–972. [Google Scholar] [CrossRef]
- Atkins, D.; Fink, K.; Slutsky, J. Better information for better health care: The Evidence-based Practice Center program and the Agency for Healthcare Research and Quality. Ann. Intern. Med. 2005, 142, 1035–1041. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Shear Rate (s−1) | |||||
|---|---|---|---|---|---|
| Sample | 0.01 | 0.1 | 1 | 10 | 100 |
| EHO-85 | 3512 ± 449 | 428.7 ± 46.3 | 51.6 ± 4.2 | 7.5 ± 0.4 | 1.4 ± 0.1 |
| Intrasite | 2702 ± 125 | 754.4 ± 13.7 | 209.6 ± 15.9 | 50.8 ± 1.4 | 9.1 ± 0.1 |
| Nu-gel | 3877 ± 287 | 1063 ± 89.7 | 216.5 ± 12.4 | 43.6 ± 1.4 | 7.8 ± 0.2 |
| VariHesive | 1393 ± 213 | 634.9 ± 73.6 | 130.0 ± 13.3 | 26.8 ± 1.8 | 5.8 ± 0.2 |
| Purilon | 16,158 ± 1811 | 2901 ± 102 | 360.2 ± 13.5 | 67.8 ± 2.5 | 11.6 ± 0.3 |
| Sample | Elastic Modulus (G′) (Pa) | Cohesive Energy (Ec) (J/m3) |
|---|---|---|
| EHO-85 | 227.1 ± 1.5 | 0.067 ± 0.001 |
| Intrasite | 2402 ± 64 | 0.023 ± 0.012 |
| Nu-gel | 867.0 ± 9.8 | 1.12 ± 0.02 |
| VariHesive | 121.5 ± 8.6 | 12.3 ± 1.5 |
| Purilon | 399.9 ± 4.1 | 9.73 ± 1.18 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Verdú-Soriano, J.; de Cristino-Espinar, M.; Luna-Morales, S.; Dios-Guerra, C.; Casado-Díaz, A.; Quesada-Gómez, J.M.; Dorado, G.; Berenguer-Pérez, M.; Vílchez, S.; Esquena, J.; et al. EHO-85, Novel Amorphous Antioxidant Hydrogel, Containing Olea europaea Leaf Extract—Rheological Properties, and Superiority over a Standard Hydrogel in Accelerating Early Wound Healing: A Randomized Controlled Trial. Pharmaceutics 2023, 15, 1925. https://doi.org/10.3390/pharmaceutics15071925
Verdú-Soriano J, de Cristino-Espinar M, Luna-Morales S, Dios-Guerra C, Casado-Díaz A, Quesada-Gómez JM, Dorado G, Berenguer-Pérez M, Vílchez S, Esquena J, et al. EHO-85, Novel Amorphous Antioxidant Hydrogel, Containing Olea europaea Leaf Extract—Rheological Properties, and Superiority over a Standard Hydrogel in Accelerating Early Wound Healing: A Randomized Controlled Trial. Pharmaceutics. 2023; 15(7):1925. https://doi.org/10.3390/pharmaceutics15071925
Chicago/Turabian StyleVerdú-Soriano, José, Marisol de Cristino-Espinar, Silvia Luna-Morales, Caridad Dios-Guerra, Antonio Casado-Díaz, José Manuel Quesada-Gómez, Gabriel Dorado, Miriam Berenguer-Pérez, Susana Vílchez, Jordi Esquena, and et al. 2023. "EHO-85, Novel Amorphous Antioxidant Hydrogel, Containing Olea europaea Leaf Extract—Rheological Properties, and Superiority over a Standard Hydrogel in Accelerating Early Wound Healing: A Randomized Controlled Trial" Pharmaceutics 15, no. 7: 1925. https://doi.org/10.3390/pharmaceutics15071925
APA StyleVerdú-Soriano, J., de Cristino-Espinar, M., Luna-Morales, S., Dios-Guerra, C., Casado-Díaz, A., Quesada-Gómez, J. M., Dorado, G., Berenguer-Pérez, M., Vílchez, S., Esquena, J., Rodríguez-Mañas, L., & Lázaro-Martínez, J. L. (2023). EHO-85, Novel Amorphous Antioxidant Hydrogel, Containing Olea europaea Leaf Extract—Rheological Properties, and Superiority over a Standard Hydrogel in Accelerating Early Wound Healing: A Randomized Controlled Trial. Pharmaceutics, 15(7), 1925. https://doi.org/10.3390/pharmaceutics15071925