

Aspects of Nanotechnology for COVID-19 Vaccine Development and Its Delivery Applications

 , ,
, , 
 , ,
, ,  and
and 
Abstract
1. Introduction
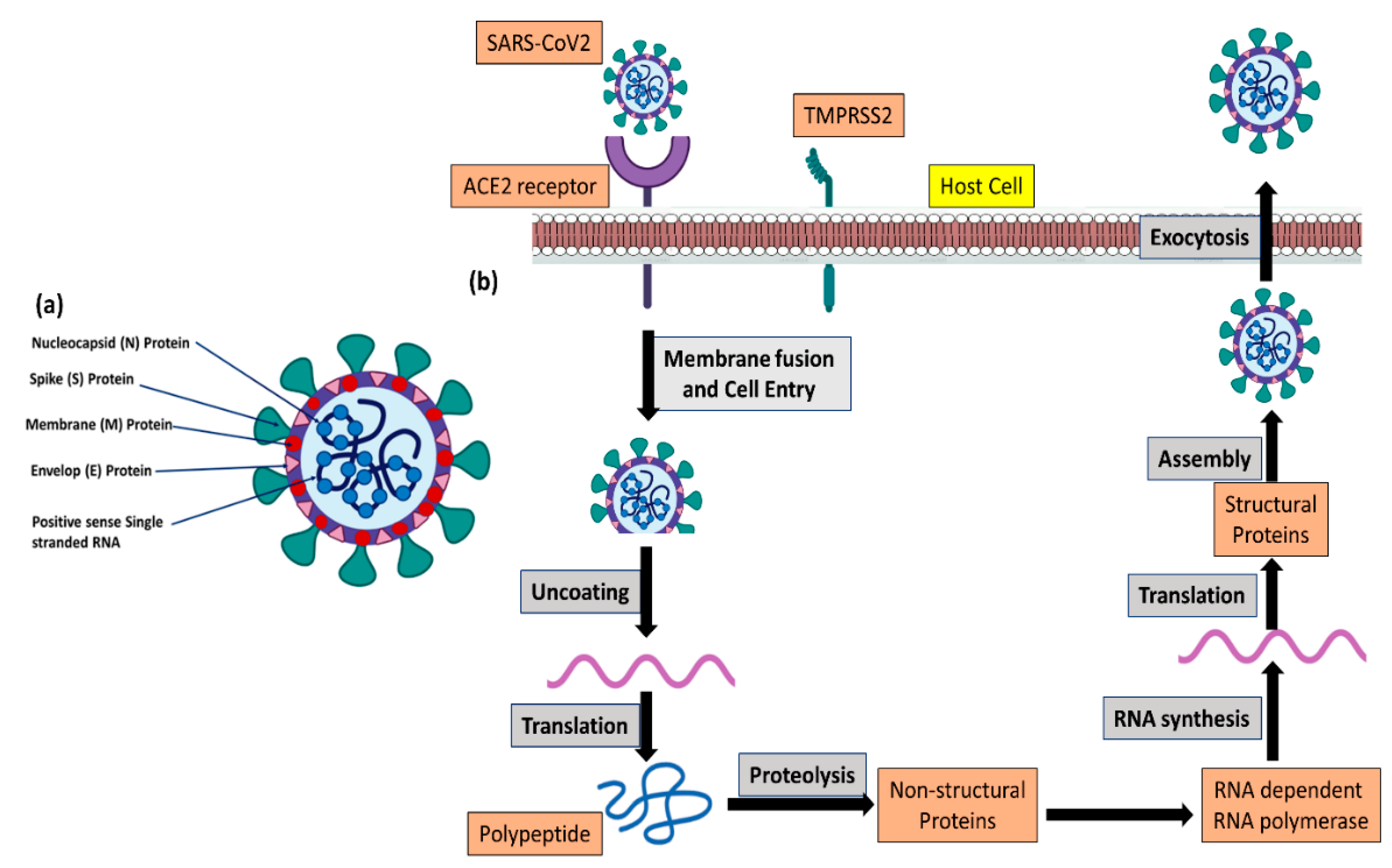
2. Pathophysiology of COVID-19
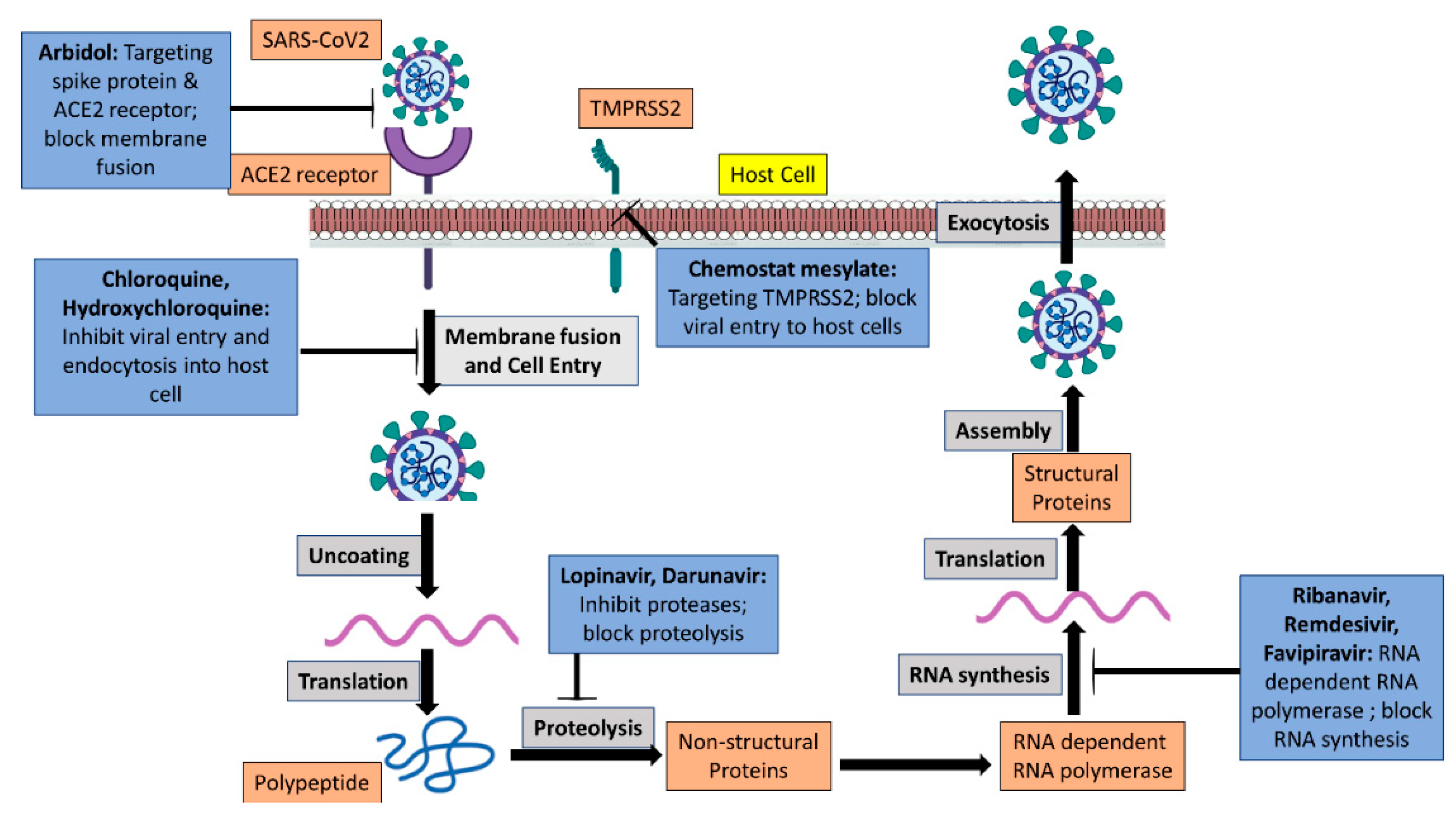
3. Therapeutic Strategies
3.1. Antiviral Drug Molecules
3.2. The S Protein and ACE2 Interaction Inhibitors
3.3. Neutralizing Antibodies
3.4. Immunotherapy
3.5. Convalescent Plasma Therapy
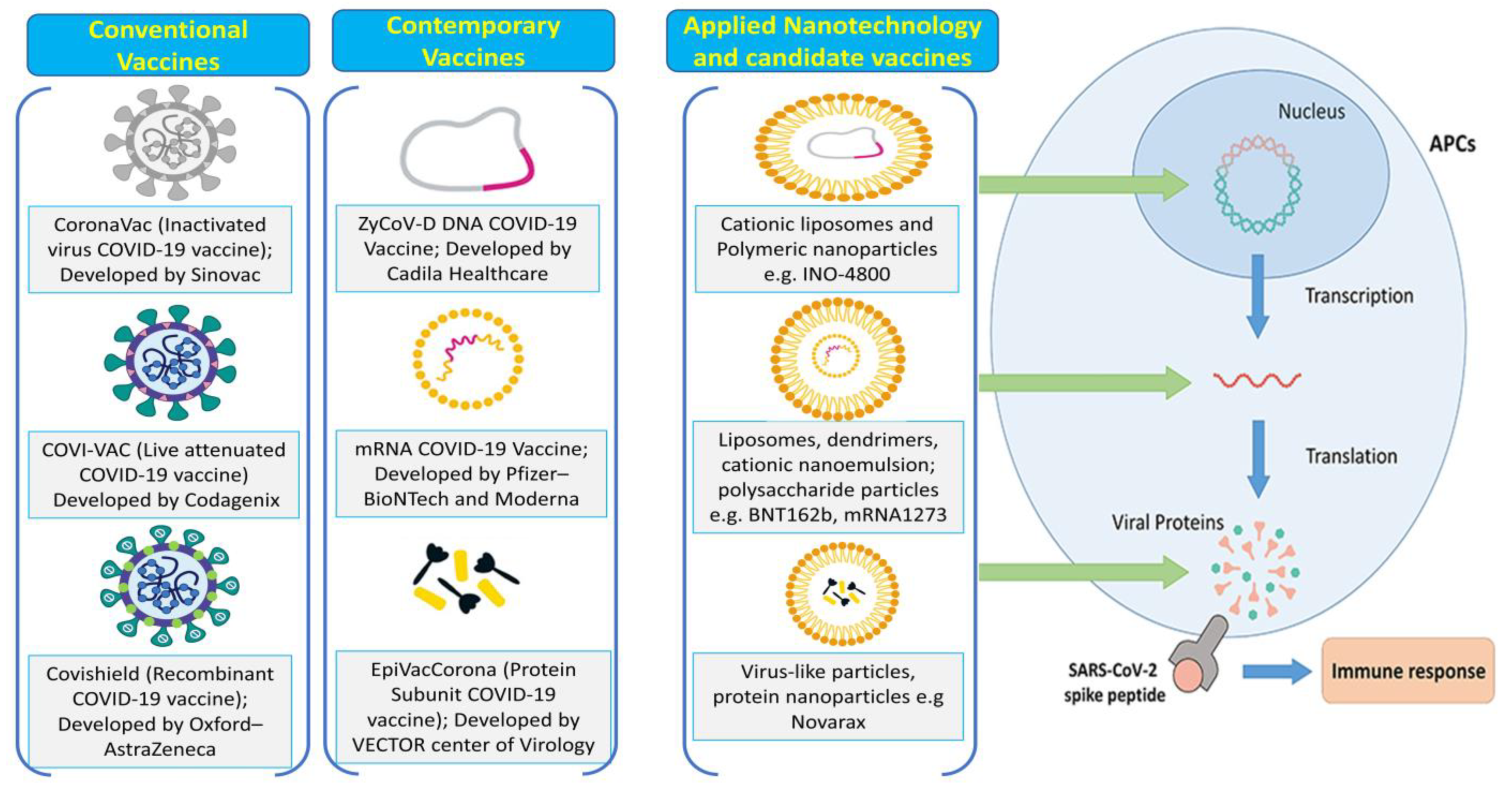
3.6. Preventive Vaccination Strategies
3.7. Inactivated or Live-Attenuated Vaccines
3.8. Recombinant Vaccines
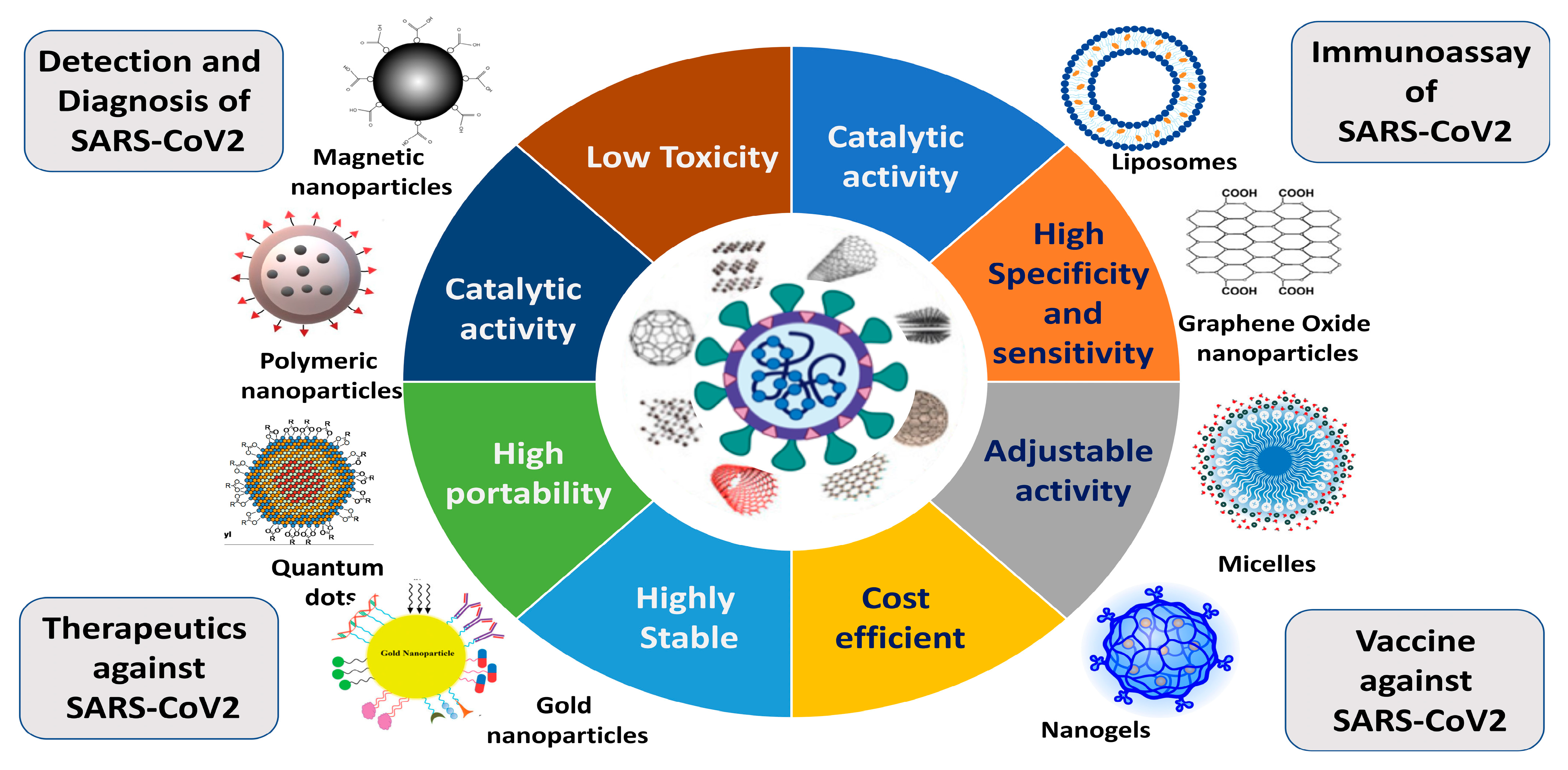
4. Application of Nanotechnology in COVID-19 Therapeutics
4.1. Theragnostic Nanoparticles
4.2. Intranasal Delivery Therapy
4.3. Organic Nanoparticle-Based Treatment Strategy
4.4. Inorganic Nanoparticle-Based Treatment Strategy
4.5. Virus-like Nanoparticle-Based Treatment Strategy
4.6. Pulmonary Delivery Using NP Inhalation Aerosols
5. Nanotechnology-Based SARS-CoV-2 Vaccine Development
5.1. Subunit Vaccines
5.2. Nucleic Acid Vaccines
5.3. Nanoparticle-Based Vaccines
6. Deactivation of Coronavirus Outside Host Cell with the Use of Nanotechnology
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Prabhakar, P.K.; Lakhanpal, J. Recent Advances in the Nucleic Acid-Based Diagnostic Tool for Coronavirus. Mol. Biol. Rep. 2020, 47, 9033–9041. [Google Scholar] [CrossRef]
- Su, S.; Wong, G.; Shi, W.; Liu, J.; Lai, A.C.K.; Zhou, J.; Liu, W.; Bi, Y.; Gao, G.F. Epidemiology, Genetic Recombination, and Pathogenesis of Coronaviruses. Trends Microbiol. 2016, 24, 490–502. [Google Scholar] [CrossRef]
- Bhattacharjee, R.; Dubey, A.K.; Ganguly, A.; Bhattacharya, B.; Mishra, Y.K.; Mostafavi, E.; Kaushik, A. State-of-Art High-Performance Nano-Systems for Mutated Coronavirus Infection Management: From Lab to Clinic. OpenNano 2022, 8, 100078. [Google Scholar] [CrossRef]
- Pooja Varahachalam, S.; Lahooti, B.; Chamaneh, M.; Bagchi, S.; Chhibber, T.; Morris, K.; Bolanos, J.F.; Kim, N.-Y.; Kaushik, A.; de Ciencias De La Salud, F.; et al. Nanomedicine for the SARS-CoV-2: State-of-the-Art and Future Prospects. Int. J. Nanomed. 2021, 16, 539–560. [Google Scholar] [CrossRef] [PubMed]
- Perlman, S.; Netland, J. Coronaviruses Post-SARS: Update on Replication and Pathogenesis. Nat. Rev. Microbiol. 2009, 7, 439–450. [Google Scholar] [CrossRef] [PubMed]
- Huang, P.; Wang, H.; Cao, Z.; Jin, H.; Chi, H.; Zhao, J.; Yu, B.; Yan, F.; Hu, X.; Wu, F.; et al. A Rapid and Specific Assay for the Detection of MERS-CoV. Front. Microbiol. 2018, 9, 1101. [Google Scholar] [CrossRef]
- Sun, J.; He, W.T.; Wang, L.; Lai, A.; Ji, X.; Zhai, X.; Li, G.; Suchard, M.A.; Tian, J.; Zhou, J.; et al. COVID-19: Epidemiology, Evolution, and Cross-Disciplinary Perspectives. Trends Mol. Med. 2020, 26, 483–495. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. CODI_19 Weekly Epidemiologic Update. Glob. Overv. 2022, 110, 1–23. [Google Scholar]
- Wang, Q.; Zhang, Y.; Wu, L.; Niu, S.; Song, C.; Zhang, Z.; Lu, G.; Qiao, C.; Hu, Y.; Yuen, K.Y.; et al. Structural and Functional Basis of SARS-CoV-2 Entry by Using Human ACE2. Cell 2020, 181, 894–904.e9. [Google Scholar] [CrossRef]
- Phan, T. Genetic Diversity and Evolution of SARS-CoV-2. Infect. Genet. Evol. 2020, 81, 104260. [Google Scholar] [CrossRef] [PubMed]
- Kujawska, M.; Mostafavi, E.; Kaushik, A. SARS-CoV-2 Getting into the Brain; Neurological Phenotype of COVID-19, and Management by Nano-Biotechnology. Neural Regen. Res. 2023, 18, 519–520. [Google Scholar] [CrossRef]
- Maurya, S.K.; Baghel, M.S.; Gaurav, Chaudhary, V.; Kaushik, A.; Gautam, A. Putative Role of Mitochondria in SARS-CoV-2 Mediated Brain Dysfunctions: A Prospect. Biotechnol. Genet. Eng. Rev. 2022, 2022, 1–26. [Google Scholar] [CrossRef] [PubMed]
- Cherusseri, J.; Savio, C.M.; Khalid, M.; Chaudhary, V.; Numan, A.; Varma, S.J.; Menon, A.; Kaushik, A. SARS-CoV-2-on-Chip for Long COVID Management. Biosensors 2022, 12, 890. [Google Scholar] [CrossRef]
- Ding, Y.; Wang, H.; Shen, H.; Li, Z.; Geng, J.; Han, H.; Cai, J.; Li, X.; Kang, W.; Weng, D.; et al. The Clinical Pathology of Severe Acute Respiratory Syndrome (SARS): A Report from China. J. Pathol. 2003, 200, 282–289. [Google Scholar] [CrossRef]
- Rabi, F.A.; al Zoubi, M.S.; Al-Nasser, A.D.; Kasasbeh, G.A.; Salameh, D.M. SARS-CoV-2 and Coronavirus Disease 2019: What We Know So Far. Pathogens 2020, 9, 231. [Google Scholar] [CrossRef]
- Lotfi, M.; Hamblin, M.R.; Rezaei, N. COVID-19: Transmission, Prevention, and Potential Therapeutic Opportunities. Clinica Chimica Acta 2020, 508, 254–266. [Google Scholar] [CrossRef]
- Lurie, N.; Saville, M.; Hatchett, R.; Halton, J. Developing Covid-19 Vaccines at Pandemic Speed. New Engl. J. Med. 2020, 382, 1969–1973. [Google Scholar] [CrossRef] [PubMed]
- Mainardes, R.M.; Diedrich, C. The Potential Role of Nanomedicine on COVID-19 Therapeutics. Ther. Deliv. 2020, 11, 411–414. [Google Scholar] [CrossRef]
- Sahu, K.K.; Lal, A.; Mishra, A.K. Latest Updates on COVID-2019: A Changing Paradigm Shift. J. Med. Virol. 2020, 92, 533–535. [Google Scholar] [CrossRef]
- Shereen, M.A.; Khan, S.; Kazmi, A.; Bashir, N.; Siddique, R. COVID-19 Infection: Emergence, Transmission, and Characteristics of Human Coronaviruses. J. Adv. Res. 2020, 24, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Petrosillo, N.; Viceconte, G.; Ergonul, O.; Ippolito, G.; Petersen, E. COVID-19, SARS and MERS: Are They Closely Related? Clin. Microbiol. Infect. 2020, 26, 729–734. [Google Scholar] [CrossRef] [PubMed]
- Jagtap, V.S.; Jha, U.; More, P.; Urmilesh Jha, D. A Review of the 2019 Novel Coronavirus (COVID-19) Based on Current Evidence. Pharma Innov. J. 2020, 9, 7–10. [Google Scholar]
- Wu, J.T.; Leung, K.; Bushman, M.; Kishore, N.; Niehus, R.; de Salazar, P.M.; Cowling, B.J.; Lipsitch, M.; Leung, G.M. Estimating Clinical Severity of COVID-19 from the Transmission Dynamics in Wuhan, China. Nat. Med. 2020, 26, 506–510. [Google Scholar] [CrossRef] [PubMed]
- Vijgen, L.; Keyaerts, E.; Moës, E.; Maes, P.; Duson, G.; van Ranst, M. Development of One-Step, Real-Time, Quantitative Reverse Transcriptase PCR Assays for Absolute Quantitation of Human Coronaviruses OC43 and 229E. J. Clin. Microbiol. 2005, 43, 5452–5456. [Google Scholar] [CrossRef] [PubMed]
- Woo, P.C.Y.; Huang, Y.; Lau, S.K.P.; Yuen, K.Y. Coronavirus Genomics and Bioinformatics Analysis. Viruses 2010, 2, 1804–1820. [Google Scholar] [CrossRef]
- Pene, F.; Merlat, A.; Vabret, A.; Rozenberg, F.; Buzyn, A.; Dreyfus, F.; Cariou, A.; Freymuth, F.; Lebon, P. Coronavirus 229E-Related Pneumonia in Immunocompromised Patients. Clin. Infect. Dis. 2003, 37, 929–932. [Google Scholar] [CrossRef]
- Chan, J.F.W.; Lau, S.K.P.; To, K.K.W.; Cheng, V.C.C.; Woo, P.C.Y.; Yue, K.Y. Middle East Respiratory Syndrome Coronavirus: Another Zoonotic Betacoronavirus Causing SARS-like Disease. Clin. Microbiol. Rev. 2015, 28, 465–522. [Google Scholar] [CrossRef]
- Yan, R.; Zhang, Y.; Li, Y.; Xia, L.; Guo, Y.; Zhou, Q. Structural Basis for the Recognition of SARS-CoV-2 by Full-Length Human ACE2. Science 2020, 367, 1444–1448. [Google Scholar] [CrossRef]
- Walls, A.C.; Park, Y.J.; Tortorici, M.A.; Wall, A.; McGuire, A.T.; Veesler, D. Structure, Function, and Antigenicity of the SARS-CoV-2 Spike Glycoprotein. Cell 2020, 181, 281–292.e6. [Google Scholar] [CrossRef]
- Kaushik, A.; Mostafavi, E. To Manage Long COVID by Selective SARS-CoV-2 Infection Biosensing Engineering Hydrogels and Electrospun Scaffolds for Wound Healing Applications View Project Aloe Vera-Mediated Synthesis of Metallic Nanoparticles View Project. Innovation 2022, 3, 100303. [Google Scholar] [CrossRef]
- Letko, M.; Marzi, A.; Munster, V. Functional Assessment of Cell Entry and Receptor Usage for SARS-CoV-2 and Other Lineage B Betacoronaviruses. Nat. Microbiol. 2020, 5, 562–569. [Google Scholar] [CrossRef] [PubMed]
- Bestle, D.; Heindl, M.R.; Limburg, H.; van Lam van, T.; Pilgram, O.; Moulton, H.; Stein, D.A.; Hardes, K.; Eickmann, M.; Dolnik, O.; et al. TMPRSS2 and Furin Are Both Essential for Proteolytic Activation of SARS-CoV-2 in Human Airway Cells. Life Sci. Alliance 2020, 3, 1–14. [Google Scholar] [CrossRef]
- Chen, L.; Li, X.; Chen, M.; Feng, Y.; Xiong, C. The ACE2 Expression in Human Heart Indicates New Potential Mechanism of Heart Injury among Patients Infected with SARS-CoV-2. Cardiovasc. Res. 2020, 116, 1097–1100. [Google Scholar] [CrossRef]
- Leung, J.M.; Yang, C.X.; Tam, A.; Shaipanich, T.; Hackett, T.L.; Singhera, G.K.; Dorscheid, D.R.; Sin, D.D. ACE-2 Expression in the Small Airway Epithelia of Smokers and COPD Patients: Implications for COVID-19. Eur. Respir. J. 2020, 55, 2000688. [Google Scholar] [CrossRef]
- van Doremalen, N.; Bushmaker, T.; Morris, D.H.; Holbrook, M.G.; Gamble, A.; Williamson, B.N.; Tamin, A.; Harcourt, J.L.; Thornburg, N.J.; Gerber, S.I.; et al. Aerosol and Surface Stability of HCoV-19 (SARS-CoV-2) Compared to SARS-CoV-1. medRxiv 2020. [Google Scholar] [CrossRef]
- Lu, X.; Zhang, L.; Du, H.; Zhang, J.; Li, Y.Y.; Qu, J.; Zhang, W.; Wang, Y.; Bao, S.; Li, Y.; et al. SARS-CoV-2 Infection in Children. New Engl. J. Med. 2020, 382, 1663–1665. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical Course and Risk Factors for Mortality of Adult Inpatients with COVID-19 in Wuhan, China: A Retrospective Cohort Study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef] [PubMed]
- Blanco-Melo, D.; Nilsson-Payant, B.E.; Liu, W.C.; Uhl, S.; Hoagland, D.; Møller, R.; Jordan, T.X.; Oishi, K.; Panis, M.; Sachs, D.; et al. Imbalanced Host Response to SARS-CoV-2 Drives Development of COVID-19. Cell 2020, 181, 1036–1045.e9. [Google Scholar] [CrossRef] [PubMed]
- Kumar, R.; Siril, P.F.; Javid, F. Unusual Anti-Leukemia Activity of Nanoformulated Naproxen and Other Non-Steroidal Anti-Inflammatory Drugs. Mater. Sci. Eng. C 2016, 69, 1335–1344. [Google Scholar] [CrossRef]
- Choy, K.T.; Wong, A.Y.L.; Kaewpreedee, P.; Sia, S.F.; Chen, D.; Hui, K.P.Y.; Chu, D.K.W.; Chan, M.C.W.; Cheung, P.P.H.; Huang, X.; et al. Remdesivir, Lopinavir, Emetine, and Homoharringtonine Inhibit SARS-CoV-2 Replication in Vitro. Antiviral. Res. 2020, 178, 104786. [Google Scholar] [CrossRef]
- Wang, Y.; Zhang, D.; Du, G.; Du, R.; Zhao, J.; Jin, Y.; Fu, S.; Gao, L.; Cheng, Z.; Lu, Q.; et al. Remdesivir in Adults with Severe COVID-19: A Randomised, Double-Blind, Placebo-Controlled, Multicentre Trial. Lancet 2020, 395, 1569–1578. [Google Scholar] [CrossRef] [PubMed]
- McCoy, J.A.; Short, W.R.; Srinivas, S.K.; Levine, L.D.; Hirshberg, A. Compassionate Use of Remdesivir for Treatment of Severe Coronavirus Disease 2019 in Pregnant Women at a United States Academic Center. Am. J. Obstet. Gynecol. MFM 2020, 2, 100164. [Google Scholar] [CrossRef]
- Hernandez, A.V.; Phan, M.T.; Rocco, J.; Pasupuleti, V.; Barboza, J.J.; Piscoya, A.; Roman, Y.M.; White, C.M. Efficacy and Safety of Hydroxychloroquine for Hospitalized Covid-19 Patients: A Systematic Review and Meta-Analysis. J. Clin. Med. 2021, 10, 2503. [Google Scholar] [CrossRef]
- Xia, S.; Zhu, Y.; Liu, M.; Lan, Q.; Xu, W.; Wu, Y.; Ying, T.; Liu, S.; Shi, Z.; Jiang, S.; et al. Fusion Mechanism of 2019-NCoV and Fusion Inhibitors Targeting HR1 Domain in Spike Protein. Cell. Mol. Immunol. 2020, 17, 765–767. [Google Scholar] [CrossRef]
- Wrapp, D.; de Vlieger, D.; Corbett, K.S.; Torres, G.M.; Wang, N.; van Breedam, W.; Roose, K.; van Schie, L.; Hoffmann, M.; Pöhlmann, S.; et al. Structural Basis for Potent Neutralization of Betacoronaviruses by Single-Domain Camelid Antibodies. Cell 2020, 181, 1004–1015.e15. [Google Scholar] [CrossRef]
- Wang, C.; Li, W.; Drabek, D.; Okba, N.M.A.; van Haperen, R.; Osterhaus, A.D.M.E.; van Kuppeveld, F.J.M.; Haagmans, B.L.; Grosveld, F.; Bosch, B.J. A Human Monoclonal Antibody Blocking SARS-CoV-2 Infection. Nat. Commun 2020, 11, 2251. [Google Scholar] [CrossRef]
- Pinto, D.; Park, Y.J.; Beltramello, M.; Walls, A.C.; Tortorici, M.A.; Bianchi, S.; Jaconi, S.; Culap, K.; Zatta, F.; De Marco, A.; et al. Cross-Neutralization of SARS-CoV-2 by a Human Monoclonal SARS-CoV Antibody. Nature 2020, 583, 290–295. [Google Scholar] [CrossRef]
- Tanaka, T.; Narazaki, M.; Kishimoto, T. Immunotherapeutic Implications of IL-6 Blockade for Cytokine Storm. Immunotherapy 2016, 8, 959–970. [Google Scholar] [CrossRef]
- Schrezenmeier, E.; Dörner, T. Mechanisms of Action of Hydroxychloroquine and Chloroquine: Implications for Rheumatology. Nat. Rev. Rheumatol. 2020, 16, 155–166. [Google Scholar] [CrossRef]
- Della-Torre, E.; Campochiaro, C.; Cavalli, G.; De Luca, G.; Napolitano, A.; La Marca, S.; Boffini, N.; Da Prat, V.; di Terlizzi, G.; Lanzillotta, M.; et al. Interleukin-6 Blockade with Sarilumab in Severe COVID-19 Pneumonia with Systemic Hyperinflammation: An Open-Label Cohort Study. Ann. Rheum. Dis. 2020, 79, 1277–1285. [Google Scholar] [CrossRef]
- Zhai, P.; Ding, Y.; Wu, X.; Long, J.; Zhong, Y.; Li, Y. The Epidemiology, Diagnosis and Treatment of COVID-19. Int. J. Antimicrob. Agents 2020, 55, 105955. [Google Scholar] [CrossRef]
- Zhou, P.; Yang, X.L.; Wang, X.G.; Hu, B.; Zhang, L.; Zhang, W.; Si, H.R.; Zhu, Y.; Li, B.; Huang, C.L.; et al. Addendum: A Pneumonia Outbreak Associated with a New Coronavirus of Probable Bat Origin. Nature 2020, 588, E6. [Google Scholar] [CrossRef] [PubMed]
- Shen, C.; Wang, Z.; Zhao, F.; Yang, Y.; Li, J.; Yuan, J.; Wang, F.; Li, D.; Yang, M.; Xing, L.; et al. Treatment of 5 Critically Ill Patients With COVID-19 With Convalescent Plasma. JAMA 2020, 323, 1582–1589. [Google Scholar] [CrossRef]
- Benvenuto, D.; Giovanetti, M.; Ciccozzi, A.; Spoto, S.; Angeletti, S.; Ciccozzi, M. The 2019-New Coronavirus Epidemic: Evidence for Virus Evolution. J. Med. Virol. 2020, 92, 455–459. [Google Scholar] [CrossRef]
- Andersen, K.G.; Rambaut, A.; Lipkin, W.I.; Holmes, E.C.; Garry, R.F. The Proximal Origin of SARS-CoV-2. Nat. Med. 2020, 26, 450–452. [Google Scholar] [CrossRef]
- Enjuanes, L.; Zuñiga, S.; Castaño-Rodriguez, C.; Gutierrez-Alvarez, J.; Canton, J.; Sola, I. Molecular Basis of Coronavirus Virulence and Vaccine Development. Adv. Virus Res. 2016, 96, 245–286. [Google Scholar] [CrossRef]
- Song, Z.; Xu, Y.; Bao, L.; Zhang, L.; Yu, P.; Qu, Y.; Zhu, H.; Zhao, W.; Han, Y.; Qin, C. From SARS to MERS, Thrusting Coronaviruses into the Spotlight. Viruses 2019, 11, 59. [Google Scholar] [CrossRef] [PubMed]
- Thi Nhu Thao, T.; Labroussaa, F.; Ebert, N.; V’kovski, P.; Stalder, H.; Portmann, J.; Kelly, J.; Steiner, S.; Holwerda, M.; Kratzel, A.; et al. Rapid Reconstruction of SARS-CoV-2 Using a Synthetic Genomics Platform. Nature 2020, 582, 561–565. [Google Scholar] [CrossRef] [PubMed]
- Xie, X.; Muruato, A.; Lokugamage, K.G.; Narayanan, K.; Zhang, X.; Zou, J.; Liu, J.; Schindewolf, C.; Bopp, N.E.; Aguilar, P.V.; et al. An Infectious CDNA Clone of SARS-CoV-2. Cell Host Microbe 2020, 27, 841–848.e3. [Google Scholar] [CrossRef]
- Chen, W.H.; Strych, U.; Hotez, P.J.; Bottazzi, M.E. The SARS-CoV-2 Vaccine Pipeline: An Overview. Curr. Trop. Med. Rep. 2020, 7, 61–64. [Google Scholar] [CrossRef] [PubMed]
- Bull, J.J.; Nuismer, S.L.; Antia, R. Recombinant Vector Vaccine Evolution. PLoS Comput. Biol. 2019, 15, e1006857. [Google Scholar] [CrossRef] [PubMed]
- Thanh Le, T.; Andreadakis, Z.; Kumar, A.; Gómez Román, R.; Tollefsen, S.; Saville, M.; Mayhew, S. The COVID-19 Vaccine Development Landscape. Nat. Rev. Drug. Discov. 2020, 19, 305–306. [Google Scholar] [CrossRef] [PubMed]
- Gomez, C.E.; Najera, J.L.; Krupa, M.; Perdiguero, B.; Esteban, M. MVA and NYVAC as Vaccines against Emergent Infectious Diseases and Cancer. Curr. Gene Ther. 2011, 11, 189–217. [Google Scholar] [CrossRef]
- Sutter, G.; Staib, C. Vaccinia Vectors as Candidate Vaccines: The Development of Modified Vaccinia Virus Ankara for Antigen Delivery. Curr. Drug Targets Infect. Disord. 2003, 3, 263–271. [Google Scholar] [CrossRef]
- Sullivan, N.J.; Sanchez, A.; Rollin, P.E.; Yang, Z.Y.; Nabel, G.J. Development of a Preventive Vaccine for Ebola Virus Infection in Primates. Nature 2000, 408, 605–609. [Google Scholar] [CrossRef] [PubMed]
- Urabe, M.; Ding, C.; Kotin, R.M. Insect Cells as a Factory to Produce Adeno-Associated Virus Type 2 Vectors. Hum. Gene Ther. 2004, 13, 1935–1943. [Google Scholar] [CrossRef]
- Li, H.; Malani, N.; Hamilton, S.R.; Schlachterman, A.; Bussadori, G.; Edmonson, S.E.; Shah, R.; Arruda, V.R.; Mingozzi, F.; Wright, J.F.; et al. Assessing the Potential for AAV Vector Genotoxicity in a Murine Model. Blood 2011, 117, 3311–3319. [Google Scholar] [CrossRef]
- Singh, A.; Singh, P.; Kumar, R.; Kaushik, A. Exploring Nanoselenium to Tackle Mutated SARS-CoV-2 for Efficient COVID-19 Management. Front. Nanotechnol. 2022, 4, 71. [Google Scholar] [CrossRef]
- Vincent, M.; de Lázaro, I.; Kostarelos, K. Graphene Materials as 2D Non-Viral Gene Transfer Vector Platforms. Gene Ther. 2016, 24, 123–132. [Google Scholar] [CrossRef]
- Yin, H.; Kanasty, R.L.; Eltoukhy, A.A.; Vegas, A.J.; Dorkin, J.R.; Anderson, D.G. Non-Viral Vectors for Gene-Based Therapy. Nat. Rev. Genet. 2014, 15, 541–555. [Google Scholar] [CrossRef] [PubMed]
- Gregory, A.E.; Titball, R.; Williamson, D. Vaccine Delivery Using Nanoparticles. Front. Cell Infect. Microbiol. 2013, 4, 13. [Google Scholar] [CrossRef]
- Panyam, J.; Labhasetwar, V. Biodegradable Nanoparticles for Drug and Gene Delivery to Cells and Tissue. Adv. Drug Deliv. Rev. 2003, 55, 329–347. [Google Scholar] [CrossRef] [PubMed]
- Shen, Y.; Hao, T.; Ou, S.; Hu, C.; Chen, L. Applications and Perspectives of Nanomaterials in Novel Vaccine Development. MedChemComm 2018, 9, 226–238. [Google Scholar] [CrossRef] [PubMed]
- Bonam, S.R.; Kotla, N.G.; Bohara, R.A.; Rochev, Y.; Webster, T.J.; Bayry, J. Potential Immuno-Nanomedicine Strategies to Fight COVID-19 like Pulmonary Infections. Nano Today 2021, 36, 101051. [Google Scholar] [CrossRef]
- Qi, F.; Wu, J.; Li, H.; Ma, G. Recent Research and Development of PLGA/PLA Microspheres/Nanoparticles: A Review in Scientific and Industrial Aspects. Front. Chem. Sci. Eng. 2018, 13, 14–27. [Google Scholar] [CrossRef]
- Levina, A.S.; Repkova, M.N.; Mazurkova, N.A.; Zarytova, V.F. Nanoparticle-Mediated Nonviral DNA Delivery for Effective Inhibition of Influenza a Viruses in Cells. IEEE Trans. Nanotechnol. 2016, 15, 248–254. [Google Scholar] [CrossRef]
- Dunning, J.; Sahr, F.; Rojek, A.; Gannon, F.; Carson, G.; Idriss, B.; Massaquoi, T.; Gandi, R.; Joseph, S.; Osman, H.K.; et al. Experimental Treatment of Ebola Virus Disease with TKM-130803: A Single-Arm Phase 2 Clinical Trial. PLoS Med. 2016, 13, e1001997. [Google Scholar] [CrossRef]
- Orkin, C.; Squires, K.E.; Molina, J.M.; Sax, P.E.; Wong, W.W.; Sussmann, O.; Kaplan, R.; Lupinacci, L.; Rodgers, A.; Xu, X.; et al. Doravirine/Lamivudine/Tenofovir Disoproxil Fumarate Is Non-Inferior to Efavirenz/Emtricitabine/Tenofovir Disoproxil Fumarate in Treatment-Naive Adults with Human Immunodeficiency Virus–1 Infection: Week 48 Results of the DRIVE-AHEAD Trial. Clin. Infect. Dis. 2019, 68, 535–544. [Google Scholar] [CrossRef]
- Cavalli, R.; Donalisio, M.; Bisazza, A.; Civra, A.; Ranucci, E.; Ferruti, P.; Lembo, D. Enhanced Antiviral Activity of Acyclovir Loaded into Nanoparticles. Methods Enzymol. 2012, 509, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Lembo, D.; Swaminathan, S.; Donalisio, M.; Civra, A.; Pastero, L.; Aquilano, D.; Vavia, P.; Trotta, F.; Cavalli, R. Encapsulation of Acyclovir in New Carboxylated Cyclodextrin-Based Nanosponges Improves the Agent’s Antiviral Efficacy. Int. J. Pharm. 2013, 443, 262–272. [Google Scholar] [CrossRef] [PubMed]
- Manzoor, S.; Saalim, M.; Imran, M.; Resham, S.; Ashraf, J. Hepatitis B Virus Therapy: What’s the Future Holding for Us? World J. Gastroenterol. 2015, 21, 12558. [Google Scholar] [CrossRef]
- Szunerits, S.; Barras, A.; Khanal, M.; Pagneux, Q.; Boukherroub, R. Nanostructures for the Inhibition of Viral Infections. Molecules 2015, 20, 14051–14081. [Google Scholar] [CrossRef]
- Broglie, J.J.; Alston, B.; Yang, C.; Ma, L.; Adcock, A.F.; Chen, W.; Yang, L. Antiviral Activity of Gold/Copper Sulfide Core/Shell Nanoparticles against Human Norovirus Virus-Like Particles. PLoS One 2015, 10, e0141050. [Google Scholar] [CrossRef]
- Sana, S.; Vadde, R.; Kumar, R.; Arla, S.; Somala, A.; Rao, K.K.; Zhijun, Z.; Boya, V.; Mondal, K.; Mamidi, N. Eco-friendly and facile production of antibacterial zinc oxide nanoparticles from Greqia Flavescens (G. flavescens) leaf extract for biomedicial applications. J. Drug Deliv. Sci. Technol. 2023, 80, 104186. [Google Scholar] [CrossRef]
- Lammers, T.; Sofias, A.M.; van der Meel, R.; Schiffelers, R.; Storm, G.; Tacke, F.; Koschmieder, S.; Brümmendorf, T.H.; Kiessling, F.; Metselaar, J.M. Dexamethasone Nanomedicines for COVID-19. Nat. Nanotechnol. 2020, 15, 622–624. [Google Scholar] [CrossRef] [PubMed]
- Alshweiat, A.; Ambrus, R.; Csóka, I. Intranasal Nanoparticulate Systems as Alternative Route of Drug Delivery. Curr. Med. Chem. 2019, 26, 6459–6492. [Google Scholar] [CrossRef]
- Costantino, H.R.; Illum, L.; Brandt, G.; Johnson, P.H.; Quay, S.C. Intranasal Delivery: Physicochemical and Therapeutic Aspects. Int. J. Pharm. 2007, 337, 1–24. [Google Scholar] [CrossRef] [PubMed]
- Marasini, N.; Kaminskas, L.M. Subunit-Based Mucosal Vaccine Delivery Systems for Pulmonary Delivery—Are They Feasible? Drug Dev. Ind. Pharm. 2019, 45, 882–894. [Google Scholar] [CrossRef] [PubMed]
- Kumar, R. Lipid-Based Nanoparticles for Drug-Delivery Systems. In Nanocarriers for Drug Delivery: Nanoscience and Nanotechnology in Drug Delivery; Elservier: Amsterdam, The Netherlands, 2019; pp. 249–284. [Google Scholar] [CrossRef]
- Kumar, R.; Islam, T.; Nurunnabi, M. Mucoadhesive Carriers for Oral Drug Delivery. J. Control. Release 2022, 351, 504–559. [Google Scholar] [CrossRef]
- Kumar, A.; Pandey, A.N.; Jain, S.K. Nasal-Nanotechnology: Revolution for Efficient Therapeutics Delivery. Drug Deliv. 2016, 23, 681–693. [Google Scholar] [CrossRef] [PubMed]
- LaBauve, A.E.; Rinker, T.E.; Noureddine, A.; Serda, R.E.; Howe, J.Y.; Sherman, M.B.; Rasley, A.; Brinker, C.J.; Sasaki, D.Y.; Negrete, O.A. Lipid-Coated Mesoporous Silica Nanoparticles for the Delivery of the ML336 Antiviral to Inhibit Encephalitic Alphavirus Infection. Sci. Rep. 2018, 8, 13990. [Google Scholar] [CrossRef]
- Adams, D.; Gonzalez-Duarte, A.; O’Riordan, W.D.; Yang, C.-C.; Ueda, M.; Kristen, A.V.; Tournev, I.; Schmidt, H.H.; Coelho, T.; Berk, J.L.; et al. Patisiran, an RNAi Therapeutic, for Hereditary Transthyretin Amyloidosis. New Engl. J. Med. 2018, 379, 11–21. [Google Scholar] [CrossRef]
- Sarkar, C.; Kommineni, N.; Butreddy, A.; Kumar, R.; Bunekar, N.; Gugulothu, K. PLGA Nanoparticles in Drug Delivery. In Nanoengineering of Biomaterials; Wiley Online Library: Hoboken, NJ, USA, 2022; pp. 217–260. [Google Scholar] [CrossRef]
- Chua, B.Y.; Al Kobaisi, M.; Zeng, W.; Mainwaring, D.; Jackson, D.C. Chitosan Microparticles and Nanoparticles as Biocompatible Delivery Vehicles for Peptide and Protein-Based Immunocontraceptive Vaccines. Mol. Pharm 2012, 9, 81–90. [Google Scholar] [CrossRef] [PubMed]
- Ashton, S.; Song, Y.H.; Nolan, J.; Cadogan, E.; Murray, J.; Odedra, R.; Foster, J.; Hall, P.A.; Low, S.; Taylor, P.; et al. Aurora Kinase Inhibitor Nanoparticles Target Tumors with Favorable Therapeutic Index In Vivo. Sci. Transl. Med. 2016, 8, 325ra17. [Google Scholar] [CrossRef]
- Lee, C.C.; MacKay, J.A.; Fréchet, J.M.J.; Szoka, F.C. Designing Dendrimers for Biological Applications. Nat. Biotechnol. 2005, 23, 1517–1526. [Google Scholar] [CrossRef] [PubMed]
- Tomalia, D.A.; Reyna, L.A.; Svenson, S. Dendrimers as Multi-Purpose Nanodevices for Oncology Drug Delivery and Diagnostic Imaging. Biochem Soc. Trans. 2007, 35, 61–67. [Google Scholar] [CrossRef]
- Salazar-González, J.A.; González-Ortega, O.; Rosales-Mendoza, S. Gold Nanoparticles and Vaccine Development. Expert Rev. Vaccines 2015, 14, 1197–1211. [Google Scholar] [CrossRef]
- Kumar, R.; Mehta, P.; Shankar, K.; Rajora, M.; Mishra, Y.; Mostafavi, E.; Kaushik, A. Nanotechnolo-gy-assisted metered-dose inhalers (MDIs) for high-performance pulmonary drug delivery applications. Pharmaceu-Tical Res. 2022, 39, 2831–2855. [Google Scholar] [CrossRef] [PubMed]
- Murata, K.; Lechmann, M.; Qiao, M.; Gunji, T.; Altert, H.J.; Liang, T.J. Immunization with Hepatitis C Virus-like Particles Protects Mice from Recombinant Hepatitis C Virus-Vaccinia Infection. Proc. Natl. Acad. Sci. USA 2003, 100, 6753–6758. [Google Scholar] [CrossRef]
- Quan, F.-S.; Compans, R.W.; Nguyen, H.H.; Kang, S.-M. Induction of Heterosubtypic Immunity to Influenza Virus by Intranasal Immunization. J. Virol. 2008, 82, 1350–1359. [Google Scholar] [CrossRef]
- Lee, Y.T.; Ko, E.J.; Lee, Y.; Kim, K.H.; Kim, M.C.; Lee, Y.N.; Kang, S.M. Intranasal Vaccination with M2e5x Virus-like Particles Induces Humoral and Cellular Immune Responses Conferring Cross-Protection against Heterosubtypic Influenza Viruses. PLoS ONE 2018, 13, e0190868. [Google Scholar] [CrossRef] [PubMed]
- Hu, C.M.J.; Fang, R.H.; Copp, J.; Luk, B.T.; Zhang, L. A Biomimetic Nanosponge That Absorbs Pore-Forming Toxins. Nat. Nanotechnol. 2013, 8, 336–340. [Google Scholar] [CrossRef]
- Rao, L.; Xia, S.; Xu, W.; Tian, R.; Yu, G.; Gu, C.; Pan, P.; Meng, Q.F.; Cai, X.; Qu, D.; et al. Decoy Nanoparticles Protect against COVID-19 by Concurrently Adsorbing Viruses and Inflammatory Cytokines. Proc. Natl. Acad. Sci. USA 2020, 117, 27141–27147. [Google Scholar] [CrossRef]
- Keller, M.D.; Ching, K.L.; Liang, F.X.; Dhabaria, A.; Tam, K.; Ueberheide, B.M.; Unutmaz, D.; Torres, V.J.; Cadwell, K. Decoy Exosomes Provide Protection against Bacterial Toxins. Nature 2020, 579, 260–264. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Honko, A.; Zhou, J.; Gong, H.; Downs, S.N.; Vasquez, J.H.; Fang, R.H.; Gao, W.; Griffiths, A.; Zhang, L. Cellular Nanosponges Inhibit SARS-CoV-2 Infectivity. Nano Lett. 2020, 20, 5570–5574. [Google Scholar] [CrossRef]
- Patil, A.A.; Rhee, W.J. Exosomes: Biogenesis, Composition, Functions, and Their Role in Pre-Metastatic Niche Formation. Biotechnol. Bioprocess. Eng. 2019, 24, 689–701. [Google Scholar] [CrossRef]
- Kuate, S.; Cinatl, J.; Doerr, H.W.; Überla, K. Exosomal Vaccines Containing the S Protein of the SARS Coronavirus Induce High Levels of Neutralizing Antibodies. Virology 2007, 362, 26. [Google Scholar] [CrossRef] [PubMed]
- Cavalcanti, I.D.L.; Cajubá de Britto Lira Nogueira, M. Pharmaceutical Nanotechnology: Which Products Are Been Designed against COVID-19? J. Nanoparticle Res. 2020, 22, 276. [Google Scholar] [CrossRef]
- Yang, W.; Peters, J.I.; Williams, R.O. Inhaled Nanoparticles—A Current Review. Int. J. Pharm. 2008, 356, 239–247. [Google Scholar] [CrossRef]
- Justo, O.R.; Moraes, Â.M. Incorporation of Antibiotics in Liposomes Designed for Tuberculosis Therapy by Inhalation. Drug Deliv. 2008, 10, 201–207. [Google Scholar] [CrossRef]
- Schreier, H.; Gonzalez-Rothi, R.J.; Stecenko, A.A. Pulmonary Delivery of Liposomes. J. Control. Release 1993, 24, 209–223. [Google Scholar] [CrossRef]
- Joshi, M.; Misra, A.N. Pulmonary Disposition of Budesonide from Liposomal Dry Powder Inhaler. Methods Find. Exp. Clin. Pharmacol. 2001, 23, 531–536. [Google Scholar] [CrossRef] [PubMed]
- White, S.; Bennett, D.B.; Cheu, S.; Conley, P.W.; Guzek, D.B.; Gray, S.; Howard, J.; Malcolmson, R.; Parker, J.M.; Roberts, P.; et al. EXUBERA®: Pharmaceutical Development of a Novel Product for Pulmonary Delivery of Insulin. Diabetes Technol. Ther. 2005, 7, 896–906. [Google Scholar] [CrossRef] [PubMed]
- Vetvicka, D.; Sivak, L.; Jogdeo, C.M.; Kumar, R.; Khan, R.; Hang, Y.; Oupický, D. Gene Silencing Delivery Systems for the Treatment of Pancreatic Cancer: Where and What to Target Next? J. Control. Release 2021, 331, 246–259. [Google Scholar] [CrossRef] [PubMed]
- Sultana, A.; Kumar, R. Modified bactofection for efficient and functional DNA delivery using invasive E. coli DH10B vector into human epithelial cell line. J. Drug Deliv. Sci. Technol. 2022, 70, 103159. [Google Scholar] [CrossRef]
- Cryan, S.A.; Devocelle, M.; Moran, P.J.; Hickey, A.J.; Kelly, J.G. Increased Intracellular Targeting to Airway Cells Using Octaarginine-Coated Liposomes: In Vitro Assessment of Their Suitability for Inhalation. Mol. Pharm. 2006, 3, 104–112. [Google Scholar] [CrossRef]
- Densmore, C.L. Advances in Noninvasive Pulmonary Gene Therapy. Curr. Drug Deliv. 2006, 3, 55–63. [Google Scholar] [CrossRef]
- Kaushik, A. Manipulative Magnetic Nanomedicine: The Future of COVID-19 Pandemic/Endemic Therapy. Expert Opin. Drug Deliv. 2020, 18, 531–534. [Google Scholar] [CrossRef]
- Walker, J.; Albert, J.; Liang, D.; Sun, J.; Schutzman, R.; Kumar, R.; White, C.; Beck-Broichsitter, M.; Schwendeman, S. In vitro degradation and wrosion behavior of commercial PLGAs used for controlled drug delivery. Drug Deliv. Transl. Res. 2023, 13, 237–251. [Google Scholar] [CrossRef]
- Tiwari, S.; Juneja, S.; Ghosal, A.; Bandara, N.; Khan, R.; Wallen, S.L.; Ramakrishna, S.; Kaushik, A. Antibacterial and Antiviral High-Performance Nanosystems to Mitigate New SARS-CoV-2 Variants of Concern. Curr. Opin. Biomed. Eng. 2022, 21, 100363. [Google Scholar] [CrossRef]
- Dubey, A.K.; Chaudhry, S.K.; Singh, H.B.; Gupta, V.K.; Kaushik, A. Perspectives on Nano-Nutraceuticals to Manage Pre and Post COVID-19 Infections. Biotechnol. Rep. 2022, 33, e00712. [Google Scholar] [CrossRef]
- Jasrotia, R.; Dhanjal, D.S.; Bhardwaj, S.; Sharma, P.; Chopra, C.; Singh, R.; Kumar, A.; Mubayi, A.; Kumar, D.; Kumar, R.; et al. Nanotechnology Based Vaccines: Cervical Cancer Management and Perspectives. J. Drug Deliv. Sci. Technol. 2022, 71, 103351. [Google Scholar] [CrossRef]
- Machhi, J.; Shahjin, F.; Das, S.; Patel, M.; Abdelmoaty, M.M.; Cohen, J.D.; Singh, P.A.; Baldi, A.; Bajwa, N.; Kumar, R.; et al. Nanocarrier Vaccines for SARS-CoV-2. Adv. Drug Deliv. Rev. 2021, 171, 215–239. [Google Scholar] [CrossRef] [PubMed]
- Machhi, J.; Shahjin, F.; Das, S.; Patel, M.; Abdelmoaty, M.M.; Cohen, J.D.; Singh, P.A.; Baldi, A.; Bajwa, N.; Kumar, R.; et al. A Role for Extracellular Vesicles in SARS-CoV-2 Therapeutics and Prevention. J. Neuroimmune Pharmacol. 2021, 16, 270–288. [Google Scholar] [CrossRef] [PubMed]
- Lu, R.; Zhao, X.; Li, J.; Niu, P.; Yang, B.; Wu, H.; Wang, W.; Song, H.; Huang, B.; Zhu, N.; et al. Genomic Characterisation and Epidemiology of 2019 Novel Coronavirus: Implications for Virus Origins and Receptor Binding. Lancet 2020, 395, 565–574. [Google Scholar] [CrossRef]
- Coleman, C.M.; Liu, Y.V.; Mu, H.; Taylor, J.K.; Massare, M.; Flyer, D.C.; Glenn, G.M.; Smith, G.E.; Frieman, M.B. Purified Coronavirus Spike Protein Nanoparticles Induce Coronavirus Neutralizing Antibodies in Mice. Vaccine 2014, 32, 3169–3174. [Google Scholar] [CrossRef] [PubMed]
- Takashima, Y.; Osaki, M.; Ishimaru, Y.; Yamaguchi, H.; Harada, A.; Takashima, Y.; Osaki, M.; Yamaguchi, H.; Harada, A.; Ishimaru, Y. Artificial Molecular Clamp: A Novel Device for Synthetic Polymerases. Angew. Chem. Int. Ed. 2011, 50, 7524–7528. [Google Scholar] [CrossRef]
- Tai, W.; He, L.; Zhang, X.; Pu, J.; Voronin, D.; Jiang, S.; Zhou, Y.; Du, L. Characterization of the Receptor-Binding Domain (RBD) of 2019 Novel Coronavirus: Implication for Development of RBD Protein as a Viral Attachment Inhibitor and Vaccine. Cell. Mol. Immunol. 2020, 17, 613–620. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Zhou, Q.; Li, Y.; Garner, L.V.; Watkins, S.P.; Carter, L.J.; Smoot, J.; Gregg, A.C.; Daniels, A.D.; Jervey, S.; et al. Research and Development on Therapeutic Agents and Vaccines for COVID-19 and Related Human Coronavirus Diseases. ACS Cent. Sci. 2020, 6, 315–331. [Google Scholar] [CrossRef]
- Tu, Y.F.; Chien, C.S.; Yarmishyn, A.A.; Lin, Y.Y.; Luo, Y.H.; Lin, Y.T.; Lai, W.Y.; Yang, D.M.; Chou, S.J.; Yang, Y.P.; et al. A Review of SARS-CoV-2 and the Ongoing Clinical Trials. Int. J. Mol. Sci. 2020, 21, 2657. [Google Scholar] [CrossRef]
- Pardi, N.; Hogan, M.J.; Porter, F.W.; Weissman, D. MRNA Vaccines—A New Era in Vaccinology. Nat. Rev. Drug Discov. 2018, 17, 261–279. [Google Scholar] [CrossRef] [PubMed]
- Mulligan, M.J.; Lyke, K.E.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Neuzil, K.; Raabe, V.; Bailey, R.; Swanson, K.A.; et al. Phase I/II Study of COVID-19 RNA Vaccine BNT162b1 in Adults. Nature 2020, 586, 589–593. [Google Scholar] [CrossRef]
- Sheahan, T.P.; Sims, A.C.; Leist, S.R.; Schäfer, A.; Won, J.; Brown, A.J.; Montgomery, S.A.; Hogg, A.; Babusis, D.; Clarke, M.O.; et al. Comparative Therapeutic Efficacy of Remdesivir and Combination Lopinavir, Ritonavir, and Interferon Beta against MERS-CoV. Nat. Commun. 2020, 11, 222. [Google Scholar] [CrossRef] [PubMed]
- Bachmann, M.F.; Jennings, G.T. Vaccine Delivery: A Matter of Size, Geometry, Kinetics and Molecular Patterns. Nat. Rev. Immunol. 2010, 10, 787–796. [Google Scholar] [CrossRef]
- Wang, L.; Shi, W.; Joyce, M.G.; Modjarrad, K.; Zhang, Y.; Leung, K.; Lees, C.R.; Zhou, T.; Yassine, H.M.; Kanekiyo, M.; et al. Evaluation of Candidate Vaccine Approaches for MERS-CoV. Nat. Commun. 2015, 6, 7712. [Google Scholar] [CrossRef] [PubMed]
- Zhang, P.; Chen, Y.; Zeng, Y.; Shen, C.; Li, R.; Guo, Z.; Li, S.; Zheng, Q.; Chu, C.; Wang, Z.; et al. Virus-Mimetic Nanovesicles as a Versatile Antigen-Delivery System. Proc. Natl. Acad. Sci. USA 2015, 112, E6129–E6138. [Google Scholar] [CrossRef] [PubMed]
- Gangadaran, P.; Hong, C.M.; Oh, J.M.; Rajendran, R.L.; Kalimuthu, S.; Son, S.H.; Gopal, A.; Zhu, L.; Baek, S.H.; Jeong, S.Y.; et al. In Vivo Non-Invasive Imaging of Radio-Labeled Exosome-Mimetics Derived From Red Blood Cells in Mice. Front. Pharmacol. 2018, 9, 817. [Google Scholar] [CrossRef] [PubMed]
- Kumar, R.; Mondal, K.; Panda, P.K.; Kaushik, A.; Abolhassani, R.; Ahuja, R.; Rubahn, H.G.; Mishra, Y.K. Core–Shell Nanostructures: Perspectives towards Drug Delivery Applications. J. Mater. Chem. B 2020, 8, 8992–9027. [Google Scholar] [CrossRef]
- Kumar, R.; Dalvi, S.V.; Siril, P.F. Nanoparticle-Based Drugs and Formulations: Current Status and Emerging Applications. ACS Appl. Nano. Mater. 2020, 3, 4944–4961. [Google Scholar] [CrossRef]
- Darnell, M.E.R.; Subbarao, K.; Feinstone, S.M.; Taylor, D.R. Inactivation of the Coronavirus That Induces Severe Acute Respiratory Syndrome, SARS-CoV. J. Virol. Methods 2004, 121, 85–91. [Google Scholar] [CrossRef]
- Chin, A.W.H.; Chu, J.T.S.; Perera, M.R.A.; Hui, K.P.Y.; Yen, H.L.; Chan, M.C.W.; Peiris, M.; Poon, L.L.M. Stability of SARS-CoV-2 in Different Environmental Conditions. Lancet Microbe 2020, 1, e10. [Google Scholar] [CrossRef]
- Orlowski, P.; Tomaszewska, E.; Gniadek, M.; Baska, P.; Nowakowska, J.; Sokolowska, J.; Nowak, Z.; Donten, M.; Celichowski, G.; Grobelny, J.; et al. Tannic Acid Modified Silver Nanoparticles Show Antiviral Activity in Herpes Simplex Virus Type 2 Infection. PLoS ONE 2014, 9, e104113. [Google Scholar] [CrossRef] [PubMed]
- Zodrow, K.; Brunet, L.; Mahendra, S.; Li, D.; Zhang, A.; Li, Q.; Alvarez, P.J.J. Polysulfone Ultrafiltration Membranes Impregnated with Silver Nanoparticles Show Improved Biofouling Resistance and Virus Removal. Water Res. 2009, 43, 715–723. [Google Scholar] [CrossRef]
- Elechiguerra, J.L.; Burt, J.L.; Morones, J.R.; Camacho-Bragado, A.; Gao, X.; Lara, H.H.; Yacaman, M.J. Interaction of Silver Nanoparticles with HIV-1. J. Nanobiotechnology 2005, 3, 6. [Google Scholar] [CrossRef] [PubMed]
- De Gusseme, B.; Sintubin, L.; Baert, L.; Thibo, E.; Hennebel, T.; Vermeulen, G.; Uyttendaele, M.; Verstraete, W.; Boon, N. Biogenic Silver for Disinfection of Water Contaminated with Viruses. Appl. Environ. Microbiol. 2010, 76, 1082–1087. [Google Scholar] [CrossRef] [PubMed]
- Joe, Y.H.; Park, D.H.; Hwang, J. Evaluation of Ag Nanoparticle Coated Air Filter against Aerosolized Virus: Anti-Viral Efficiency with Dust Loading. J. Hazard Mater. 2016, 301, 547–553. [Google Scholar] [CrossRef]
- Warnes, S.L.; Little, Z.R.; Keevil, C.W. Human Coronavirus 229E Remains Infectious on Common Touch Surface Materials. mBio 2015, 6, e01697-15. [Google Scholar] [CrossRef]
- Grass, G.; Rensing, C.; Solioz, M. Metallic Copper as an Antimicrobial Surface. Appl. Environ. Microbiol. 2011, 77, 1541–1547. [Google Scholar] [CrossRef]
- Borkow, G.; Zhou, S.S.; Page, T.; Gabbay, J. A Novel Anti-Influenza Copper Oxide Containing Respiratory Face Mask. PLoS ONE 2010, 5, e11295. [Google Scholar] [CrossRef]
- Tu, Z.; Guday, G.; Adeli, M.; Haag, R. Multivalent Interactions between 2D Nanomaterials and Biointerfaces. Adv. Mater. 2018, 30, e1706709. [Google Scholar] [CrossRef]
- Song, Z.; Wang, X.; Zhu, G.; Nian, Q.; Zhou, H.; Yang, D.; Qin, C.; Tang, R. Virus Capture and Destruction by Label-Free Graphene Oxide for Detection and Disinfection Applications. Small 2014, 11, 1171–1176. [Google Scholar] [CrossRef]
- Singh, R.; Hong, S.; Jang, J. Label-Free Detection of Influenza Viruses Using a Reduced Graphene Oxide-Based Electrochemical Immunosensor Integrated with a Microfluidic Platform. Sci. Rep. 2017, 7, 42771. [Google Scholar] [CrossRef] [PubMed]
- Palmieri, V.; Papi, M. Can Graphene Take Part in the Fight against COVID-19? Nano Today 2020, 33, 100883. [Google Scholar] [CrossRef]
- Spinowitz, B.S.; Kausz, A.T.; Baptista, J.; Noble, S.D.; Sothinathan, R.; Bernardo, M.V.; Brenner, L.; Pereira, B.J.G. Ferumoxytol for Treating Iron Deficiency Anemia in CKD. J. Am. Soc. Nephrol. 2008, 19, 1599. [Google Scholar] [CrossRef] [PubMed]
- Abo-zeid, Y.; Williams, G.R. The Potential Anti-Infective Applications of Metal Oxide Nanoparticles: A Systematic Review. Wiley Interdiscip Rev. Nanomed. Nanobiotechnol. 2020, 12, e1592. [Google Scholar] [CrossRef] [PubMed]
- Ahamed, M.; Alhadlaq, H.A.; Khan, M.A.M.; Akhtar, M.J. Selective Killing of Cancer Cells by Iron Oxide Nanoparticles Mediated through Reactive Oxygen Species via P53 Pathway. J. Nanoparticle Res. 2013, 15, 1225. [Google Scholar] [CrossRef]
- Rab, S.; Javaid, M.; Haleem, A.; Vaishya, R. An Update on the Global Vaccine Development for Coronavirus. Diabetes Metab. Syndr. 2020, 14, 2053. [Google Scholar] [CrossRef]
- Yadavalli, T.; Shukla, D. Role of Metal and Metal Oxide Nanoparticles as Diagnostic and Therapeutic Tools for Highly Prevalent Viral Infections. Nanomedicine 2017, 13, 219–230. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Presentation of Antigen | Nanoparticles as a Delivery System | Vaccine Antigens | Advantages | Disadvantages |
|---|---|---|---|---|
| Antigenic components packed in nanoparticle | Lipid nanoparticle/nano formulation | DNA and mRNA | Completely synthetic Increases stability and regulates transportation of nucleic acid Highly immunogenic Adjuvant not needed Customized for surface charge and lipid components | Need a specialized cold chain for storage Comparatively costly Some myocarditis-type adverse reaction occurs |
| Polymer nanoparticle/nano formulation | Receptor-binding domain (RBD) | Customized for surface charge, shape, and size Targeted delivery of adjuvant and antigen Very effective for intranasal application with the use of mucosal adhesive polymer components | Low loading capability Packaging limits the immune recognition of antigenic protein and slows the immune response | |
| Antigenic components presented in nanoparticle core | Virus-like nanoparticles/nano formulation | Spike (S) protein, membrane (M) protein, envelope (E) protein | Mimic the natural virus Rapid production can be scaled up A large number of viral proteins can be delivered | Needs complicated supportive viruses or sometimes cell lines also Restricted regulation of the viral protein structure and orientations |
| Protein nanoparticles/nano formulation | Spike (S) protein and receptor-binding domain (RBD) | Increased immunogenicity compared with subunit vaccine Customized for surface charge, shape, and size At a time, together display heterologous antigenic components | No scientific data available on scalable formation Need cell line in the production and regulatory endorsement Need formulation along with adjuvant | |
| Micelle nanoparticles/nano formulation | Spike (S) protein | Present a large number of viral proteins in natural viral-like fashion | Very low stability No scientific data available on scalable formation | |
| Liposomes | Spike (S) protein and receptor-binding domain (RBD) | Completely synthetic Customized for surface charge, shape, and size At a time, together present adjuvant and antigen | Half-life and stability can be affected by the associated antigenic components No in vivo stability data available on liposome and antigenic components conjugates |
| Nanoparticles Category | Developed by | Nanoparticle Vaccine Candidate [Registration Number of the Candidate] |
|---|---|---|
| Lipid nanoparticles | Moderna, NIAID | mRNA-1273 (LNPs) [NCT04760132] |
| Pfizer/BioNTech, Fosun Pharma | BNT162b2 (3 LNP-mRNAs [NCT04760132] | |
| Moderna, NIAID | mRNA-1273.351 LNPs [EUCTR2021-000930-32] | |
| CureVac AG | CVnCoV mRNA vaccine [NCT04674189] | |
| Academy of Military Science (AMS), Walvax Biotechnology and Suzhou Abogen Biosciences | SARS-CoV-2 mRNA vaccine (ARCoV) [NCT04847102] | |
| Arcturus Therapeutics | ARCT-021 mRNA vaccine [NCT04668339; NCT04728347] | |
| Sanofi Pasteur and Translate Bio | MRT5500 mRNA vaccine [NCT04798027] | |
| Daiichi Sankyo Co., Ltd. | DS-5670a mRNA vaccine [NCT04821674] | |
| Elixirgen Therapeutics, Inc. | EXG-5003 [NCT04863131] | |
| GlaxoSmithKline | CoV2 SAM LNP [NCT04758962] | |
| Imperial College London | LNP-nCoVsaRNA [ISRCTN17072692] | |
| Providence Therapeutics | PTX-COVID19-B, mRNA vaccine [NCT04765436] | |
| SENAI CIMATEC | HDT-301: self-replicating mRNA-LNP vaccine [NCT04844268] | |
| ModernaTX, Inc. | mRNA-1283, a potentially refrigerator-stable LNP vaccine [NCT04813796] | |
| Chulalongkorn University | ChulaCov19 mRNA vaccine [NCT04566276] | |
| Shanghai East Hospital and Stemirna Therapeutics | mRNA-LNP COVID-19 vaccine [ChiCTR2100045984] | |
| MRC/UVRI and LSHTM Uganda Research Unit | LNP-nCoV saRNA-02 vaccine [NCT04934111] | |
| Virus-like nanoparticles | Medicago Inc. | Coronavirus-like particle (CoVLP) [NCT04636697] |
| The Scientific and Technological Research Council of Turkey | VLP vaccine [NCT04962893] | |
| Serum Institute of India, Accelagen Pty, SpyBiotech | RBD SARS-CoV-2 HBsAg VLP vaccine [ACTRN12620000817943] | |
| VBI Vaccine Inc. | VBI-2902a (Enveloped VLP of S protein) [NCT04773665] | |
| Radboud University | ABNCoV2 capsid VLP (cVLP) [NCT04839146] | |
| Protein nanoparticles | SK Bioscience Co., Ltd. | RBD-I53-50 nanoparticle [NCT05007951] |
| Walter Reed Army Institute of Research (WRAIR) | S protein-ferritin nanoparticle [NCT04784767] | |
| Micelles | Novavax | SARS-CoV-2 rS/Matrix M1-Adjuvant [NCT04611802; EUCTR2020-004123-16-GB; NCT04583995] |
| Vaccine Name | Encoded Antigen | Manufacturer/Developer |
|---|---|---|
| mRNA-1273 | Spike | Moderna |
| BNT162b1/BNT162b2/BNT162b3 | Spike | Pfizer |
| CureVac COVID-19 vaccine (CVnCoV) | Spike | GlaxoSmithKline/CureVac |
| LNP-nCoVsaRNA | Spike | Imperial College London |
| ARCT-021/ARCT-164/ARCT-165 | Spike | Duke-NUS Medical School |
| ARCoV | Receptor-binding domain | AMS/Walvax/Suzhou |
| TAK-919 | Full-length spike protein prefusion stabilized | Takeda/Moderna |
| ChulaCov19 | Full-length spike protein | Chulalongkorn University |
| EG-COVID | Full-length spike protein | Eye-GENE |
| SW-0123 | Full-length spike protein | Stemirna Therapeutics/ Shanghai East Hospital |
| PTXCOVID19B | Full-length spike protein | Providence Therapeutics |
| MRT5500 (VAW00001) | Full-length spike protein 2P modified furin cleavage site | Translate Bio/Sanofi |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Prabhakar, P.K.; Khurana, N.; Vyas, M.; Sharma, V.; Batiha, G.E.-S.; Kaur, H.; Singh, J.; Kumar, D.; Sharma, N.; Kaushik, A.; et al. Aspects of Nanotechnology for COVID-19 Vaccine Development and Its Delivery Applications. Pharmaceutics 2023, 15, 451. https://doi.org/10.3390/pharmaceutics15020451
Prabhakar PK, Khurana N, Vyas M, Sharma V, Batiha GE-S, Kaur H, Singh J, Kumar D, Sharma N, Kaushik A, et al. Aspects of Nanotechnology for COVID-19 Vaccine Development and Its Delivery Applications. Pharmaceutics. 2023; 15(2):451. https://doi.org/10.3390/pharmaceutics15020451
Chicago/Turabian StylePrabhakar, Pranav Kumar, Navneet Khurana, Manish Vyas, Vikas Sharma, Gaber El-Saber Batiha, Harpreet Kaur, Jashanpreet Singh, Deepak Kumar, Neha Sharma, Ajeet Kaushik, and et al. 2023. "Aspects of Nanotechnology for COVID-19 Vaccine Development and Its Delivery Applications" Pharmaceutics 15, no. 2: 451. https://doi.org/10.3390/pharmaceutics15020451
APA StylePrabhakar, P. K., Khurana, N., Vyas, M., Sharma, V., Batiha, G. E.-S., Kaur, H., Singh, J., Kumar, D., Sharma, N., Kaushik, A., & Kumar, R. (2023). Aspects of Nanotechnology for COVID-19 Vaccine Development and Its Delivery Applications. Pharmaceutics, 15(2), 451. https://doi.org/10.3390/pharmaceutics15020451