
Fabrication and Characterisation of 3D-Printed Triamcinolone Acetonide-Loaded Polycaprolactone-Based Ocular Implants

 ,
,  , ,
, ,  and
and
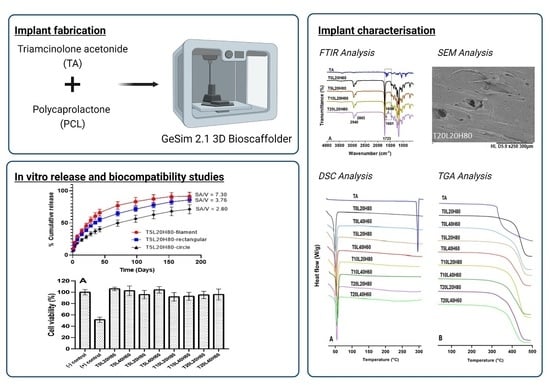
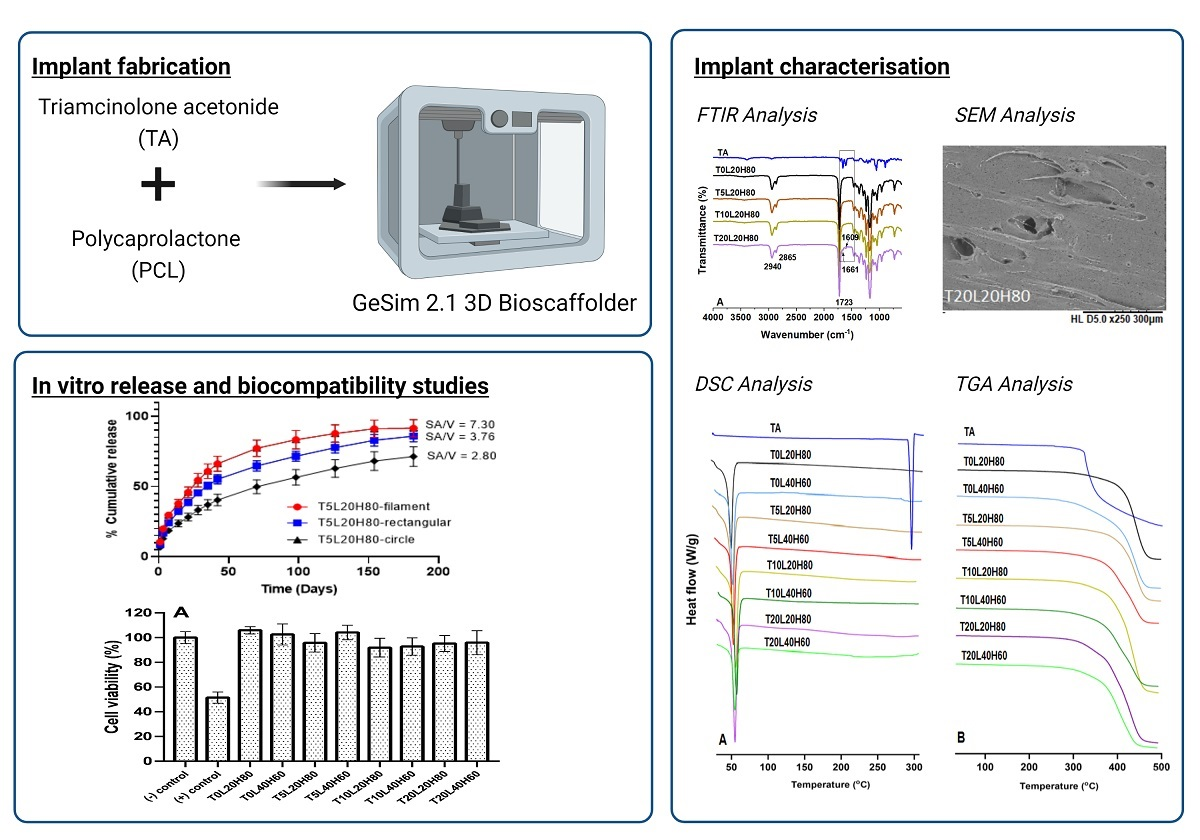
Abstract
1. Introduction
2. Materials and Methods
2.1. Materials
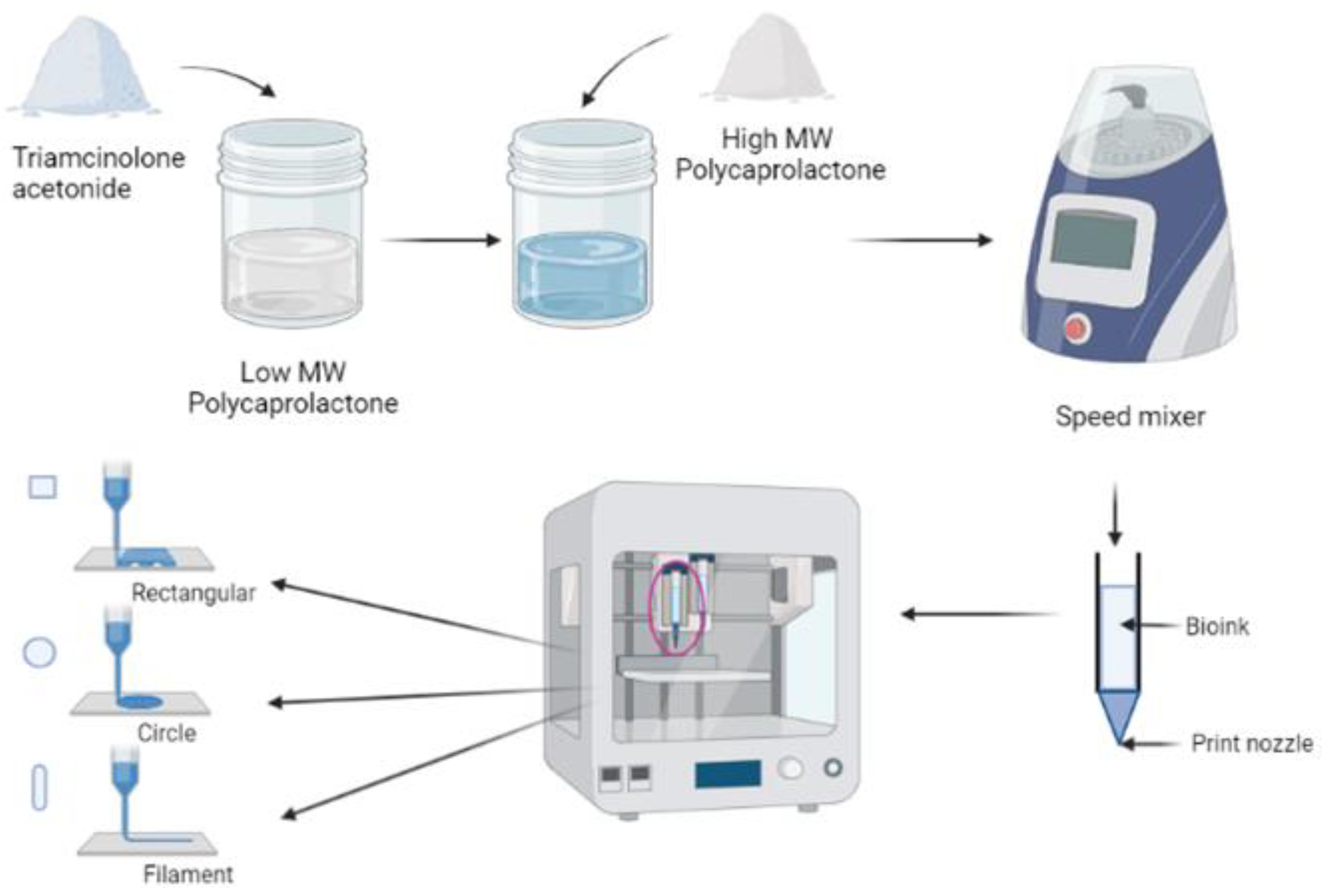
2.2. Fabrication of TA-Loaded PCL Implants
2.3. Characterisation of TA-Loaded PCL Implants
2.4. Scaffold Dimensions Characterisation
2.5. Drug Content Analysis
2.6. In Vitro Drug Release Study
2.7. Implants Degradation
2.8. In Vitro Biocompatibility Study
2.8.1. Cell Culture
2.8.2. Cell Passage
2.8.3. Sample Preparation
2.8.4. Cell Viability Assay
2.9. Statistical Analysis
3. Results and Discussion
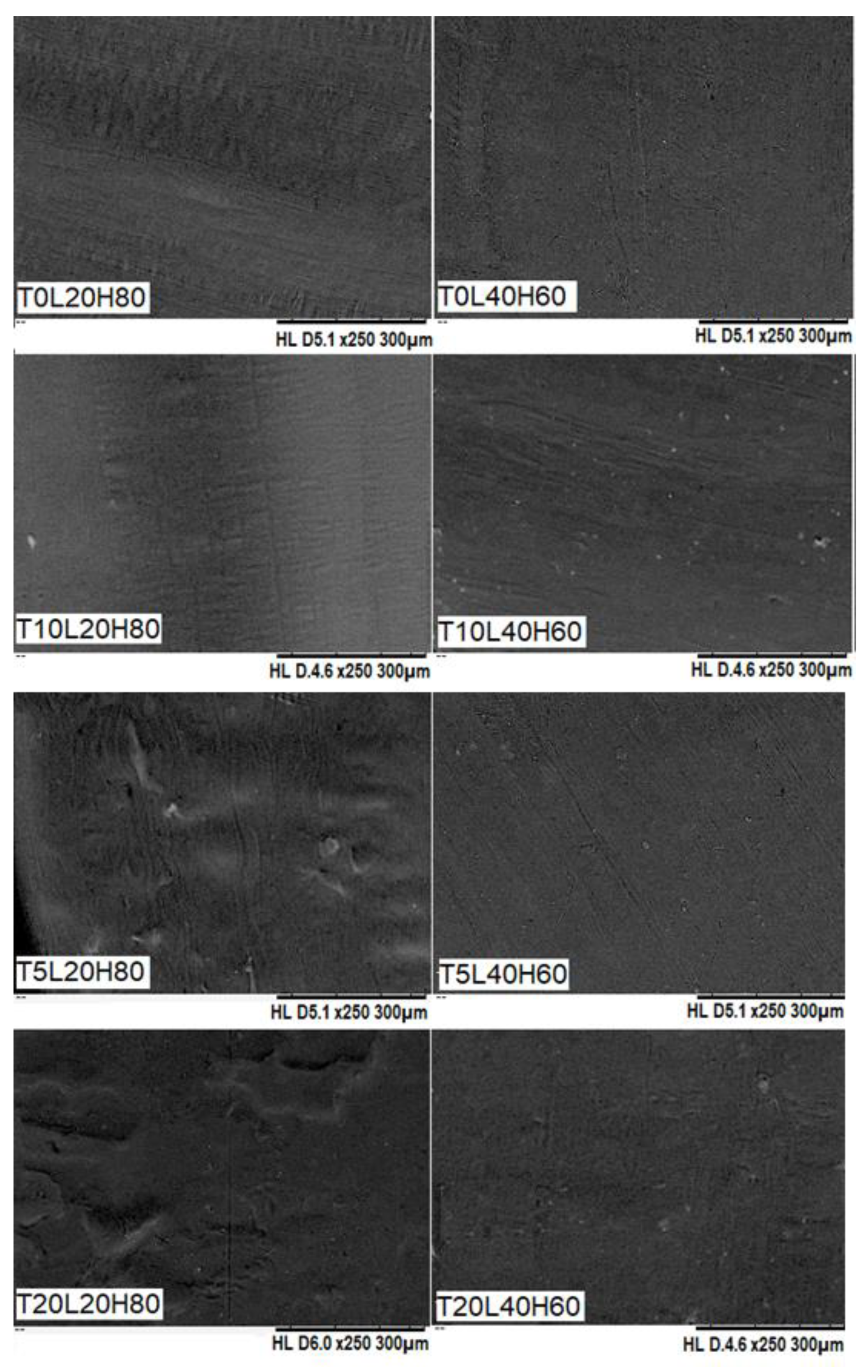
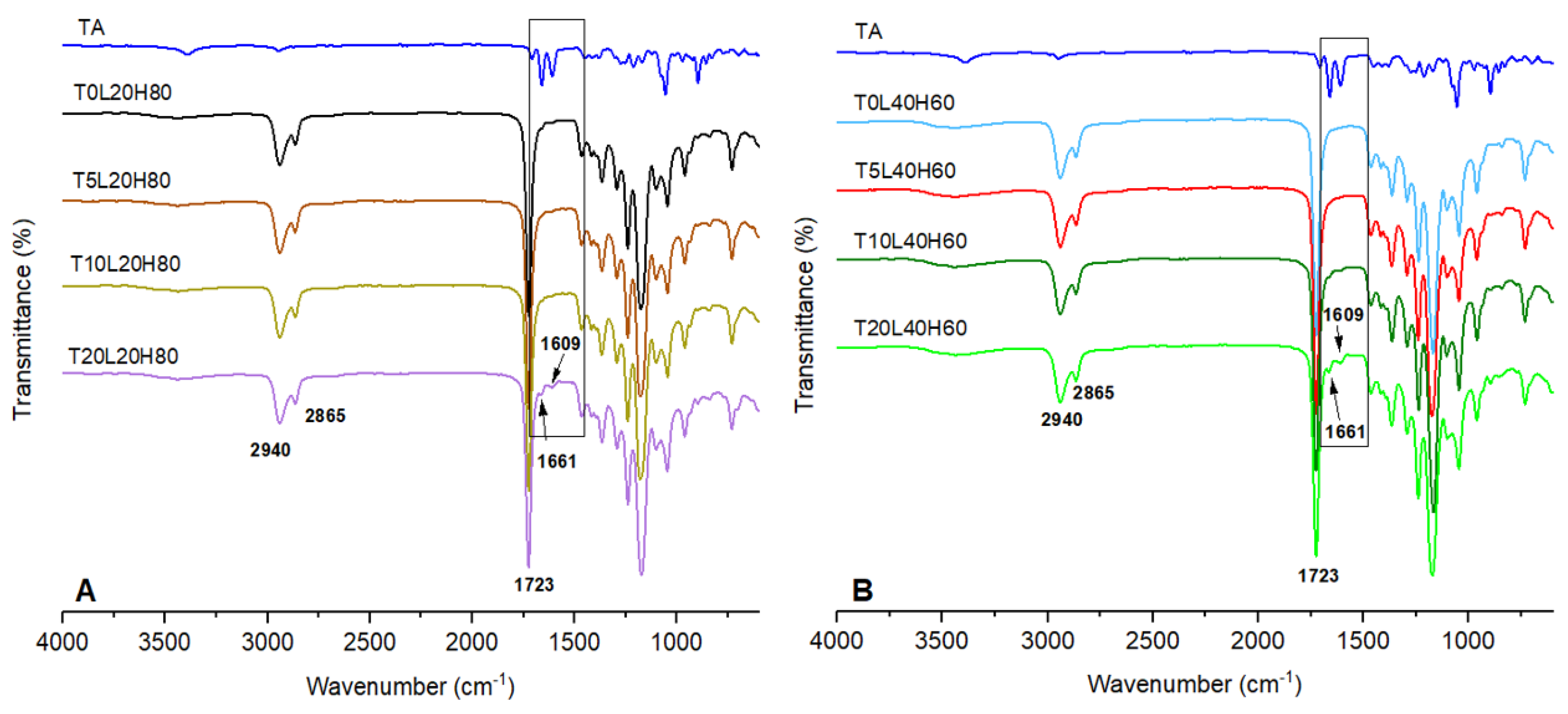
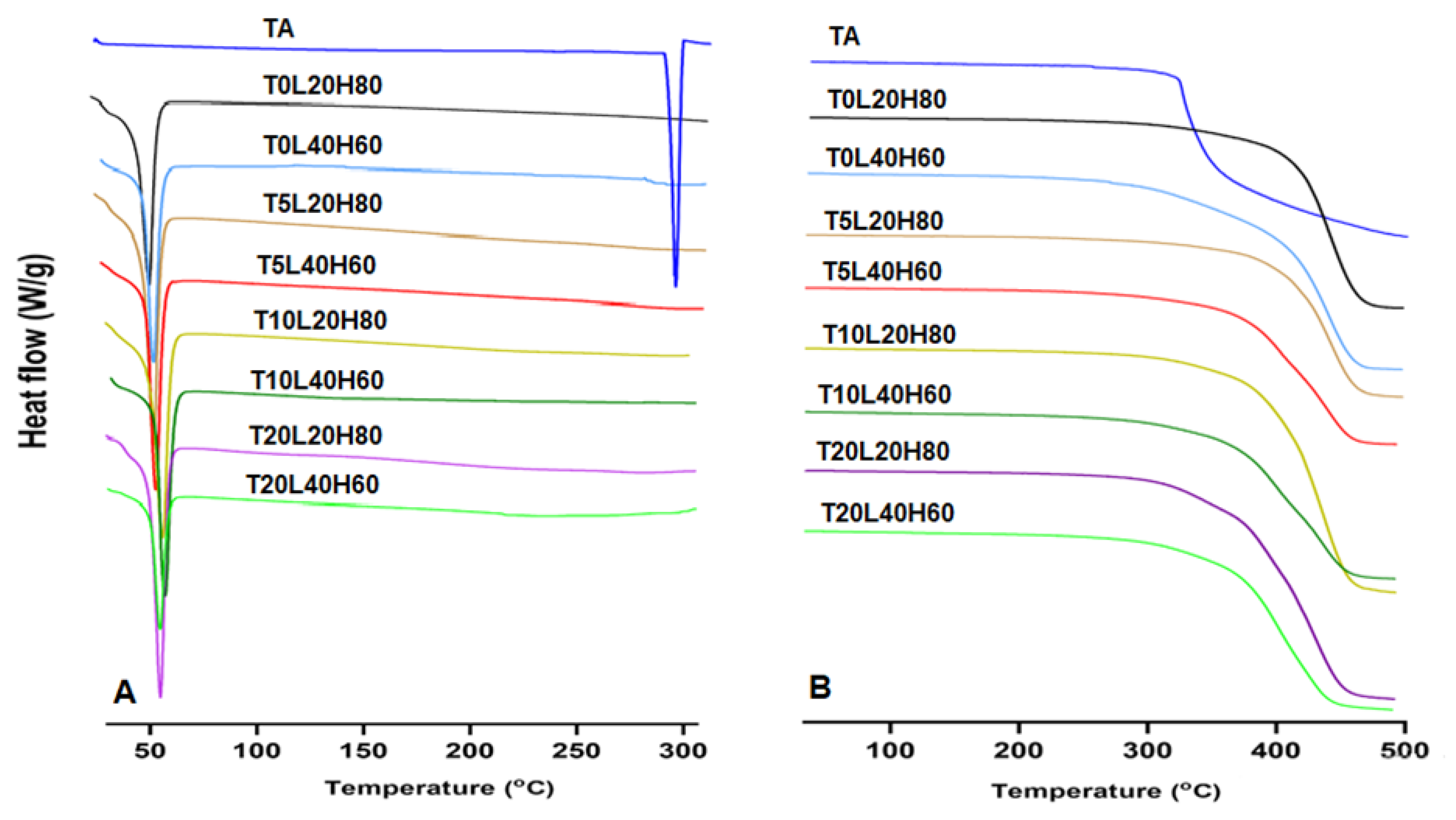
3.1. Fabrication and Characterisation of TA-Loaded PCL Implants
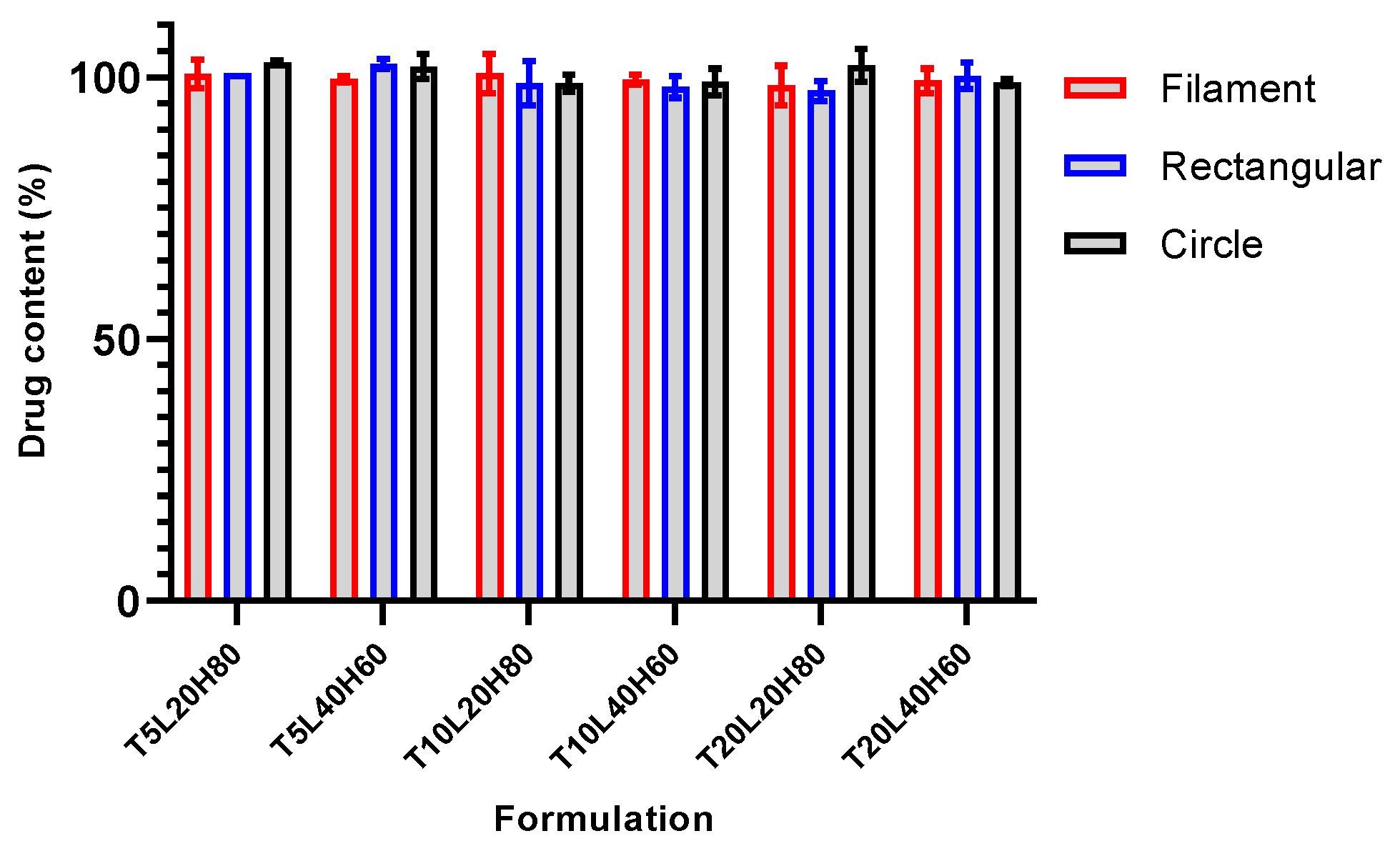
3.2. TA Content Analysis
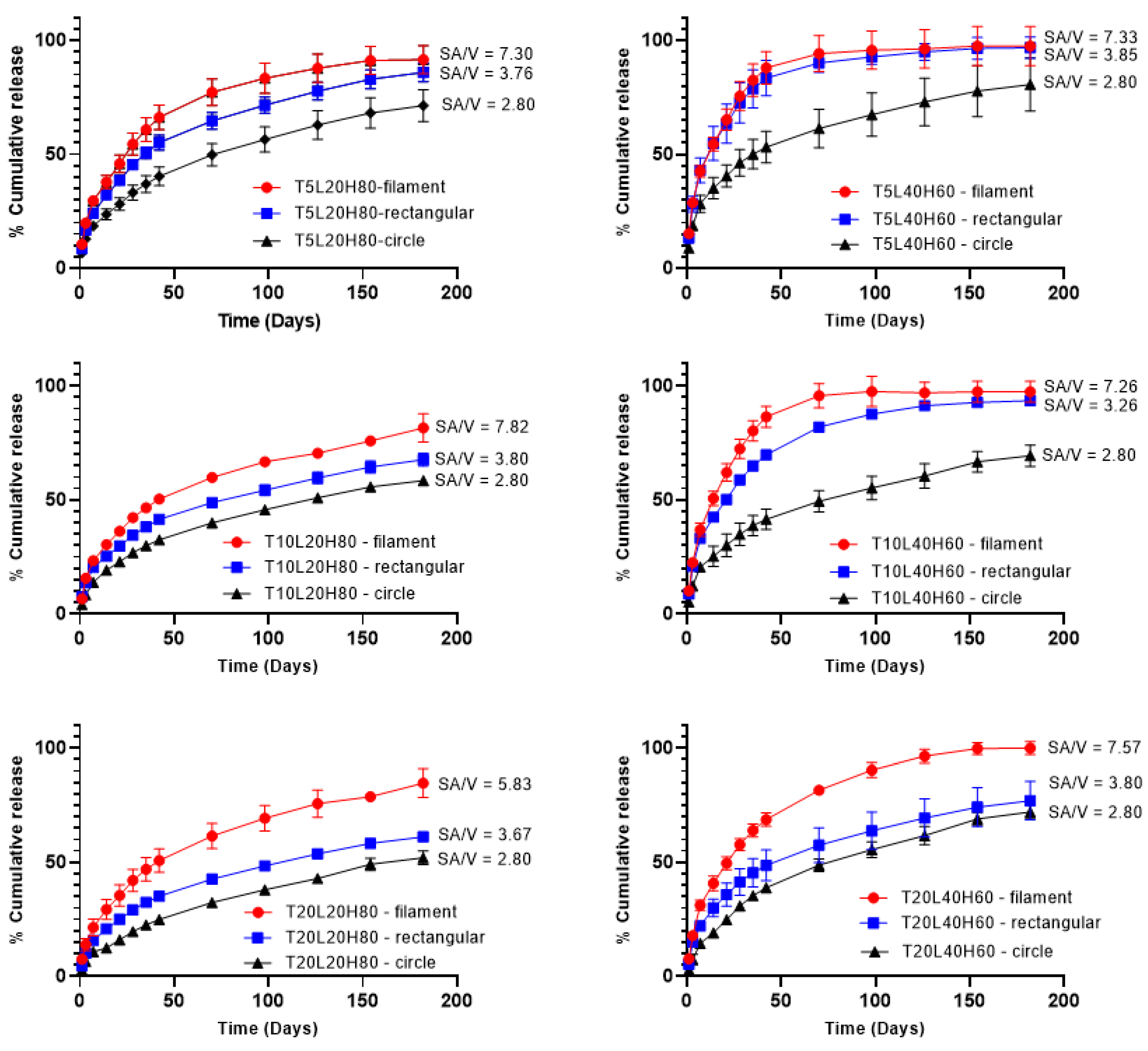
3.3. In Vitro Release Study
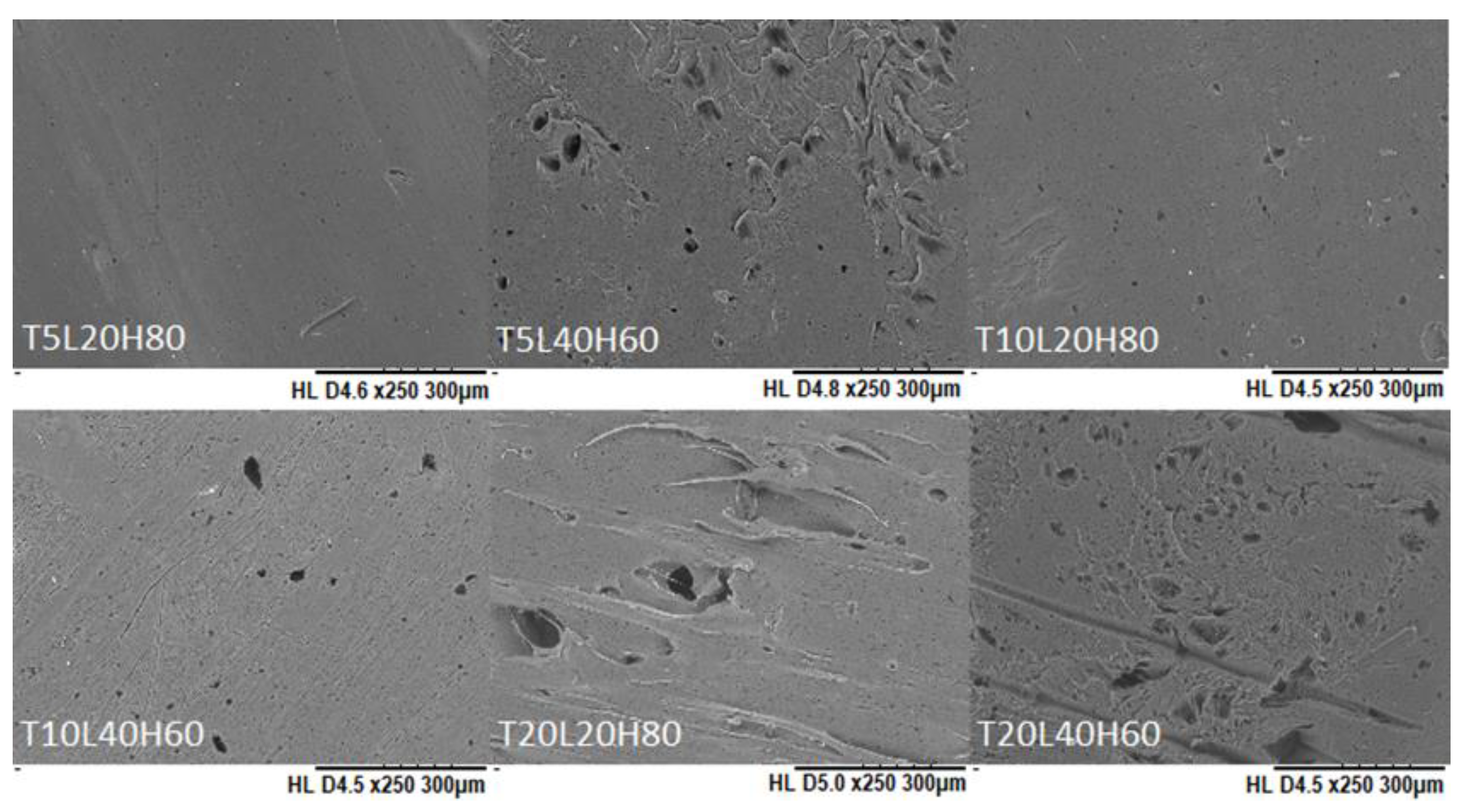
3.4. Implant Degradation
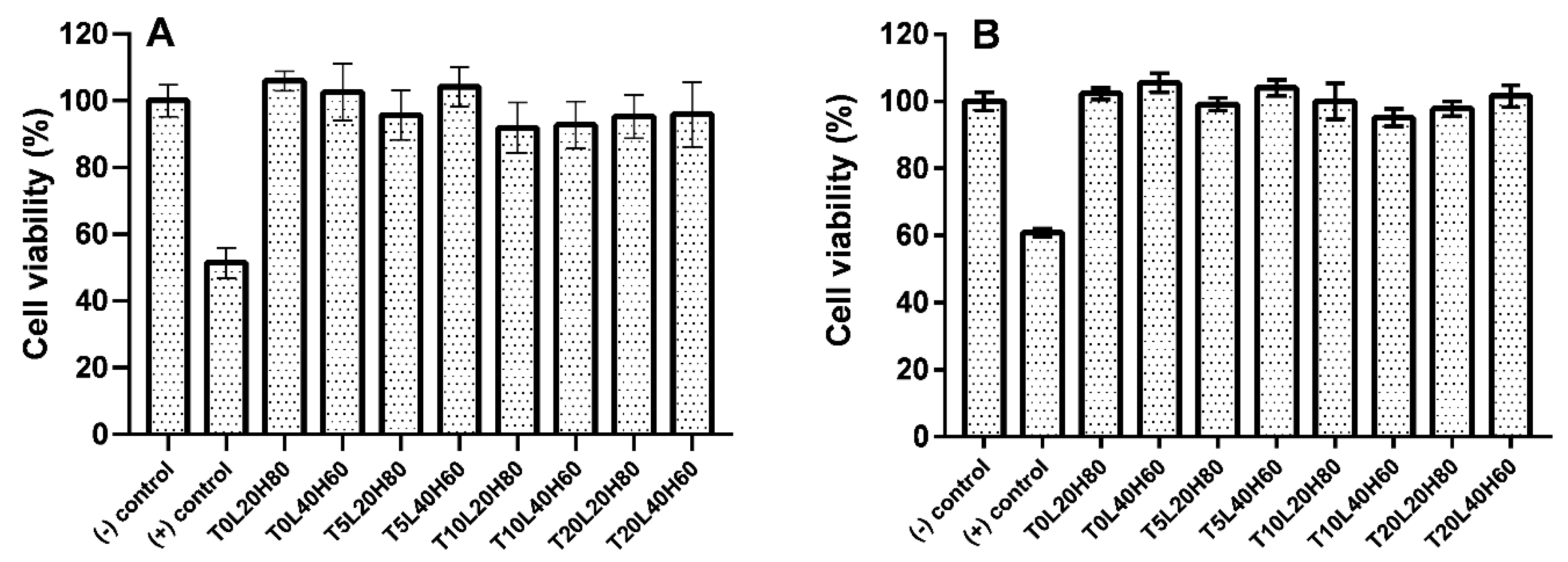
3.5. Biocompatibility Study
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. World Report on Vision; WHO: Geneva, Switzerland, 2019. [Google Scholar]
- Souto, E.B.; Dias-Ferreira, J.; López-Machado, A.; Ettcheto, M.; Cano, A.; Espuny, A.C.; Espina, M.; Garcia, M.L.; Sánchez-López, E. Advanced Formulation Approaches for Ocular Drug Delivery: State-Of-The-Art and Recent Patents. Pharmaceutics 2019, 11, 460. [Google Scholar] [CrossRef]
- Geroski, D.H.; Edelhauser, H.F. Drug delivery for posterior segment eye disease. Investig. Ophthalmol. Vis. Sci. 2000, 41, 961–964. [Google Scholar]
- Cooper, R.C.; Yang, H. Hydrogel-based ocular drug delivery systems: Emerging fabrication strategies, applications, and bench-to-bedside manufacturing considerations. J. Control. Release 2019, 306, 29–39. [Google Scholar] [CrossRef]
- Hughes, P.M.; Olejnik, O.; Chang-Lin, J.-E.; Wilson, C.G. Topical and systemic drug delivery to the posterior segments. Adv. Drug Deliv. Rev. 2005, 57, 2010–2032. [Google Scholar] [CrossRef]
- Pinto, F.C.H.; Junior, D.S.C.; Oréfice, R.L.; Ayres, E.; Andrade, S.P.; Lima, L.D.C.; Lima Moura, S.A.; Da Silva, G.R. Controlled release of triamcinolone acetonide from polyurethane implantable devices: Application for inhibition of inflammatoryangiogenesis. J. Mater. Sci. Mater. Med. 2012, 23, 1431–1445. [Google Scholar] [CrossRef]
- Chen, H.; Sun, S.; Li, J.; Du, W.; Zhao, C.; Hou, J.; Xu, Y.; Cheng, L. Different Intravitreal Properties of Three Triamcinolone Formulations and Their Possible Impact on Retina Practice. Investig. Opthalmol. Vis. Sci. 2013, 54, 2178–2185. [Google Scholar] [CrossRef]
- Couch, S.S. Intravitreal triamcinolone for intraocular inflammation and associated macular edema. Clin. Ophthalmol. 2008, 3, 41–47. [Google Scholar] [CrossRef]
- Roesel, M.; Gutfleisch, M.; Heinz, C.; Heimes, B.; Zurek-Imhoff, B.; Heiligenhaus, A. Orbital floor triamcinolone acetonide injections for the management of active non-infectious uveitis. Eye 2008, 23, 910–914. [Google Scholar] [CrossRef]
- Ren, Y.; Du, S.; Zheng, D.; Shi, Y.; Pan, L.; Yan, H. Intraoperative intravitreal triamcinolone acetonide injection for prevention of postoperative inflammation and complications after phacoemulsification in patients with uveitic cataract. BMC Ophthalmol. 2021, 21, 245. [Google Scholar] [CrossRef]
- Huang, X.; Chau, Y. Intravitreal nanoparticles for retinal delivery. Drug Discov. Today 2019, 24, 1510–1523. [Google Scholar] [CrossRef]
- Lee, S.S.; Hughes, P.; Ross, A.D.; Robinson, M.R. Biodegradable Implants for Sustained Drug Release in the Eye. Pharm. Res. 2010, 27, 2043–2053. [Google Scholar] [CrossRef] [PubMed]
- Larrañeta, E.; Raj Singh, T.R.; Donnelly, R.F. Long-Acting Drug Delivery Systems Pharmaceutical, Clinical, and Regulatory Aspects, 1st ed.; Elsevier: Amsterdam, The Netherlands, 2021; 392p. [Google Scholar]
- Quarterman, J.C.; Geary, S.M.; Salem, A.K. Evolution of drug-eluting biomedical implants for sustained drug delivery. Eur. J. Pharm. Biopharm. 2021, 159, 21–35. [Google Scholar] [CrossRef]
- Del Amo, E.M.; Urtti, A. Current and future ophthalmic drug delivery systems: A shift to the posterior segment. Drug Discov. Today 2008, 13, 135–143. [Google Scholar] [CrossRef] [PubMed]
- Malavia, N.; Kaiser, P.K. Overview of sustained-release drug-delivery systems. Retina Today 2015, 67–69. [Google Scholar]
- Adrianto, M.F.; Annuryanti, F.; Wilson, C.G.; Sheshala, R.; Thakur, R.R.S. In vitro dissolution testing models of ocular implants for posterior segment drug delivery. Drug Deliv. Transl. Res. 2021, 12, 1355–1375. [Google Scholar] [CrossRef] [PubMed]
- Woodruff, M.A.; Hutmacher, D.W. The return of a forgotten polymer—Polycaprolactone in the 21st century. Prog. Polym. Sci. 2010, 35, 1217–1256. [Google Scholar] [CrossRef]
- Muwaffak, Z.; Goyanes, A.; Clark, V.; Basit, A.W.; Hilton, S.T.; Gaisford, S. Patient-specific 3D scanned and 3D printed antimicrobial polycaprolactone wound dressings. Int. J. Pharm. 2017, 527, 161–170. [Google Scholar] [CrossRef]
- Nyitray, C.E.; Chang, R.; Faleo, G.; Lance, K.D.; Bernards, D.A.; Tang, Q.; Desai, T.A. Polycaprolactone Thin-Film Micro- and Nanoporous Cell-Encapsulation Devices. ACS Nano 2015, 9, 5675–5682. [Google Scholar] [CrossRef] [PubMed]
- Castilla-Cortázar, I.; Más-Estellés, J.; Meseguer-Dueñas, J.M.; Ivirico, J.E.; Marí, B.; Vidaurre, A. Hydrolytic and enzymatic degradation of a poly(ε-caprolactone) network. Polym. Degrad. Stab. 2012, 97, 1241–1248. [Google Scholar] [CrossRef]
- Abedalwafa, M.; Wang, F.; Wang, L.; Li, C. Biodegradable poly-epsilon-caprolactone (PCL) for tissue engineering applications: A review. Rev. Adv. Mater. Sci. 2013, 34, 123–140. [Google Scholar]
- Kim, J.; Kudisch, M.; Mudumba, S.; Asada, H.; Aya-Shibuya, E.; Bhisitkul, R.B.; Desai, T.A. Biocompatibility and Pharmacokinetic Analysis of an Intracameral Polycaprolactone Drug Delivery Implant for Glaucoma. Investig. Opthalmol. Vis. Sci. 2016, 57, 4341–4346. [Google Scholar] [CrossRef]
- Kim, J.; Kudisch, M.; da Silva, N.R.K.; Asada, H.; Aya-Shibuya, E.; Bloomer, M.M.; Mudumba, S.; Bhisitkul, R.B.; Desai, T.A. Long-term intraocular pressure reduction with intracameral polycaprolactone glaucoma devices that deliver a novel anti-glaucoma agent. J. Control. Release 2017, 269, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Sun, S.; Li, J.; Li, X.; Lan, B.; Zhou, S.; Meng, Y.; Cheng, L. Episcleral drug film for better-targeted ocular drug delivery and controlled release using multilayered poly-ϵ-caprolactone (PCL). Acta Biomater. 2016, 37, 143–154. [Google Scholar] [CrossRef] [PubMed]
- Meng, Y.; Sun, S.; Li, J.; Nan, K.; Lan, B.; Jin, Y.; Chen, H.; Cheng, L. Sustained release of triamcinolone acetonide from an episcleral plaque of multilayered poly-ε-caprolactone matrix. Acta Biomater. 2014, 10, 126–133. [Google Scholar] [CrossRef]
- Beeley, N.R.F.; Rossi, J.V.; Mello-Filho, P.A.A.; Mahmoud, M.I.; Fujii, G.Y.; De Juan, E., Jr.; Varner, S.E. Fabrication, implantation, elution, and retrieval of a steroid-loaded polycaprolactone subretinal implant. J. Biomed. Mater. Res. Part A 2005, 73A, 437–444. [Google Scholar] [CrossRef] [PubMed]
- Korelidou, A.; Domínguez-Robles, J.; Magill, E.R.; Eleftheriadou, M.; Cornelius, V.A.; Donnelly, R.F.; Margariti, A.; Larrañeta, E. 3D-printed reservoir-type implants containing poly(lactic acid)/poly(caprolactone) porous membranes for sustained drug delivery. Biomater. Adv. 2022, 139, 213024. [Google Scholar] [CrossRef]
- Utomo, E.; Domínguez-Robles, J.; Moreno-Castellanos, N.; Stewart, S.A.; Picco, C.J.; Anjani, Q.K.; Simón, J.A.; Peñuelas, I.; Donnelly, R.F.; Larraneta, E. Development of intranasal implantable devices for schizophrenia treatment. Int. J. Pharm. 2022, 624, 122061. [Google Scholar] [CrossRef]
- PPicco, C.J.; Domínguez-Robles, J.; Utomo, E.; Paredes, A.J.; Volpe-Zanutto, F.; Malinova, D.; Donnelly, R.F.; Larrañeta, E. 3D-printed implantable devices with biodegradable rate-controlling membrane for sustained delivery of hydrophobic drugs. Drug Deliv. 2022, 29, 1038–1048. [Google Scholar] [CrossRef]
- Domínguez-Robles, J.; Shen, T.; Cornelius, V.A.; Corduas, F.; Mancuso, E.; Donnelly, R.F.; Margariti, A.; Lamprou, D.A.; Larrañeta, E. Development of drug loaded cardiovascular prosthesis for thrombosis prevention using 3D printing. Mater. Sci. Eng. C 2021, 129, 112375. [Google Scholar] [CrossRef]
- Domínguez-Robles, J.; Utomo, E.; Cornelius, V.A.; Anjani, Q.K.; Korelidou, A.; Gonzalez, Z.; Donnelly, R.F.; Margariti, A.; Delgado-Aguilar, M.; Tarrés, Q.; et al. TPU-based antiplatelet cardiovascular prostheses prepared using fused deposition modelling. Mater. Des. 2022, 220, 110837. [Google Scholar] [CrossRef]
- Domínguez-Robles, J.; Diaz-Gomez, L.; Utomo, E.; Shen, T.; Picco, C.J.; Alvarez-Lorenzo, C.; Concheiro, A.; Donnelly, R.F.; Larrañeta, E. Use of 3D Printing for the Development of Biodegradable Antiplatelet Materials for Cardiovascular Applications. Pharmaceuticals 2021, 14, 921. [Google Scholar] [CrossRef] [PubMed]
- Stewart, S.A.; Domínguez-Robles, J.; Utomo, E.; Picco, C.J.; Corduas, F.; Mancuso, E.; Amir, M.N.; Bahar, M.A.; Sumarheni, S.; Donnelly, R.F.; et al. Poly(caprolactone)-based subcutaneous implant for sustained delivery of levothyroxine. Int. J. Pharm. 2021, 607, 121011. [Google Scholar] [CrossRef] [PubMed]
- Bosworth, L.A.; Downes, S. Physicochemical characterisation of degrading polycaprolactone scaffolds. Polym. Degrad. Stab. 2010, 95, 2269–2276. [Google Scholar] [CrossRef]
- Sun, M.; Downes, S. Physicochemical characterisation of novel ultra-thin biodegradable scaffolds for peripheral nerve repair. J. Mater. Sci. Mater. Med. 2009, 20, 1181–1192. [Google Scholar] [CrossRef]
- Lam, C.X.F.; Savalani, M.M.; Teoh, S.-H.; Hutmacher, D.W. Dynamics of in vitro polymer degradation of polycaprolactone-based scaffolds: Accelerated versus simulated physiological conditions. Biomed. Mater. 2008, 3, 034108. [Google Scholar] [CrossRef] [PubMed]
- Zehnder, T.; Freund, T.; Demir, M.; Detsch, R.; Boccaccini, A.R. Fabrication of Cell-Loaded Two-Phase 3D Constructs for Tissue Engineering. Materials 2016, 9, 887. [Google Scholar] [CrossRef]
- Dumpa, N.R.; Bandari, S.; Repka, M.A. Novel Gastroretentive Floating Pulsatile Drug Delivery System Produced via Hot-Melt Extrusion and Fused Deposition Modeling 3D Printing. Pharmaceutics 2020, 12, 52. [Google Scholar] [CrossRef]
- Mathew, E.; Domínguez-Robles, J.; Stewart, S.A.; Mancuso, E.; O’Donnell, K.; Larrañeta, E.; Lamprou, D.A. Fused Deposition Modeling as an Effective Tool for Anti-Infective Dialysis Catheter Fabrication. ACS Biomater. Sci. Eng. 2019, 5, 6300–6310. [Google Scholar] [CrossRef]
- Stewart, S.A.; Domínguez-Robles, J.; McIlorum, V.J.; Mancuso, E.; Lamprou, D.A.; Donnelly, R.F.; Larrañeta, E. Development of a Biodegradable Subcutaneous Implant for Prolonged Drug Delivery Using 3D Printing. Pharmaceutics 2020, 12, 105. [Google Scholar] [CrossRef]
- Seoane-Viaño, I.; Trenfield, S.J.; Basit, A.W.; Goyanes, A. Translating 3D printed pharmaceuticals: From hype to real-world clinical applications. Adv. Drug Deliv. Rev. 2021, 174, 553–575. [Google Scholar] [CrossRef]
- Vivero-Lopez, M.; Xu, X.; Muras, A.; Otero, A.; Concheiro, A.; Gaisford, S.; Basit, A.W.; Alvarez-Lorenzo, C.; Goyanes, A. Anti-biofilm multi drug-loaded 3D printed hearing aids. Mater. Sci. Eng. C 2020, 119, 111606. [Google Scholar] [CrossRef]
- Seoane-Viaño, I.; Ong, J.J.; Luzardo-Álvarez, A.; González-Barcia, M.; Basit, A.W.; Otero-Espinar, F.J.; Goyanes, A. 3D printed tacrolimus suppositories for the treatment of ulcerative colitis. Asian J. Pharm. Sci. 2020, 16, 110–119. [Google Scholar] [CrossRef]
- Farmer, Z.-L.; Utomo, E.; Domínguez-Robles, J.; Mancinelli, C.; Mathew, E.; Larrañeta, E.; Lamprou, D.A. 3D printed estradiol-eluting urogynecological mesh implants: Influence of material and mesh geometry on their mechanical properties. Int. J. Pharm. 2020, 593, 120145. [Google Scholar] [CrossRef]
- Afsana; Jain, V.; Haider, N.; Jain, K. 3D Printing in Personalized Drug Delivery. Curr. Pharm. Des. 2019, 24, 5062–5071. [Google Scholar] [CrossRef]
- Ritger, P.L.; Peppas, N.A. A simple equation for description of solute release I. Fickian and non-fickian release from non-swellable devices in the form of slabs, spheres, cylinders or discs. J. Control. Release 1987, 5, 23–36. [Google Scholar] [CrossRef]
- Larrañeta, E.; Martínez-Ohárriz, C.; Vélaz, I.; Zornoza, A.; Machín, R.; Isasi, J.R. In Vitro Release from Reverse Poloxamine/α-Cyclodextrin Matrices: Modelling and Comparison of Dissolution Profiles. J. Pharm. Sci. 2014, 103, 197–206. [Google Scholar] [CrossRef]
- Costa, P.; Lobo, J.M.S. Modeling and comparison of dissolution profiles. Eur. J. Pharm. Sci. 2001, 13, 123–133. [Google Scholar] [CrossRef]
- Munj, H.R.; Lannutti, J.J.; Tomasko, D.L. Understanding drug release from PCL/gelatin electrospun blends. J. Biomater. Appl. 2017, 31, 933–949. [Google Scholar] [CrossRef]
- Liaskoni, A.; Wildman, R.D.; Roberts, C.J. 3D printed polymeric drug-eluting implants. Int. J. Pharm. 2021, 597, 120330. [Google Scholar] [CrossRef]
- García-Millán, E.; Quintáns-Carballo, M.; Otero-Espinar, F.J. Solid-state characterization of triamcinolone acetonide nanosuspensiones by X-ray spectroscopy, ATR Fourier transforms infrared spectroscopy and differential scanning calorimetry analysis. Data Brief 2017, 15, 133–137. [Google Scholar] [CrossRef]
- Elzein, T.; Nasser-Eddine, M.; Delaite, C.; Bistac, S.; Dumas, P. FTIR study of polycaprolactone chain organization at interfaces. J. Colloid Interface Sci. 2004, 273, 381–387. [Google Scholar] [CrossRef]
- Stewart, S.A.; Domínguez-Robles, J.; McIlorum, V.J.; Gonzalez, Z.; Utomo, E.; Mancuso, E.; Lamprou, D.A.; Donnelly, R.F.; Larrañeta, E. Poly(caprolactone)-Based Coatings on 3D-Printed Biodegradable Implants: A Novel Strategy to Prolong Delivery of Hydrophilic Drugs. Mol. Pharm. 2020, 17, 3487–3500. [Google Scholar] [CrossRef]
- Kmiec, E.B.; Borjigin, M.; Eskridge, C.; Niamat, R.; Strouse, B.; Bialk, P. Electrospun fiber membranes enable proliferation of genetically modified cells. Int. J. Nanomed. 2013, 8, 855–864. [Google Scholar] [CrossRef]
- Mashak, A.; Mobedi, H.; Mahdavi, H. A Comparative Study of Progesterone and Lidocaine Hydrochloride Release from Poly(L-lactide) Films. Pharm. Sci. 2015, 21, 77–85. [Google Scholar] [CrossRef]
- Long, J.; Nand, A.V.; Ray, S.; Mayhew, S.; White, D.; Bunt, C.R.; Seyfoddin, A. Development of customised 3D printed biodegradable projectile for administrating extended-release contraceptive to wildlife. Int. J. Pharm. 2018, 548, 349–356. [Google Scholar] [CrossRef]
- Nand, A.V.; Ray, S.; Travas-Sejdic, J.; Kilmartin, P.A. Characterization of polyethylene terephthalate/polyaniline blends as potential antioxidant materials. Mater. Chem. Phys. 2012, 134, 443–450. [Google Scholar] [CrossRef]
- Boubriak, O.; Urban, J.; Akhtar, S.; Meek, K.; Bron, A. The Effect of Hydration and Matrix Composition on Solute Diffusion in Rabbit Sclera. Exp. Eye Res. 2000, 71, 503–514. [Google Scholar] [CrossRef]
- Kompella, U.B.; Bandi, N.; Ayalasomayajula, S. Subconjunctival Nano- and Microparticles Sustain Retinal Delivery of Budesonide, a Corticosteroid Capable of Inhibiting VEGF Expression. Investig. Opthalmol. Vis. Sci. 2003, 44, 1192–1201. [Google Scholar] [CrossRef]
- Isyar, M.; Yilmaz, I.; Nusran, G.; Guler, O.; Yalcin, S.; Mahirogullari, M. Safety of bioabsorbable implants in vitro. BMC Surg. 2015, 15, 127. [Google Scholar] [CrossRef]
- Stewart, S.A.; Waite, D.; Domínguez-Robles, J.; McAlister, E.; Permana, A.D.; Donnelly, R.F.; Larrañeta, E. HPLC method for levothyroxine quantification in long-acting drug delivery systems. Validation and evaluation of bovine serum albumin as levothyroxine stabilizer. J. Pharm. Biomed. Anal. 2021, 203, 114182. [Google Scholar] [CrossRef]
- Reddy, M.S.; Sindoori, K. Formulation development and evaluation of triamcinolone acetonide intramuscular in-situ nano suspension. Int. J. Pharm. Biol. Sci. 2018, 8, 344–351. [Google Scholar]
- Reynolds, T.D.; Mitchell, S.A.; Balwinski, K.M. Investigation of the Effect of Tablet Surface Area/Volume on Drug Release from Hydroxypropylmethylcellulose Controlled-Release Matrix Tablets. Drug Dev. Ind. Pharm. 2002, 28, 457–466. [Google Scholar] [CrossRef]
- Goyanes, A.; Robles Martinez, P.; Buanz, A.; Basit, A.W.; Gaisford, S. Effect of geometry on drug release from 3D printed tablets. Int. J. Pharm. 2015, 494, 657–663. [Google Scholar] [CrossRef]
- Kamath, S.M.; Sridhar, K.; Jaison, D.; Gopinath, V.; Ibrahim, B.K.M.; Gupta, N.; Sundaram, A.; Sivaperumal, P.; Padmapriya, S.; Patil, S.S. Fabrication of tri-layered electrospun polycaprolactone mats with improved sustained drug release profile. Sci. Rep. 2020, 10, 18179. [Google Scholar] [CrossRef]
- Rychter, M.; Baranowska-Korczyc, A.; Milanowski, B.; Jarek, M.; Maciejewska, B.M.; Coy, E.L.; Lulek, J. Cilostazol-Loaded Poly(ε-Caprolactone) Electrospun Drug Delivery System for Cardiovascular Applications. Pharm. Res. 2018, 35, 32. [Google Scholar] [CrossRef]
- Li, N.-N.; Fu, C.-P.; Zhang, L.-M. Using casein and oxidized hyaluronic acid to form biocompatible composite hydrogels for controlled drug release. Mater. Sci. Eng. C 2014, 36, 287–293. [Google Scholar] [CrossRef]
- Lao, L.L.; Venkatraman, S.S.; Peppas, N.A. Modeling of drug release from biodegradable polymer blends. Eur. J. Pharm. Biopharm. 2008, 70, 796–803. [Google Scholar] [CrossRef]
- Kim, K.; Yu, M.; Zong, X.; Chiu, J.; Fang, D.; Seo, Y.-S.; Hsiao, B.S.; Chu, B.; Hadjiargyrou, M. Control of degradation rate and hydrophilicity in electrospun non-woven poly(d,l-lactide) nanofiber scaffolds for biomedical applications. Biomaterials 2003, 24, 4977–4985. [Google Scholar] [CrossRef]
- Chen, V.J.; Ma, P.X. The effect of surface area on the degradation rate of nano-fibrous poly(l-lactic acid) foams. Biomaterials 2006, 27, 3708–3715. [Google Scholar] [CrossRef]
- Bölgen, N.; Menceloǧlu, Y.Z.; Acatay, K.; Vargel, I.; Pişkin, E. In vitro and in vivo degradation of non-woven materials made of poly(ε-caprolactone) nanofibers prepared by electrospinning under different conditions. J. Biomater. Sci. Polym. Ed. 2005, 16, 1537–1555. [Google Scholar] [CrossRef]
- International Organization for Standardization. Tests for in-vitro cytotoxicity. In Biological Evaluation of Medical Devices, 3rd ed.; ISO: Geneva, Switzerland, 2009; pp. 1–11. [Google Scholar]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Formulation | Composition (% w/w) | L-PCL/H-PCL Ratio | ||
|---|---|---|---|---|
| L-PCL | H-PCL | TA | ||
| T0L20H80 | 20 | 80 | 0 | 20/80 |
| T0L40H60 | 40 | 60 | 0 | 40/60 |
| T5L20H80 | 19 | 76 | 5 | 20/80 |
| T5L40H60 | 38 | 57 | 5 | 40/60 |
| T10L20H80 | 18 | 72 | 10 | 20/80 |
| T10L40H60 | 36 | 54 | 10 | 40/60 |
| T20L20H80 | 16 | 64 | 20 | 20/80 |
| T20L40H60 | 32 | 48 | 20 | 40/60 |
| Formulation | Shape | Surface Area | Volume | SA/V Ratio |
|---|---|---|---|---|
| T5L20H80 | Filament | 12.98 ± 0.27 | 1.78 ± 0.07 | 7.30 ± 0.14 |
| Rectangular | 19.49 ± 0.66 | 5.18 ± 0.23 | 3.76 ± 0.04 | |
| Circle | 54.73 ± 1.52 | 19.53 ± 0.63 | 2.80 ± 0.01 | |
| T5L40H60 | Filament | 13.00 ± 0.22 | 1.77 ± 0.05 | 7.33 ± 0.07 |
| Rectangular | 18.17 ± 0.62 | 4.72 ± 0.23 | 3.85 ± 0.05 | |
| Circle | 55.48 ± 0.58 | 19.84 ± 0.24 | 2.80 ± 0.01 | |
| T10L20H80 | Filament | 12.10 ± 0.60 | 1.55 ± 0.15 | 7.82 ± 0.37 |
| Rectangular | 18.89 ± 1.91 | 4.98 ± 0.65 | 3.80 ± 0.13 | |
| Circle | 54.73 ± 1.09 | 19.53 ± 0.45 | 2.80 ± 0.01 | |
| T10L40H60 | Filament | 13.18 ± 0.18 | 1.82 ± 0.06 | 7.26 ± 0.12 |
| Rectangular | 19.70 ± 0.11 | 5.23 ± 0.02 | 3.76 ± 0.01 | |
| Circle | 54.48 ± 0.95 | 19.43 ± 0.45 | 2.80 ± 0.01 | |
| T20L20H80 | Filament | 13.99 ± 0.12 | 2.40 ± 0.04 | 5.83 ± 0.06 |
| Rectangular | 21.16 ± 0.34 | 5.77 ± 0.12 | 3.67 ± 0.02 | |
| Circle | 53.48 ± 0.75 | 19.01 ± 0.31 | 2.80 ± 0.01 | |
| T20L40H60 | Filament | 12.56 ± 0.32 | 1.66 ± 0.08 | 7.57 ± 0.19 |
| Rectangular | 18.78 ± 0.75 | 4.94 ± 0.26 | 3.80 ± 0.05 | |
| Circle | 54.60 ± 0.38 | 19.48 ± 0.16 | 2.80 ± 0.00 |
| Formulation | Filament | Rectangular | Circle | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Korsmeyer–Peppas | Higuchi | Korsmeyer– Peppas | Higuchi | Korsmeyer– Peppas | Higuchi | ||||
| R2 | n | R2 | R2 | n | R2 | R2 | n | R2 | |
| T5L20H80 | 0.9954 | 0.461 | 0.9939 | 0.9942 | 0.472 | 0.9851 | 0.9982 | 0.433 | 0.9850 |
| T5L40H60 | 0.9922 | 0.446 | 0.9812 | 0.9796 | 0.475 | 0.9750 | 0.9869 | 0.378 | 0.9325 |
| T10L20H80 | 0.9911 | 0.437 | 0.9679 | 0.9962 | 0.386 | 0.9448 | 0.9964 | 0.431 | 0.9834 |
| T10L40H60 | 0.9925 | 0.552 | 0.9922 | 0.9920 | 0.477 | 0.9904 | 0.9863 | 0.411 | 0.9515 |
| T20L20H80 | 0.9963 | 0.497 | 0.9942 | 0.9966 | 0.426 | 0.9771 | 0.9917 | 0.454 | 0.9870 |
| T20L40H60 | 0.9923 | 0.518 | 0.9907 | 0.9856 | 0.437 | 0.9606 | 0.9891 | 0.509 | 0.9902 |
| Formulation | Mass Loss of PCL (%) | ||
|---|---|---|---|
| Filament | Rectangular | Circle | |
| T5L20H80 | 12.34 ± 0.23 | 11.00 ± 0.19 | 9.92 ± 0.62 |
| T5L40H60 | 14.20 ± 0.67 | 14.08 ± 1.74 | 13.42 ± 1.32 |
| T10L20H80 | 13.02 ± 0.32 | 12.05 ± 1.04 | 10.18 ± 0.36 |
| T10L40H60 | 14.81 ± 1.37 | 14.40 ± 1.04 | 14.25 ± 0.20 |
| T20L20H80 | 14.41 ± 0.84 | 13.77 ± 0.93 | 10.38 ± 0.70 |
| T20L40H60 | 18.27 ± 2.52 | 16.97 ± 1.04 | 16.63 ± 2.00 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Annuryanti, F.; Domínguez-Robles, J.; Anjani, Q.K.; Adrianto, M.F.; Larrañeta, E.; Thakur, R.R.S. Fabrication and Characterisation of 3D-Printed Triamcinolone Acetonide-Loaded Polycaprolactone-Based Ocular Implants. Pharmaceutics 2023, 15, 243. https://doi.org/10.3390/pharmaceutics15010243
Annuryanti F, Domínguez-Robles J, Anjani QK, Adrianto MF, Larrañeta E, Thakur RRS. Fabrication and Characterisation of 3D-Printed Triamcinolone Acetonide-Loaded Polycaprolactone-Based Ocular Implants. Pharmaceutics. 2023; 15(1):243. https://doi.org/10.3390/pharmaceutics15010243
Chicago/Turabian StyleAnnuryanti, Febri, Juan Domínguez-Robles, Qonita Kurnia Anjani, Muhammad Faris Adrianto, Eneko Larrañeta, and Raghu Raj Singh Thakur. 2023. "Fabrication and Characterisation of 3D-Printed Triamcinolone Acetonide-Loaded Polycaprolactone-Based Ocular Implants" Pharmaceutics 15, no. 1: 243. https://doi.org/10.3390/pharmaceutics15010243
APA StyleAnnuryanti, F., Domínguez-Robles, J., Anjani, Q. K., Adrianto, M. F., Larrañeta, E., & Thakur, R. R. S. (2023). Fabrication and Characterisation of 3D-Printed Triamcinolone Acetonide-Loaded Polycaprolactone-Based Ocular Implants. Pharmaceutics, 15(1), 243. https://doi.org/10.3390/pharmaceutics15010243