

Patient Perceptions and Potential Utility of Pharmacogenetic Testing in Chronic Pain Management and Opioid Use Disorder in the Camden Opioid Research Initiative

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Populations
2.2. Genetic and Non-Genetic Data Collection
2.3. Data Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Heil, J.; Zajic, S.; Albertson, E.; Brangan, A.; Jones, I.; Roberts, W.; Sabia, M.; Bodofsky, E.; Resch, A.; Rafeq, R.; et al. The Genomics of Opioid Addiction Longitudinal Study (GOALS): Study design for a prospective evaluation of genetic and non-genetic factors for development of and recovery from opioid use disorder. BMC Med. Genom. 2021, 14, 16. [Google Scholar] [CrossRef]
- Scheinfeldt, L.B.; Brangan, A.; Kusic, D.M.; Kumar, S.; Gharani, N. Common Treatment, Common Variant: Evolutionary Prediction of Functional Pharmacogenomic Variants. J. Pers. Med. 2021, 11, 131. [Google Scholar] [CrossRef]
- Relling, M.V.; Evans, W.E. Pharmacogenomics in the clinic. Nature 2015, 526, 343–350. [Google Scholar] [CrossRef]
- Bank, P.C.D.; Swen, J.J.; Guchelaar, H.J. Implementation of Pharmacogenomics in Everyday Clinical Settings. Adv. Pharmacol. 2018, 83, 219–246. [Google Scholar] [CrossRef]
- Gharani, N.; Keller, M.A.; Stack, C.B.; Hodges, L.M.; Schmidlen, T.J.; Lynch, D.E.; Gordon, E.S.; Christman, M.F. The Coriell personalized medicine collaborative pharmacogenomics appraisal, evidence scoring and interpretation system. Genome Med. 2013, 5, 93. [Google Scholar] [CrossRef]
- Rasmussen-Torvik, L.J.; Stallings, S.C.; Gordon, A.S.; Almoguera, B.; Basford, M.A.; Bielinski, S.J.; Brautbar, A.; Brilliant, M.H.; Carrell, D.S.; Connolly, J.J.; et al. Design and anticipated outcomes of the eMERGE-PGx project: A multicenter pilot for preemptive pharmacogenomics in electronic health record systems. Clin. Pharmacol. Ther. 2014, 96, 482–489. [Google Scholar] [CrossRef]
- Relling, M.V.; Krauss, R.M.; Roden, D.M.; Klein, T.E.; Fowler, D.M.; Terada, N.; Lin, L.; Riel-Mehan, M.; Do, T.P.; Kubo, M.; et al. New Pharmacogenomics Research Network: An Open Community Catalyzing Research and Translation in Precision Medicine. Clin. Pharmacol. Ther. 2017, 102, 897–902. [Google Scholar] [CrossRef]
- Crews, K.R.; Hicks, J.K.; Pui, C.H.; Relling, M.V.; Evans, W.E. Pharmacogenomics and individualized medicine: Translating science into practice. Clin. Pharmacol. Ther. 2012, 92, 467–475. [Google Scholar] [CrossRef]
- Zajic, S.C.; Jarvis, J.P.; Zhang, P.; Rajula, K.D.; Brangan, A.; Brenner, R.; Dempsey, M.P.; Christman, M.F. Individuals with CYP2C8 and CYP2C9 reduced metabolism haplotypes self-adjusted ibuprofen dose in the Coriell Personalized Medicine Collaborative. Pharm. Genom. 2019, 29, 49–57. [Google Scholar] [CrossRef]
- Lee, Y.M.; McKillip, R.P.; Borden, B.A.; Klammer, C.E.; Ratain, M.J.; O’Donnell, P.H. Assessment of patient perceptions of genomic testing to inform pharmacogenomic implementation. Pharm. Genom. 2017, 27, 179–189. [Google Scholar] [CrossRef] [Green Version]
- Magarbeh, L.; Gorbovskaya, I.; Le Foll, B.; Jhirad, R.; Muller, D.J. Reviewing pharmacogenetics to advance precision medicine for opioids. Biomed. Pharm. 2021, 142, 112060. [Google Scholar] [CrossRef]
- Deodhar, M.; Turgeon, J.; Michaud, V. Contribution of CYP2D6 Functional Activity to Oxycodone Efficacy in Pain Management: Genetic Polymorphisms, Phenoconversion, and Tissue-Selective Metabolism. Pharmaceutics 2021, 13, 1466. [Google Scholar] [CrossRef]
- Stamer, U.M.; Zhang, L.; Book, M.; Lehmann, L.E.; Stuber, F.; Musshoff, F. CYP2D6 genotype dependent oxycodone metabolism in postoperative patients. PLoS ONE 2013, 8, e60239. [Google Scholar] [CrossRef]
- Smith, D.M.; Weitzel, K.W.; Elsey, A.R.; Langaee, T.; Gong, Y.; Wake, D.T.; Duong, B.Q.; Hagen, M.; Harle, C.A.; Mercado, E.; et al. CYP2D6-guided opioid therapy improves pain control in CYP2D6 intermediate and poor metabolizers: A pragmatic clinical trial. Genet. Med. 2019, 21, 1842–1850. [Google Scholar] [CrossRef]
- Crews, K.R.; Monte, A.A.; Huddart, R.; Caudle, K.E.; Kharasch, E.D.; Gaedigk, A.; Dunnenberger, H.M.; Leeder, J.S.; Callaghan, J.T.; Samer, C.F.; et al. Clinical Pharmacogenetics Implementation Consortium Guideline for CYP2D6, OPRM1, and COMT Genotypes and Select Opioid Therapy. Clin. Pharmacol. Ther. 2021, 110, 888–896. [Google Scholar] [CrossRef]
- Nakhaee, S.; Hoyte, C.; Dart, R.C.; Askari, M.; Lamarine, R.J.; Mehrpour, O. A review on tramadol toxicity: Mechanism of action, clinical presentation, and treatment. Forensic Toxicol. 2021, 39, 293–310. [Google Scholar] [CrossRef]
- Lurcott, G. The effects of the genetic absence and inhibition of CYP2D6 on the metabolism of codeine and its derivatives, hydrocodone and oxycodone. Anesth. Prog. 1998, 45, 154–156. [Google Scholar]
- Cardia, L.; Calapai, G.; Quattrone, D.; Mondello, C.; Arcoraci, V.; Calapai, F.; Mannucci, C.; Mondello, E. Preclinical and Clinical Pharmacology of Hydrocodone for Chronic Pain: A Mini Review. Front. Pharmacol. 2018, 9, 1122. [Google Scholar] [CrossRef]
- Sordo, L.; Barrio, G.; Bravo, M.J.; Indave, B.I.; Degenhardt, L.; Wiessing, L.; Ferri, M.; Pastor-Barriuso, R. Mortality risk during and after opioid substitution treatment: Systematic review and meta-analysis of cohort studies. BMJ 2017, 357, j1550. [Google Scholar] [CrossRef]
- Segui, H.A.; Melin, K.; Quinones, D.S.; Duconge, J. A review of the pharmacogenomics of buprenorphine for the treatment of opioid use disorder. J. Transl. Genet. Genom. 2020, 4, 263–277. [Google Scholar] [CrossRef]
- Meaden, C.W.; Mozeika, A.; Asri, R.; Santos, C.D. A review of the existing literature on buprenorphine pharmacogenomics. Pharm. J. 2021, 21, 128–139. [Google Scholar] [CrossRef] [PubMed]
- Ettienne, E.B.; Ofoegbu, A.; Maneno, M.K.; Briggs, J.; Ezeude, G.; Williams, S.; Walker, C.; Chapman, E. Pharmacogenomics and Opioid Use Disorder: Clinical Decision Support in an African American Cohort. J. Natl. Med. Assoc. 2019, 111, 674–681. [Google Scholar] [CrossRef] [PubMed]
- Li, H. A statistical framework for SNP calling, mutation discovery, association mapping and population genetical parameter estimation from sequencing data. Bioinformatics 2011, 27, 2987–2993. [Google Scholar] [CrossRef]
- Team, R.C. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020. [Google Scholar]
- Crews, K.R.; Gaedigk, A.; Dunnenberger, H.M.; Klein, T.E.; Shen, D.D.; Callaghan, J.T.; Kharasch, E.D.; Skaar, T.C.; Clinical Pharmacogenetics Implementation, C. Clinical Pharmacogenetics Implementation Consortium (CPIC) guidelines for codeine therapy in the context of cytochrome P450 2D6 (CYP2D6) genotype. Clin. Pharmacol. Ther. 2012, 91, 321–326. [Google Scholar] [CrossRef] [PubMed]
- Singh, D.R.; Nag, K.; Shetti, A.N.; Krishnaveni, N. Tapentadol hydrochloride: A novel analgesic. Saudi J. Anaesth. 2013, 7, 322–326. [Google Scholar] [CrossRef] [PubMed]
- Olson, J.E.; Rohrer Vitek, C.R.; Bell, E.J.; McGree, M.E.; Jacobson, D.J.; St Sauver, J.L.; Caraballo, P.J.; Griffin, J.M.; Roger, V.L.; Bielinski, S.J. Participant-perceived understanding and perspectives on pharmacogenomics: The Mayo Clinic RIGHT protocol (Right Drug, Right Dose, Right Time). Genet. Med. 2017, 19, 819–825. [Google Scholar] [CrossRef]
- Zhou, H.; Rentsch, C.T.; Cheng, Z.; Kember, R.L.; Nunez, Y.Z.; Sherva, R.M.; Tate, J.P.; Dao, C.; Xu, K.; Polimanti, R.; et al. Association of OPRM1 Functional Coding Variant With Opioid Use Disorder: A Genome-Wide Association Study. JAMA Psychiatry 2020, 77, 1072–1080. [Google Scholar] [CrossRef]
- Zubiaur, P.; Prosper-Cuesta, D.N.; Novalbos, J.; Mejia-Abril, G.; Navares-Gomez, M.; Villapalos-Garcia, G.; Soria-Chacartegui, P.; Abad-Santos, F. Patients’ Perceptions of Pharmacogenetic Testing and Access to Their Results: State of the Art in Spain and Systematic Review. J. Pers. Med. 2022, 12, 270. [Google Scholar] [CrossRef]
- Rogausch, A.; Prause, D.; Schallenberg, A.; Brockmoller, J.; Himmel, W. Patients’ and physicians’ perspectives on pharmacogenetic testing. Pharmacogenomics 2006, 7, 49–59. [Google Scholar] [CrossRef]
- Botham, J.; Shilling, V.; Jones, J. Patient and public understanding of the concept of ‘personalised medicine’ in relation to cancer treatment: A systematic review. Future Healthc. J. 2021, 8, e703–e708. [Google Scholar] [CrossRef]
- Lemke, A.A.; Hulick, P.J.; Wake, D.T.; Wang, C.; Sereika, A.W.; Yu, K.D.; Glaser, N.S.; Dunnenberger, H.M. Patient perspectives following pharmacogenomics results disclosure in an integrated health system. Pharmacogenomics 2018, 19, 321–331. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
| GOALS (N = 125) | OPTIN (N = 119) | |
|---|---|---|
| Female | 70 (56%) | 75 (63%) |
| Male | 55 (44%) | 44 (37%) |
| Hispanic or Latino | 28 (22%) | 16 (13%) |
| Not Hispanic or Latino | 93 (74%) | 98 (82%) |
| Unknown | 4 (3%) | 5 (4%) |
| Asian | 2 (2%) | 1 (<1%) |
| Black or African-American | 24 (19%) | 27 (23%) |
| Native Hawaiian or other Pacific Islander | 1 (<1%) | 0 (0%) |
| Other | 3 (2%) | 2 (2%) |
| White(Caucasian) | 86 (69%) | 79 (66%) |
| More than one race | 6 (5%) | 7 (6%) |
| Unknown | 3 (2%) | 3 (3%) |
| Mean age at survey (years) ± SD | 40.5 ± 11 | 55.8 ± 11 |
| GOALS (N = 125) | OPTIN (N = 119) | |
|---|---|---|
| “Have you been exposed to genetics before enrolling in the study?” | ||
| Yes | 36 (29%) | 42 (35%) |
| No | 80 (64%) | 70 (59%) |
| Don’t know | 7 (6%) | 4 (3%) |
| No Answer | 2 (2%) | 3 (3%) |
| “Through which sources [have you been exposed to genetics before enrolling in the study]?” Please note, N is based on respondents who answered “Yes” to having been exposed to genetics before enrolling in the study (N = 36 for GOALS; N = 42 for OPTIN; participants could choose more than one response or could choose “other” and enter free text). | ||
| Books | 5 (14%) | 5 (12%) |
| Genetic or personalized medicine websites | 6 (17%) | 4 (10%) |
| High school or college-level courses | 22 (61%) | 25 (61%) |
| Internet | 9 (25%) | 11 (27%) |
| News or magazine articles | 9 (25%) | 5 (12%) |
| Other: common knowledge | 1 (3%) | 0 (0%) |
| Other: jail | 1 (3%) | 0 (0%) |
| Other: previous genetic testing | 5 (14%) | 5 (12%) |
| Other: tv/documentaries | 0 (0%) | 2 (5%) |
| Other: direct to consumer genetic testing | 0 (0%) | 3 (7%) |
| Other: other study | 0 (0%) | 2 (5%) |
| Other: family | 0 (0%) | 1 (2%) |
| Other: previous clinical care | 0 (0%) | 0 (0%) |
| OPTIN: “If there was a genetic test that would advise you and your doctor about your risk for developing opioid use disorder, how much would you want to get tested?” GOALS: “If there was a genetic test that would advise your doctor on which of the three opioid use disorder medication-assisted treatments (buprenorphine/Subutex, methadone/Dolophine or naltrexone/Vivitrol) would work best for you, how much would you want to get tested?” | ||
| Extremely | 54 (43%) | 33 (28%) |
| Considerably | 28 (22%) | 32 (27%) |
| Moderately | 22 (18%) | 20 (17%) |
| Slightly | 7 (6%) | 7 (6%) |
| Not at All | 7 (6%) | 13 (11%) |
| Don’t Know | 5 (4%) | 8 (7%) |
| Don’t Want to Answer | 0 (0%) | 2 (2%) |
| No Answer | 2 (2%) | 4 (3%) |
| “Compared to most people, how would you rate your knowledge of genetics?” | ||
| Better than most people | 13 (10%) | 19 (16%) |
| About average | 66 (53%) | 63 (53%) |
| Less than most people | 32 (26%) | 26 (22%) |
| Don’t know | 12 (10%) | 7 (6%) |
| Don’t want to answer | 0 (0%) | 1 (1%) |
| No Answer | 2 (2%) | 3 (3%) |
| “Do you look for information about opioid use disorder?” | ||
| Yes | 84 (67%) | 42 (35%) |
| No | 37 (30%) | 72 (61%) |
| Don’t know | 2 (2%) | 2 (2%) |
| No Answer | 2 (2%) | 3 (3%) |
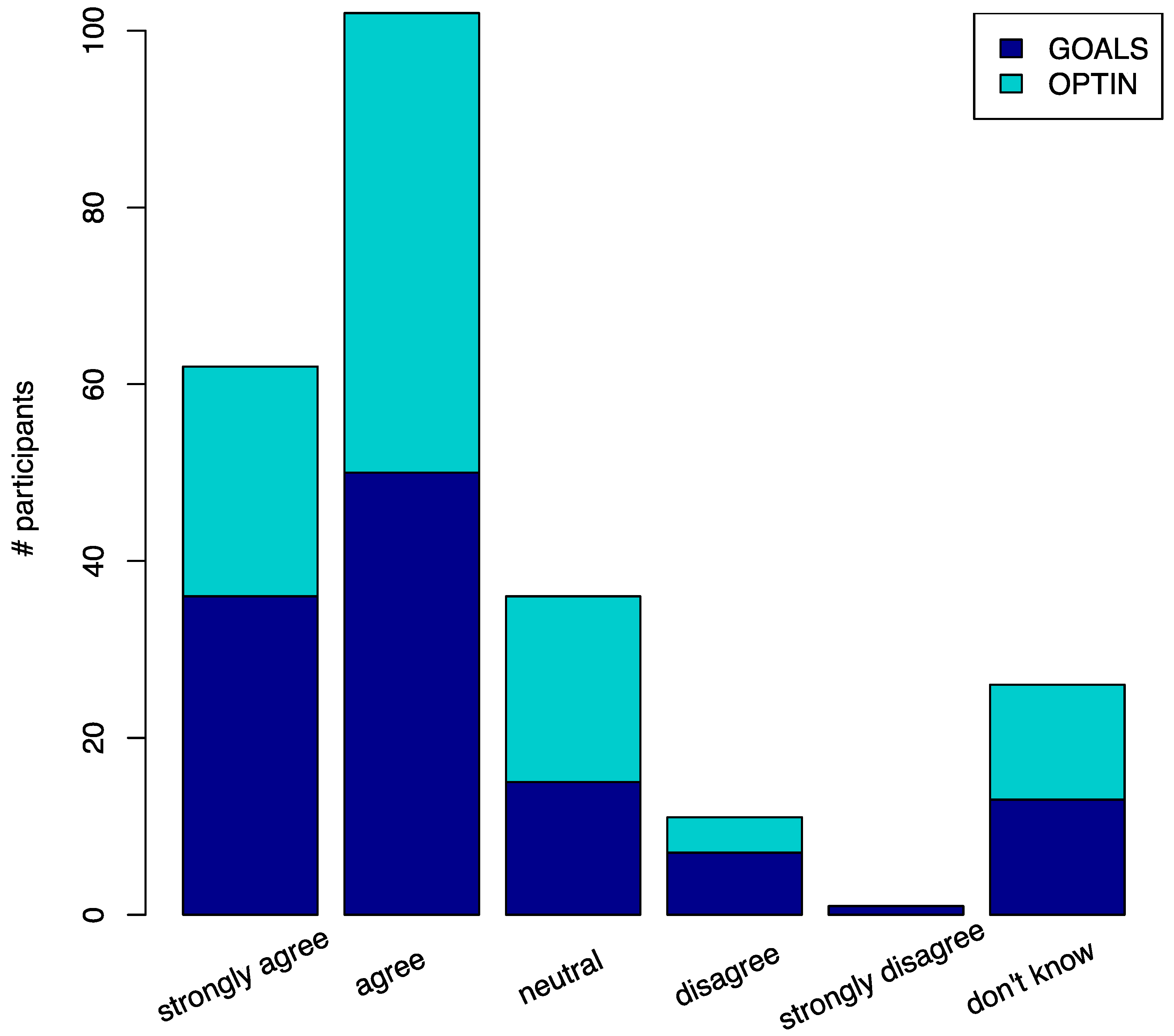
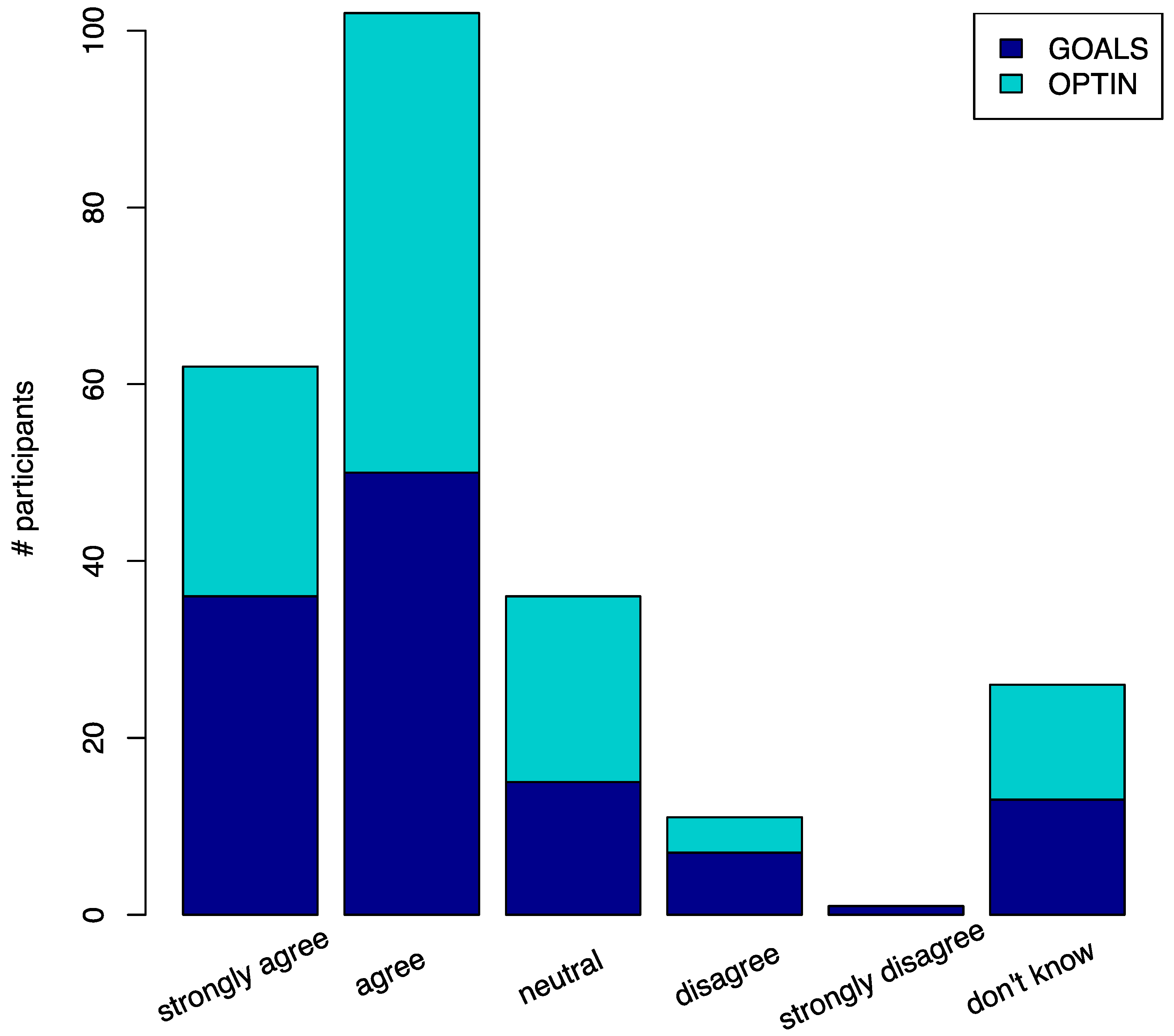
| “Genetics have the potential to improve my medical care.” | ||
| Strongly agree | 36 (29%) | 26 (22%) |
| Agree | 50 (40%) | 52 (44%) |
| Neutral | 15 (12%) | 21 (18%) |
| Disagree | 7 (6%) | 4 (3%) |
| Strongly disagree | 1 (1%) | 0 (0%) |
| Don’t know | 13 (10%) | 13 (11%) |
| Don’t want to answer | 1 (1%) | 0 (0%) |
| No answer | 2 (2%) | 3 (3%) |
| “I am concerned about who will be able to access my genetic test results.” | ||
| Strongly agree | 7 (6%) | 9 (8%) |
| Agree | 19 (15%) | 27 (23%) |
| Neutral | 19 (15%) | 26 (22%) |
| Disagree | 52 (42%) | 37 (31%) |
| Strongly disagree | 19 (15%) | 11 (9%) |
| Don’t know | 7 (6%) | 6 (5%) |
| No answer | 2 (2%) | 3 (3%) |
| “Genetic testing puts people at risk for genetic discrimination.” | ||
| Strongly agree | 6 (5%) | 2 (2%) |
| Agree | 9 (7%) | 13 (11%) |
| Neutral | 20 (16%) | 21 (18%) |
| Disagree | 57 (46%) | 46 (39%) |
| Strongly disagree | 20 (16%) | 13 (11%) |
| Don’t know | 11 (9%) | 20 (17%) |
| Don’t want to answer | 0 (0%) | 1 (1%) |
| No answer | 2 (2%) | 3 (3%) |
| “I would change my lifestyle based on genetic test results.” | ||
| Strongly agree | 10 (8%) | 14 (12%) |
| Agree | 37 (30%) | 34 (29%) |
| Neutral | 37 (30%) | 26 (22%) |
| Disagree | 19 (15%) | 21 (18%) |
| Strongly disagree | 6 (5%) | 6 (5%) |
| Don’t know | 13 (10%) | 15 (13%) |
| Don’t want to answer | 1 (1 %) | 0 (0%) |
| No answer | 2 (2%) | 3 (3%) |
| “Were you ever told that you had a risk for developing opioid or substance use problems based on your family history?” | ||
| Yes | 39 (31%) | 14 (12%) |
| No | 78 (62%) | 100 (84%) |
| Don’t know | 6 (5%) | 2 (2%) |
| No answer | 2 (2%) | 3 (3%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kusic, D.; Heil, J.; Zajic, S.; Brangan, A.; Dairo, O.; Smith, G.; Morales-Scheihing, D.; Buono, R.J.; Ferraro, T.N.; Haroz, R.; et al. Patient Perceptions and Potential Utility of Pharmacogenetic Testing in Chronic Pain Management and Opioid Use Disorder in the Camden Opioid Research Initiative. Pharmaceutics 2022, 14, 1863. https://doi.org/10.3390/pharmaceutics14091863
Kusic D, Heil J, Zajic S, Brangan A, Dairo O, Smith G, Morales-Scheihing D, Buono RJ, Ferraro TN, Haroz R, et al. Patient Perceptions and Potential Utility of Pharmacogenetic Testing in Chronic Pain Management and Opioid Use Disorder in the Camden Opioid Research Initiative. Pharmaceutics. 2022; 14(9):1863. https://doi.org/10.3390/pharmaceutics14091863
Chicago/Turabian StyleKusic, Dara, Jessica Heil, Stefan Zajic, Andrew Brangan, Oluseun Dairo, Gretchen Smith, Diego Morales-Scheihing, Russell J. Buono, Thomas N. Ferraro, Rachel Haroz, and et al. 2022. "Patient Perceptions and Potential Utility of Pharmacogenetic Testing in Chronic Pain Management and Opioid Use Disorder in the Camden Opioid Research Initiative" Pharmaceutics 14, no. 9: 1863. https://doi.org/10.3390/pharmaceutics14091863
APA StyleKusic, D., Heil, J., Zajic, S., Brangan, A., Dairo, O., Smith, G., Morales-Scheihing, D., Buono, R. J., Ferraro, T. N., Haroz, R., Salzman, M., Baston, K., Bodofsky, E., Sabia, M., Resch, A., & Scheinfeldt, L. B. (2022). Patient Perceptions and Potential Utility of Pharmacogenetic Testing in Chronic Pain Management and Opioid Use Disorder in the Camden Opioid Research Initiative. Pharmaceutics, 14(9), 1863. https://doi.org/10.3390/pharmaceutics14091863