
Creating Acceptable Tablets 3D (CAT 3D): A Feasibility Study to Evaluate the Acceptability of 3D Printed Tablets in Children and Young People

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Filament Production
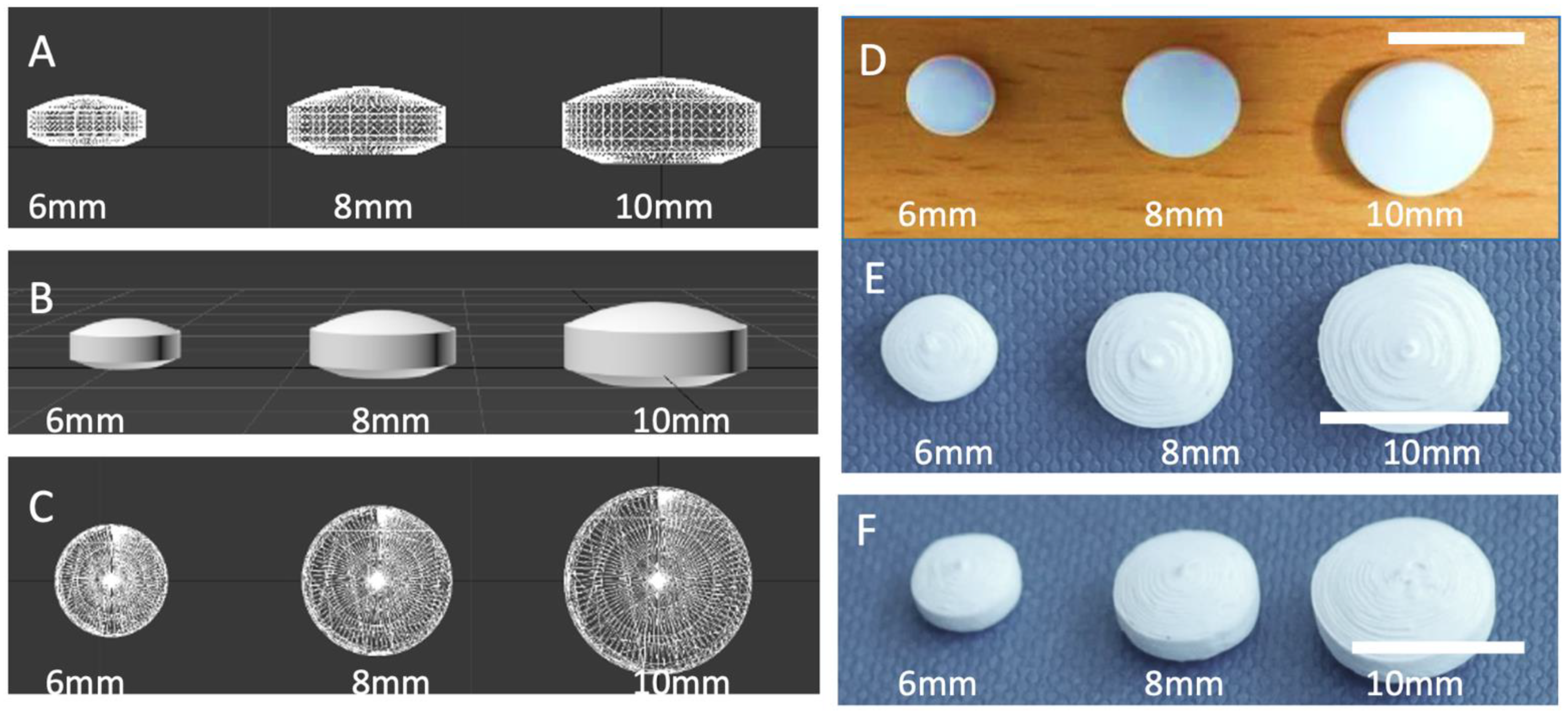
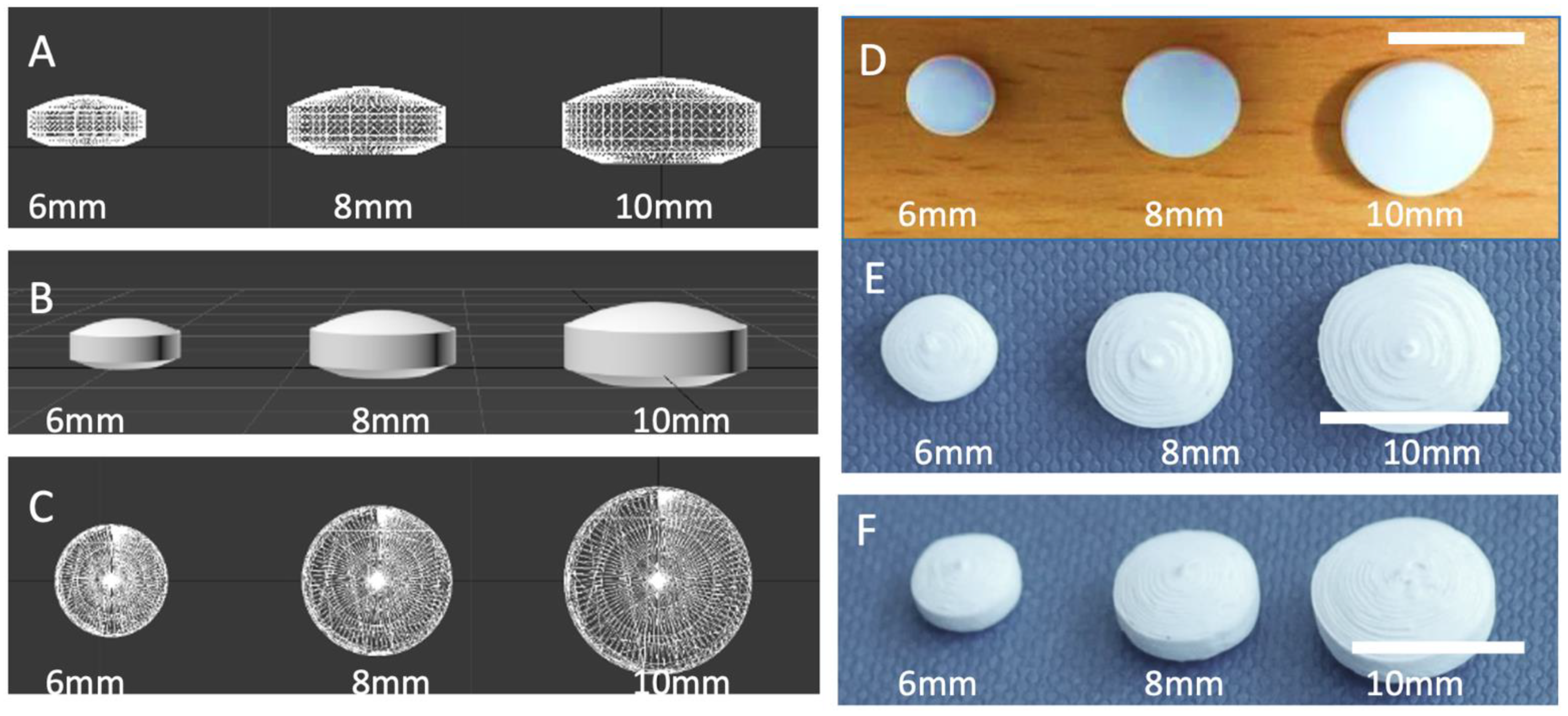
2.3. Design and 3DP of Tablets
2.4. Heavy Metal Assay
2.5. Residual Solvents Studies
2.6. Acceptability Studies
2.6.1. Setting
2.6.2. Participants
2.6.3. Consent
2.6.4. Patient and Public Involvement
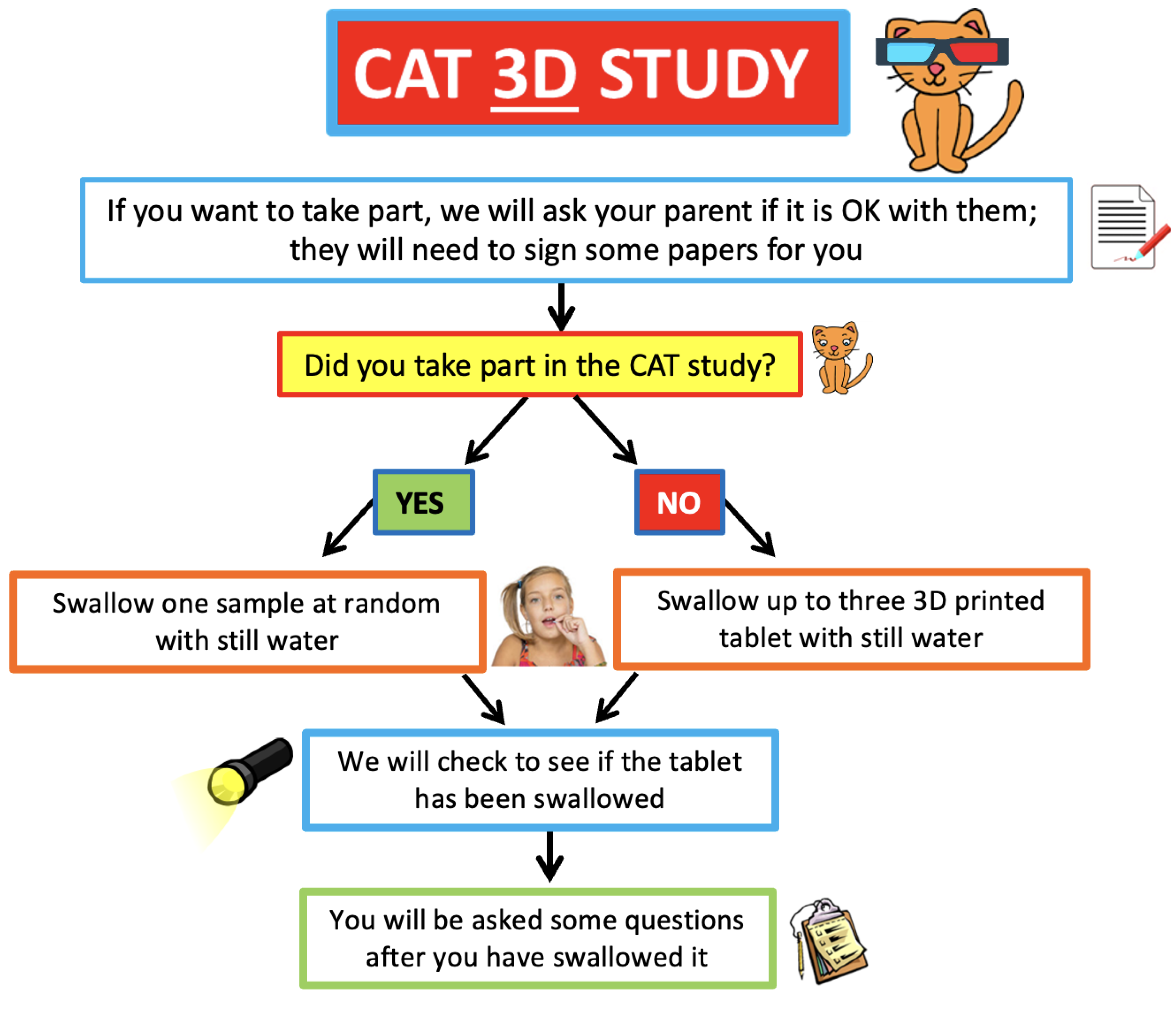
2.6.5. Interventions
2.6.6. Staff Training
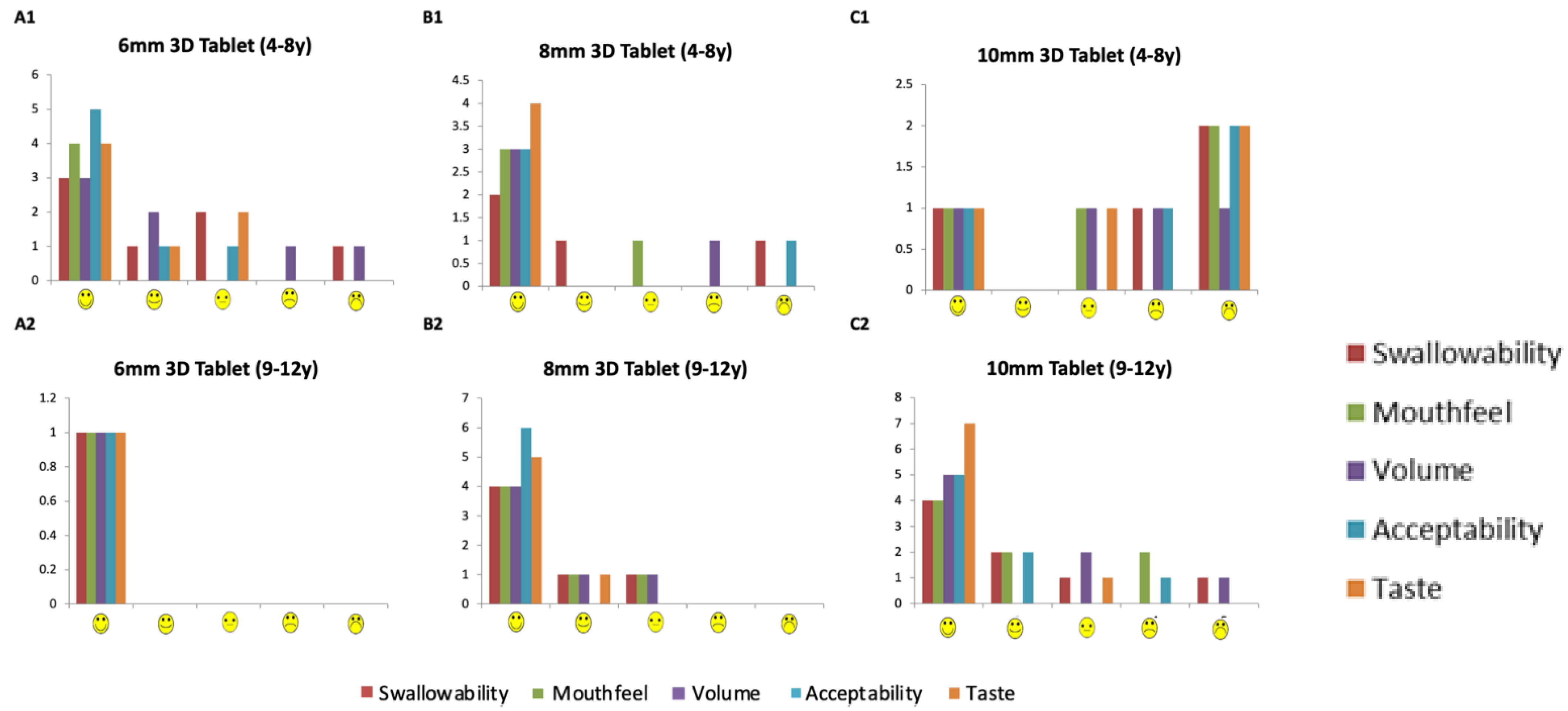
2.6.7. Outcomes
2.7. Regulatory Approvals
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Matsui, D. Current Issues in Pediatric Medication Adherence. Pediatric Drugs 2007, 9, 283–288. [Google Scholar] [CrossRef]
- Venables, R.; Batchelor, H.; Hodson, J.; Stirling, H.; Marriott, J. Determination of Formulation Factors That Affect Oral Medicines Acceptability in a Domiciliary Paediatric Population. Int. J. Pharm. 2015, 480, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Kozarewicz, P. Regulatory Perspectives on Acceptability Testing of Dosage Forms in Children. Int. J. Pharm. 2014, 469, 245–248. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. Development of Paediatric Medicines: Points to Consider in Formulation. WHO Annex 5 WHO Technical Report Series 970. 2012. Available online: https://www.who.int/publications/m/item/trs970-annex-5-development-of-paediatric-medicines-points-to-consider-in-formulation (accessed on 21 January 2022).
- European Medicines Agency. Guideline on Pharmaceutical Development of Medicines for Paediatric Use; European Medicines Agency: Amsterdam, The Netherlands, 2013; Volume 44, pp. 1–24. Available online: http://www.ema.europa.eu/docs/en_GB/document_library/Scientific_guideline/2013/07/WC500147002.pdf (accessed on 21 January 2022).
- Richey, R.H.; Hughes, C.; Craig, J.V.; Shah, U.U.; Ford, J.L.; Barker, C.E.; Peak, M.; Nunn, A.J.; Turner, M.A. A Systematic Review of the Use of Dosage Form Manipulation to Obtain Required Doses to Inform Use of Manipulation in Paediatric Practice. Int. J. Pharm. 2017, 518, 155–166.7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richey, R.H.; Shah, U.U.; Peak, M.; Craig, J.V.; Ford, J.L.; Barker, C.E.; Nunn, A.J.; Turner, M.A. Manipulation of Drugs to Achieve the Required Dose Is Intrinsic to Paediatric Practice but Is Not Supported by Guidelines or Evidence. BMC Pediatrics 2013, 13, 18. [Google Scholar] [CrossRef] [Green Version]
- Richey, R.H.; Craig, J.V.; Shah, U.U.; Ford, J.L.; Barker, C.E.; Peak, M.; Nunn, A.J.; Turner, M.A. The Manipulation of Drugs to Obtain the Required Dose: Systematic Review. J. Adv. Nurs. 2012, 68, 2103–2112. [Google Scholar] [CrossRef] [PubMed]
- Richey, R.H.; Craig, J.V.; Shah, U.U.; Nunn, A.J.; Turner, M.A.; Barker, C.E.; Ford, J.L.; Peak, M. MODRIC—Manipulation of Drugs in Children. Int. J. Pharm. 2013, 457, 339–341. [Google Scholar] [CrossRef]
- Trofimiuk, M.; Wasilewska, K.; Winnicka, K. How to Modify Drug Release in Paediatric Dosage Forms? Novel Technologies and Modern Approaches with Regard to Children’s Population. Int. J. Mol. Sci. 2019, 20, 3200. [Google Scholar] [CrossRef] [Green Version]
- Klingmann, V.; Spomer, N.; Lerch, C.; Stoltenberg, I.; Frömke, C.; Bosse, H.M.; Breitkreutz, J.; Meissner, T. Favorable Acceptance of Mini-Tablets Compared with Syrup: A Randomized Controlled Trial in Infants and Preschool Children. J. Pediatrics 2013, 163, 1728–1732.e1. [Google Scholar] [CrossRef]
- Thomson, S.A.; Tuleu, C.; Wong, I.C.K.; Keady, S.; Pitt, K.G.; Sutcliffe, A.G. Minitablets: New Modality to Deliver Medicines to Preschool-Aged Children. Pediatrics 2009, 123, e235–e238. [Google Scholar] [CrossRef] [PubMed]
- Ranmal, S.R.; Cram, A.; Tuleu, C. Age-Appropriate and Acceptable Paediatric Dosage Forms: Insights into End-User Perceptions, Preferences and Practices from the Children’s Acceptability of Oral Formulations (CALF) Study. Int. J. Pharm. 2016, 514, 296–307. [Google Scholar] [CrossRef] [PubMed]
- Alessandrini, E.; Brako, F.; Scarpa, M.; Lupo, M.; Bonifazi, D.; Pignataro, V.; Cavallo, M.; Cullufe, O.; Enache, C.; Nafria, B.; et al. Children’s Preferences for Oral Dosage Forms and Their Involvement in Formulation Research via Eptri (European Paediatric Translational Research Infrastructure). Pharmaceutics 2021, 13, 730. [Google Scholar] [CrossRef] [PubMed]
- Palekar, S.; Nukala, P.K.; Mishra, S.M.; Kipping, T.; Patel, K. Application of 3D Printing Technology and Quality by Design Approach for Development of Age-Appropriate Pediatric Formulation of Baclofen. Int. J. Pharm. 2019, 556, 106–116. [Google Scholar] [CrossRef]
- Scoutaris, N.; Ross, S.A.; Douroumis, D. 3D Printed “Starmix” Drug Loaded Dosage Forms for Paediatric Applications. Pharm. Res. 2018, 35, 34. [Google Scholar] [CrossRef]
- Rycerz, K.; Stepien, K.A.; Czapiewska, M.; Arafat, B.T.; Habashy, R.; Isreb, A.; Peak, M.; Alhnan, M.A. Embedded 3D Printing of Novel Bespoke Soft Dosage Form Concept for Pediatrics. Pharmaceutics 2019, 11, 630. [Google Scholar] [CrossRef] [Green Version]
- Karavasili, C.; Gkaragkounis, A.; Moschakis, T.; Ritzoulis, C.; Fatouros, D.G. Pediatric-Friendly Chocolate-Based Dosage Forms for the Oral Administration of Both Hydrophilic and Lipophilic Drugs Fabricated with Extrusion-Based 3D Printing. Eur. J. Pharm. Sci. 2020, 147, 105291. [Google Scholar] [CrossRef]
- Goyanes, A.; Madla, C.M.; Umerji, A.; Duran Piñeiro, G.; Giraldez Montero, J.M.; Lamas Diaz, M.J.; Gonzalez Barcia, M.; Taherali, F.; Sánchez-Pintos, P.; Couce, M.L.; et al. Automated Therapy Preparation of Isoleucine Formulations Using 3D Printing for the Treatment of MSUD: First Single-Centre, Prospective, Crossover Study in Patients. Int. J. Pharm. 2019, 567, 118497. [Google Scholar] [CrossRef] [PubMed]
- Januskaite, P.; Xu, X.; Ranmal, S.R.; Gaisford, S.; Basit, A.W.; Tuleu, C.; Goyanes, A. I Spy with My Little Eye: A Paediatric Visual Preferences Survey of 3d Printed Tablets. Pharmaceutics 2020, 12, 1100. [Google Scholar] [CrossRef]
- Bracken, L.; McDonough, E.; Ashleigh, S.; Wilson, F.; Shakeshaft, J.; Ohia, U.; Mistry, P.; Jones, H.; Kanji, N.; Liu, F.; et al. Can Children Swallow Tablets? Outcome Data from a Feasibility Study to Assess the Acceptability of Different-Sized Placebo Tablets in Children (Creating Acceptable Tablets (CAT)). BMJ Open 2020, 10, e036508. [Google Scholar] [CrossRef]
- Beck, M.H.; Cataldo, M.; Slifer, K.J.; Pulbrook, V.; Guhman, J.K. Teaching Children with Attention Deficit Hyperactivity Disorder (ADHD) and Autistic Disorder (AD) How to Swallow Pills. Clin. Pediatrics 2005, 44, 515–526. [Google Scholar] [CrossRef] [PubMed]
- Tse, Y.; Vasey, N.; Dua, D.; Oliver, S.; Emmet, V.; Pickering, A.; Lim, E. The KidzMed Project: Teaching Children to Swallow Tablet Medication. Arch. Dis. Child. 2020, 105, 1105–1107. [Google Scholar] [CrossRef]
- Cantor, S.L.; Khan, M.A.; Gupta, A. Development and Optimization of Taste-Masked Orally Disintegrating Tablets (ODTs) of Clindamycin Hydrochloride. Drug Dev. Ind. Pharm. 2015, 41, 1156–1164. [Google Scholar] [CrossRef]
- Lou, H.; Liu, M.; Qu, W.; Hu, Z.; Brunson, E.; Johnson, J.; Almoazen, H. Evaluation of Chlorpheniramine Maleate Microparticles in Orally Disintegrating Film and Orally Disintegrating Tablet for Pediatrics. Drug Dev. Ind. Pharm. 2014, 40, 910–918. [Google Scholar] [CrossRef] [PubMed]
- Lou, H.; Liu, M.; Wang, L.; Mishra, S.R.; Qu, W.; Johnson, J.; Brunson, E.; Almoazen, H. Development of a Mini-Tablet of Co-Grinded Prednisone-Neusilin Complex for Pediatric Use. AAPS PharmSciTech 2013, 14, 950–958. [Google Scholar] [CrossRef] [Green Version]
- Pawar, H.A.; Joshi, P.R. Development and Evaluation of Taste Masked Granular Formulation of Satranidazole by Melt Granulation Technique. J. Pharm. 2014, 2014, 789676. [Google Scholar] [CrossRef] [Green Version]
- Kabeya, K.; Satoh, H.; Hori, S.; Sawada, Y. Experimental Study on Patient Preferences Regarding the Shape and Size of Medical Tablets and Capsules Using Three-Dimensionally Printed Plastic Model Formulations. Patient Prefer. Adherence 2021, 15, 863–870. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, R.K.; More, A.T. Some Aesthetic Considerations for over The-Counter (OTC) Pharmaceutical Products. Int. J. Biotechnol. 2010, 11, 267. [Google Scholar] [CrossRef]
- Bakhatwar, M.; Chikkala, S.R. Three Dimensional Printing in Pharmaceutical Technology—An Overview of Innovations. Innov. Pharm. Pharmacother. 2019, 7, 67–71. [Google Scholar]
- Boetker, J.; Water, J.J.; Aho, J.; Arnfast, L.; Bohr, A.; Rantanen, J. Modifying Release Characteristics from 3D Printed Drug-Eluting Products. Eur. J. Pharm. Sci. 2016, 90, 47–52. [Google Scholar] [CrossRef]
- Henry, S.; de Vadder, L.; Decorte, M.; Francia, S.; van Steenkiste, M.; Saevels, J.; Vanhoorne, V.; Vervaet, C. Development of a 3D-Printed Dosing Platform to Aid in Zolpidem Withdrawal Therapy. Pharmaceutics 2021, 13, 1684. [Google Scholar] [CrossRef]
- Lin, Y.; Huang, Y.; Cai, Z.B.; Wang, J. Accuracy Study of Tablet-Splitting. Chin. Pharm. J. 2013, 48, 193–197. [Google Scholar] [CrossRef]
- Watson, C.; Webb, E.A.; Kerr, S.; Davies, J.H.; Stirling, H.; Batchelor, H. How Close Is the Dose? Manipulation of 10 mg Hydrocortisone Tablets to Provide Appropriate Doses to Children. Int. J. Pharm. 2018, 545, 57–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rieder, M. If Children Ruled the Pharmaceutical Industry: The Need for Pediatric Formulations. Drug News Perspect. 2010, 23, 23. [Google Scholar] [CrossRef] [PubMed]
- Suárez-González, J.; Magariños-Triviño, M.; Díaz-Torres, E.; Cáceres-Pérez, A.R.; Santoveña-Estévez, A.; Fariña, J.B. Individualized Orodispersible Pediatric Dosage Forms Obtained by Molding and Semi-Solid Extrusion by 3D Printing: A Comparative Study for Hydrochlorothiazide. J. Drug Deliv. Sci. Technol. 2021, 66, 102884. [Google Scholar] [CrossRef]
- Quodbach, J.; Bogdahn, M.; Breitkreutz, J.; Chamberlain, R.; Eggenreich, K.; Elia, A.G.; Gottschalk, N.; Gunkel-Grabole, G.; Hoffmann, L.; Kapote, D.; et al. Quality of FDM 3D Printed Medicines for Pediatrics: Considerations for Formulation Development, Filament Extrusion, Printing Process and Printer Design. Ther. Innov. Regul. Sci. 2021, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Krause, J.; Müller, L.; Sarwinska, D.; Seidlitz, A.; Sznitowska, M.; Weitschies, W. 3D Printing of Mini Tablets for Pediatric Use. Pharmaceuticals 2021, 14, 143. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Size of 3D Printed Tablet | 6 mm | 8 mm | 10 mm |
|---|---|---|---|
| Swallowability | |||
| Participants aged 4–8 years able to swallow the placebo tablet | 7 (100%) | 3 (75%) | 2 (50%) |
| Participants aged 9–12 years able to swallow the placebo tablet | 1 (100%) | 6 (100%) | 7 (87.5%) |
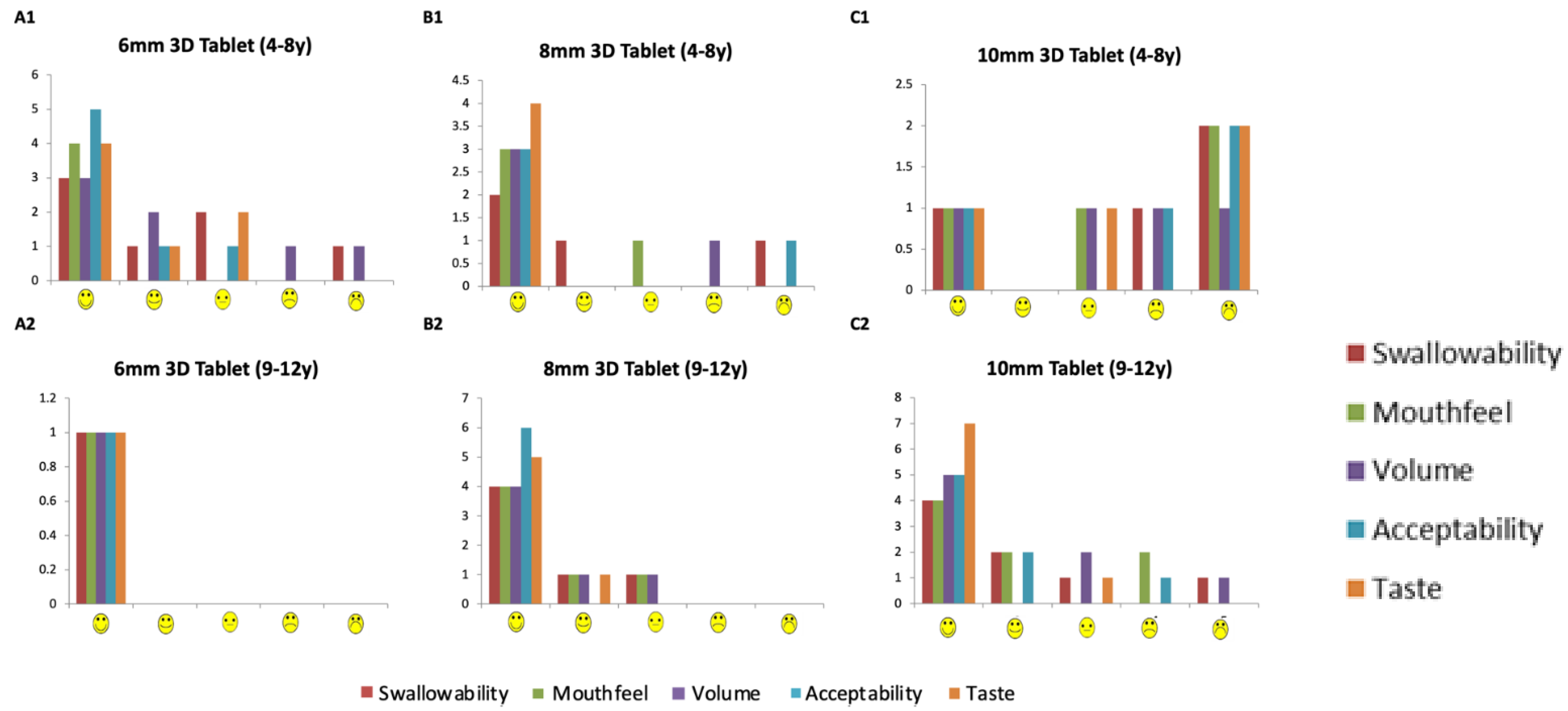
| Rated acceptable on a hedonic scale by participants aged 4–8 years | 6 (87.5%) | 3 (75%) | 1 (25%) |
| Rated acceptable on a hedonic scale by participants aged 9–12 years | 1 (100%) | 6 (100%) | 7 (87.5%) |
| Taste | |||
| Rated acceptable on a hedonic scale by participants aged 4–8 years | 7 (100%) | 4 (100%) | 2 (50%) |
| Rated acceptable on a hedonic scale by participants aged 9–12 years | 1 (100%) | 6 (100%) | 8 (100%) |
| The volume of water consumed to swallow each placebo tablet | |||
| Average volume of water (mL) required by participants aged 4–8 years ±SD, (range). | 27.4 ± 14.9 mL (5–48 mL) | 15.3 ± 11.8 mL (8–29 mL) | 71.5 ± 38.9 mL (44–99 mL) |
| Average volume of water (mL) required by participants aged 9–12 years | 9 mL † | 16.7 ± 5.8 mL (11–25 mL) | 34 ± 16.6 mL (20–59 mL) |
| Rated acceptable on hedonic scale by participants aged 4–8 years | 5 (71.4%) | 3 (75%) | 2 (50%) |
| Rated acceptable on hedonic scale by participants aged 9–12 years | 1 (100%) | 6 (100%) | 7 (87.5%) |
| Overall Acceptability 4–12 years | |||
| Rated acceptable on hedonic scale | 100% | 90% | 67% |
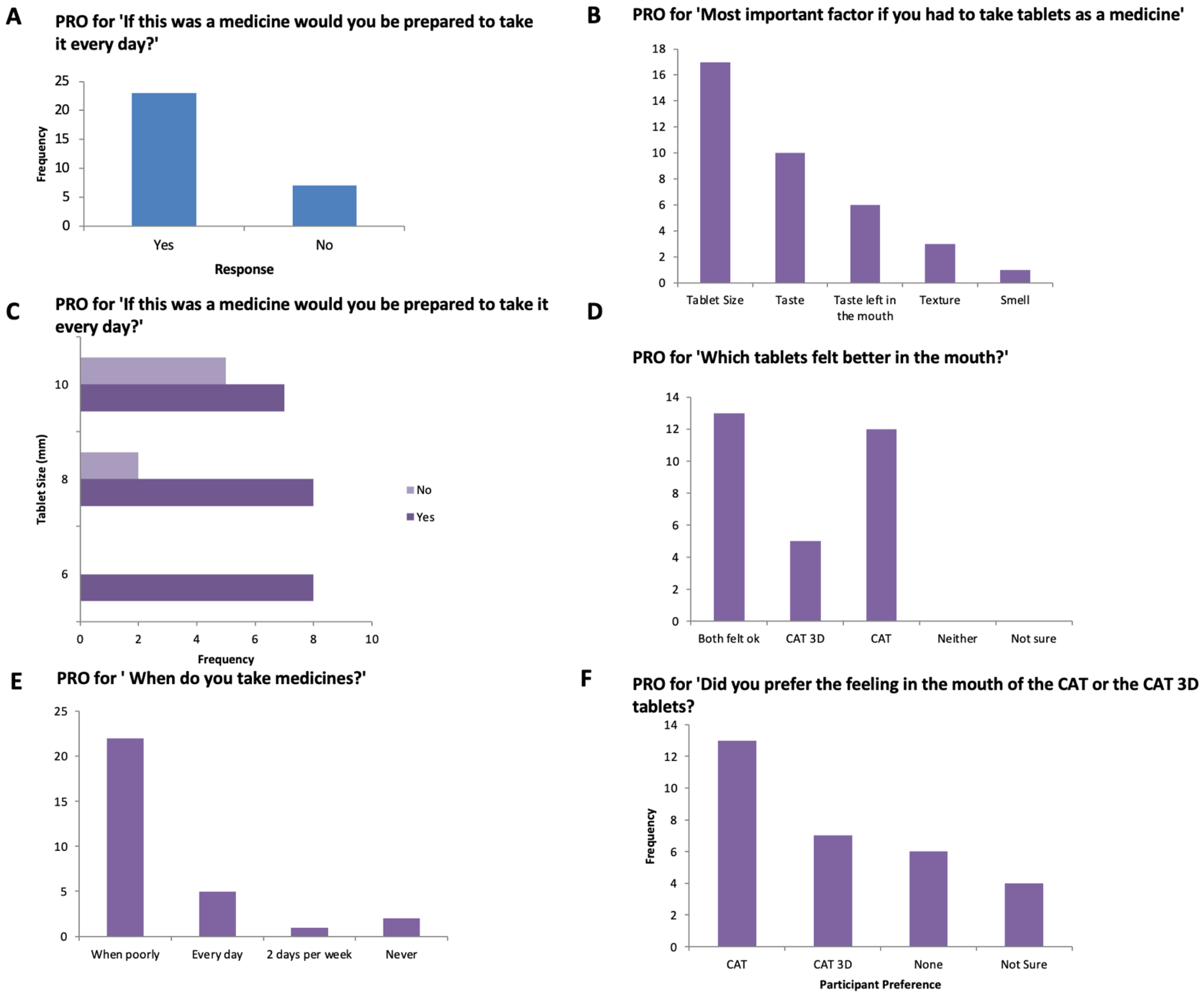
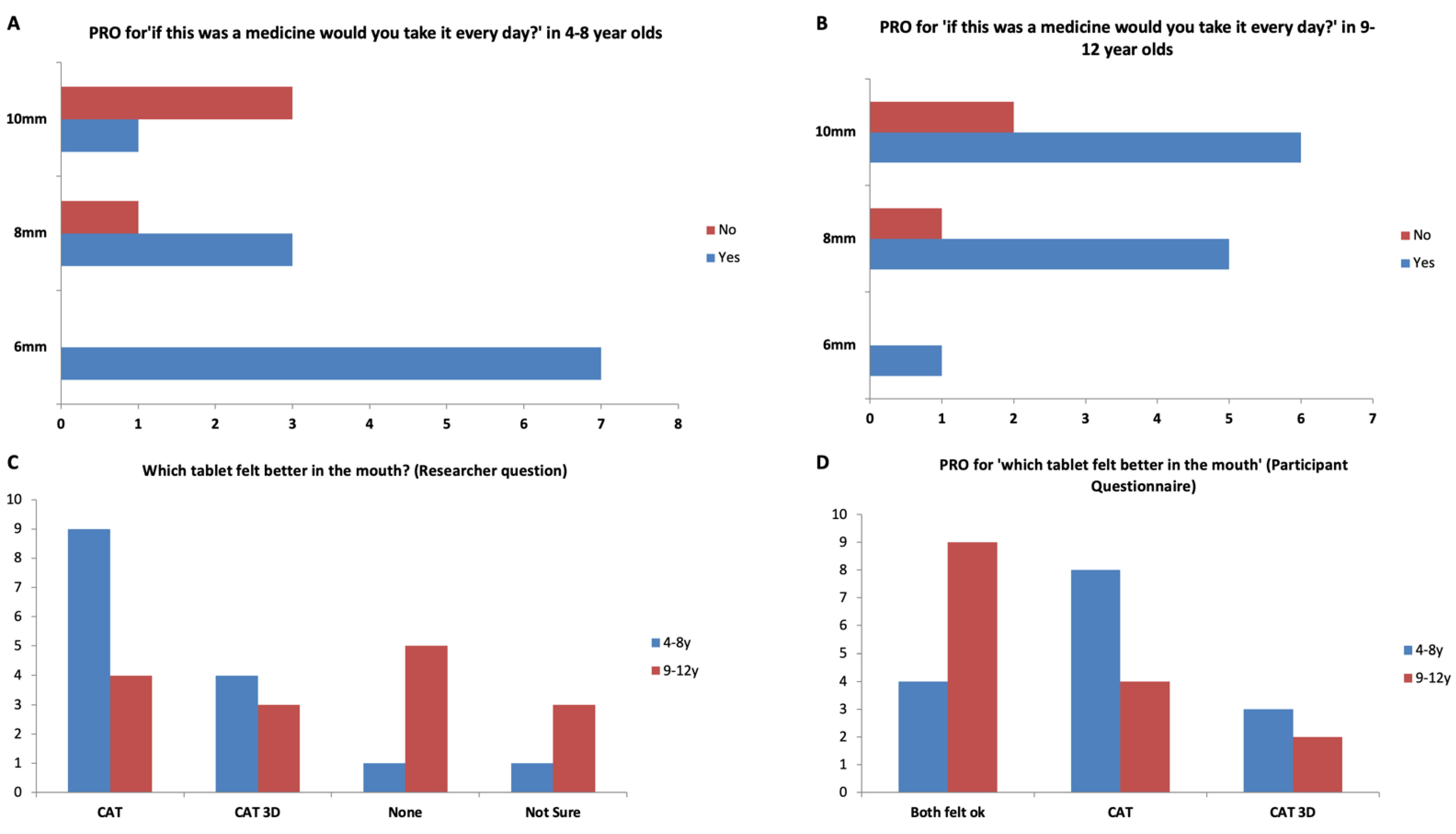
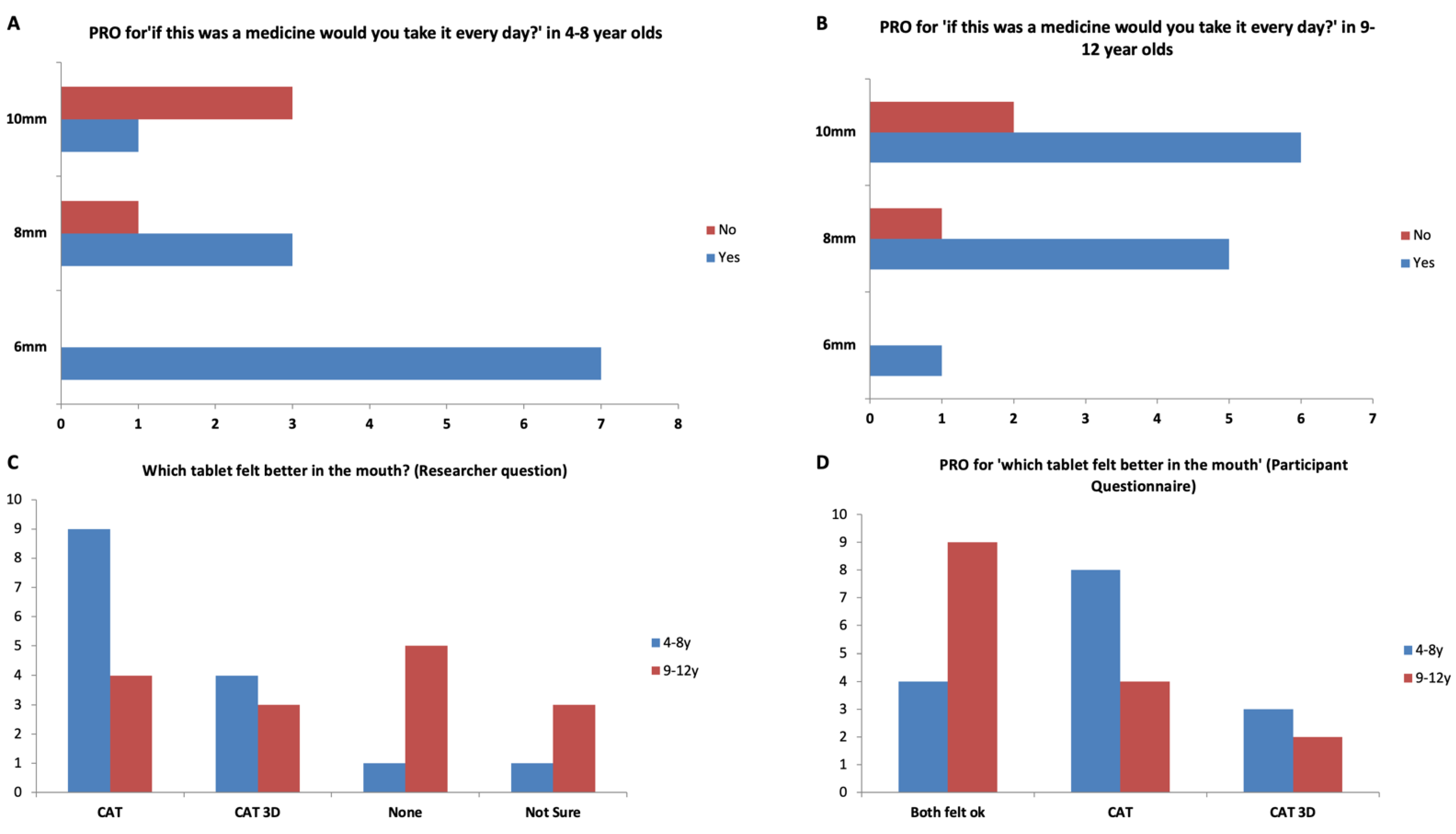
| Willing to take the placebo tablet every day if it was a medicine (participants aged 4–8 years) | 8/8 (100%) | 8/9 (89%) | 7/9 (77.8%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bracken, L.; Habashy, R.; McDonough, E.; Wilson, F.; Shakeshaft, J.; Ohia, U.; Garcia-Sorribes, T.; Isreb, A.; Alhnan, M.A.; Peak, M. Creating Acceptable Tablets 3D (CAT 3D): A Feasibility Study to Evaluate the Acceptability of 3D Printed Tablets in Children and Young People. Pharmaceutics 2022, 14, 516. https://doi.org/10.3390/pharmaceutics14030516
Bracken L, Habashy R, McDonough E, Wilson F, Shakeshaft J, Ohia U, Garcia-Sorribes T, Isreb A, Alhnan MA, Peak M. Creating Acceptable Tablets 3D (CAT 3D): A Feasibility Study to Evaluate the Acceptability of 3D Printed Tablets in Children and Young People. Pharmaceutics. 2022; 14(3):516. https://doi.org/10.3390/pharmaceutics14030516
Chicago/Turabian StyleBracken, Louise, Rober Habashy, Emma McDonough, Fiona Wilson, Joanne Shakeshaft, Udeme Ohia, Tamar Garcia-Sorribes, Abdullah Isreb, Mohamed A. Alhnan, and Matthew Peak. 2022. "Creating Acceptable Tablets 3D (CAT 3D): A Feasibility Study to Evaluate the Acceptability of 3D Printed Tablets in Children and Young People" Pharmaceutics 14, no. 3: 516. https://doi.org/10.3390/pharmaceutics14030516
APA StyleBracken, L., Habashy, R., McDonough, E., Wilson, F., Shakeshaft, J., Ohia, U., Garcia-Sorribes, T., Isreb, A., Alhnan, M. A., & Peak, M. (2022). Creating Acceptable Tablets 3D (CAT 3D): A Feasibility Study to Evaluate the Acceptability of 3D Printed Tablets in Children and Young People. Pharmaceutics, 14(3), 516. https://doi.org/10.3390/pharmaceutics14030516