A Novel Treatment Modality for Malignant Peripheral Nerve Sheath Tumor Using a Dual-Effect Liposome to Combine Photodynamic Therapy and Chemotherapy


Abstract
1. Introduction
2. Materials and Methods
2.1. Cell Lines
2.2. Preparation of PL-cDDP and PL-cDDP-Ce6
2.3. In Vitro Cytotoxicity of PL-cDDP-Ce6 against MPNST Cells
2.4. In Vivo Therapeutic Effect in Mice Bearing S462-TY Xenograft Tumor
2.5. Tissue Preparation for Histopathology, Complete Blood Cell Count, and Biochemical Analysis
2.6. ELISA of Soluble Axl Level
2.7. Statistics
3. Results
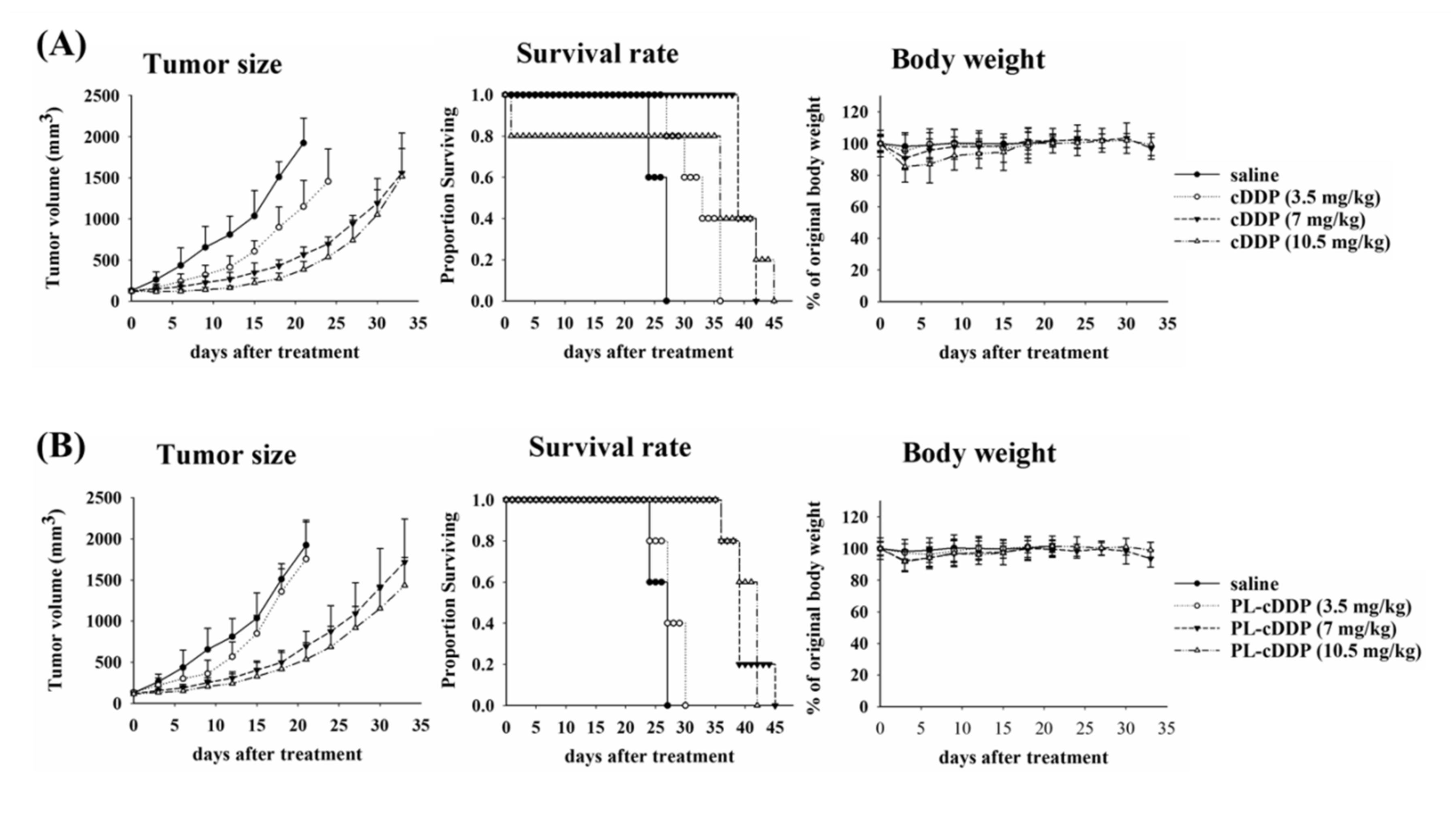
3.1. The Anti-Tumor Efficacy of Free-cDDP or PL-cDDP in S462TY Xenograft Mouse Model
3.2. The Cytotoxic Effect of PL-cDPP-Ce6 In Vitro against MPNST Cells
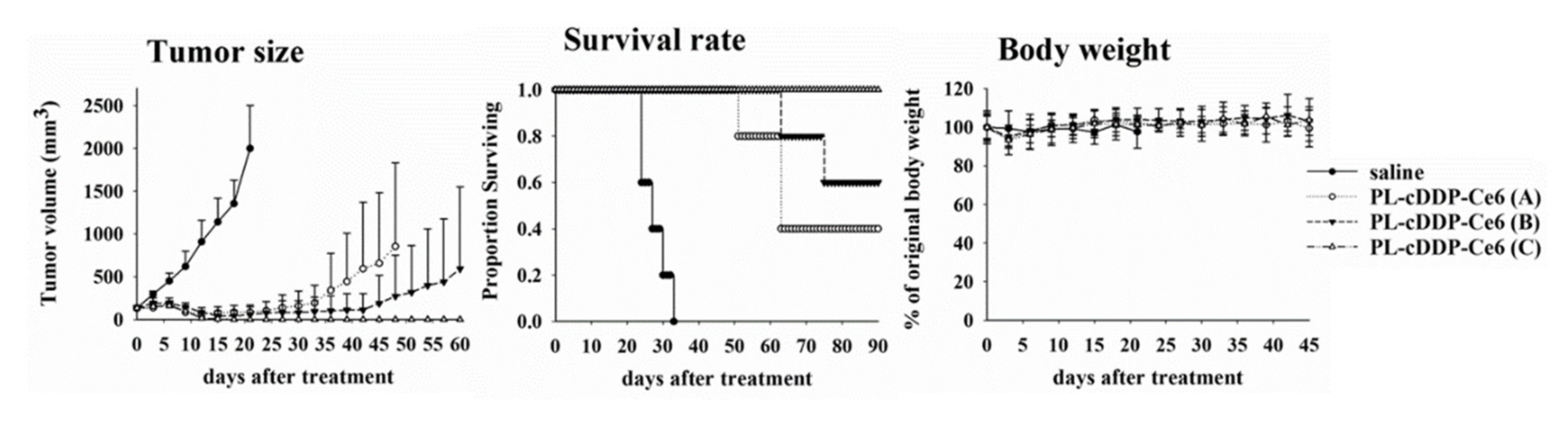
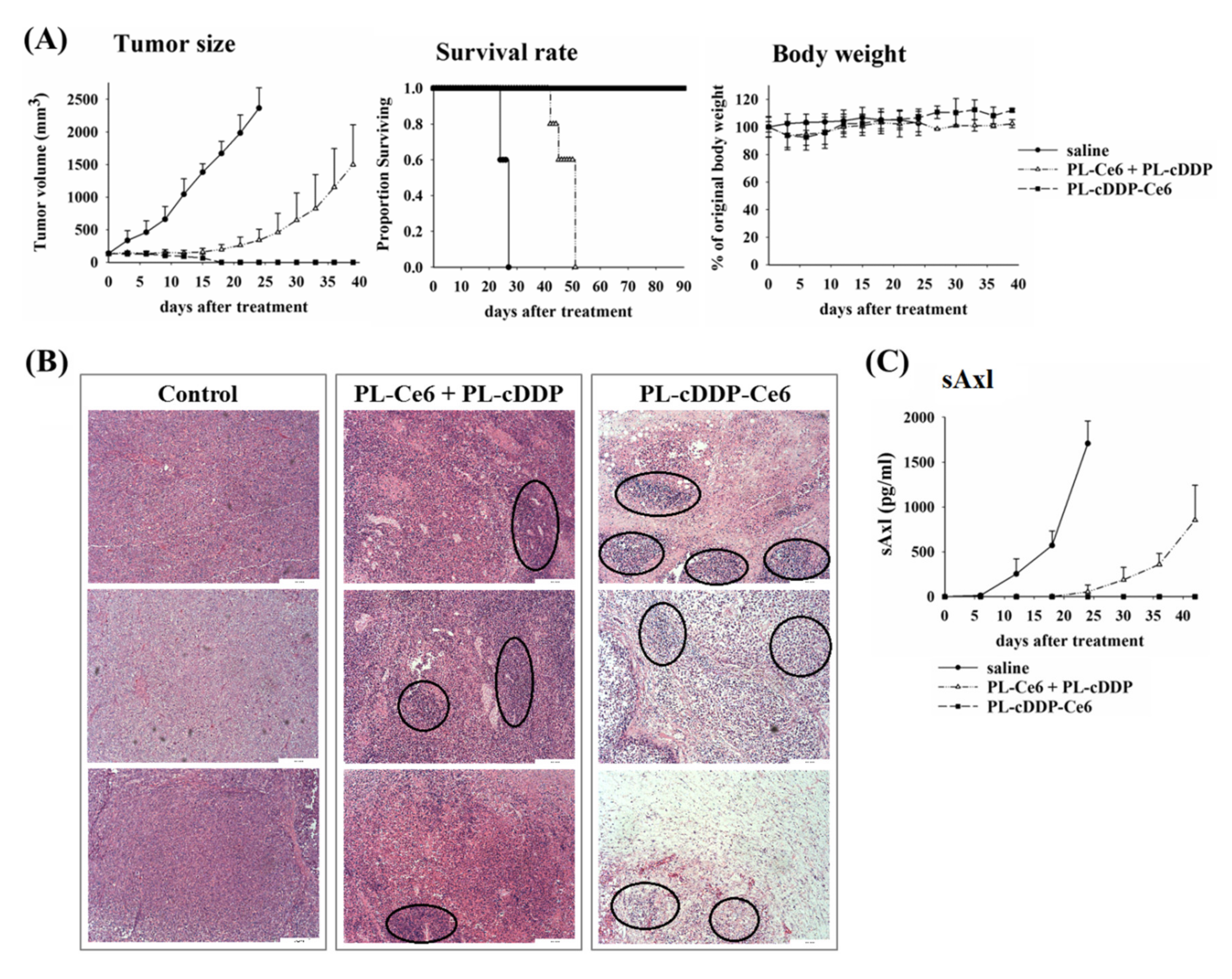
3.3. The Antitumor Efficacy of PL-cDPP-Ce6 In Vivo against S462TY Xenograft Tumor
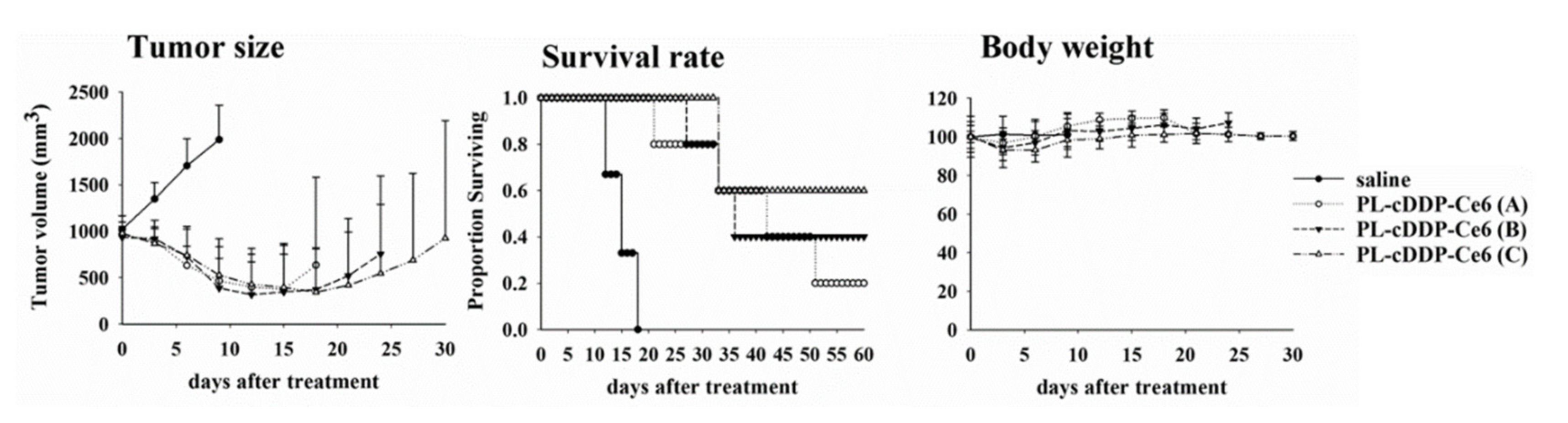
3.4. PL-cDDP-Ce6 Treatment for Larger MPNST Xenograft Tumor
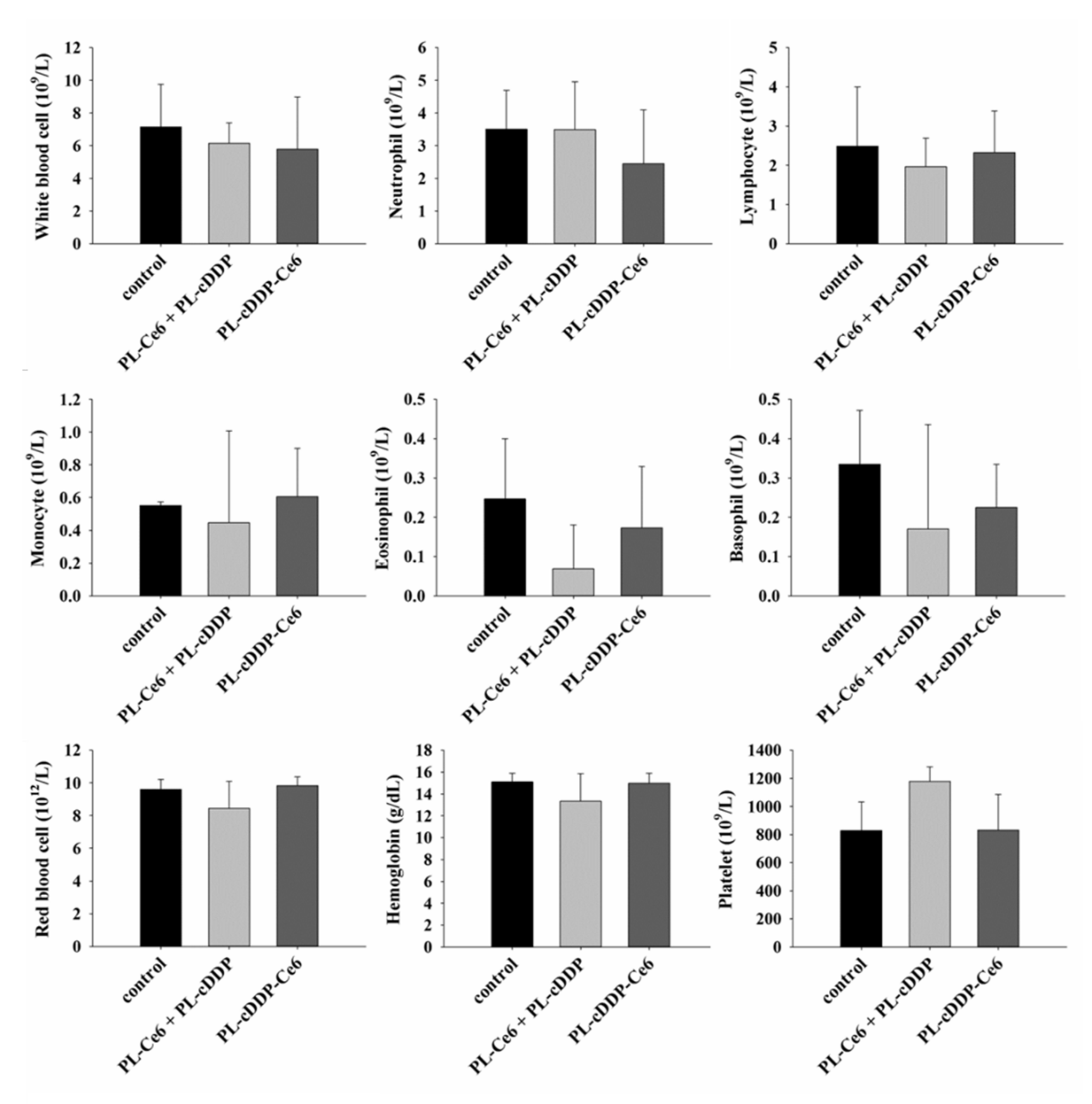
3.5. Safety Evaluation of PL-cDDP-Ce6
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Friedman, J.M. Neurofibromatosis: Phenotype, Natural History, and Pathogenesis, 3d ed.; Johns Hopkins University Press: Baltimore, MD, USA, 1999. [Google Scholar]
- Waggoner, D.J.; Towbin, J.; Gottesman, G.; Gutmann, D.H. Clinic-based study of plexiform neurofibromas in neurofibromatosis 1. Am. J. Med Genet. 2000, 92, 132–135. [Google Scholar] [CrossRef]
- Korf, B.R. Plexiform neurofibromas. Am. J. Med Genet. 1999, 89, 31–37. [Google Scholar] [CrossRef]
- Woodruff, J.M.; Selig, A.M.; Crowley, K.; Allen, P.W. Schwannoma (neurilemoma) with malignant transformation. A rare, distinctive peripheral nerve tumor. Am. J. Surg. Pathol. 1994, 18, 882–895. [Google Scholar] [CrossRef] [PubMed]
- Evans, D.G.; Baser, M.E.; McGaughran, J.; Sharif, S.; Howard, E.; Moran, A. Malignant peripheral nerve sheath tumours in neurofibromatosis 1. J. Med Genet. 2002, 39, 311–314. [Google Scholar] [CrossRef] [PubMed]
- Casali, P.G.; Jost, L.; Sleijfer, S.; Verweij, J.; Blay, J.Y.; Group, E.G.W. Soft tissue sarcomas: ESMO clinical recommendations for diagnosis, treatment and follow-up. Ann. Oncol. Off. J. Eur. Soc. Med Oncol. 2008, 19, ii89–ii93. [Google Scholar] [CrossRef]
- Kroep, J.R.; Ouali, M.; Gelderblom, H.; Le Cesne, A.; Dekker, T.J.; Van Glabbeke, M.; Hogendoorn, P.C.; Hohenberger, P. First-line chemotherapy for malignant peripheral nerve sheath tumor (MPNST) versus other histological soft tissue sarcoma subtypes and as a prognostic factor for MPNST: An EORTC soft tissue and bone sarcoma group study. Ann. Oncol. Off. J. Eur. Soc. Med Oncol. 2011, 22, 207–214. [Google Scholar] [CrossRef]
- Florea, A.M.; Busselberg, D. Cisplatin as an anti-tumor drug: Cellular mechanisms of activity, drug resistance and induced side effects. Cancers 2011, 3, 1351–1371. [Google Scholar] [CrossRef]
- Klippstein, T.H.; Mitrou, P.S.; Kochendorfer, K.J.; Bergmann, L. High-dose adriamycin (ADM) and cis-platinum (DDP) in advanced soft-tissue sarcomas and invasive thymomas. A pilot study. Cancer Chemother. Pharmacol. 1984, 13, 78–81. [Google Scholar] [CrossRef]
- Landy, H.; Feun, L.; Markoe, A.; Patchen, S.; Bruce, J.; Marcus, J.; Levi, A. Extended remission of a recurrent median nerve malignant peripheral nerve sheath tumor after multimodal treatment. Case report. J. Neurosurg. 2005, 103, 760–763. [Google Scholar] [CrossRef]
- Jung, H.I.; Lee, H.U.; Ahn, T.S.; Lee, J.E.; Lee, H.Y.; Cho, H.D.; Lee, S.C.; Bae, S.H. Primary hepatic malignant peripheral nerve sheath tumor successfully treated with combination therapy: A case report and literature review. Ann. Surg. Treat. Res 2016, 91, 327–331. [Google Scholar] [CrossRef]
- Zamboni, W.C.; Gervais, A.C.; Egorin, M.J.; Schellens, J.H.; Zuhowski, E.G.; Pluim, D.; Joseph, E.; Hamburger, D.R.; Working, P.K.; Colbern, G.; et al. Systemic and tumor disposition of platinum after administration of cisplatin or STEALTH liposomal-cisplatin formulations (SPI-077 and SPI-077 B103) in a preclinical tumor model of melanoma. Cancer Chemother. Pharmacol. 2004, 53, 329–336. [Google Scholar] [CrossRef] [PubMed]
- Wheate, N.J.; Walker, S.; Craig, G.E.; Oun, R. The status of platinum anticancer drugs in the clinic and in clinical trials. Dalton Trans. 2010, 39, 8113–8127. [Google Scholar] [CrossRef] [PubMed]
- Bandak, S.; Goren, D.; Horowitz, A.; Tzemach, D.; Gabizon, A. Pharmacological studies of cisplatin encapsulated in long-circulating liposomes in mouse tumor models. Anticancer Drugs 1999, 10, 911–920. [Google Scholar] [CrossRef] [PubMed]
- Dolmans, D.E.; Fukumura, D.; Jain, R.K. Photodynamic therapy for cancer. Nat. Rev. Cancer 2003, 3, 380–387. [Google Scholar] [CrossRef] [PubMed]
- Dougherty, T.J.; Gomer, C.J.; Henderson, B.W.; Jori, G.; Kessel, D.; Korbelik, M.; Moan, J.; Peng, Q. Photodynamic therapy. J. Natl. Cancer Inst. 1998, 90, 889–905. [Google Scholar] [CrossRef]
- Abbas, S.; Jerjes, W.; Upile, T.; Vaz, F.; Hopper, C. The palliative role of PDT in recurrent advanced nasopharyngeal carcinoma: Case series. Photodiagnosis Photodyn. Ther. 2012, 9, 142–147. [Google Scholar] [CrossRef]
- Wildeman, M.A.; Nyst, H.J.; Karakullukcu, B.; Tan, B.I. Photodynamic therapy in the therapy for recurrent/persistent nasopharyngeal cancer. Head Neck Oncol. 2009, 1, 40. [Google Scholar] [CrossRef][Green Version]
- Jerjes, W.; Upile, T.; Alexander Mosse, C.; Hamdoon, Z.; Morcos, M.; Morley, S.; Hopper, C. Prospective evaluation of 110 patients following ultrasound-guided photodynamic therapy for deep seated pathologies. Photodiagnosis Photodyn. Ther. 2011, 8, 297–306. [Google Scholar] [CrossRef]
- Jerjes, W.; Upile, T.; Hamdoon, Z.; Mosse, C.A.; Akram, S.; Morley, S.; Hopper, C. Interstitial PDT for vascular anomalies. Lasers Surg. Med. 2011, 43, 357–365. [Google Scholar] [CrossRef]
- Shah, P.; Jerjes, W.; Upile, T.; Hopper, C. The effective management of a leg hemangioma using ultrasound-guided interstitial photodynamic therapy. Photodiagnosis Photodyn. Ther. 2010, 7, 201–203. [Google Scholar] [CrossRef]
- Gomer, C.J.; Rucker, N.; Ferrario, A.; Wong, S. Properties and applications of photodynamic therapy. Radiat. Res. 1989, 120, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Peng, P.C.; Hong, R.L.; Tsai, Y.J.; Li, P.T.; Tsai, T.; Chen, C.T. Dual-effect liposomes encapsulated with doxorubicin and chlorin e6 augment the therapeutic effect of tumor treatment. Lasers Surg. Med. 2015, 47, 77–87. [Google Scholar] [CrossRef] [PubMed]
- Peng, P.C.; Hong, R.L.; Tsai, T.; Chen, C.T. Co-Encapsulation of Chlorin e6 and Chemotherapeutic Drugs in a PEGylated Liposome Enhance the Efficacy of Tumor Treatment: Pharmacokinetics and Therapeutic Efficacy. Pharmaceutics 2019, 11, 617. [Google Scholar] [CrossRef]
- Johansson, G.; Peng, P.C.; Huang, P.Y.; Chien, H.F.; Hua, K.T.; Kuo, M.L.; Chen, C.T.; Lee, M.J. Soluble AXL: A possible circulating biomarker for neurofibromatosis type 1 related tumor burden. PLoS ONE 2014, 9, e115916. [Google Scholar] [CrossRef] [PubMed]
- Johansson, G.; Mahller, Y.Y.; Collins, M.H.; Kim, M.O.; Nobukuni, T.; Perentesis, J.; Cripe, T.P.; Lane, H.A.; Kozma, S.C.; Thomas, G.; et al. Effective in vivo targeting of the mammalian target of rapamycin pathway in malignant peripheral nerve sheath tumors. Mol. Cancer Ther. 2008, 7, 1237–1245. [Google Scholar] [CrossRef] [PubMed]
- Miller, S.J.; Rangwala, F.; Williams, J.; Ackerman, P.; Kong, S.; Jegga, A.G.; Kaiser, S.; Aronow, B.J.; Frahm, S.; Kluwe, L.; et al. Large-scale molecular comparison of human schwann cells to malignant peripheral nerve sheath tumor cell lines and tissues. Cancer Res. 2006, 66, 2584–2591. [Google Scholar] [CrossRef]
- Mahller, Y.Y.; Vaikunth, S.S.; Ripberger, M.C.; Baird, W.H.; Saeki, Y.; Cancelas, J.A.; Crombleholme, T.M.; Cripe, T.P. Tissue inhibitor of metalloproteinase-3 via oncolytic herpesvirus inhibits tumor growth and vascular progenitors. Cancer Res. 2008, 68, 1170–1179. [Google Scholar] [CrossRef]
- Carli, M.; Ferrari, A.; Mattke, A.; Zanetti, I.; Casanova, M.; Bisogno, G.; Cecchetto, G.; Alaggio, R.; De Sio, L.; Koscielniak, E.; et al. Pediatric malignant peripheral nerve sheath tumor: The Italian and German soft tissue sarcoma cooperative group. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2005, 23, 8422–8430. [Google Scholar] [CrossRef]
- Hamdoon, Z.; Jerjes, W.; Al-Delayme, R.; Hopper, C. Solitary giant neurofibroma of the neck subjected to photodynamic therapy: Case study. Head Neck Oncol. 2012, 4, 30. [Google Scholar] [CrossRef]
- Edmonson, J.H.; Ryan, L.M.; Blum, R.H.; Brooks, J.S.; Shiraki, M.; Frytak, S.; Parkinson, D.R. Randomized comparison of doxorubicin alone versus ifosfamide plus doxorubicin or mitomycin, doxorubicin, and cisplatin against advanced soft tissue sarcomas. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 1993, 11, 1269–1275. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control | PL-Ce6 + PL-cDDP | PL-cDDP-Ce6 | |
|---|---|---|---|
| AST (U/l) | 86.7 ± 36.7 | 142.3 ± 93.9 | 173.7 ± 125.4 |
| ALT (U/l) | 39.7 ± 26.1 | 21.7 ± 4.0 | 40.3 ± 25.7 |
| CPK (U/l) | 144.3 ± 18.5 | 151.7 ± 59.5 | 161.3 ± 70.9 |
| LDH (U/l) | 1110.0 ± 211.7 | 3816.7 ± 3041.8 | 2933.3 ± 1325.1 |
| BUN (mg/dL) | 23.23 ± 2.89 | 22.43 ± 5.16 | 23.93 ± 2.15 |
| CRE (mg/dL) | 0.10 ± 0.00 | 0.37 ± 0.25 | 0.13 ± 0.06 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, C.-T.; Peng, P.-C.; Tsai, T.; Chien, H.-F.; Lee, M.-J. A Novel Treatment Modality for Malignant Peripheral Nerve Sheath Tumor Using a Dual-Effect Liposome to Combine Photodynamic Therapy and Chemotherapy. Pharmaceutics 2020, 12, 317. https://doi.org/10.3390/pharmaceutics12040317
Chen C-T, Peng P-C, Tsai T, Chien H-F, Lee M-J. A Novel Treatment Modality for Malignant Peripheral Nerve Sheath Tumor Using a Dual-Effect Liposome to Combine Photodynamic Therapy and Chemotherapy. Pharmaceutics. 2020; 12(4):317. https://doi.org/10.3390/pharmaceutics12040317
Chicago/Turabian StyleChen, Chin-Tin, Po-Chun Peng, Tsuimin Tsai, Hsiung-Fei Chien, and Ming-Jen Lee. 2020. "A Novel Treatment Modality for Malignant Peripheral Nerve Sheath Tumor Using a Dual-Effect Liposome to Combine Photodynamic Therapy and Chemotherapy" Pharmaceutics 12, no. 4: 317. https://doi.org/10.3390/pharmaceutics12040317
APA StyleChen, C.-T., Peng, P.-C., Tsai, T., Chien, H.-F., & Lee, M.-J. (2020). A Novel Treatment Modality for Malignant Peripheral Nerve Sheath Tumor Using a Dual-Effect Liposome to Combine Photodynamic Therapy and Chemotherapy. Pharmaceutics, 12(4), 317. https://doi.org/10.3390/pharmaceutics12040317