

Multiscale Modeling of Hospital Length of Stay for Successive SARS-CoV-2 Variants: A Multi-State Forecasting Framework



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
- Derive phase-specific LoS distributions and quantify how age modifies these durations;
- Estimate time-dependent probabilities for transitions to critical care, discharge, or death, providing a direct interface for bed-availability alert systems;
- Assess parameter identifiability and stability given a moderate sample size;
- Demonstrate that variant- and age-adaptive estimations of LoS parameters yield accurate projections of ward- and ICU-specific demand in different epidemic contexts.
2. Data and Methods
2.1. Data
2.2. Gamma Distribution
2.3. Probabilistic Transition Model
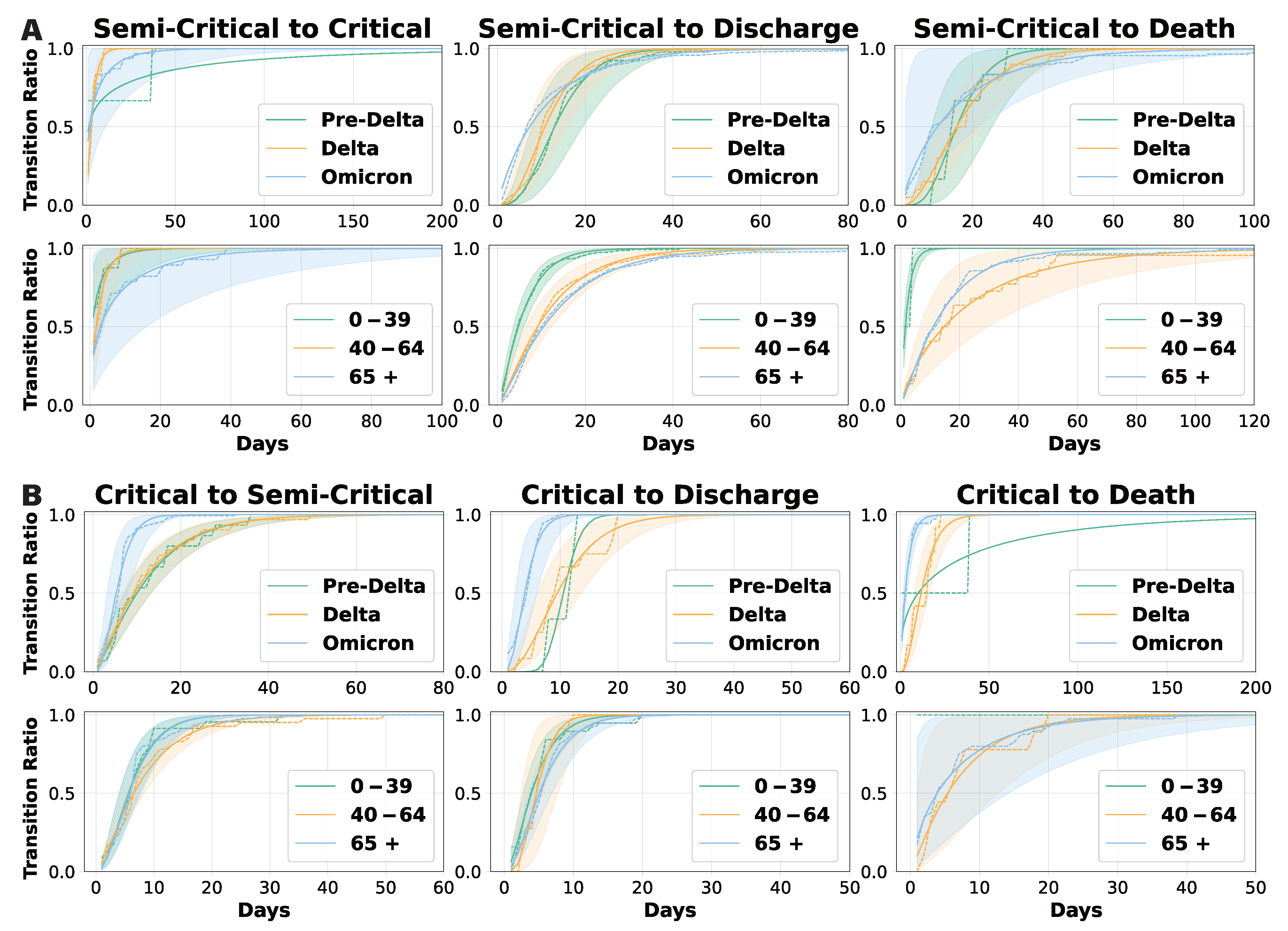
- Upon admission, a patient is placed in either a semi-critical ward (M) or a critical ward (C).
- If the patient recovers, they transition to the discharged state (D), which is an absorbing state with no further transitions.
- If the patient’s condition deteriorates to death, they transition to the death state (X), another absorbing state.
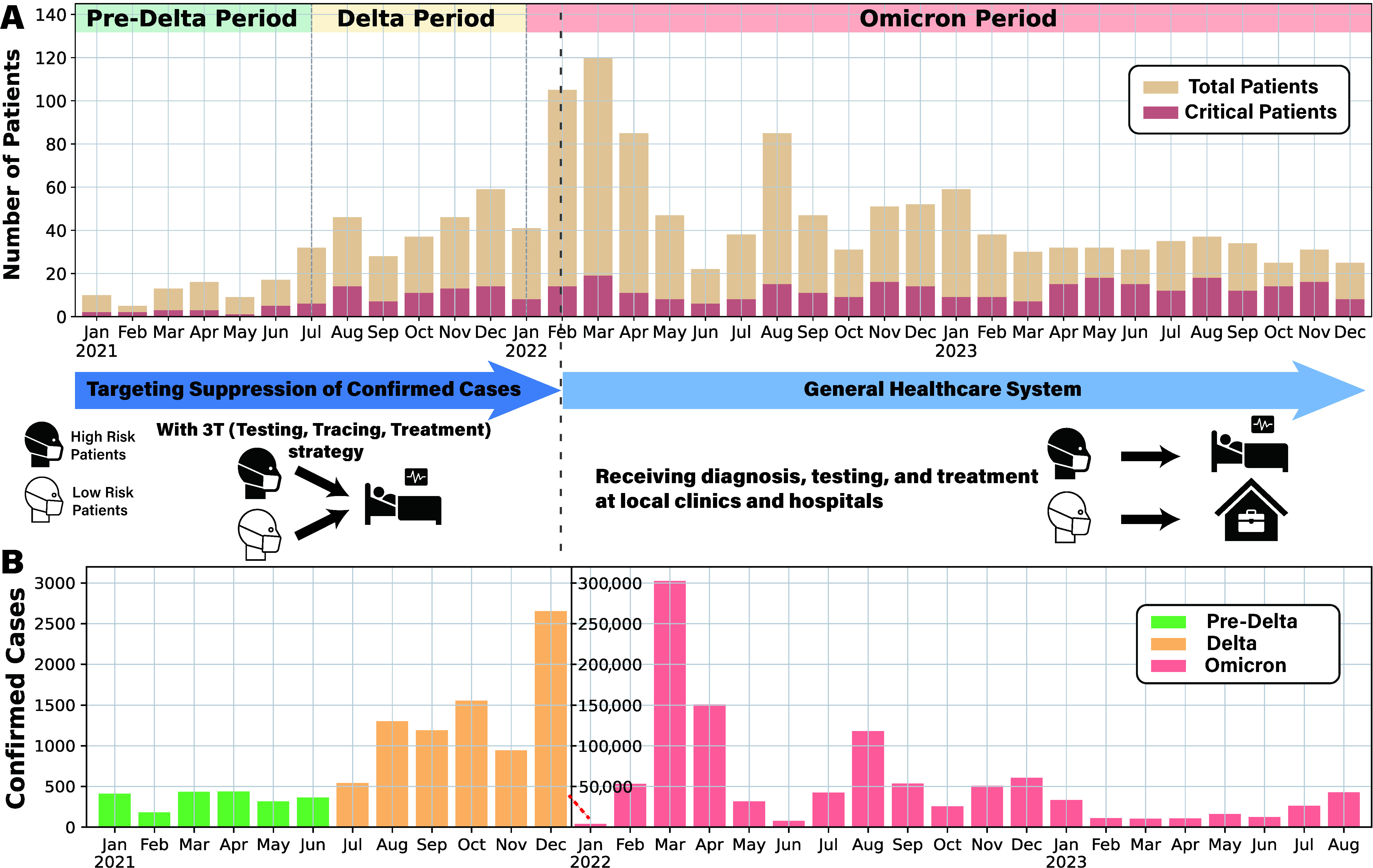
- Epidemic waves: Pre-Delta, Delta, and Omicron, denoted as w.
- Age groups: 0–39, 40–64, and 65+, denoted as a.
- State transitions: Represented as k.
3. Results
3.1. Data Analysis
3.2. Daily Transition Probability Analysis
3.3. Model-Based Analysis of Hospital Length of Stay
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. WHO Coronavirus Disease (COVID-19) Dashboard. 2020. Available online: https://covid19.who.int/ (accessed on 1 May 2025).
- World Health Organization. Novel Coronavirus (2019-nCoV): Situation Report 3; Technical Report; World Health Organization: Geneve, Switzerland, 2020. [Google Scholar]
- Ministry of Health and Welfare, Central Disaster and Safety Countermeasures Headquarters. COVID-19: Changes in Infectious Disease Response Over the Past 3 Years; Ministry of Health and Welfare (MOHW): Seoul, Republic of Korea, 2023. [Google Scholar]
- Gonçalves-Bradley, D.C.; Lannin, N.A.; Clemson, L.; Cameron, I.D.; Shepperd, S. Discharge planning from hospital. Cochrane Database Syst. Rev. 2022, 1, CD000313. [Google Scholar] [CrossRef]
- Bottle, A.; Middleton, S.; Kalkman, C.J.; Livingston, E.H.; Aylin, P. Global comparators project: International comparison of hospital outcomes using administrative data. Health Serv. Res. 2013, 48, 2081–2100. [Google Scholar] [CrossRef] [PubMed]
- Iwamoto, S.; Muhar, B.K.; Chen, H.; Chu, H.; Johnstone, M.; Sidhu, A.; Chu, H.; Fischer, J.; Chu, G. Different COVID-19 treatments’ impact on hospital length of stay. Eur. J. Med. Res. 2023, 28, 218. [Google Scholar] [CrossRef] [PubMed]
- Alimohamadi, Y.; Sepandi, M.; Dadgar, A.; Nezhad, H.S.; Mosaed, R.; Jame, S.Z.B. Hospital length of stay among COVID-19 patients: An application of competing risk analysis. J. Biostat. Epidemiol. 2021, 7, 224–234. [Google Scholar] [CrossRef]
- Larson, M.G.; Dinse, G.E. A mixture model for the regression analysis of competing risks data. J. R. Stat. Soc. Ser. C (Appl. Stat.) 1985, 34, 201–211. [Google Scholar] [CrossRef]
- Faddy, M.; Graves, N.; Pettitt, A. Modeling length of stay in hospital and other right skewed data: Comparison of phase-type, gamma and log-normal distributions. Value Health 2009, 12, 309–314. [Google Scholar] [CrossRef]
- Mahboub, B.; Bataineh, M.T.A.; Alshraideh, H.; Hamoudi, R.; Salameh, L.; Shamayleh, A. Prediction of COVID-19 hospital length of stay and risk of death using artificial intelligence-based modeling. Front. Med. 2021, 8, 592336. [Google Scholar] [CrossRef]
- Clark, D.E.; Ostrander, K.R.; Cushing, B.M. A multistate model predicting mortality, length of stay, and readmission for surgical patients. Health Serv. Res. 2016, 51, 1074–1094. [Google Scholar] [CrossRef]
- Tobin, R.J.; Wood, J.G.; Jayasundara, D.; Sara, G.; Walker, C.R.; Martin, G.E.; McCaw, J.M.; Shearer, F.M.; Price, D.J. Real-time analysis of hospital length of stay in a mixed SARS-CoV-2 Omicron and Delta epidemic in New South Wales, Australia. BMC Infect. Dis. 2023, 23, 28. [Google Scholar] [CrossRef]
- Grosso, F.M.; Presanis, A.M.; Kunzmann, K.; Jackson, C.; Corbella, A.; Grasselli, G.; Andreassi, A.; Bodina, A.; Gramegna, M.; Castaldi, S.; et al. Decreasing hospital burden of COVID-19 during the first wave in Regione Lombardia: An emergency measures context. BMC Public Health 2021, 21, 1612. [Google Scholar]
- Taylor, S.L.; Sen, S.; Greenhalgh, D.G.; Lawless, M.; Curri, T.; Palmieri, T.L. A competing risk analysis for hospital length of stay in patients with burns. JAMA Surg. 2015, 150, 450–456. [Google Scholar] [CrossRef]
- Kociurzynski, R.; D’Ambrosio, A.; Papathanassopoulos, A.; Bürkin, F.; Hertweck, S.; Eichel, V.M.; Heininger, A.; Liese, J.; Mutters, N.T.; Peter, S.; et al. Forecasting local hospital bed demand for COVID-19 using on-request simulations. Sci. Rep. 2023, 13, 21321. [Google Scholar] [CrossRef]
- Capistran, M.A.; Capella, A.; Christen, J.A. Forecasting hospital demand in metropolitan areas during the current COVID-19 pandemic and estimates of lockdown-induced 2nd waves. PLoS ONE 2021, 16, e0245669. [Google Scholar] [CrossRef] [PubMed]
- Jackson, C.H.; Tom, B.D.; Kirwan, P.D.; Mandal, S.; Seaman, S.R.; Kunzmann, K.; Presanis, A.M.; De Angelis, D. A comparison of two frameworks for multi-state modelling, applied to outcomes after hospital admissions with COVID-19. Stat. Methods Med. Res. 2022, 31, 1656–1674. [Google Scholar] [CrossRef] [PubMed]
- Keogh, R.H.; Diaz-Ordaz, K.; Jewell, N.P.; Semple, M.G.; De Wreede, L.C.; Putter, H.; Investigators, I. Estimating distribution of length of stay in a multi-state model conditional on the pathway, with an application to patients hospitalised with Covid-19. Lifetime Data Anal. 2023, 29, 288–317. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.S.; Min, H.S.; Moon, J.Y.; Lim, D.; Kim, Y.; Ko, E.; Kim, Y.S.; Kim, J.; Lee, J.; Sung, H.K. Patient and hospital characteristics predict prolonged emergency department length of stay and in-hospital mortality: A nationwide analysis in Korea. BMC Emerg. Med. 2022, 22, 183. [Google Scholar] [CrossRef]
- Kim, J.S.; Seo, D.W.; Kim, Y.J.; Jeong, J.; Kang, H.; Han, K.S.; Kim, S.J.; Lee, S.W.; Ahn, S.; Kim, W.Y. Prolonged length of stay in the emergency department and increased risk of in-hospital cardiac arrest: A nationwide population-based study in South Korea, 2016–2017. J. Clin. Med. 2020, 9, 2284. [Google Scholar] [CrossRef]
- Buttigieg, S.C.; Abela, L.; Pace, A. Variables affecting hospital length of stay: A scoping review. J. Health Organ. Manag. 2018, 32, 463–493. [Google Scholar] [CrossRef]
- Hu, Z.; Huang, X.; Zhang, J.; Fu, S.; Ding, D.; Tao, Z. Differences in clinical characteristics between delta variant and wild-type SARS-CoV-2 infected patients. Front. Med. 2022, 8, 792135. [Google Scholar] [CrossRef]
- Guo, Y.; Han, J.; Zhang, Y.; He, J.; Yu, W.; Zhang, X.; Wu, J.; Zhang, S.; Kong, Y.; Guo, Y.; et al. SARS-CoV-2 omicron variant: Epidemiological features, biological characteristics, and clinical significance. Front. Immunol. 2022, 13, 877101. [Google Scholar] [CrossRef]
- Davies, N.G.; Klepac, P.; Liu, Y.; Prem, K.; Jit, M.; Eggo, R.M. Age-dependent effects in the transmission and control of COVID-19 epidemics. Nat. Med. 2020, 26, 1205–1211. [Google Scholar] [CrossRef] [PubMed]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.; Buis, K.; Zhao, X. A comprehensive toolbox for the gamma distribution: The gammadist package. J. Qual. Technol. 2023, 55, 75–87. [Google Scholar] [CrossRef]
- Murata, A.; Watanabe, S.I.I.; Sasaki, H.; Kawase, H.; Nosaka, M. Assessing Goodness of Fit to a Gamma Distribution and Estimating Future Projection on Daily Precipitation Frequency Using Regional Climate Model Simulations over Japan with and without the Influence of Tropical Cyclones. J. Hydrometeorol. 2020, 21, 2997–3010. [Google Scholar] [CrossRef]
- Virtanen, P.; Gommers, R.; Oliphant, T.E.; Haberland, M.; Reddy, T.; Cournapeau, D.; Burovski, E.; Peterson, P.; Weckesser, W.; Bright, J.; et al. SciPy 1.0: Fundamental Algorithms for Scientific Computing in Python. Nat. Methods 2020, 17, 261–272. [Google Scholar] [CrossRef]
- Vugrin, K.W.; Swiler, L.P.; Roberts, R.M.; Stucky-Mack, N.J.; Sullivan, S.P. Confidence region estimation techniques for nonlinear regression in groundwater flow: Three case studies. Water Resour. Res. 2007, 43. [Google Scholar] [CrossRef]
- Moré, J.J. The Levenberg-Marquardt algorithm: Implementation and theory. In Proceedings of the Numerical Analysis: Proceedings of the Biennial Conference, Dundee, UK, 28 June–1 July 1977; Springer: Berlin/Heidelberg, Germany, 2006; pp. 105–116. [Google Scholar]
- Prentice, R.L.; Kalbfleisch, J.D.; Peterson Jr, A.V.; Flournoy, N.; Farewell, V.T.; Breslow, N.E. The analysis of failure times in the presence of competing risks. Biometrics 1978, 34, 541–554. [Google Scholar] [CrossRef]
- Andersen, P.K.; Keiding, N. Multi-state models for event history analysis. Stat. Methods Med. Res. 2002, 11, 91–115. [Google Scholar] [CrossRef] [PubMed]
- Kalbfleisch, J.D.; Prentice, R.L. The Statistical Analysis of Failure Time Data; John Wiley & Sons: Hoboken, NJ, USA, 2002. [Google Scholar]
- Carpenter, J.; Bithell, J. Bootstrap confidence intervals: When, which, what? A practical guide for medical statisticians. Stat. Med. 2000, 19, 1141–1164. [Google Scholar] [CrossRef]
- Reingruber, J.; Papale, A.; Ruckly, S.; Timsit, J.F.; Holcman, D. Data-driven multiscale dynamical framework to control a pandemic evolution with non-pharmaceutical interventions. PLoS ONE 2023, 18, e0278882. [Google Scholar] [CrossRef]
- Seong, H.; Hyun, H.J.; Yun, J.G.; Noh, J.Y.; Cheong, H.J.; Kim, W.J.; Song, J.Y. Comparison of the second and third waves of the COVID-19 pandemic in South Korea: Importance of early public health intervention. Int. J. Infect. Dis. 2021, 104, 742–745. [Google Scholar] [CrossRef] [PubMed]
- Modes, M.E.; Directo, M.P.; Melgar, M.; Johnson, L.R.; Yang, H.; Chaudhary, P.; Bartolini, S.; Isonaka, S.; Chen, P. Clinical Characteristics and Outcomes Among Adults Hospitalized with Laboratory-Confirmed SARS-CoV-2 Infection During Periods of B.1.617.2 (Delta) and B.1.1.529 (Omicron) Variant Predominance—One Hospital, California, July 15–September 23, 2021, and December 21, 2021–January 27, 2022. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 217–223. [Google Scholar] [PubMed]
- Alimohamadi, Y.; Yekta, E.M.; Sepandi, M.; Sharafoddin, M.; Arshadi, M.; Hesari, E. Hospital length of stay for COVID-19 patients: A systematic review and meta-analysis. Multidiscip. Respir. Med. 2022, 17, 856. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Xue, L.; Legido-Quigley, H.; Khan, M.; Wu, H.; Peng, X.; Li, X.; Li, P. Understanding factors influencing the length of hospital stay among non-severe COVID-19 patients: A retrospective cohort study in a Fangcang shelter hospital. PLoS ONE 2020, 15, e0240959. [Google Scholar] [CrossRef]
- Grasselli, G.; Pesenti, A.; Cecconi, M. Critical care utilization for the COVID-19 outbreak in Lombardy, Italy: Early experience and forecast during an emergency response. JAMA 2020, 323, 1545–1546. [Google Scholar] [CrossRef]
- Murthy, S.; Gomersall, C.D.; Fowler, R.A. Care for critically ill patients with COVID-19. JAMA 2020, 323, 1499–1500. [Google Scholar] [CrossRef]
- Preiss, A.; Hadley, E.; Jones, K.; Stoner, M.C.; Kery, C.; Baumgartner, P.; Bobashev, G.; Tenenbaum, J.; Carter, C.; Clement, K.; et al. Incorporation of near-real-time hospital occupancy data to improve hospitalization forecast accuracy during the COVID-19 pandemic. Infect. Dis. Model. 2022, 7, 277–285. [Google Scholar] [CrossRef]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus–infected pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef]
- Parker, F.; Martínez, D.A.; Scheulen, J.; Ghobadi, K. An Interactive Decision-Support Dashboard for Optimal Hospital Capacity Management. arXiv 2024, arXiv:2403.15634. [Google Scholar]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, M.; Kim, J.; Kim, H.; Tobin, R.J.; Lee, S. Multiscale Modeling of Hospital Length of Stay for Successive SARS-CoV-2 Variants: A Multi-State Forecasting Framework. Viruses 2025, 17, 953. https://doi.org/10.3390/v17070953
Choi M, Kim J, Kim H, Tobin RJ, Lee S. Multiscale Modeling of Hospital Length of Stay for Successive SARS-CoV-2 Variants: A Multi-State Forecasting Framework. Viruses. 2025; 17(7):953. https://doi.org/10.3390/v17070953
Chicago/Turabian StyleChoi, Minchan, Jungeun Kim, Heesung Kim, Ruarai J. Tobin, and Sunmi Lee. 2025. "Multiscale Modeling of Hospital Length of Stay for Successive SARS-CoV-2 Variants: A Multi-State Forecasting Framework" Viruses 17, no. 7: 953. https://doi.org/10.3390/v17070953
APA StyleChoi, M., Kim, J., Kim, H., Tobin, R. J., & Lee, S. (2025). Multiscale Modeling of Hospital Length of Stay for Successive SARS-CoV-2 Variants: A Multi-State Forecasting Framework. Viruses, 17(7), 953. https://doi.org/10.3390/v17070953