
Dynamics of Clinical, Radiological, and Biological Expression in Hospitalised COVID-19 Patients and Post-Infectious Mortality: Comparison Between 2024 and 2020
 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Demographic Data
3.2. Medical History and Comorbid Conditions
3.3. Clinical Manifestations of COVID-19
3.4. Laboratory Findings
3.5. Radiological Findings
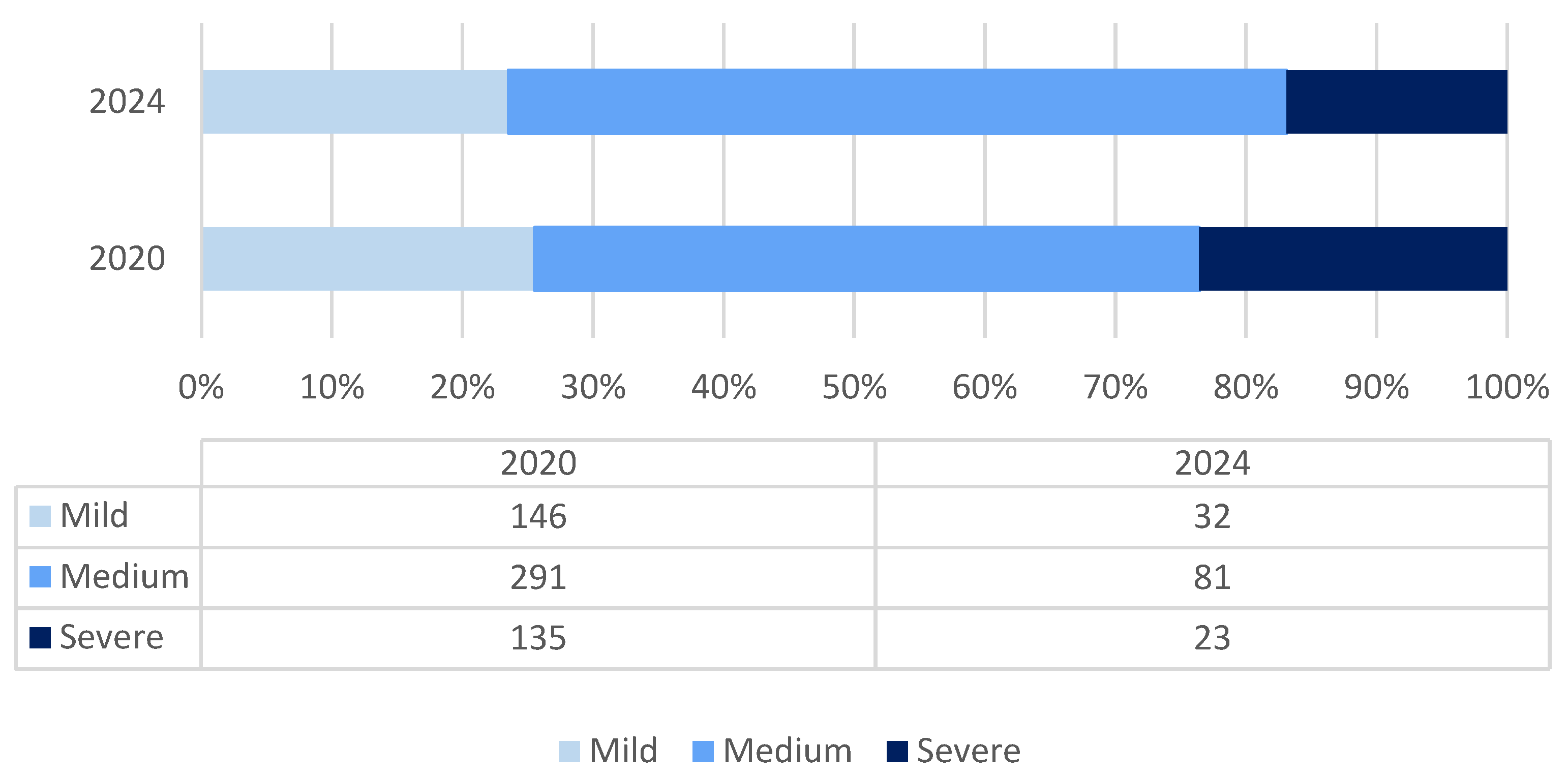
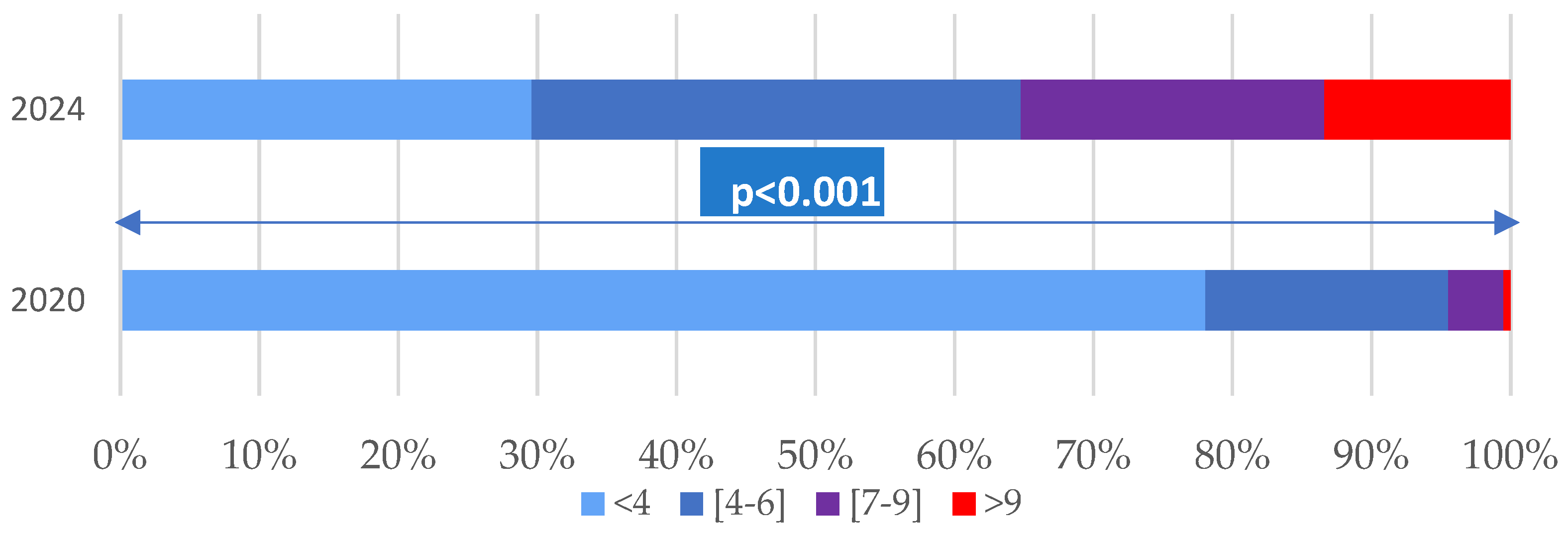
3.6. Clinical Forms, Complications, and Post-COVID-19 Deaths
3.7. Dynamics of COVID-19 Infection and Characteristics of Hospitalised Patients
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ALT | alanine aminotransferases |
| AST | aspartate aminotransferases |
| BMI | Body Mass Index |
| CK | creatine kinase |
| COVID-19 | Coronaviral Infection Disease-2019 |
| CRP | C Reactive Protein |
| NLR | Neutrophil/Lymphocyte ratio |
| OR | Odds Ratio |
| SARS-CoV-2 | Severe Acute Respiratory Syndrome Coronavirus-2 |
Appendix A

{kind=link}
{kind=link}
{kind=link}
| 2024: n1 = 138 | 2020: n2 = 583 | p * | |||||
|---|---|---|---|---|---|---|---|
| Average ± SD | Median | Max; min | Average ± SD | Median | Max; min | ||
| Temperature °C | 36.9 ± 0.75 | 36.7 | 39.3;36 | 36.24 ±0.61 | 36 | 0.6; 27.8 | 0.010 |
| Heart Ratio/min | 89.7 ± 15.92 | 89 | 28; 16 | 90.38 ± 2.90 | 89 | 42; 11 | 0.598 |
| Systolic BP mmHg | 131.22 ± 19.87 | 129.5 | 195; 80 | 131.43 ± 19.37 | 130 | 80; 204 | 0.981 |
| Diastolic BP mmHg | 79.53 ±11.88 | 80 | 113; 49 | 83.29 ± 13.84 | 82 | 144; 40 | 0.002 |
| Respiratory Rate/min | 19.35 ± 2.69 | 18 | 16.5; 6.4 | 20.35 ± 1.86 | 20 | 18.3;5.1 | <0.001 |
| Oxygen Saturation (%) | 95.54 ± 3.32 | 96 | 99;79 | 95.38 ±3.68 | 96 | 70;100 | 0.993 |
| 2024: n1 = 138 | 2020: n2 = 583 | p * | |||||
|---|---|---|---|---|---|---|---|
| Average ± SD | Median | Max; min | Average ± SD | Median | Max; min | ||
| WBC × 103/mm3 | 7.42 ± 3.38 | 6.55 | 17.1; 0.87 | 6.78 ± 3.49 | 6 | 0.6; 27.8 | 0.010 |
| N/Ly | 4.24 ± 3.78 | 3 | 22.2; 0.44 | 3.61 ± 3.58 | 2.43 | 38.15; 0.16 | 0.010 |
| Hb [g/dL] | 12.17 ± 2.01 | 12.1 | 16.5; 6.4 | 13.47 ± 1.86 | 13.5 | 18.3;5.1 | <0.001 |
| PTL × 103/mm3 | 212.54 ± 84.40 | 195 | 528; 45 | 230.77 ± 93.51 | 213.5 | 691; 14 | 0.018 |
| PCR | 72.59 ± 75.21 | 54 | 373;0.15 | 81.26 ± 81.40 | 48 | 330; 1 | 0.518 |
| ALT UI/L | 37.47 ± 45.26 | 31 | 340;6 | 50.75 | 33.5 | 706; 11 | <0.001 |
| AST UI/L | 38.29 ± 37.94 | 23.25 | 208;18 | 43.99 ± 34.79 | 33 | 287; 12 | <0.001 |
| CK | 157.86 ± 182.19 | 93 | 1322;16 | 177.26 ± 480.72 | 96 | 87; 52 | 0.511 |
| D-Dimers | 1619.71 ± 1946.5 | 933 | 10,000; 110 | 945 ± 1312.31 | 544.5 | 10,000; 100 | <0.001 |
| n1-2024 | % | n2-2020 | % | p | CI 0.95 | |
|---|---|---|---|---|---|---|
| Interstitial pattern | 103 | 74.6 | 197 | 33.7 | <0.001 | 0.325; 0.491 |
| Unilateral opacities | 17 | 12.3 | 50 | 8.5 | 0.173 | −0.022; 0.097 |
| Bilateral opacities | 12 | 8.6 | 263 | 45.5 | <0.001 | −0.431;−0.306 |
| Normal | 16 | 11.5 | 116 | 19.8 | 0.023 | −0.145;-0.020 |
| 2024 N1 = 137 | % | 2020 N2 = 583 | % | OR | CI 95 | p * | |
|---|---|---|---|---|---|---|---|
| Pneumonia | 127 | 92% | 439 | 75.3% | 4.16 | 2.22;7.78 | <0.001 |
| ARF | 25 | 18% | 175 | 30% | 1.98 | 1.22;3.07 | 0.004 |
| Hepatitis | 7 | 5% | 278 | 47.6% | 17.39 | 9.52;31.78 | <0.001 |
| CDD | 23 | 16.7% | 11 | 1.9% | 10.4 | 5.57;19.39 | <0.001 |
| Severe forms | 23 | 23.1% | 135 | 16.6% | 1.50 | 0.92;2.44 | 0.097 |
| Survival >90 days | 125 | 91% | 561 | 96% | 2.65 | 1.33;5.28 | 0.005 |
References
- CDC. Coronavirus Disease 2019 (COVID-19) 2020 Interim Case Definition. 2021. Available online: https://ndc.services.cdc.gov/case-definitions/coronavirus-disease-2019-2021/ (accessed on 21 January 2025).
- ECDC. Case Definition for Coronavirus Disease 2019 (COVID-19), as of 3 December 2020. 2020. Available online: https://www.ecdc.europa.eu/en/covid-19/surveillance/case-definition (accessed on 21 January 2025).
- World Health Organization. (2020). WHO COVID-19: Case Definitions: Updated in Public Health Surveillance for COVID-19, Published 16 December 2020. World Health Organization. Available online: https://iris.who.int/handle/10665/337834 (accessed on 21 January 2025).
- WHO Team. Epidemic and Pandemic Preparedness and Prevention (EPP)/Technical Document: COVID-19 Global Risk Assessment. Available online: https://www.who.int/publications/m/item/covid-19-global-risk-assessment (accessed on 16 February 2025).
- Ulrichs, T.; Rolland, M.; Wu, J.; Nunes, M.C.; El Guerche-Séblain, C.; Chit, A. Changing epidemiology of COVID-19: Potential future impact on vaccines and vaccination strategies. Expert Rev. Vaccines 2024, 23, 510–522. [Google Scholar] [CrossRef] [PubMed]
- Strategic Preparedness, Readiness and Response Plan to End the Global COVID-19 Emergency in 2022; World Health Organization: Geneva, Switzerland, 2022; (WHO/WHE/SPP/2022.01). Available online: https://www.who.int/publications/i/item/WHO-WHE-SPP-2022.1 (accessed on 12 January 2025).
- Swiss Re Institute. The Future of Excess Mortality After COVID-19. Available online: https://www.swissre.com/institute/research/topics-and-risk-dialogues/health-and-longevity/covid-19-pandemic-synonymous-excess-mortality.html (accessed on 10 March 2025).
- World Health Organization. ICD-11 Revision. Available online: https://icd.who.int/en (accessed on 11 January 2025).
- Drosdowsky, A.; Gough, K. The Charlson Comorbidity Index: Problems with use in epidemiological research. J. Clin. Epidemiol. 2022, 148, 174–177. [Google Scholar] [CrossRef] [PubMed]
- Charlson Comorbidity Index (CCI). Available online: https://www.mdcalc.com/calc/3917/charlson-comorbidity-index-cci (accessed on 11 January 2025).
- Ministry of Health. ORDER No. 1274 of February 28, 2024, for the Approval of the NATIONAL MEDICAL PRACTICE PROTOCOL Regarding the Treatment of SARS-CoV-2 Virus Infection; OFFICIAL GAZETTE No. 179 of March 5, 2024; Romanian Ministry of Health. Available online: https://legislatie.just.ro/public/DetaliiDocument/224341 (accessed on 21 January 2025).
- Ministerul Sanatatii. ORDINUL nr. 1.274 din 28 Februarie 2024 Pentru Aprobarea PROTOCOL NAȚIONAL de Practică Medicală Privind Tratamentul Infecției cu Virusul SARS-CoV-2. MONITORUL OFICIAL nr. 179 din 5 martie 2024; Ministerul Sanatatii. Available online: https://legislatie.just.ro/public/DetaliiDocument/279606 (accessed on 21 January 2025).
- Stoian, M.; Andone, A.; Boeriu, A.; Bândilă, S.R.; Dobru, D.; Laszlo, S.Ș.; Corău, D.; Arbănași, E.M.; Russu, E.; Stoian, A. COVID-19 and Clostridioides difficile Coinfection Analysis in the Intensive Care Unit. Antibiotics 2024, 13, 367. [Google Scholar] [CrossRef] [PubMed]
- Baruch, J.; Rojek, A.; Kartsonaki, C.; Vijayaraghavan, B.K.T.; Gonçalves, B.P.; Pritchard, M.G.; Merson, L.; Dunning, J.; Hall, M.; Sigfrid, L.; et al. Symptom-based case definitions for COVID-19: Time and geographical variations for detection at hospital admission among 260,000 patients. Influenza Other Respir. Viruses 2022, 16, 1040–1050. [Google Scholar] [CrossRef] [PubMed]
- Maison, D.P.; Tasissa, H.; Deitchman, A.; Peluso, M.J.; Deng, Y.; Miller, F.D.; Henrich, T.J.; Gerschenson, M. COVID-19 clinical presentation, management, and epidemiology: A concise compendium. Front. Public Health 2025, 13, 1498445. [Google Scholar] [CrossRef] [PubMed]
- Vasile, M.C.; Arbune, A.A.; Lupasteanu, G.; Vlase, C.M.; Popovici, G.C.; Arbune, M. Epidemiologic and Clinic Characteristics of the First Wave of the COVID-19 Pandemic in Hospitalized Patients from Galați County. J. Clin. Med. 2021, 10, 4210. [Google Scholar] [CrossRef] [PubMed]
- Sankar, K.; Modi, N.; Polyak, A.; Directo, M.P.; Johnson, L.R.; Kho, N.; Isonaka, S.K.; Pedraza, I.; Chen, P.; Modes, M.E. Comparison of clinical characteristics and outcomes of critically ill adults with SARS-CoV-2 infection during Delta and Omicron variant predominance periods: A single-hospital retrospective cohort study. BMJ Open Respir. Res. 2023, 10, e001274. [Google Scholar] [CrossRef] [PubMed]
- Cui, G.; Sun, Y.; Zou, Y.; Sun, R.; Gao, Y.; Liu, X.; Zhou, Y.; Zhang, D.; Wang, X.; Li, Y.; et al. Dynamic changes of Bacterial Microbiomes in Oropharynx during Infection and Recovery of COVID-19 Omicron Variant. PLoS Pathog. 2024, 20, e1012075. [Google Scholar] [CrossRef] [PubMed]
- Vlase, C.M.; Stuparu Cretu, M.; Vasile, M.C.; Popovici, G.C.; Arbune, M. Comparative Epidemiological and Clinical Outcomes on COVID-19 and Seasonal Influenza Hospitalized Patients during 2023. Infect. Dis. Rep. 2024, 16, 783–793. [Google Scholar] [CrossRef] [PubMed]
- Han, Y.; Guo, J.; Li, X.; Zhong, Z. Differences in clinical characteristics between coronavirus disease 2019 (COVID-19) and influenza: A systematic review and meta-analysis. NPJ Prim. Care Respir. Med. 2025, 35, 8. [Google Scholar] [CrossRef] [PubMed]
- Ho, M.; Levy, T.J.; Koulas, I.; Founta, K.; Coppa, K.; Hirsch, J.S.; Davidson, K.W.; Spyropoulos, A.C.; Zanos, T.P. Longitudinal dynamic clinical phenotypes of in-hospital COVID-19 patients across three dominant virus variants in New York. Int. J. Med. Inform. 2024, 181, 105286. [Google Scholar] [CrossRef] [PubMed]
- Murphy, S.A.; Khalil, F.; Fayaz, M.; Robinson, L.; Cummings, N.M. Mortality 30 and 90 Days After Hospitalisation for COVID-19: Prognostic Factors on Admission to Hospital. J. Glob. Med. 2021, 1, e13. [Google Scholar] [CrossRef]
- Hor, C.P.; Teo, L.K.; Wang, H.X.; Teoh, Y.J.; Chong, T.L.; Yen, C.H.; Mutalib, N.A.; Cheng, J.T. Morbidity and Mortality Outcomes for Patients with Moderate-to-Severe COVID-19 Diseases: A Post-Hospitalization Follow-Up Study. Int. J. Infect. Dis. 2023, 130, S152–S153. [Google Scholar] [CrossRef] [PubMed Central]
- Newman, J.; Flower, L.; Jones, R.; Phillips, V.; Couturier, D.-L.; Law, M.; Toshner, M.; Summers, C. Longer term post-hospital morbidity and mortality following admission with COVID-19: A systematic review and meta-analysis. ERJ Open Res. 2025. Available online: https://publications.ersnet.org/content/erjor/early/2025/02/20/2312054101281-2024 (accessed on 21 January 2025). [CrossRef]
- Pappas, A.G.; Panagopoulos, A.; Rodopoulou, A.; Alexandrou, M.; Chaliasou, A.-L.; Skianis, K.; Kranidioti, E.; Chaini, E.; Papanikolaou, I.; Kalomenidis, I. Moderate COVID-19: Clinical Trajectories and Predictors of Progression and Outcomes. J. Pers. Med. 2022, 12, 1472. [Google Scholar] [CrossRef] [PubMed]
| 2024 | % | 2020 | % | OR | CI95 | p * | ||
|---|---|---|---|---|---|---|---|---|
| Dementia | YES NO | 22 115 | 16.1% | 22 561 | 3.77% | 4.878 | 2.74;8.66 | <0.001 |
| Cerebrovascular Accident | YES NO | 17 119 | 12.5% | 15 568 | 2.57% | 5.409 | 2.81;10.409 | <0.001 |
| Chronic Heart Faillure | YES NO | 74 63 | 54% | 59 524 | 10.1% | 10.43 | 7.09;15.34 | <0.001 |
| Myocardial infarction | YES NO | 7 131 | 5.07% | 8 575 | 1.37% | 3.84 | 1.46;10.06 | 0.006 |
| Chronic Pulmonary Disease | YES NO | 27 110 | 19.7% | 15 568 | 2.57% | 9.29 | 5.26;16.39 | <0.001 |
| Liver disease | YES NO | 37 101 | 26.82% | 27 556 | 4.63% | 7.69 | 4.73;12.52 | <0.001 |
| Chronic kidney disease | YES NO | 17 121 | 12.3% | 24 559 | 4.12% | 3.27 | 1.75;6.08 | <0.001 |
| Diabetes mellitus | YES NO | 25 113 | 18.1% | 60 523 | 10.3% | 1.92 | 1.16;3.18 | 0.010 |
| Hemiplegia | YES NO | 7 131 | 5.07% | 7 576 | 1.2% | 4.39 | 1.65;11.70 | 0.003 |
| Peripheral vascular disease | YES NO | 15 123 | 10.9% | 6 577 | 1.03% | 11.72 | 5.37;25.59 | <0.001 |
| Connective tissue disease | YES NO | 1 137 | 0.72% | 5 578 | 0.86% | 1.18 | 0.13;10.20 | 0.877 |
| Peptic ulcer disease | YES NO | 23 115 | 16.62% | 5 578 | 0.86% | 22.11 | 10.76;45.43 | <0.001 |
| AIDS | YES NO | 3 135 | 2.17% | 5 578 | 0.86% | 2.56 | 10.76;45.43 | 0.184 |
| Tumors/ leukemia lymphoma/ | YES NO | 19 119 | 13.8% | 27 556 | 4.63% | 3.28 | 1.82;5.93 | <0.001 |
| Hypertenssion | YES NO | 81 55 | 59.6% | 175 408 | 30% | 3.43 | 2.36;4.98 | <0.001 |
| Obesity | YES NO | 28 70 | 28.6% | 176 269 | 39.6% | 1.63 | 1.01;2.62 | 0.042 |
| 2024 | % | 2020 | % | OR | CI95 | p * | ||
|---|---|---|---|---|---|---|---|---|
| Fever | Yes No | 86 52 | 62.3% | 290 292 | 49.8% | 1.66 | 1.14;2.43 | 0.008 |
| Chills | Yes No | 36 102 | 26.1% | 102 481 | 17.5% | 1.66 | 1.07;2.56 | 0.021 |
| Headache | Yes No | 41 97 | 29.7% | 144 439 | 24.7% | 1.28 | 0.85;1.94 | 0.225 |
| Myalgia | Yes No | 31 106 | 22.6% | 195 388 | 33.4% | 1.71 | 1.11;2.64 | 0.014 |
| Arthralgia | Yes No | 14 123 | 10.2% | 47 536 | 8.06% | 1.29 | 0.69;2.42 | 0.507 |
| Sore throat | Yes No | 31 107 | 22.5% | 123 460 | 21.1% | 1.08 | 0.639;1.693 | 0.724 |
| Rhinorrhea | Yes No | 15 118 | 10.9% | 18 565 | 3.9% | 3.85 | 1.97;7.53 | <0.001 |
| Cough | Yes No | 79 59 | 57.2% | 217 366 | 62.8% | 1.25 | 0.86;1.835 | 0.229 |
| Dyspnea | Yes No | 19 119 | 13.8% | 76 507 | 13% | 1.06 | 0.62;1.82 | 0.819 |
| Vomiting | Yes No | 8 130 | 5.8% | 23 560 | 3.95% | 1.49 | 0.65;3.40 | 0.334 |
| Diarrhea | Yes No | 25 112 | 18.2% | 81 502 | 13.9% | 1.38 | 0.84;2.26 | 0.195 |
| Asthenia | Yes No | 72 66 | 52.2% | 225 358 | 38.6% | 1.73 | 1.19;2.51 | 0.003 |
| Appetite loss | Yes No | 28 108 | 20.4% | 207 376 | 35.5% | 2.14 | 1.37;3.33 | 0.007 |
| Loss of small/taste | Yes No | 1 137 | 0.72% | 118 465 | 20.2% | 34.76 | 9.93;121.64 | <0.001 |
| Syncope | Yes No | 5 133 | 3.62% | 1 582 | 0.17% | 21.87 | 4.84;98.72 | <0.001 |
| Vertigo | Yes No | 4 134 | 2.9% | 46 537 | 7.89% | 2.86 | 1.06;7.76 | 0.037 |
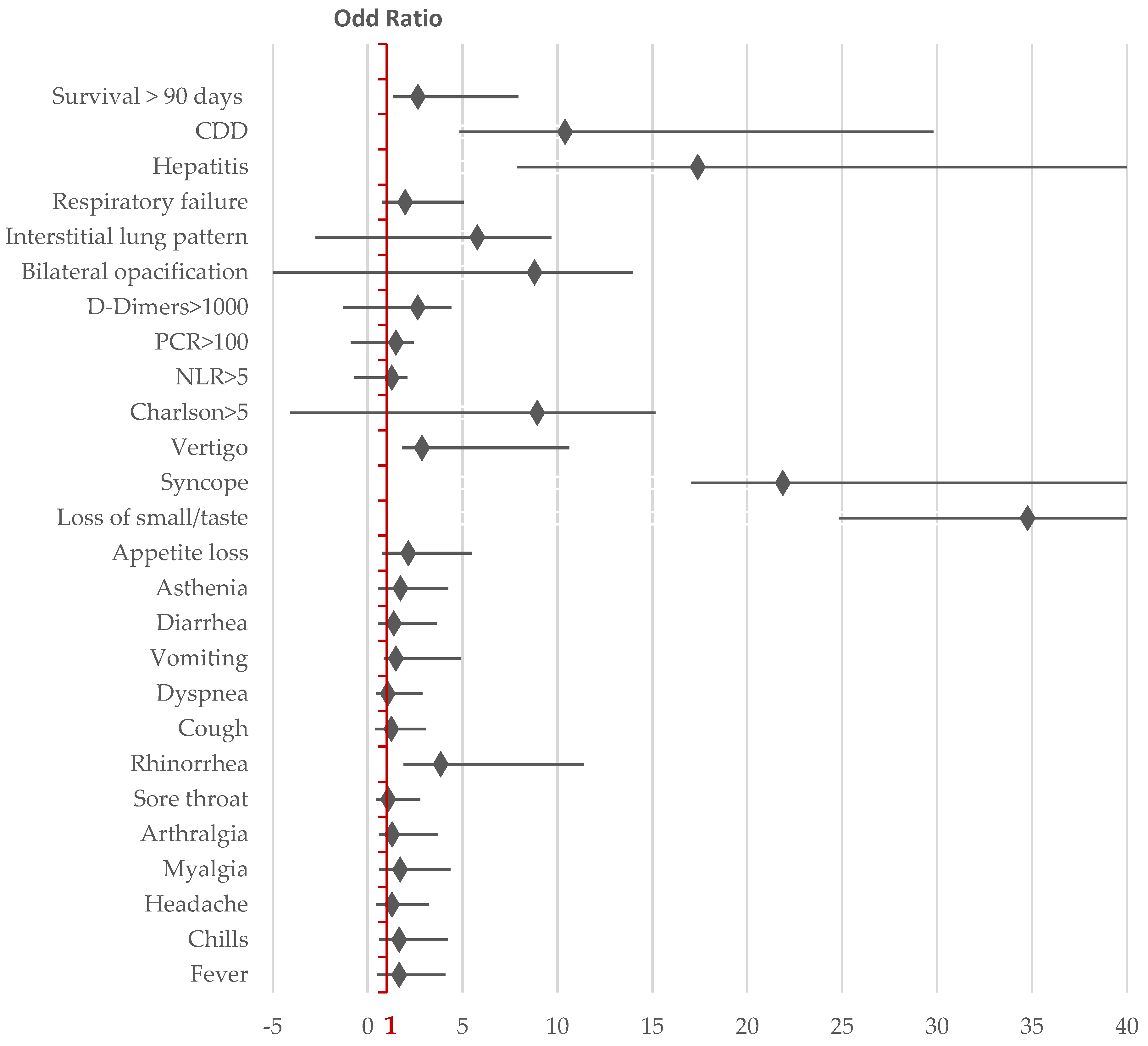
| 90 Days After-COVID-19 Hospitalisation | Survive N1 = 687 | Death N2 = 35 | OR | CI95 | p | |
|---|---|---|---|---|---|---|
| Male | Yes No | 396 326 | 23 12 | 2.42 | 1.21;4.86 | 0.012 |
| Charlson>5 | Yes No | 553 134 | 22 13 | 6.98 | 3.73;13.06 | <0.001 |
| Clostridioides difficile Diarrhoea | Yes No | 26 661 | 9 26 | 8.80 | 4.26;18.14 | <0.001 |
| CRP > 100 mg/dL | Yes No | 95 592 | 18 17 | 6.59 | 3.55;12.25 | <0.001 |
| NLR > 5 | Yes No | 129 558 | 19 16 | 5.13 | 2.73;9.66 | <0.001 |
| D-Dimers > 1000 mg/L | Yes No | 131 556 | 22 13 | 4.28 | 3.84;13.41 | <0.001 |
| Dementia | Yes No | 37 650 | 7 28 | 4.39 | 1,92;9.99 | <0.001 |
| Chronic Heart Disease | Yes No | 120 566 | 13 22 | 2.78 | 1.40;5.54 | 0.003 |
| Diabetes | Yes No | 80 607 | 6 29 | 1.56 | 0.63;3.87 | 0.327 |
| Obesity | Yes No | 198 329 | 6 11 | 0.906 | 0.33;2.48 | 0.848 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vlase, C.-M.; Plesea-Condratovici, A.; Arbune, A.-A.; Goroftei-Bogdan, R.-E.; Gutu, C.; Arbune, M. Dynamics of Clinical, Radiological, and Biological Expression in Hospitalised COVID-19 Patients and Post-Infectious Mortality: Comparison Between 2024 and 2020. Viruses 2025, 17, 630. https://doi.org/10.3390/v17050630
Vlase C-M, Plesea-Condratovici A, Arbune A-A, Goroftei-Bogdan R-E, Gutu C, Arbune M. Dynamics of Clinical, Radiological, and Biological Expression in Hospitalised COVID-19 Patients and Post-Infectious Mortality: Comparison Between 2024 and 2020. Viruses. 2025; 17(5):630. https://doi.org/10.3390/v17050630
Chicago/Turabian StyleVlase, Constantin-Marinel, Alina Plesea-Condratovici, Anca-Adriana Arbune, Roxana-Elena Goroftei-Bogdan, Cristian Gutu, and Manuela Arbune. 2025. "Dynamics of Clinical, Radiological, and Biological Expression in Hospitalised COVID-19 Patients and Post-Infectious Mortality: Comparison Between 2024 and 2020" Viruses 17, no. 5: 630. https://doi.org/10.3390/v17050630
APA StyleVlase, C.-M., Plesea-Condratovici, A., Arbune, A.-A., Goroftei-Bogdan, R.-E., Gutu, C., & Arbune, M. (2025). Dynamics of Clinical, Radiological, and Biological Expression in Hospitalised COVID-19 Patients and Post-Infectious Mortality: Comparison Between 2024 and 2020. Viruses, 17(5), 630. https://doi.org/10.3390/v17050630