
Development and Validation of the CARRA-VID Prognostic Score: C Reactive Protein to Albumin Ratio, Red Blood Cell Distribution Width and Age-Based Score for Prognostication of Hospitalized COVID-19 Patients

 ,
,  , , , , ,
, , , , , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Methods
2.2. Statistical Methods
2.3. The Process of Score Development
3. Results
3.1. Overview of the Development and Validation Cohorts of Patients
3.2. Overview of the CARRA-VID Score in the Development Cohort
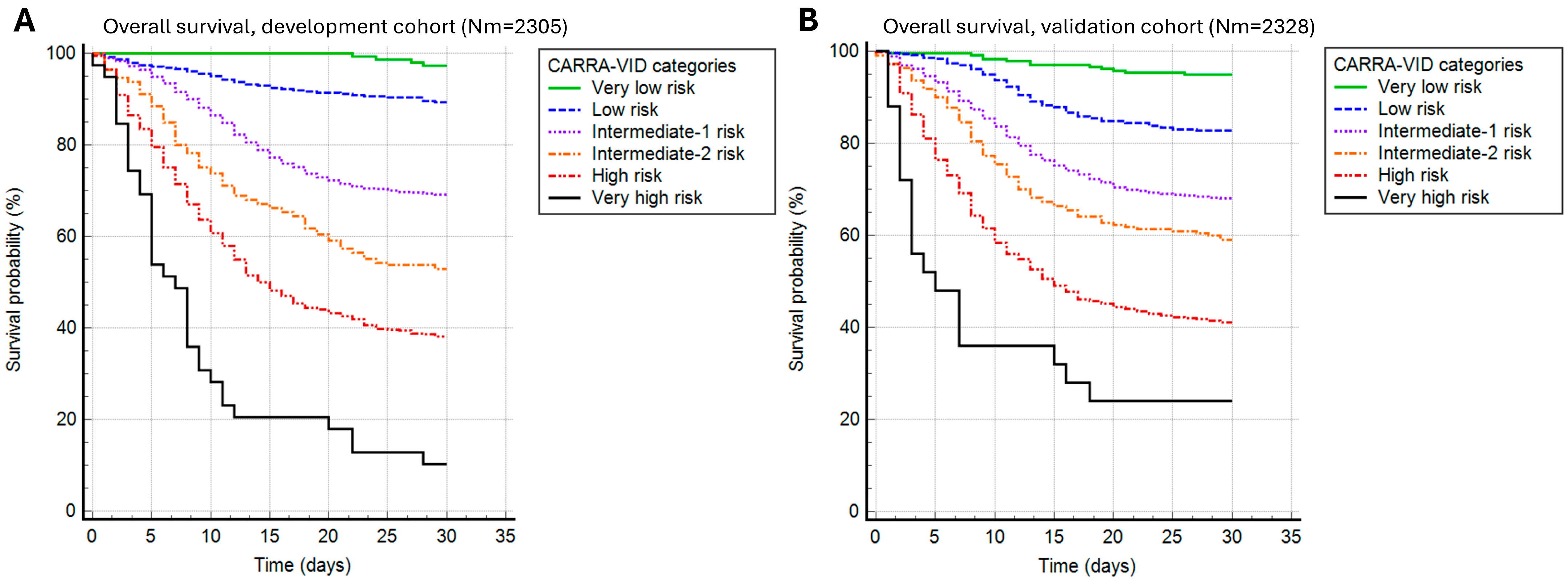
3.3. Prognostic Properties of the CARRA-VID Score in the Development and Validation Cohorts
3.4. Comparison of the CARRA-VID Score to Other Established Prognostic Systems
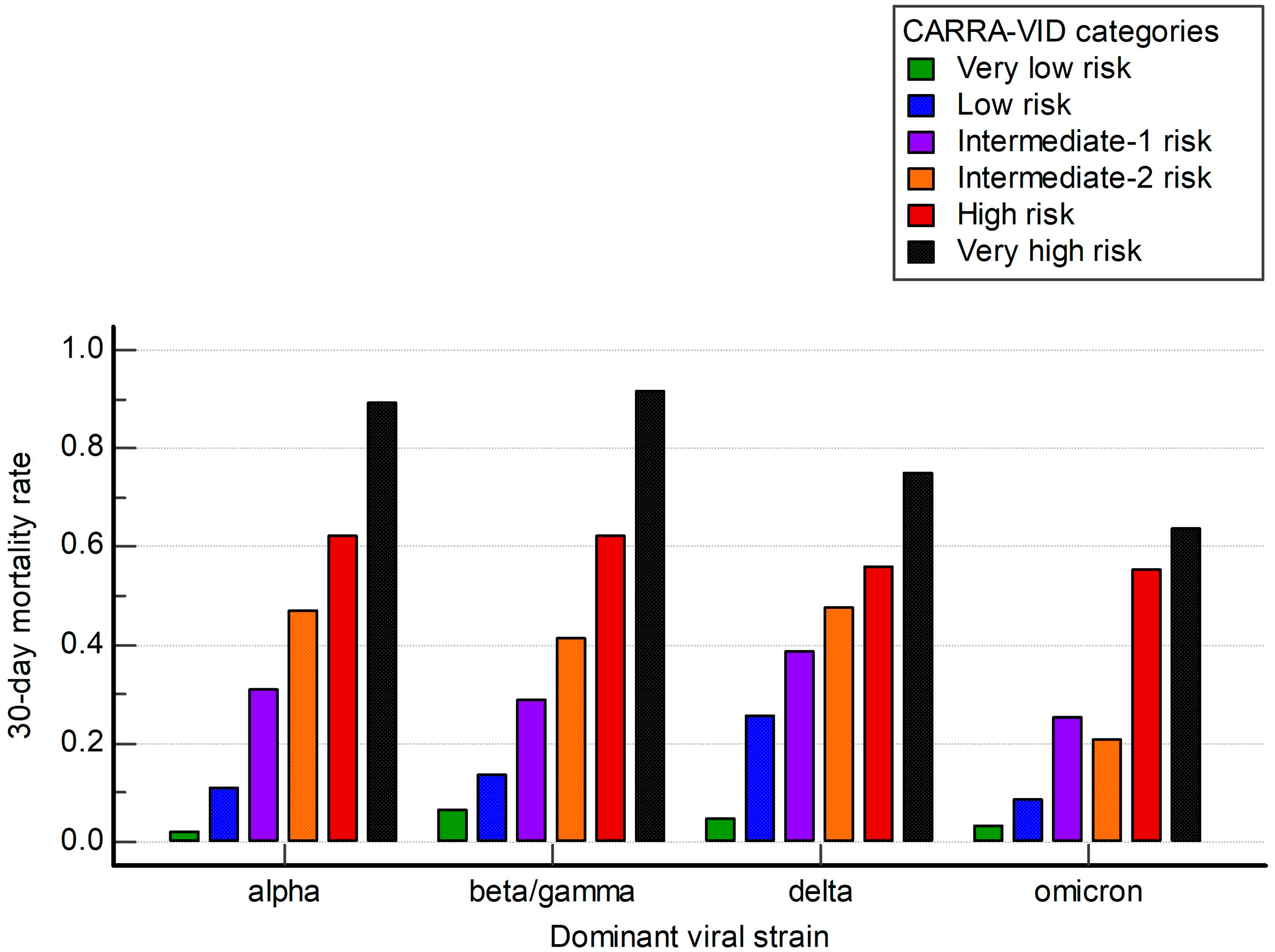
3.5. Usefulness of the CARRA-VID Score over Different Time Periods Dominated by Distinct Viral Strains
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ciotti, M.; Angeletti, S.; Minieri, M.; Giovannetti, M.; Benvenuto, D.; Pascarella, S.; Sagnelli, C.; Bianchi, M.; Bernardini, S.; Ciccozzi, M. COVID-19 Outbreak: An Overview. Chemotherapy 2019, 64, 215–223. [Google Scholar] [CrossRef]
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72,314 Cases From the Chinese Center for Disease Control and Prevention. Jama 2020, 323, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- Obeagu, E.I.; Obeagu, G.U. Thromboinflammation in COVID-19: Unraveling the interplay of coagulation and inflammation. Medicine 2024, 103, e38922. [Google Scholar] [CrossRef]
- Montazersaheb, S.; Hosseiniyan Khatibi, S.M.; Hejazi, M.S.; Tarhriz, V.; Farjami, A.; Ghasemian Sorbeni, F.; Farahzadi, R.; Ghasemnejad, T. COVID-19 infection: An overview on cytokine storm and related interventions. Virol. J. 2022, 19, 92. [Google Scholar] [CrossRef] [PubMed]
- Park, M.D. Macrophages: A Trojan horse in COVID-19? Nat. Rev. Immunol. 2020, 20, 351. [Google Scholar] [CrossRef] [PubMed]
- Robinson, M.W.; Harmon, C.; O’Farrelly, C. Liver immunology and its role in inflammation and homeostasis. Cell. Mol. Immunol. 2016, 13, 267–276. [Google Scholar] [CrossRef]
- Cha, H.J. Erythropoiesis: Insights from a genomic perspective. Exp. Mol. Med. 2024, 56, 2099–2104. [Google Scholar] [CrossRef]
- Lucijanic, M.; Krecak, I. The Complete Blood Count: Increasing Its Precision and Impact. Ann. Intern. Med. 2023, 176, eL230164. [Google Scholar] [CrossRef]
- Yang, C.; Suda, T. Microenvironmental dynamics in steady-state and stress erythropoiesis. Blood Sci. 2025, 7, e00219. [Google Scholar] [CrossRef]
- Patel, K.V.; Semba, R.D.; Ferrucci, L.; Newman, A.B.; Fried, L.P.; Wallace, R.B.; Bandinelli, S.; Phillips, C.S.; Yu, B.; Connelly, S.; et al. Red cell distribution width and mortality in older adults: A meta-analysis. J. Gerontol. A Biol. Sci. Med. Sci. 2010, 65, 258–265. [Google Scholar] [CrossRef]
- Lucijanic, M.; Cicic, D.; Stoos-Veic, T.; Pejsa, V.; Rahelic, D.; Lucijanic, T.; Vasilj, T.; Ivic, M.; Sedinic, M.; Kusec, R. Combining information on C reactive protein and serum albumin into the Glasgow Prognostic Score strongly discriminates survival of myelofibrosis patients. Blood Cells Mol. Dis. 2018, 72, 14–16. [Google Scholar] [CrossRef] [PubMed]
- Karampela, I.; Chrysanthopoulou, E.; Simitsis, P.; Skyllas, G.; Christodoulatos, G.S.; Antonakos, G.; Kandri, E.; Armaganidis, A.; Dalamaga, M. C-reactive protein/albumin ratio as a prognostic biomarker in critically ill septic patients: A prospective study. Eur. Respir. J. 2020, 56, 2751. [Google Scholar] [CrossRef]
- Haider Kazmi, S.J.; Zafar, M.T.; Zia, B.F.; Khalid, S.R.; Kumar, V.; Tabassum, S.; Ali, A.; Aziz, N.; Khan, N.A.; Kumari, K.; et al. Role of serum C-reactive protein (CRP)/Albumin ratio in predicting the severity of acute pancreatitis: A retrospective cohort. Ann. Med. Surg. 2022, 82, 104715. [Google Scholar] [CrossRef] [PubMed]
- Sunar, İ.; Ataman, Ş. Serum C-Reactive Protein/Albumin Ratio in Rheumatoid Arthritis and its Relationship With Disease Activity, Physical Function, and Quality of Life. Arch. Rheumatol. 2020, 35, 247–253. [Google Scholar] [CrossRef]
- Wu, J.; Tan, W.; Chen, L.; Huang, Z.; Mai, S. Clinicopathologic and prognostic significance of C-reactive protein/albumin ratio in patients with solid tumors: An updated systemic review and meta-analysis. Oncotarget 2018, 9, 13934–13947. [Google Scholar] [CrossRef]
- Lippi, G.; Plebani, M. Red blood cell distribution width (RDW) and human pathology. One size fits all. Clin. Chem. Lab. Med. 2014, 52, 1247–1249. [Google Scholar] [CrossRef]
- Piskač Živković, N.; Lucijanić, M.; Bušić, N.; Jurin, I.; Atić, A.; Andrilović, A.; Penović, T.; Domić, I.; Gnjidić, J.; Demaria, M.; et al. The associations of age, sex, and comorbidities with survival of hospitalized patients with coronavirus disease 2019: Data from 4014 patients from a tertiary-center registry. Croat. Med. J. 2022, 63, 36–43. [Google Scholar] [CrossRef]
- Lucijanić, M.; Stojić, J.; Atić, A.; Čikara, T.; Osmani, B.; Barišić-Jaman, M.; Andrilović, A.; Bistrović, P.; Zrilić Vrkljan, A.; Lagančić, M.; et al. Clinical and prognostic significance of C-reactive protein to albumin ratio in hospitalized coronavirus disease 2019 (COVID-19) patients: Data on 2309 patients from a tertiary center and validation in an independent cohort. Wien. Klin. Wochenschr. 2022, 134, 377–384. [Google Scholar] [CrossRef]
- Lucijanić, M.; Jordan, A.; Jurin, I.; Piskač Živković, N.; Sorić, E.; Hadžibegović, I.; Atić, A.; Stojić, J.; Rudan, D.; Jakšić, O.; et al. Red cell distribution width is a potent prognostic parameter for in-hospital and post-discharge mortality in hospitalized coronavirus disease 2019 patients: A registry-based cohort study on 3941 patients. Croat. Med. J. 2022, 63, 44–52. [Google Scholar] [CrossRef]
- World Health Organization. Clinical Management of COVID-19: Interim Guidance, 27 May 2020; World Health Organization: Geneva, Switzerland, 2020.
- Subbe, C.P.; Kruger, M.; Rutherford, P.; Gemmel, L. Validation of a modified Early Warning Score in medical admissions. Qjm 2001, 94, 521–526. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef] [PubMed]
- Oken, M.M.; Creech, R.H.; Tormey, D.C.; Horton, J.; Davis, T.E.; McFadden, E.T.; Carbone, P.P. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am. J. Clin. Oncol. 1982, 5, 649–655. [Google Scholar] [CrossRef] [PubMed]
- Lim, W.S.; van der Eerden, M.M.; Laing, R.; Boersma, W.G.; Karalus, N.; Town, G.I.; Lewis, S.A.; Macfarlane, J.T. Defining community acquired pneumonia severity on presentation to hospital: An international derivation and validation study. Thorax 2003, 58, 377–382. [Google Scholar] [CrossRef]
- King, J.T., Jr.; Yoon, J.S.; Rentsch, C.T.; Tate, J.P.; Park, L.S.; Kidwai-Khan, F.; Skanderson, M.; Hauser, R.G.; Jacobson, D.A.; Erdos, J.; et al. Development and validation of a 30-day mortality index based on pre-existing medical administrative data from 13,323 COVID-19 patients: The Veterans Health Administration COVID-19 (VACO) Index. PLoS ONE 2020, 15, e0241825. [Google Scholar] [CrossRef]
- Knight, S.R.; Ho, A.; Pius, R.; Buchan, I.; Carson, G.; Drake, T.M.; Dunning, J.; Fairfield, C.J.; Gamble, C.; Green, C.A.; et al. Risk stratification of patients admitted to hospital with covid-19 using the ISARIC WHO Clinical Characterisation Protocol: Development and validation of the 4C Mortality Score. Bmj 2020, 370, m3339. [Google Scholar] [CrossRef]
- Lucijanic, M.; Skelin, M.; Lucijanic, T. Survival analysis, more than meets the eye. Biochem. Med. (Zagreb.) 2017, 27, 14–18. [Google Scholar] [CrossRef] [PubMed]
- Lucijanic, M.; Soric, E.; Sedinic Lacko, M.; Sabljic, A.; Krecak, I.; Bistrovic, P.; Jordan, A.; Manola, S.; Jaksic, O.; Lucijanic, T.; et al. Gradual increase in red cell distribution width is similarly prognostic for in-hospital mortality in both anemic and non-anemic COVID-19 patients. J. Med. Virol. 2022, 94, 3509–3511. [Google Scholar] [CrossRef]
- Al-Rawi, Z.S.; Gorial, F.I.; Al-Bayati, A.A. Red Cell Distribution Width in Rheumatoid arthritis. Mediterr. J. Rheumatol. 2018, 29, 38–42. [Google Scholar] [CrossRef]
- Jordan, A.; Trkulja, V.; Jurin, I.; Marević, S.; Đerek, L.; Lukšić, I.; Manola, Š.; Lucijanić, M. Accounting for Red Cell Distribution Width Improves Risk Stratification by Commonly Used Mortality/Deterioration Risk Scores in Adult Patients Hospitalized Due to COVID-19. Life 2024, 14, 1267. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Development Cohort (N = 2305) | Validation Cohort (N = 2328) | p Value | |
|---|---|---|---|
| Age (years) | 73 (64–81) | 70 (60–79) | <0.001 * |
| Male sex | 1323 (57.4%) | 1287 (55.3%) | 0.147 |
| ECOG status on admission | 3 (1–4) | 3 (1–4) | 0.872 |
| MEWS score | 2 (1–4) | 3 (1–4) | <0.001 * |
| COVID-19 severity | |||
| Mild | 217 (9.4%) | 121 (6.8%) | <0.001 * |
| Moderate | 110 (4.8%) | 68 (3.8%) | |
| Severe | 1609 (69.8%) | 1252 (70.1%) | |
| Critical | 369 (16%) | 345 (19.3%) | |
| Co-infection on admission | 335 (14.5%) | 187 (10.1%) | <0.001 * |
| Charlson comorbidity index | 4 (3–6) | 4 (2–5) | <0.001 * |
| CRP (mg/L) | 91.1 (42.9–153.8) | 93.5 (43.3–158.9) | 0.334 |
| Albumin (g/L) | 32 (28–35) | 31.5 (29–34) | 0.5271 |
| RDW (%) | 14.1 (13.4–15.3) | 13.9 (13.3–15) | <0.001 * |
| Dominant viral strain | |||
| Alpha | 2259 (98%) | - | <0.001 * |
| Beta/Gamma | 46 (2%) | 1155 (49.6%) | |
| Delta | - | 816 (35.1%) | |
| Omicron | - | 357 (15.3%) |
| Development Cohort | sCARRA-VID Low Risk | sCARRA-VID Intermediate Risk | sCARRA-VID High Risk | p Value |
|---|---|---|---|---|
| Number of patients | 534 (23.2%) | 1126 (48.9%) | 645 (28%) | - |
| Age (years) | 59 (51–67) | 73 (65–80) | 82 (75–87) | <0.001 * |
| Male sex | 339 (63.5%) | 641 (56.9%) | 343 (53.2%) | <0.001 * |
| Day of disease on admission | 6 (1–9) | 5 (1–9) | 4 (1–8) | 0.001 * |
| ECOG status on admission | 1 (1–3) | 2 (1–3) | 3 (2–4) | <0.001 * |
| Pneumonia | 429 (80.3%) | 1024 (90.9%) | 619 (96%) | <0.001 * |
| Oxygen therapy | 382 (71.5%) | 957 (85%) | 599 (92.9%) | <0.001 * |
| MEWS score | 2 (1–3) | 2 (1–4) | 3 (1–4) | <0.001 * |
| COVID-19 severity | ||||
| Mild | 97 (18.2%) | 95 (8.4%) | 25 (3.9%) | <0.001 * |
| Moderate | 38 (7.1%) | 55 (4.9%) | 17 (2.6%) | |
| Severe | 351 (65.7%) | 803 (71.3%) | 455 (70.5%) | |
| Critical | 48 (9%) | 173 (15.4%) | 148 (22.9%) | |
| Co-infection on admission | 35 (6.6%) | 160 (14.2%) | 140 (21.7%) | <0.001 * |
| Charlson comorbidity index | 2 (1–4) | 4 (3–6) | 6 (4–7) | <0.001 * |
| Arterial hypertension | 298 (55.8%) | 831 (73.8%) | 491 (76.1%) | <0.001 * |
| Diabetes mellitus | 134 (25.1%) | 383 (34%) | 214 (33.2%) | 0.005 * |
| Hyperlipoproteinemia | 117 (21.9%) | 285 (25.3%) | 152 (23.6%) | 0.569 |
| Obesity | 170 (31.8%) | 338 (30%) | 143 (22.2%) | <0.001 * |
| Cong. heart failure | 42 (7.9%) | 177 (15.7%) | 158 (24.5%) | <0.001 * |
| Atrial fibrillation | 30 (5.6%) | 205 (18.2%) | 179 (27.8%) | <0.001 * |
| Coronary artery disease | 76 (14.2%) | 183 (16.3%) | 107 (16.6%) | 0.285 |
| Peripheral artery disease | 23 (4.3%) | 88 (7.8%) | 62 (9.6%) | <0.001 * |
| Previous CVI | 31 (5.8%) | 125 (11.1%) | 99 (15.3%) | <0.001 * |
| Previous myocardial inf. | 43 (8.1%) | 109 (9.7%) | 64 (9.9%) | 0.288 |
| Chr. kidney disease | 38 (7.1%) | 153 (13.6%) | 104 (16.1%) | <0.001 * |
| COPD | 33 (6.2%) | 88 (7.8%) | 54 (8.4%) | 0.165 |
| Chronic liver disease | 21 (3.9%) | 44 (3.9%) | 18 (2.8%) | 0.273 |
| Liver cirrhosis | 9 (1.7%) | 19 (1.7%) | 10 (1.6%) | 0.849 |
| Active malignancy | 38 (7.1%) | 127 (11.3%) | 108 (16.7%) | <0.001 * |
| Metastatic malignancy | 21 (3.9%) | 85 (7.5%) | 6 (10.2%) | <0.001 * |
| Dementia | 31 (5.8%) | 180 (16%) | 217 (33.6%) | <0.001 * |
| Alcohol use | 33 (6.2%) | 83 (7.4%) | 26 (4%) | 0.093 |
| Smoking | 46 (8.6%) | 76 (6.7%) | 19 (2.9%) | <0.001 * |
| IL-6 (pg/mL) | 22.9 (8.7–65.5) | 50.9 (22.1–118.4) | 105.5 (47.9–271.5) | <0.001 * |
| Procalcitonin (ng/mL) | 0.09 (0.05–0.21) | 0.21 (0.09–0.63) | 0.59 (0.22–2.69) | <0.001 * |
| WBC (×109/L) | 7.45 (5.3–10.2) | 7.8 (5.6–11) | 9.3 (6.7–13.2) | <0.001 * |
| Abs. lymphocytes (×109/L) | 1.0 (0.7–1.5) | 0.8 (0.53–1.2) | 0.7 (0.5–1.0) | <0.001 * |
| Hemoglobin (g/L) | 135 (122–144) | 127 (113–140) | 119 (104–133) | <0.001 * |
| Platelets (×109/L) | 222.5 (173–305) | 218 (159–297) | 219 (156–298) | 0.270 |
| CRP (mg/L) | 34.1 (14–82.8) | 88.4 (46.5–138.6) | 154.4 (93.9–215.1) | <0.001 * |
| Ferritin (µg/L) | 634 (309–1182) | 725 (416–1291) | 741 (411–1351) | 0.001 * |
| D-dimers (mg/L FEU) | 0.82 (0.51–1.88) | 1.37 (0.77–3.21) | 2.21 (1.15–4.25) | <0.001 * |
| CKD-EPI eGFR (ml/min/1.73 m2) | 92.2 (73.9–102.8) | 71.9 (48.2–90) | 54.2 (32.6–77.4) | <0.001 * |
| LDH (U/L) | 288 (213–388.8) | 355 (258–482) | 374.5 (274–514) | <0.001 * |
| AST (U/L) | 36 (25–56) | 41.5 (29–64) | 45 (30–71) | <0.001 * |
| ALT (U/L) | 33 (21–56) | 31 (19–52) | 28 (17–46) | <0.001 * |
| GGT (U/L) | 45 (24–89.7) | 43 (26–87) | 40.5 (22–80) | 0.183 |
| ALP (U/L) | 67 (53–86) | 70 (55–96) | 80 (59–110) | <0.001 * |
| Total bilirubin (µmol/L) | 10.5 (8.2–14.2) | 11.2 (8.6–15.6) | 12 (8.7–17.7) | <0.001 * |
| Albumin (g/L) | 35 (32–38) | 32 (29–34) | 29 (26–32) | <0.001 * |
| PT (%) | 104 (95–111) | 101 (90–109) | 94 (84–104) | <0.001 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lucijanic, M.; Piskac Zivkovic, N.; Busic, N.; Stojic, J.; Atic, A.; Derek, L.; Krecak, I.; Barsic, B.; Luksic, I. Development and Validation of the CARRA-VID Prognostic Score: C Reactive Protein to Albumin Ratio, Red Blood Cell Distribution Width and Age-Based Score for Prognostication of Hospitalized COVID-19 Patients. Viruses 2025, 17, 629. https://doi.org/10.3390/v17050629
Lucijanic M, Piskac Zivkovic N, Busic N, Stojic J, Atic A, Derek L, Krecak I, Barsic B, Luksic I. Development and Validation of the CARRA-VID Prognostic Score: C Reactive Protein to Albumin Ratio, Red Blood Cell Distribution Width and Age-Based Score for Prognostication of Hospitalized COVID-19 Patients. Viruses. 2025; 17(5):629. https://doi.org/10.3390/v17050629
Chicago/Turabian StyleLucijanic, Marko, Nevenka Piskac Zivkovic, Nikolina Busic, Josip Stojic, Armin Atic, Lovorka Derek, Ivan Krecak, Bruno Barsic, and Ivica Luksic. 2025. "Development and Validation of the CARRA-VID Prognostic Score: C Reactive Protein to Albumin Ratio, Red Blood Cell Distribution Width and Age-Based Score for Prognostication of Hospitalized COVID-19 Patients" Viruses 17, no. 5: 629. https://doi.org/10.3390/v17050629
APA StyleLucijanic, M., Piskac Zivkovic, N., Busic, N., Stojic, J., Atic, A., Derek, L., Krecak, I., Barsic, B., & Luksic, I. (2025). Development and Validation of the CARRA-VID Prognostic Score: C Reactive Protein to Albumin Ratio, Red Blood Cell Distribution Width and Age-Based Score for Prognostication of Hospitalized COVID-19 Patients. Viruses, 17(5), 629. https://doi.org/10.3390/v17050629